
Abstract
Mexican President Andrés Manuel López Obrador's historic election victory in 2018 marked a sharp break from past decades of neoliberal socioeconomic policies. López Obrador campaigned on the promise of deep reform, with health care high on his agenda. The public health care sector had been decimated by decades of budget cuts, eroding workers’ morale and patients’ confidence, and crippling all aspects of the system. This article looks back to the creation of the nation's public health care system in the early twentieth century during the administration of President Lázaro Cárdenas (1934–1940). This “universal” system was designed to implement a central social justice goal of the Mexican Revolution of health care for all. The program rested on two pillars: providing care to the nation's vast, impoverished rural population and actively engaging communities in their own health care. Our objective is to critically assess the two presidents’ health care initiatives within the distinct historical contexts of their administrations.
Keywords
This article compares the health care policies and programs of the current Mexican president, Andrés Manuel López Obrador (2018–2024), with those of Lázaro Cárdenas del Río (1934–1940). Since Mexico was established as a constitutional republic in 1917, they are the only presidents among its 27 administrations who affirmatively sought to implement the constitution's social justice commitments to improve the lives of ordinary people. Our objective is to critically assess the two presidents’ health care initiatives within the distinct historical contexts of their administrations.
When Mexico's 22nd President, Andrés Manuel López Obrador, took office in 2018, his country was at a crossroads. Mexico's nearly four decades-long experiment with harsh neoliberal policies failed to generate the promised prosperity. There was also widespread disillusionment with the country's established political parties and government institutions. López Obrador (popularly known by his initials as AMLO) promised deep reform, with health care high on his agenda. The public health care sector had been decimated by decades of budget cuts that eroded workers’ morale and patients’ confidence and crippled all aspects of the health care system. López Obrador was elected by a landslide. He received more votes than any other candidate in Mexican history, thereby winning the strong mandate he had campaigned for. MORENA (Movimiento de Regeneración Nacional/National Regeneration Movement), the party he founded in 2011, and its allies now also govern most of Mexico's 32 states. López Obrador fashioned himself a transformational leader, inspired by Mexico's first transformational leader, Lázaro Cárdenas del Río (1934–1940). President Cárdenas implemented fundamental social justice measures, including a framework for the delivery of health care for all. This article looks back to the creation of the nation's public health system during the presidency of Lázaro Cárdenas. Our objective is to critically assess the two presidents’ health care initiatives within contexts of their administrations.
We begin with an examination of Mexico's social conditions at the time Lázaro Cárdenas assumed office, devoting special attention to the nation's health. Following is a section introducing the federal health care system Cárdenas instituted, highlighting innovations to meet the specific needs of the country at the time. We next move to the second part of the twentieth century to consider the social conditions that contributed to López Obrador's landslide election victory. Then we present the health challenges the country faced when López Obrador assumed office, his efforts to ameliorate them, and the results to date. In closing, we assess whether President Cárdenas's early efforts to assure universal access to health care have been fulfilled by President López Obrador.
Research Methods
Data for this article come principally from Google Scholar and PubMed searches, in that they are the most comprehensive international databases on health in the Latin American region. Please note that the objective of this investigation is not a literature review per se, but rather to use published sources to characterize key dimensions of Mexican public health and health care during the administrations of Lázaro Cárdenas del Río (1934–1940) and Manuel López Obrador (2018–2024).
Our search terms and number of articles initially identified were as follows [GS: Google Scholar; PM = PubMed]. For the terms “políticas de salud en el gobierno de Lázaro Cárdenas” [GS:22,700] [PM:0], “health policies in the Lazaro Cardenas administration” [GS:15,700] [PM:2]. For the terms “políticas de salud en el gobierno de López Obrador” [GS:14,300] [PM:0], “health policies in the Lopez Obrador administration” [GS:9,440] [PM:124]. For the terms “historia de la salud pública en México” [GS:637,000] [PM:23], “history of public health in Mexico” [GS:3,700,000] [PM:5,350], and for the terms “el sistema de salud en México” [GS:1,190,000] [PM:86], “the Mexican health system” [GS:3,420,000] [PM:2,031]. In each instance we considered all peer-reviewed literature our search terms produced and assessed their relevance for our points. Our inclusion criteria, therefore, were a source's relevance and credibility (e.g., 1 ). Excluded were sources not germane to our investigation (e.g.,2,3). We also drew upon our own original research (e.g.,4–6).
Such official documents as the Diario Oficial de La Federación/Official Gazette of the Federation 7 and the Decreto de Creación de la Ley General de Salud /Creation Decree of the General Health Law, 8 and reports by INEGI (National Institute of Statistics and Geography, 9 and CONEVAL (National Council for the Evaluation of Social Development Policy 10 were also consulted where appropriate.
Mexico at the Beginning of the Cárdenas Administration
Here we summarize Mexico's social conditions when Lázaro Cárdenas took office in 1934.
