
Abstract
Informal employment has been identified as an important social determinant of health. This article addresses the processes through which informal employment affects workers’ health in Chile. The study's methodological approach was based on qualitative interviews with 34 formal and informal workers. The findings show how workers perceive informal employment as negatively affecting their mental and physical health through different dimensions of their living and working conditions. Incorporating a gender perspective proves to be integral to the analysis of these processes. The article concludes by discussing how neoliberalism underlies such vulnerability processes and negatively impacts on the population's health.
Keywords
An understanding of health that goes beyond the hospital-centric biomedical model and the narrow focus on risk factors related to individual lifestyles exposes the social causes of disease and their deep political roots. 1 Within this frame, neoliberalism and its manifestations in neoliberal economic and social policies have been highlighted as crucial determinants of health and well-being worldwide. 2
Neoliberalism is connected with adverse global health outcomes through complex systemic, dynamic, multilevel, and multicausal processes.3,4 Given that informality is an employment condition closely associated with state deregulation, 5 we argue that the expansion of informal employment is also an important way in which neoliberalism has become embodied in ill health, focusing specifically on the study of the emblematic context of Chile, which has served as a social laboratory for the implementation of neoliberal economic and labor policies. While informal employment clearly preceded the development of neoliberalism, the institutionalization of informality and its widespread extension beyond the private market to the public sector has happened alongside the implementation of such policies.
Although informal employment is widespread worldwide, it has rarely been analyzed from the point of view of health inequalities. 6 Some studies have identified an association between informal employment and ill health.7,8 Informality has been shown to be related to worse self-perceived physical and mental health, 9 but there is a lack of research on how workers experience such relationships, which is needed to advance our understanding of the ways in which neoliberal socioeconomic policies eventually get “under the skin.” The main aim of this article is to fill this gap by deepening our understanding of how workers perceive informal employment as adversely affecting their health and producing health inequalities. A second aim is to incorporate a gender perspective into the understanding of these processes. We do so by tracing the links between different dimensions of living and working conditions and negative health outcomes according to the experiences of formal and informal Chilean workers by means of a qualitative research design.
Informal Employment as a Social Determinant of Health
Changes in labor markets since the 1980s have led to the proliferation of more precarious forms of employment both in advanced economies and beyond, so that employment has gradually lost its role as a source of guaranteed rights and social protection. 10 These transformations have had an unequal and detrimental impact on the population's health to the extent that, drawing on increasingly available scientific evidence, 11 Williams, Schrecker, and Bambra declared employment insecurity as one of the “neoliberal epidemics” worldwide. 12
Studies have delved into the harmful health consequences of unfavorable employment and working conditions, showing a higher prevalence of occupational accidents 13 and an increased risk of suffering from poor mental health.14,15 Despite this increasing interest in the impact of working and living conditions on health, 16 few efforts have been made to examine the processes behind such associations, particularly concerning the relationship between informal employment and health.
The Effects of Informal Employment on Health
Informal employment is an adverse employment condition which has been conceptualized as a category of employment conditions that is different from precarious employment. 6 According to the International Labour Organization, 17 informal employment is an unregulated form of work that can present different characteristics depending on whether it takes place in the formal or informal sector or in households. This absence of regulation includes the lack of a formal agreement between employers and employeesa, as well as a lack of labor regulation or social protection. 18
The few studies examining the impact of informal employment on health have shown a clear association between informality and poor mental health.8,19,20 They have also revealed its physical repercussions on occupational health.21,22,23 The clearest evidence in this direction is provided by empirical studies analyzing informal employment and workers’ health from a population perspective.7,24 These studies consistently reveal a (gendered) association between informal employment and ill health. However, we know little about either the processes by which informality affects health or the gendered nature of this relationship.
We expect informality to have specific detrimental effects on health due to the lack of social protection and labor regulations. These distinctive features are likely to produce specific outcomes in terms of perceived insecurity, material deprivation, social isolation, and access to safety measures, affecting physical and mental health.
Our theoretical approach draws on a broad definition of health that considers general feelings of malaise or discomfort, such as suffering, a sense of failure, anguish, and depressive states—all elements that have been associated with the harmful characteristics of employment, such as non-recognition, intensification of work, and isolation. 25 Therefore, we understand health effects as the systematic expression of different signs or symptoms of discomfort which are triggered by material conditions, situations, and states related to poor living and working conditions.
The Need for a Gender Perspective
A number of studies have examined the relationships among different dimensions of employment conditions as gendered determinants of physical and mental health. 26 However, to our knowledge, no studies have yet examined the processes through which informality affects health from a gender perspective. This gap exists despite women being over-represented in informal employment across the world. 27 Women's over-representation in informality has been attributed to the fact that they are widely employed as domestic workers 28 and that they are the main performers of home-based work, 29 types of work that both generally take place within an informal employment relationship. In Latin America, women's labor market participation has increased significantly in recent decades, not least as part of households’ strategies to supplement their incomes. 30 Such increases in women's employment have mainly been in the informal sector, which accounts for more than 80 percent of job creation in some countries. 31
Previous research has also established that, compared with those in a formal employment relationship, informality results in worse health outcomes for Chilean workers, 32 although the relationship was only statistically significant for men; formal employment did not seem to have the same protective effect for women. 9 This highlights the importance of applying a gender perspective to the analysis of the relationship between informality and health, which, theoretically and analytically, considers the links between gender segregation and working conditions that potentially impact health, as well the interrelations between productive and reproductive work.
The Chilean Context
Informal employment has become increasingly widespread, even in advanced economies, 33 following neoliberal structural labor market reforms over the last four decades. In Latin America, a significant share of informal activities has been subordinated to the formal economy through downsizing, subcontracting, and outsourcing processes, resulting in a loss of social protection for workers.30,34 In 1990, informal employment reached 40 percent of the active population in Latin America 31 and has remained at very high levels ever since, even through the pandemic period. 35
Chile has been considered an early and paradigmatic example of the implementation of neoliberal policies in the region, notably during the civic-military dictatorship of 1973–1990. 36 A series of radical reforms severely transformed the labor market, resulting in the proliferation of informal employment. A salient characteristic of these processes has been the downsizing of public employment through the expansion of contracts for service provision, which are civil agreements under which there is no labor link with the service's commissioner. 37 Significantly, these new forms involve a skilled labor force, with the public administration as a main commissioner of their services, in a context of depleted public budgets and restrictions on public employment. This represents a qualitative transformation that has contributed to the normalization and institutionalization of informality. These reforms were accompanied by the expansion of ideologies of entrepreneurship and individual effort and responsibility. 38
Moreover, due to market deregulations and an active policy of dismantling trade unions, unionization and union activity have decreased, while entrepreneurship has been promoted. 39 In this context, the recent increase in the employed population has been, in large part, due to the rise in self-employment (increasing by 5.3% in 2016, 2.0% in 2019, 8.0% in 2021, and 4.3% in 2023, 40 a category which often falls within the definition of informal employment 41 and which is characterized by low wages. The average monthly wage for self-employed workers is US$385 (while the national average wage is US$681), although half of these workers earn less than US$299. 42
Although the share of informal employment in Chile is lower than in most Latin American countries, 43 with official reports placing it at 27 percent, 44 studies show that this figure has been significantly underestimated and that informality more accurately accounts for almost 40 percent of all employment. 41 This percentage rises to 45 percent among women, approximately 10 percent higher than for men.9,31
Methods
Research Strategy
This study used a qualitative methodology inspired by grounded theory 45 to explore the experience of informal employment and the process whereby informal workers in Chile perceive effects on health. The study developed an abductive strategy, 46 starting from the broad a priori standpoint that employment has repercussions on health and the quality of life through employment's effects on living and working conditions. 47 This strategy aimed to identify how workers perceive the processes by which these two domains (living and working conditions) affect their health. The approach and research instruments were approved by the Ethical Committee of Clinical Investigation of Parc de Salut MAR de Barcelona.
Data
The data for the study were obtained from semi-structured interviews conducted with 34 workers, selected by means of an intentional sampling strategy that sought the inclusion of the full spectrum of types of formal and informal employment, as defined by Ruiz and colleagues. 37 The sample included four groups of workers: dependent formal workers (salaried with contracts, homeworkers with contracts, and domestic workers with contracts); dependent informal workers (salaried with fee contracts, homeworkers with fee contracts, salaried without contracts, homeworkers without contracts, domestic workers without contracts, and family workers); non-dependent formal workers (employers with five or more workers and self-employed professionals); and non-dependent informal workers (employers with fewer than five workers and non-professional self-employed workers). We defined workers subject to an employer-employee relationship as dependent workers, and those who worked independently—i.e., had several clients but no employer—as non-dependent workers. Table 1 describes the sample in detail and provides the codes used to identify excerpts from interviews.
Sample Characteristics.