At the time of the 1910–1920 revolution, Mexico was predominantly a rural, vastly unequal nation. President Porfirio Díaz's nineteenth century agricultural policies had displaced from their lands virtually all Mexican peasants and indigenous communities and concentrated its ownership among the rich. 11 By 1910, nearly all of Mexico's territory was devoted to commercial agriculture. In a population of around 15 million, there were 7,500 large landholders (hacendados) and only 45,000 mid-sized farmers. The Catholic church owned about half the nation's arable land and tens of millions of hectares had been sold by the government to powerful American interests, including Hearst and Texas Oil. This greed-driven expropriation failed to leave enough land for domestic cultivation and, ultimately, caused massive food shortages and urban rioting. 12
At the end of the revolution, then, around 3.5 million Mexicans worked as agricultural laborers, 2.5 million of whom owned absolutely nothing 13 ; slightly over six in ten (66.6%) lived in small settlements of 2500 inhabitants or fewer. 14 Nearly 90 percent of all settlements lacked roads, access to railroads, telegraph and telephone services, mail, priests, markets, and steel tractors. 15 There was a similar lack of associated infrastructure, including electricity, sewers, and plumbing, and virtually a complete absence of licensed physicians, nurses, and pharmacists.
The impact of the long revolution on Mexico's health was devastating. Entire communities were weakened by poverty and debilitated by endemic disease, and often died at an early age. 16 The 1930 census found that most certified and registered deaths were due to preventable diseases, mainly diarrhea and enteritis, pneumonia, respiratory infections, typhoid, and paratyphoid. Indeed, in 1934, 42.5 percent of deaths were of infectious and parasitic origin, with at least 25,000 deaths from malaria, 12,000 from tuberculosis, and 6,000 from dysentery. 1 That census also revealed just 4,767 licensed and registered physicians for a population of more than 16 million, the vast majority of whom were concentrated in major cities. Mainstream medical attention was all but nonexistent especially in states with large indigenous populations.
The Lázaro Cárdenas's presidency (1934–1940) brought hope to a nation worn down by years of civil war. He came to power through the interacting dynamics of an overwhelming popular vote (98.2%); an agreement within the National Revolutionary Party (NPR), the hegemonic political party antecedent to the Institutional Revolutionary Party (PRI) which held uninterrupted predominance from 1929 to 2000; and the corrupt institutional powers of the state. Nevertheless, Cárdenas quickly mobilized unprecedented popular support. At the end of 1933 as the NPR presidential candidate, he proposed the country's first six-year governing plan (1934–1940) designed to implement primary unmet economic and social goals of the 1917 Constitution. The plan conceptualized a strong central interventionist state designed to oversee the development, management, and regulation of the country's economic and social activities, while also guaranteeing private property and individual rights. 17 Moreover, in 1937 Cárdenas issued a manifesto to integrate disenfranchised sectors including peasants, manual workers, women, youth groups, and the army into the party's formal structure. 18
While the 1917 Constitution recognized the rights of small farmers to own land, it was not until the Cárdenas administration that this right came to fruition. By the end of his term, nearly half of Mexico's arable lands (over 18 million hectares) had been redistributed, although little of it was high quality farmland. Landless peasants also became eligible for credit at government banks, a demand critical to the success of small farmers. Cárdenas guaranteed other important social rights, the core principles of which were social solidarity, equality, inalienability, state subsidization, and stakeholder participation. He also nationalized foreign-owned industries, including Mexico's vast oil reserves and railroads, bolstering the country's position as a sovereign nation.
The Dawn of Public Health in Mexico
Notably, the Cárdenas government established institutionalized health services and a formal program of medical attention in rural areas.
The president believed that Mexico would never become a rich modern nation without sweeping land reform, much more intensive agricultural production, and major improvements in the economic and social conditions of average citizens. Yet he feared these objectives could not be met in the absence of a vast expansion of rural medical services.
15
In a major speech the president proclaimed,
President Cardenas favored a national health care system to address the poor health of the country's vast rural population and to implement the revolution's promise of health care for all. He recognized, however, that this endeavor would require not simply a major reorganization of existing health services, but also an in-depth understanding of the specific health problems within each of Mexico's many diverse regions and careful planning and administering allocated resources. Also, indispensable would be training the personnel to be sent into the remote countryside. Visionary physician Miguel E. Bustamante laid bare the scope of the need when he said this medical corps must become “health evangelists to whom [would fall] the tasks that were needed in every corner . . . for that profound hygienic and sanitary transformation in the country”. 20 Because the elite and educated considered the poor health of the rural population a result of their “stupidity and ignorance,” also essential would be “expansion of educational programs and health propaganda, promotion of preventive medicine, and eradication of beliefs and practices viewed by health authorities as harmful for the health and morality of the individual and the collectivity”.20, p. 748
Cárdenas prioritized maternal and child health (in 1935 alone, at least 100,000 children died) in addition to the health of workers and peasants from marginalized rural areas. In 1936 he created mobile sanitary brigades, rural hygiene centers, and the visiting nurse and Rural Agrarian Medical Services. These programs quickly bore fruit. While life expectancy in 1930 was only 33 years, by 1940 it had reached 41.5 while general mortality dropped from 26.6 to 22.8 per 100,000 during the same period. In 1935, there were 5,205 reported deaths from smallpox, in sharp contrast with 1940 when there were only 1,341. 1 , p. 624
Nevertheless, not all the president's contemporaries were convinced that inserting doctors into rural areas and prioritizing health education were key to Mexico's socioeconomic transformation. Some saw the approach as too narrow and destined to yield a lesser payoff than major infrastructural investment such as roads, telecommunications, and housing.(20, p. 773)
President Cárdenas's Initial Priorities for the Nation's Health
During Cárdenas's first six months in office, he proposed a massive 5.5 percent increase in the federal budget for health services in outlying communities. In 1934 the Servicios Coordinados de Salubridad y Asistencia (Coordinated Services for Health and Assistance) was established as a cost-shared collaboration between the federal Secretaría de Salubridad y Asistencia (Secretary of Health and Assistance) and state governments. A four-tiered structure of health units was created with staffing determined by a region's size. Some physicians were assigned to brigadas móviles (mobile brigades) to travel the countryside in the event of an epidemic or natural disaster. These mobile brigades were designated as both health emissaries and misiones culturales (cultural missions), charged with health education, teaching maternal and infant care, administering immunizations, and providing general medical consultations. 21 In the area of infrastructure, the president prioritized delivery of potable water to remote populations and formal campaigns against malaria and onchocerciasis (river blindness). 22 Important strides were also made in the expansion of health care institutions. 23
Cárdenas's Two Pillars for Extending Health Services to Marginalized Communities
Cárdenas’s vision for improving the nation's health rested on two pillars: assigning pasantes de medicina (interns) to communities throughout the countryside and community activism, that is, community engagement in its own health care.
Pillar One: Pasantes de Medicina (Interns). Commentators of the day were harshly critical of Cárdenas's circumscribed vision for Mexican modernization. They saw him blaming the country's poor health on the lack of doctors when there were far deeper problems, including lack of clean water, roads, housing, and inadequate nutrition.20, p. 773 Ignoring these critiques, in 1936, the Cárdenas administration proposed to Congress that all medical students be obligated to spend six months to one year living in remote rural regions to learn firsthand about health and health problems there. This “social service” (servicio social) requirement was not intended as an arbitrary exercise of state power, and factors like family needs were considered in assigning doctors to communities. President Cárdenas's vision of what the social service requirement could achieve was an expansive one: Beyond simply mandating young physicians to live and work in rural settings, he wanted them to internalize the more abstract revolutionary goal of health care for all. Indeed, Gustavo Baz, then-director of National Autonomous University of Mexico (UNAM)'s School of Medicine (Mexico's premier medical school), told the 1936 graduating class (the first who had been assigned pasante placements), “You have all completed six years of study . . . normally you would receive your degree within a few months . . . but instead, I have come to ask that you patriotically lend yourselves to one of the most singular experiments that has ever been recorded in the history of medicine.(19, p. 398
This turned out to be no small task. Mexican physicians of the day were mainly from privileged urban backgrounds and held the same prejudices against poor and indigenous people as their social class contemporaries—that they were dirty, stupid, ignorant, and boorish. These prejudices heavily influenced medical students’ attitudes about the nascent pasante program.
Pasantes’ responsibilities included much more than patient care and inoculations. Focusing on the larger objective of creating socially conscious physicians genuinely dedicated to rural Mexicans’ health and well-being, the pasantes were to conduct community-wide social and health surveys, produce periodic summaries, and a final report upon their completion of service. They were required to adopt an ethnographic approach, eliciting the community's history, climate, economic potential of lands, quality of nearby roads, natality and mortality, ethnicity, eating habits, and major health problems.19, pp. 399–400 The pasante was to synthesize this information into at a “community health diagnosis,” which was also to include information on herbal and other empirical treatments, birth customs, and childcare. The medical establishment expressed special interest in “traditional” medical practices because it wanted them eradicated.
Community reception to the pasantes was mixed. Some were cautiously welcomed and their services appreciated, while others were marginalized, stigmatized, isolated, accused of witchcraft, and even forced to flee their communities. But above all, the greatest impediment to the success of the pasante program was most pasantes’ antipathy toward working to benefit the rural populations they had been dispatched to serve. While some pasantes embodied the revolutionary ideal of bringing medical care to remote regions, most saw the requirement as simply an obstacle in their path toward certification. Indeed, critics within the medical establishment were convinced that the pasante program was bound to fail because young doctors did not want to leave comfortable urban lives and lucrative medical practices.22, p. 9 Others felt the very idea of universal social service for physicians was ill conceived, exploitative, a blatant state effort to take over medical care, and possibly a step toward communism.20, pp. 773–774
Given the extent of resistance, in 1938, just two years after the pasante program began, the new profession of rural physician was created. Young men from the countryside were selected with the idea that they would be more easily integrated into rural communities and that their rural roots would inspire them to become committed agents of social change. But many established physicians, holding the same class biases as pasantes, blocked the ability of these rural doctors to succeed. For example, rural physicians were denied entry into public hospitals for required training, treated disrespectfully, and taunted as “second class medical doctors,” “improvised physicians,” and “charlatans”.20, p. 779 Consequently, this brief experiment was abandoned in the mid-1940s.