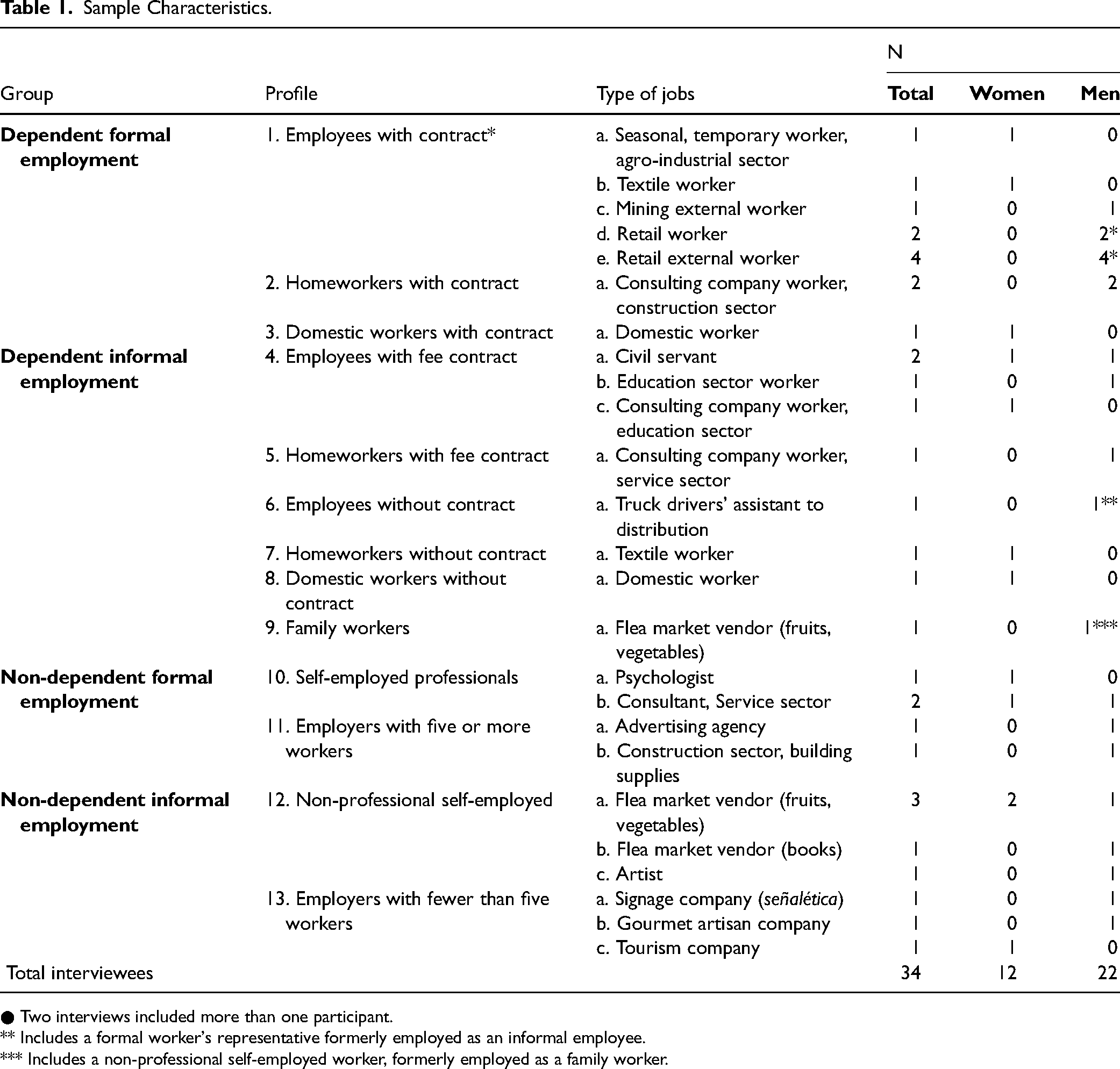
● Two interviews included more than one participant.
** Includes a formal worker's representative formerly employed as an informal employee.
*** Includes a non-professional self-employed worker, formerly employed as a family worker.
Initial access to participants was facilitated by the non-governmental organization Fundación Sol, followed by snowball sampling. All in-depth interviews were conducted by this article's first author and addressed a range of themes, including employment and working conditions (current and former), quality of life and self-perceptions of health (including both work injuries and illnesses), and other broad expressions of physical and mental health-related issues. We also targeted their coverage of basic needs and unpaid caring responsibilities. Interviews had an average duration of 100 min. The fieldwork was conducted between September 2014 and July 2015 in Santiago, the capital of Chile. We argue that the data we collected still demonstrates the reality of the Chilean labor market, given that its legal framework and structural characteristics have remained mostly unchanged.
Analysis
Interviews were analyzed following the constant comparative method 48 in a process of hierarchical coding using Atlas.ti version 7.5 software. The codes were constructed abductively based on flexible theoretically derived guidelines, allowing significant room for emerging codes. The coding process led to the identification of relevant dimensions and subdimensions of working and living conditions that were perceived to trigger health effects. Interviews were first coded and analyzed vertically, that is, taking the experience of each participant as a whole into account. Second, horizontal analyses were performed to identify the similarities and differences between the cases. In this way, we examined the particularities and shared realities of informal workers in contrast to formal workers, and their implications in terms of health and quality of life. While the accounts of formal workers were used as a reference for comparison, we drew mostly on excerpts from informal workers to illustrate the main findings.