Pillar Two: Community Engagement. Community action or community engagement was the second pillar on which President Cárdenas's health plan was based. Local committees consisting of community members would be established for health promotion and would work with the community as a whole to define their most critical health problems and develop plans for remediation. Priority would be given to community and household-level problems, including garbage and waste disposal and improved infrastructure. A multidisciplinary perspective based on existing models for community engagement and prior successful health promotion projects would guide training and implementation. 24
But, as with the pasante program, there were major barriers to implementation. Simple lack of political will was primary, and opportunities to define and operationalize the concepts of community action/engagement were not pursued. There was also never a serious effort to rebalance the single-minded focus of the health system away from curative allopathic medicine toward a more holistic and preventive orientation.25,26 Lack of a dedicated budget was another major issue. Additional practical problems included the question of who would supervise the community health committees and what criteria would count as success or failure and progress or stagnation. Designating community engagement as a core on which the Mexican national health care system rested remained an ideal. 27
In 1935, Lázaro Cárdenas commissioned the creation of a social security institute to be funded jointly by the state, insured workers, and their employers. Although the plan was approved by both legislative bodies, it was not until 1943 that it passed into law. 28 La Ley del Seguro Social (the Social Security Law) mandated legal responsibility for the nation's collective health to the state. The following year the Instituto Mexicano Seguro Social (IMSS, the Mexican Social Security Institute), a system of pensions and health care services for all Mexican citizens was established. But this mandate was never fully realized because large segments of the population (e.g., informal sector workers, the self-employed, poor rural, and indigenous workers) were never incorporated into the system. 29
Mexico After Cárdenas and Before López Obrador: The Consolidation of Neoliberalism
Mexico experienced economic stability and growing prosperity during the half century following the end of World War II. Still, the country endured other significant problems important among which was persistent external interference. During the 1960s and 1970s, successive governments accepted massive U.S. and international loans for infrastructure development with the expectation that the loans would be easily repaid with projected oil revenues. When the global oil glut of the 1980s produced a dizzying fall in oil prices, the Mexican government found itself unable to pay even the interest on these loans and defaulted, producing systemic economic collapse. A perpetual cycle of indebtedness followed which progressively intensified as international lenders