Findings
The analysis of the interviews allowed us to identify a range of dimensions and subdimensions of living and working conditions that workers perceived affected their physical and mental health. Tables 2 and 3 present a summary of these perceived effects and indicate whether they were identified among formal or informal workers for the domains of living and working conditions respectively. Uncertainty and material scarcity are the two main dimensions of living conditions through which informality is experienced as affecting health. Psychosocial risks, a lack of safety measures, and extended availability and working times are the three dimensions of working conditions perceived to affect health.
Perceived Health Effects of Relevant Dimensions and Subdimensions of Living Conditions.
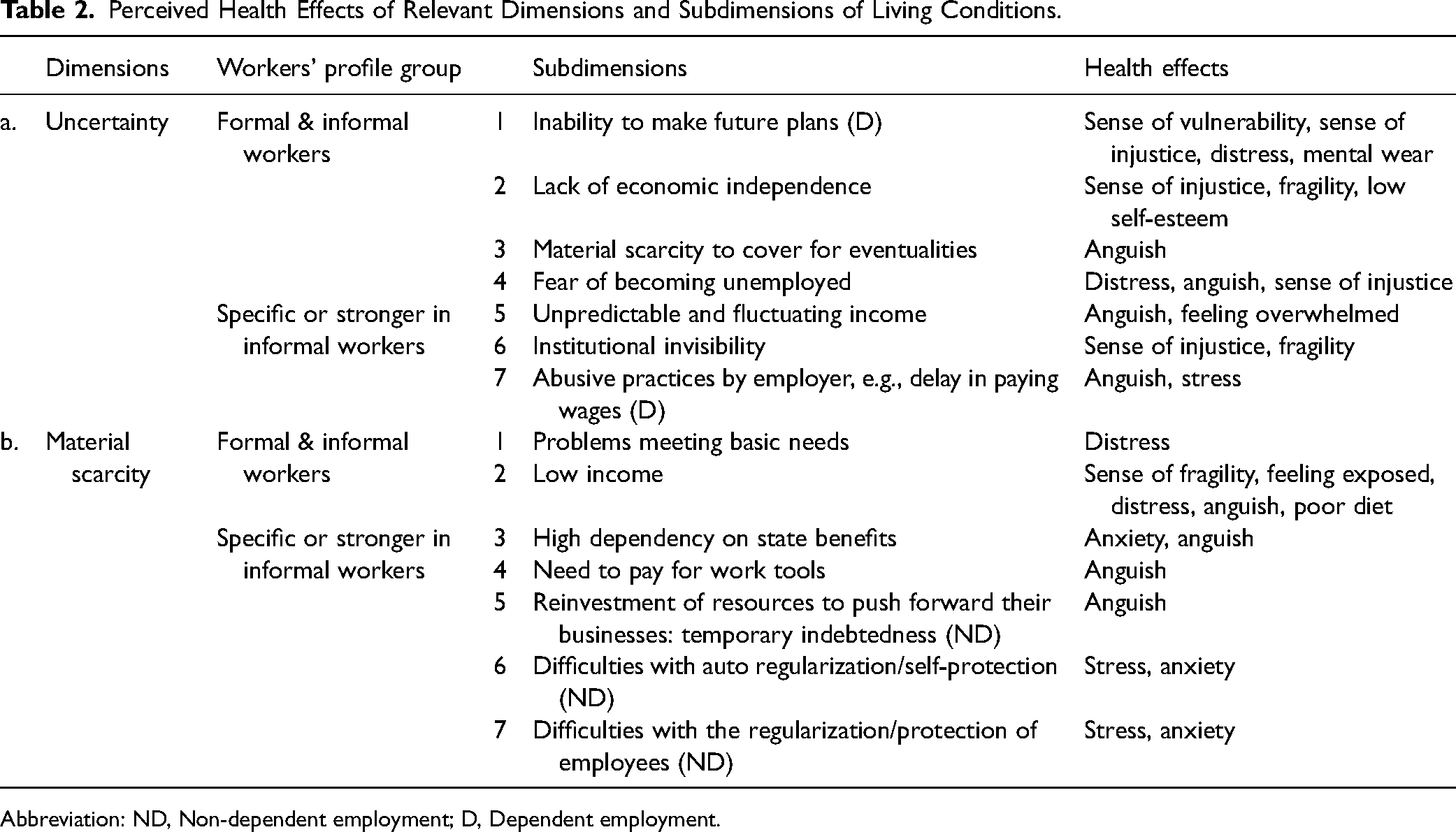
Abbreviation: ND, Non-dependent employment; D, Dependent employment.
Perceived Health Effects of Relevant Dimensions and Subdimensions of Working Conditions.
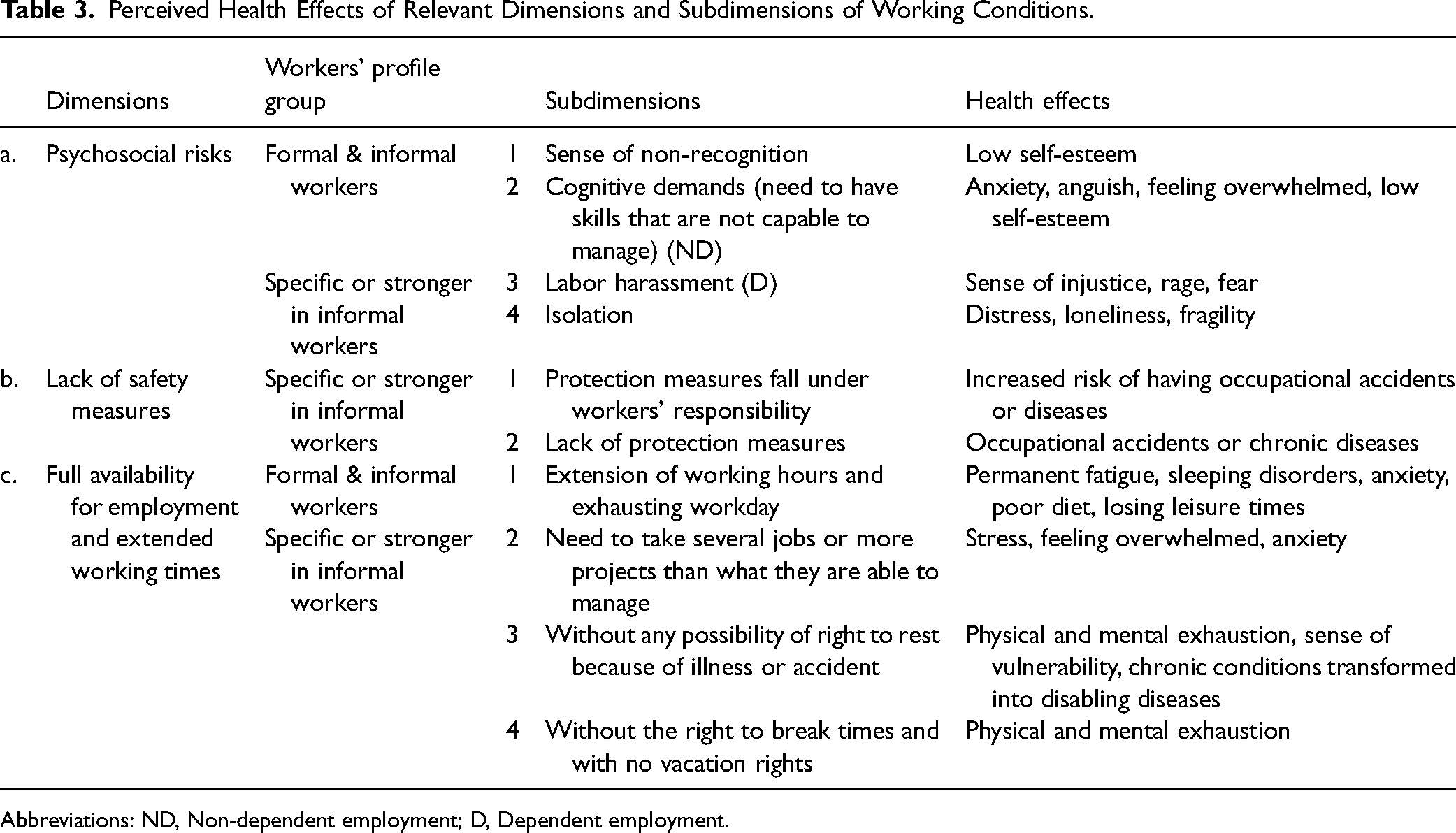
Abbreviations: ND, Non-dependent employment; D, Dependent employment.