set punishing conditions for issuing further loans. These conditions included eliminating most tariffs and other trade barriers on products and services, nationalizing the private banking system, devaluing the Mexican peso, imposing structural adjustment “shock measures,” comprehensive foreign exchange controls, and fundamental reconceptualization of the social welfare responsibilities of the state. A further condition was modification of the 1943 Social Security Law to no longer be fully subsidized by the state.
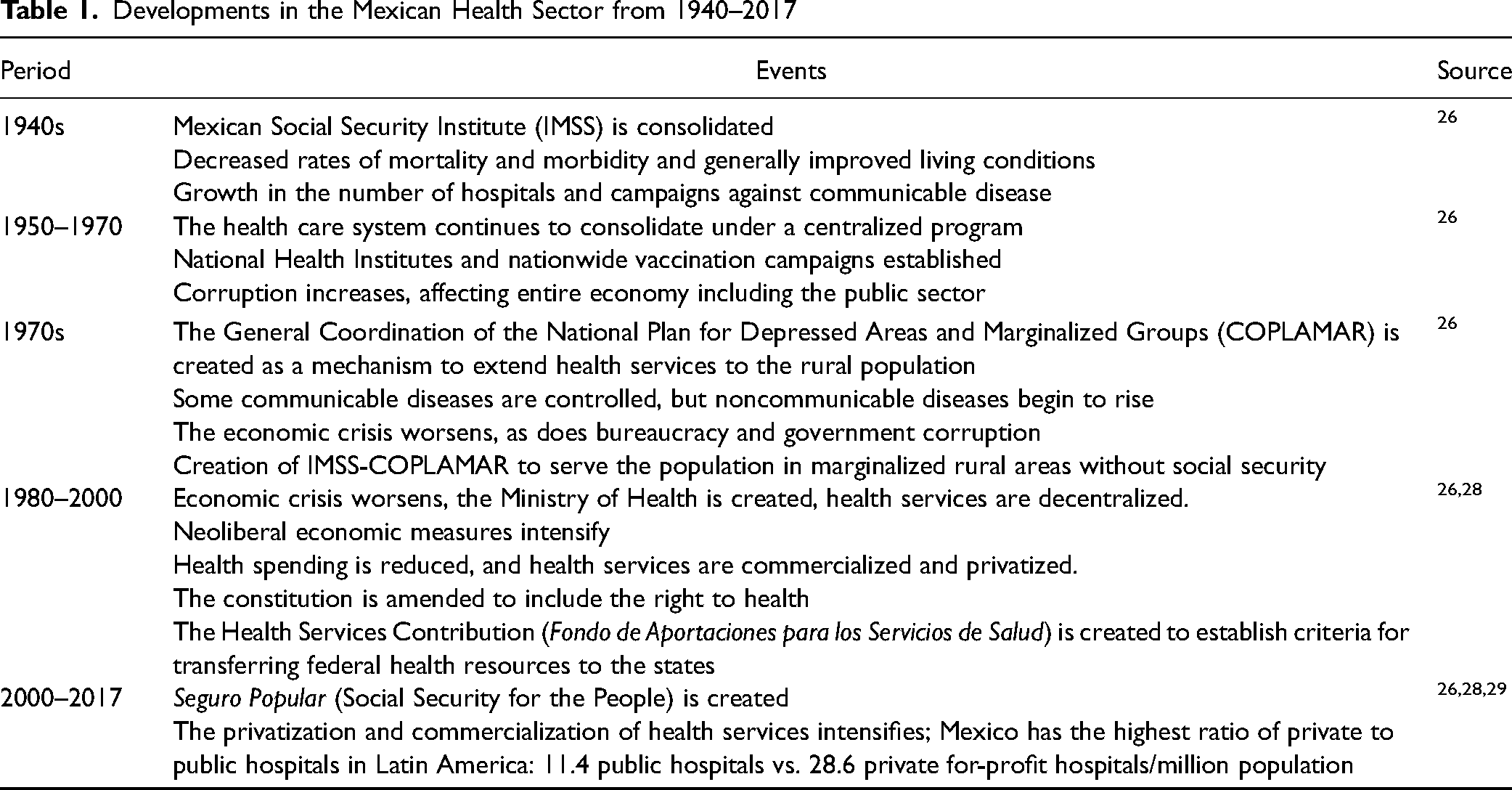
Yet even these drastic measures of the 1980s and 1990s were not enough to rescue Mexico's economy. 30 Making matters worse was the 1994 passage of the North American Free Trade Agreement (NAFTA), which precipitated massive financial speculation, capital flight, and another economic collapse. To recoup losses, the U.S. Treasury and the International Monetary Fund created a US$50 billion bailout fund, with access conditioned on further acceptance of NAFTA's austerity measures, including strict control of public finances and introduction of tariff-free markets into the country's protectionist economy. 31 Mexico was also obliged to carry out further structural reform that included dismantling state agencies, deregulating many more industries, removing nearly all import restrictions, and partially privatizing key economic sectors including railroads, airlines, ports, petrol, and financial services. The state was also forced to discontinue subsidies and other programs to aid small farmers, devastating the agricultural sector. Some farmers turned to planting marijuana and poppies while vast numbers migrated domestically or to the United States, sometimes even becoming a source of cartel labor.32,33 These sociopolitical and economic developments that followed Lázaro Cárdenas's administration are key to understanding the significance of Andrés Manual López Obrador's 2018 election victory. (Table 1).
Developments in the Mexican Health Sector from 1940–2017
Mexican Social and Public Health at the Start of López Obrador's Administration (December 2018)
López Obrador called the landslide vote that brought him to power in 2018 the mandate for the change he had campaigned for. He characterized it as a victory for ordinary people and a repudiation of the neoliberal austerity that had caused massive upward wealth redistribution and major cuts in the social safety net. 34 He boldly regarded his administration as Mexico's Fourth Transformation, seeking to rhetorically link it to the three earlier transformational periods in Mexican history: the Independence Movement (1810–1821), La Reforma (1858–1861), and the Mexican Revolution (1910–1920). Despite widespread fear among the privileged that his administration would usher in radical socialism, he described his governing philosophy as “anti-neoliberal but moderate.” Rather than challenging the foundations of the capitalistic system, the new president aimed for “a model of capitalism with a human face”, 35 , p. 2 that is, capitalism sensitive to fundamental human needs.