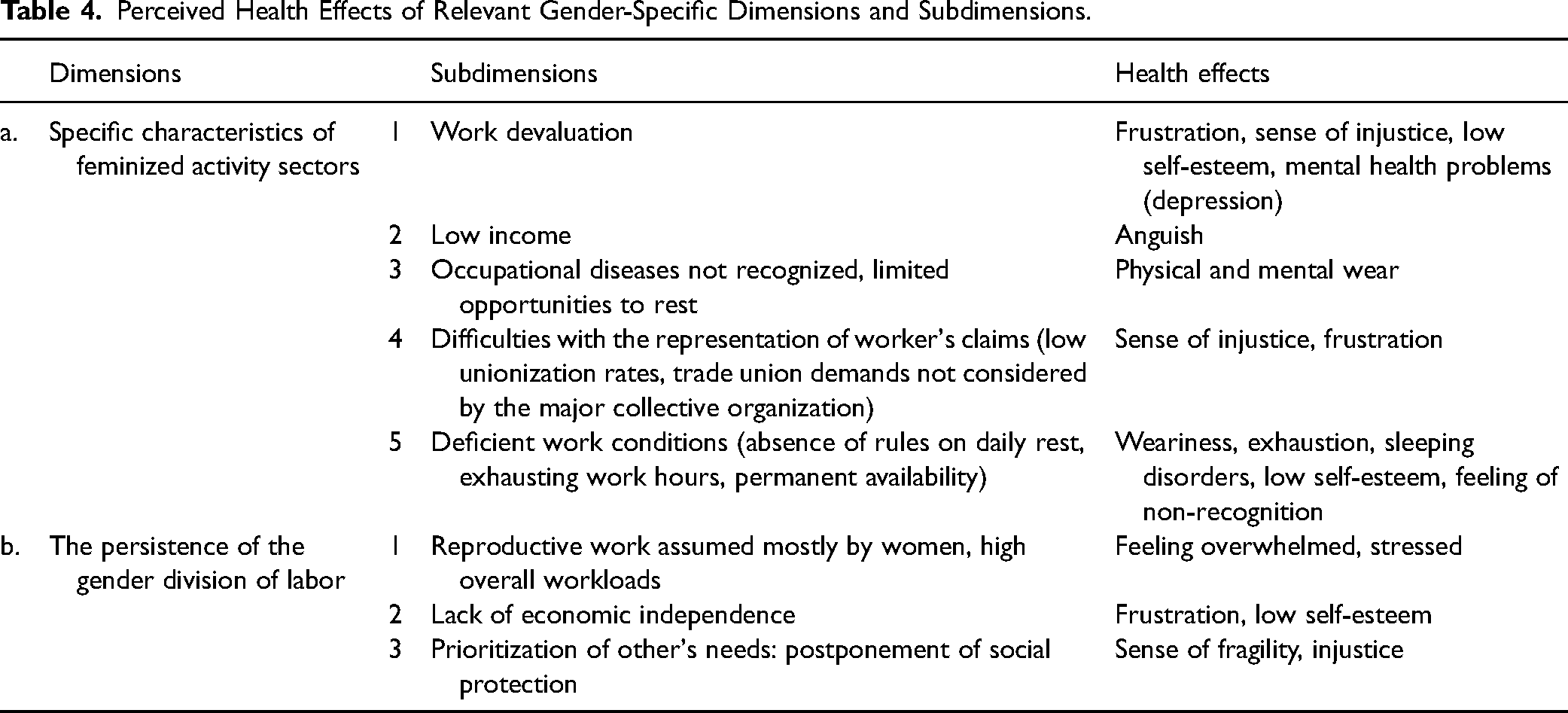
Some of the conditions and situations identified within each dimension are relevant to both formal and informal workers as a result of the often-precarious employment conditions of the former; others are specific or more applicable to informal workers, stemming from their lack of regulation and social protection. The commonality or specificity in the experience of the different factors has been systematically identified in Tables 2 and 3, while in Table 4 we focus on the commonalities found in feminized employment sectors. Such commonalities account for the lack of the protective effect of formal employment for women, which is explained in more detail in the corresponding sub-section of the findings.
Perceived Health Effects of Relevant Gender-Specific Dimensions and Subdimensions.
The findings apply to both dependent and non-dependent workers unless otherwise indicated. The detailed dimensions and subdimensions of working and living conditions that workers perceived that triggered negative health outcomes presented in the tables are identified in the article by the number of the table and the subdimension code (e.g., 2.a.6. for “institutional invisibility”).
Living Conditions: Uncertainty
The dimension of uncertainty comprises different processes related to a lack of stability, producing insecurity and difficulties for anticipating or planning for one's future—particularly common and intense among informal workers due to their lower wages and lack of employment regulations. Institutions have insufficiently addressed the needs of informal workers (2.a.6.), particularly the impossibility of their making future plans (2.a.1.). This leads to a strong sense of vulnerability and injustice, distress, and mental wear and tear. As one interviewee expressed it: Vulnerability—that's the word, feeling vulnerable. Developing short-term life strategies…you limit your possibilities of human development for that reason because you don’t know if you will continue working. Issues of projecting oneself, of having that possibility of planning in the long term, that's problematic when there is no work (4.a. male). They pay you on Wednesdays of the other week, they pay you on Monday, [they say] we have not been able, we’ll deposit it on Saturday, on Sunday. If we did not manage that money well, we would most likely always be without money on Friday…. They never pay us on Friday…everywhere we have worked it's the same story (7.a. female).