Given the size of the population still without social security coverage and access to health services, López Obrador has advocated for further extension of such services, as had been President Cárdenas's intention. The new president campaigned with the promise that, if elected, his administration would institute a completely new public health care system, often citing Denmark as a model. He argued that a better system was needed because, while the twentieth century had seen important health gains for Mexico's general population, there were also serious declines. On the positive side, during the 1980s infant mortality dropped from 69 to 38 per thousand live births, and overall mortality from 9.9 to 7 per thousand. 36 Yet devastating problems also emerged due, in part, to the nation's aging population, in concert with the environmental degradation typical of an impoverished country rapidly transitioning from mainly rural to predominantly urban. The environmental problems were further exacerbated by NAFTA's requirements. 26
Since NAFTA's passage, the country's health has deteriorated further, with dramatic increases in disorders associated with the ubiquitous “junk food” culture that quickly displaced traditional eating habits. 37 Diabetes mellitus is now a major cause of Mexican morbidity and disability and the second leading cause of death, with an estimated prevalence of 15 percent (approx. 28 million adults). Over the past thirty years, mortality attributable to diabetes increased by an astonishing 77 percent, presumably attributable in large part to sharply increased sugar consumption. 38 Significant health damage secondary to diabetes is also on the rise, including impaired vision (13.9% retina damage, 6.6% total loss of sight; 39) and other serious chronic conditions. Sinisterra-Loaiza and colleagues 39 compared age-adjusted morbidity in Mexico with the economically comparable countries of Argentina, Brazil, and Chile. They found Mexico with the highest rate of ischemic heart diseases (diet can play an important role), along with much higher death rates from malnutrition 40 and anemia.42,a In addition, infectious diseases such as tuberculosis, acute respiratory and diarrheal infections, HIV, and maternal mortality remain significant problems. 43
Toward Universal Healthcare: Convergence or Divergence from Cárdenas to López Obrador?
When López Obrador assumed office in 2018, he found a population not only in poor health but with tens of millions (27%) without guaranteed access to medical services. 44 To fulfill Cárdenas's dream of health care for all, he pledged a program that would provide all uninsured Mexicans with enrollment, services, and medicines free of charge. To offer health services appropriate to the targeted populations, health care institutions would be reoriented away from strict reliance on allopathic (biomedicine) medicine toward preventive medicine and wellness care. Core questions, then, would not only be how many doctors, clinics, beds, and medications are needed to assure the nation's health, but also how much illness can be averted through preventive health measures and how communities could be organized to enhance members’ health and wellbeing.
Upon taking office, López Obrador announced the creation of the federal Institute of Health for Wellbeing (Instituto de Salud para el Bienestar, INSABI). Its mission is to establish integrated networks of Mexico's major health care institutions of IMSS, the Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (Institute of Security and Social Services for State Workers), Pemex (Petróleos Mexicanos, Mexican Petroleum) and state health systems. Primary care centers would be staffed by interdisciplinary Equipos de Salud para el Bienestar (Healthcare Teams for Well-Being) with assistance from local communities. This was a nod toward restoring the community action/participation component of Cárdenas's health care plan. 27 Local groups would prioritize their community's most pressing health-related concerns and collectively develop strategies to alleviate them.