Even though the experience of uncertainty is common to formal and informal workers, informal workers do not receive benefits or monetary compensation when they are dismissed. This heightened uncertainty is related to distress, anguish, and a sense of injustice, resulting in a greater dependence on the employer. Family workers, in particular, suffer a lack of economic independence, especially when their pay is based on daily profits that are unpredictable and fluctuate (2.a.5.). This uncertainty forces them to maintain the bond with the family business, which leads to issues of self-esteem.
Living Conditions: Material Scarcity
This second dimension refers to scarcity in the most tangible ways, mainly associated with income. Both informal and precarious formal workers experience problems meeting basic needs from low incomes. However, dependent informal workers fall outside the scope of regulation that guarantees a minimum wage, which is one main factor that explains their low wages (2.b.2.). This situation leads to a state of vulnerability that is aggravated, as it often adds to other abuses from employers such as delays in paying or the failure to pay wages: Spending so much time working, from 10 a.m. until 9 p.m., almost 12 h, and barely seeing [getting paid] anything, practically nothing, or seeing very little, the minimum, but when I tell you that it is the minimum, it is the minimum…. It is useful to pay your bills, to go to the supermarket, buy something for the week, and that's it (7.a. female). They have always told me that when I retire, I won’t have anything…. Now I need to focus on myself and that implies contributing for my retirement, because if I don’t do it, I won’t have anything (8.a. female). I have a flea market and I have two months without any [income], and also that is strongly affected by the money I invest, or the portion of money that I have to reinvest remaining from previous projects…. I have vulnerability, that is, it's hard paying the money I need to pay for my daughter, I don’t have social security…. It has a great impact in the psychological aspect… always making bets, starting all over again, and that's very stressful, highly stressful. You have to reinvent yourself again and again (12.b. male). Those [employers] who are more nervous and anxious, the days of paying taxes, salary, or social security, have a nervous breakdown, because when you don’t meet all the resources needed.… They suffer, there are suicides, there are divorces, there are a thousand things (13.a. male).
Working Conditions: Psychosocial Risks
Psychosocial risks include physical and organizational isolation and situations of abuse at work, with a lack of measures to counteract them. Concerning this dimension, formal and informal workers share a sense of non-recognition (3.a.1.). In addition, non-dependent informal workers experience high cognitive demands (3.a.2.) when they are required to have certain competencies to develop a successful business, thus requiring certain self-management skills for which they are ill prepared. Consequently, they experience anxiety, anguish, a sense of being overwhelmed, and low self-esteem—problems that increase in the face of non-recognition resulting from the institutional invisibility associated with informality: The vast majority of entrepreneurs are obliged to, because they didn’t find other work, but they are not skilled enough to be good entrepreneurs.… The poverty is shared; they get little, but their workers also get little…. The whole system pushes them to cheat, to avoid taxes…. They don’t have training, they don’t have resources, they don’t have access to credit. They face only adverse situations (13.a. male). When I entered [the job], there were plant managers offering [workers] to continue with the work in exchange for being sexually intimate, and they did it several times. There were people so desperate to work that they did it (4.a. male). The treatment is different, unworthy, of the worker without a contract, eventual or occasional, as they call it…. Here you have first- and second-level workers, ones you [the employee] comply with, [are] up to date with their contributions, taxes, and contracts, the visible face of the company, the first folder; but you have another folder behind, where you have people in a deplorable situation (6.a. male).
Working Conditions: the Lack of Safety Measures
This dimension refers to the lack of an institutional framework guaranteeing the provision and enforcement of preventive safety measures. The situations and conditions related to this dimension are particularly acute among informal workers, as they suffer from the lack of an institutional or organizational structure to provide and enforce the use of prevention measures (3.b.1. and 3.b.2.). The responsibility for ensuring occupational health lies with the workers themselves, who do not have the training, resources, or tools to develop prevention and protection strategies. This enhances the risk of accidents and occupational disease, which may become chronic and eventually disabling: It's just a matter of them looking after themselves, because I have even gone to visit colleagues in sewing workshops where they are working at night and with almost no light (7.a. female)!
Working Conditions: Full Availability for Employment and Extended Working Times
This dimension relates to extended working times and the limited opportunities for rest. There are cases of both formal and informal workers who need to extend their working hours (3.c.1.), but informal workers especially lack control over their income or work volumes, and there is no institutional framework to serve as a back-up against instability and material deprivation. As a result, informal workers often work two jobs with no time to rest. Working at two jobs means working in parallel on two or more projects to ensure some income stability, which is often more than they can handle (3.c.2.). These workers are forced to be constantly available and in touch with both of their jobs, leading to exhausting workdays with scarcely any time for recovery and leisure. Both body and mind are over-exerted, and the worker is affected by a permanent state of fatigue. The consequences for their health include sleeping disorders, anxiety, and exposure to the effects of a bad or insufficient diet: Now [I work] approximately 50 h, but there were times when it was 70, 80 h, and even 100…. Very poor quality of life…. When I had a lot of jobs, I had medical leave because of stress, I got pretty sick. You get into a maelstrom…. I naturalized it, I thought I was capable of doing it, and it brought me consequences. In fact, I have a lot of health problems primarily due to stress. Depression, as well (4.a. male). My health is poor. It was good until recently, but old age already started, my bones hurt with the cold.… Since my 40s, I have never rested…. Basically, since I started in the flea market [of fruits and vegetables], I have not rested (12.a. female).