In August 2022, INSABI was suspended, and its functions transferred to IMSS, which then became the only federal entity providing healthcare to people without social security coverage. The newly created IMSS Bienestar Program is universal, one hundred percent state-funded, and without copays or other costs to users. It is designed to prioritize preventive health care through integrated networks of services and suppliers. Moreover, all medical staff will become state employees, be offered security of employment through long-term contracts, and assured comparable working conditions across clinical professions. The president recognized that such guarantees will be crucial for improving morale and creating dedicated, committed medical personnel. These guarantees also offer a dramatic contrast from the neoliberal period when staff turnover was high for all personnel, but particularly for physicians and nurses, who were generally hired on temporary short-term contracts with low wages, high risk of being fired, limited benefits, and no collective bargaining power. 45 The IMSS Bienestar Program will become operational in 24 of Mexico's 32 states by the end of López Obrador's administration in 2024, having enrolled 68 percent of the country's uninsured (the governors of six states chose not to participate in the program.).
Another way López Obrador plans to improve access to health care services while significantly reducing public costs is by purchasing hospitals that currently operate under public/private partnership agreements (asociaciones público-privadas). The president stated that maintaining this type of “exploitational” plan, introduced by former presidents, costs many times more than buying the facilities outright, adding, “When [former governments] gave you the contracts, you were the favored ones, but that has changed; now the favored children are the Mexicans, the people.” 46 , p. 6
The Impact of Cárdenas's and López Obrador's Policies on the Social Determinants of Health
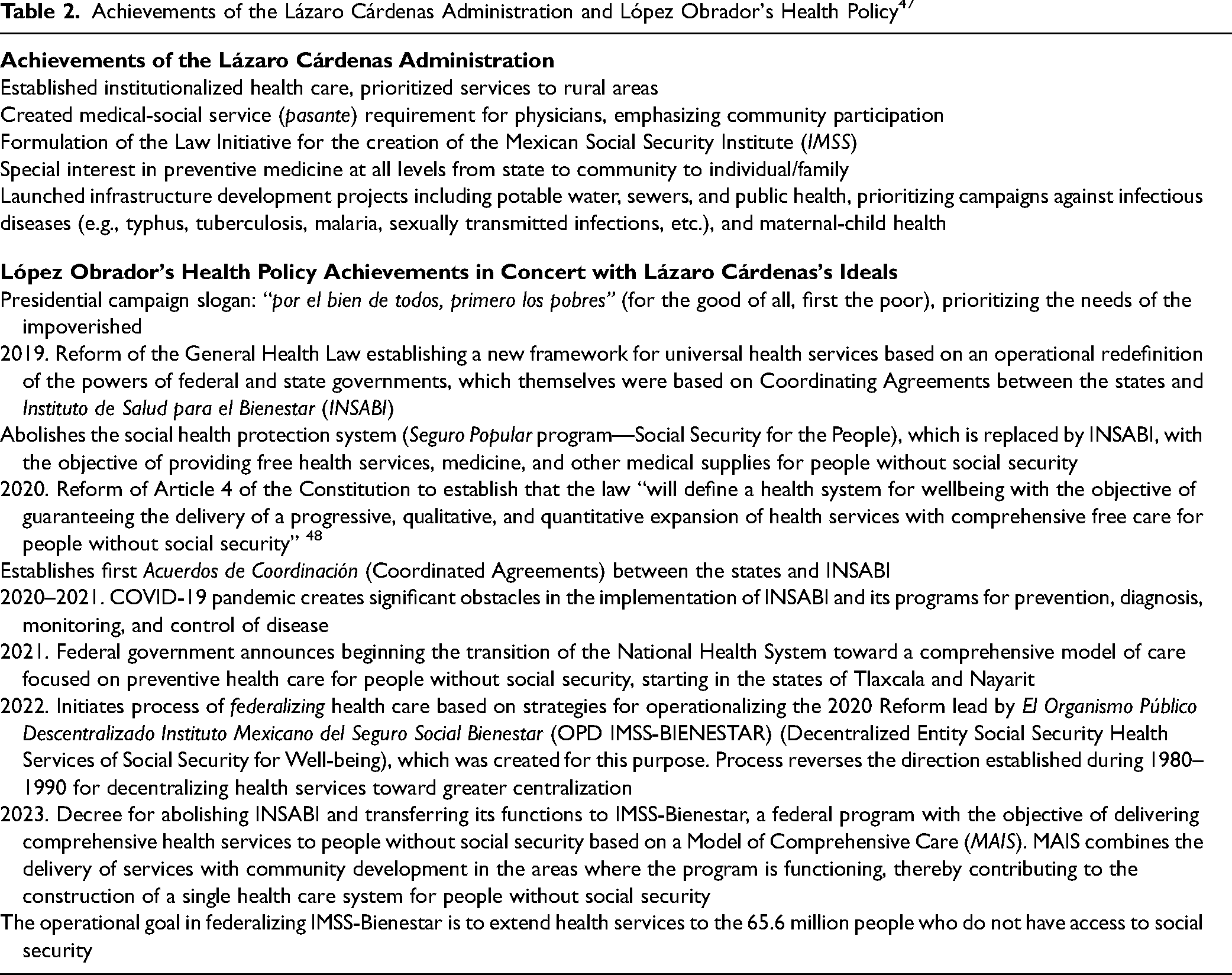
Table 2 summarizes President Lázaro Cárdenas’ achievements in the health sector and the policy actions taken by President López Obrador that reflect Lázaro Cárdenas's ideals.
Achievements of the Lázaro Cárdenas Administration and López Obrador's Health Policy 47
Comparing the impact on the nation's health of the two presidents’ health policies is obviously not a straightforward proposition, given the passage of time and the distinct socio-historical contexts of their governments. Lázaro Cárdenas's policies were broad and consistent with the country's immense needs. Most notably, they involved improving the dismal material conditions of the great majority of Mexicans by instituting reforms in the educational, labor (e.g., improving working conditions for laborers and peasants), and agrarian sectors (e.g., redistributing more than 20 million hectares, enabling peasants to get credit and loans); making infrastructural improvements for the widely dispersed indigenous communities; and expanding and strengthening the health sector. 48 That is, Cárdenas prioritized reducing poverty and improving quality of life as much as providing the poorest citizens with access to medical care. Yet these significant achievements would not endure, as successive administrations did not share Lázaro Cárdenas's social justice values.
Most of López Obrador's initiatives have been directed specifically toward reducing inequality between the poor and the rich (“primero los pobres”). 49 For example, he significantly increased the official minimum wage, in part to compensate for its 70 percent decline in spending power since the late 1970s; when López Obrador entered office, Mexico's minimum wage was among the lowest in Latin America. He also instituted the Senior Citizens Program, a universal pension for people aged 65 and over; he created scholarships for low-income students and established new public institutions for higher education (beginning in the 1980s, growth in public colleges and universities stagnated while their private counterparts flourished). 50 He also launched the Programa Sembrando Vida (Sowing Life Program) to support peasants in reforestation efforts, and the Programa Jóvenes Construyendo el Futuro (Program for Youth Building the Future), a one-year scholarship to help youth become more competitive in the labor market.
Consequently, there has been significant progress in reducing poverty and economic inequality during the Lopez Obrador administration. This has been achieved by, among other methods, increasing purchasing power through significant increases in the minimum wage, holding taxes constant, and controlling the price of gasoline. Similarly, a process of strengthening the IMSS-Bienestar Program was initiated and, remarkably, much of this progress occurred during the COVID-19 pandemic and an intensified “war on drugs.”
However, much work remains before most Mexicans can be assured a healthy and secure existence. The inequalities in access to quality health care seen in 2018 at the start of López Obrador's six-year term remain virtually unchanged. These inequalities include significant differences by socioeconomic stratum, based on whether one is enrolled in social security, maintains urban or rural residence, and of indigenous ethnicity, among others. At the same time, some health care indicators such as the number of doctors and nurses per 1,000 inhabitants; access to services for serious illness (e.g., percentage of diabetes cases diagnosed and controlled in the country); and outcomes (e.g., mortality rates for children under five, ratio of maternal deaths per 100,000, mortality rate from tuberculosis) place Mexico close to the average of countries of Latin America and the Caribbean, yet far from those established by the Organization for Economic Cooperation and Development (OECD), to which Mexico belongs. 51
One limitation of our research is that the administrations of Lázaro Cárdenas and Andrés Manual López Obrador are separated by nearly a century, an era of contradictory economic and political developments and characterized by the social historian Eric Hobsbawm as “the age of extremes”. 52 Moreover, while we can assess the legacy of President Cárdenas's policies on the nation and its people through the lens of time, we need a generation or more to make comparable assessments of López Obrador's legacy.
Another limitation is that a focus on a specific aspect of Mexican health policy—infant mortality or immunization campaigns, for example—may have produced more meaningful results. We opted, however, not to do so given the vast methodological challenges of such an approach. Chief among these is historical and contemporary variability in criteria for diagnosis, definition, and measurement of sociosanitary conditions, as well as important variation in difficult-to-measure problems associated with access to and availability of quality health care. For infant mortality, for example, the definition has changed from death in the first 24 h postpartum to death of an infant who manifests at least one vital sign. Similarly, both the definition and management of tuberculosis have changed over time. In essence, then, our work has aimed to broadly analyze public health policies focused on health care for the most socially vulnerable groups.
Here we have offered a first attempt to analyze the health policies of Presidents Lázaro Cárdenas and Andrés Manual López Obrador. They are Mexico's only two left-leaning presidents among the country's 27, beginning in 1913 with Victoriano Huerta's coup over the democratically elected Francisco I. Madero. These other administrations have mostly neglected the interests of the Mexican public in favor of those of elite people and their own. While further analysis is required based on their way of governing and their actual efforts to reduce poverty and inequality between rich and poor, Cárdenas and Lopez Obrador stand out from the other presidents. A more systematic analysis of the legacy of each of the other 25 presidents could focus on aspects of their policies that supported and harmed the poor. As interesting as it might be, such an analysis is beyond this article's scope.
Conclusions: Were Presidents Cárdenas and López Obrador's Health Policies Transformational?
As was the case during the Lázaro Cárdenas administration, President López Obrador inherited a health sector with extensive structural deficiencies. Key among both were a notable lack of health care workers and major infrastructural obstacles to strengthening and expanding health services, especially for the most vulnerable people. For President Cárdenas, the most vulnerable was the rural population; for President López Obrador, it is the tens of millions without social security today.
Among Lázaro Cárdenas's many achievements was the birth of institutionalized health care. López Obrador will be remembered for significantly strengthening health services for the population with scarce or no access to such services. The pillars of the Cárdenas program for delivering rural health care were creating a social/medical service requirement for medical interns and community action/participation. López Obrador has retained Cárdenas's social/medical service requirement and support for community-based action. In addition, he has federalized health services operated by the IMSS-Bienestar Program and by so doing, is seeking to guarantee the constitutional right to progressive, quantitative, and qualitative health services for Mexico's marginalized populations. As was the case with Cárdenas's innovations, those of López Obrador are neither easily implemented nor popular with the establishment.
Two important factors may further impede the short-term success of López Obrador's program. The IMSS-Bienestar Program has failed to implement a community action component within primary health care, neglecting the health benefits such programs may offer. For example, it was program administrators who established the local health committees without the benefit of community participation. This means that the objective of community engagement is being ignored. Moreover, while the program seeks to guarantee access both to primary care and core specialties, it is structured so that the importance of highly specialized medical services (e.g., advanced diagnostics, procedures, and treatments performed in state-of-the-art facilities) is further reinforced. It would be better to see much greater emphasis on community-based actions to prevent illness performed by trained individuals who are supported by their communities, as well as a stronger system for the delivery of primary care. Instead, we see a framework that prizes the allopathic (biomedical) model and neglects both preventive care and traditional medicine practitioners, including midwives and other traditional healers. Federalizing health services and increasing the number of clinical specialists without meaningful community engagement will inevitably result in a system less capable of meeting the needs of Mexico's most vulnerable populations. This was a problem Lázaro Cárdenas faced and never satisfactorily resolved. By all appearances, Andrés Manuel López Obrador is on the same path.
Footnotes
Acknowledgments
The authors thank Richard M. Rosenthal, Rosalynn A. Vega, Cristina Gordillo Marroquín, Yuyan (Gloria) Yang, and Callum Bohn for patient, generous conceptual and editorial assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.