The Gendered Relationship Between Informality and Health
The findings show that gender affects the relationship between informality and health in two ways: the specificity of feminized activity sectors, and the persistence of gendered division of labor (see Table 4). The situations and processes described below affect the female working population as a whole, and not only informal workers. This finding could explain the lack of differences in health outcomes between formal and informal female workers observed by Ruiz and colleagues. 9
The first axis alludes to the fact that feminized activity sectors are particularly marked by precarious employment and working conditions, low social and economic value, the lack of recognition of occupational diseases, and specific problems for collective organization. The retail trade is a paradigmatic example of deficient working conditions crossing the frontiers of formality and informality. The lack of breaks, the heightened intensity of work, and the exposure to multiple sanitary and health risks (4.a.5.) generate a permanent state of fatigue and sleep disorders. Similarly, seasonal agrarian workers, whose employment opportunities are limited to a specific period of the year, tend to increase their working hours in the crop season. They work without rest and for prolonged periods of time, regardless of whether they have an employment contract or not: Women in the fruit [industry] are the most vulnerable—they do the most precarious jobs in this country, after domestic work, after the clothing industry…. Women [in the clothing industry] are in an extremely precarious job because, with their own infrastructure, in their house, they have to do the seams, the dressmaking for the [sewing] workshops. That is the most absolute precariousness because you don’t have any benefit, you don’t have anything to go to a doctor, or primary care, you have nothing…. The wages for agro-industry remain stalled. What happens is that there are women who are working a lot to get very low salaries…. [This] means working overtime, and overtime, from eight a.m. until one a.m. (1.a. female). In the textile area, all our fellow workers who are older than 60 continue working. And they don’t work until 65, they work until they cannot anymore…. We have fellows working in companies older than 76…. That's because retirement is very little, it's not enough for them to live (1.b. female). If I am already mistreated psychologically and they tell me that I’m crazy, it's striking. That's where the girls fall down, they sink, here [the domestic workers’ association guesthouse]. Girls arrive very wounded psychologically…. Because of the psychological abuse of the employers, and of the children, who are sometimes more cruel…. Many girls suffer from depression for that reason (3.a. female).
Women also encounter more difficulties in articulating their demands in terms of trade union representation (4.a.4.). They report problems in situating their demands within the trade unions’ agenda: Many times, you asked to speak and they didn’t want you to because you were a woman, until I understood that nobody listens to someone who doesn’t shout. So, I learned to bang on the table, I learned to impose myself…. In the union world, you have to be three times better than men to achieve something…. I have felt a lot of discrimination (1.b. female). I have a colleague, she starts working at 9 a.m. and ends at around 5 a.m., can you believe? She goes to bed around 5:30 and gets up around 8 a.m., sleeps very little…. She works during the day, does things [domestic work], and at night she works [as a seamstress] and sleeps four, three hours, two hours (7.a. female).
Other Sources of Inequality
Analysis of the interviews also revealed other factors that intervene in how informality affects health, either by protecting or over-exposing workers to negative health outcomes. Among these, it is important to highlight the following: (a) self-care awareness, that is, awareness and knowledge about how to prevent possible ailments and illnesses resulting from one's job, or how to take care of oneself in the event of illness, which is often related to having a high educational level or specific training; (b) resources derived from personal relations, that is, possessing a social network facilitating access to employment opportunities and social and community support; (c) the composition and protective capacity of the household—for instance, being able to access a family health plan; and (d) property ownership, which may provide endorsement in given situations, such as when applying for a bank loan. Each of these elements relates to the worker's social position more generally, reflecting how social inequalities manifest themselves in health inequalities and, more specifically, how they intervene in the relationship between informality and health.
Discussion
In this article, we identified the processes whereby informality leads to negative effects on workers’ health and well-being in Chile by comparing the situations of formal and informal workers. The results showed that the situation of informality results in exposure to hazards, which are associated with five crucial dimensions of informal workers’ poor living and working conditions: uncertainty, material scarcity, psychosocial risks, full availability for employment and extended working times, and lack of safety measures at work. Such exposure has consequences for both mental and physical health, ranging from physical exhaustion to feelings of anguish, stress, frustration, and low self-esteem. We created Figure 1 to synthesize the model we put forward and to visualize the perceived links between informal employment and health inequalities.
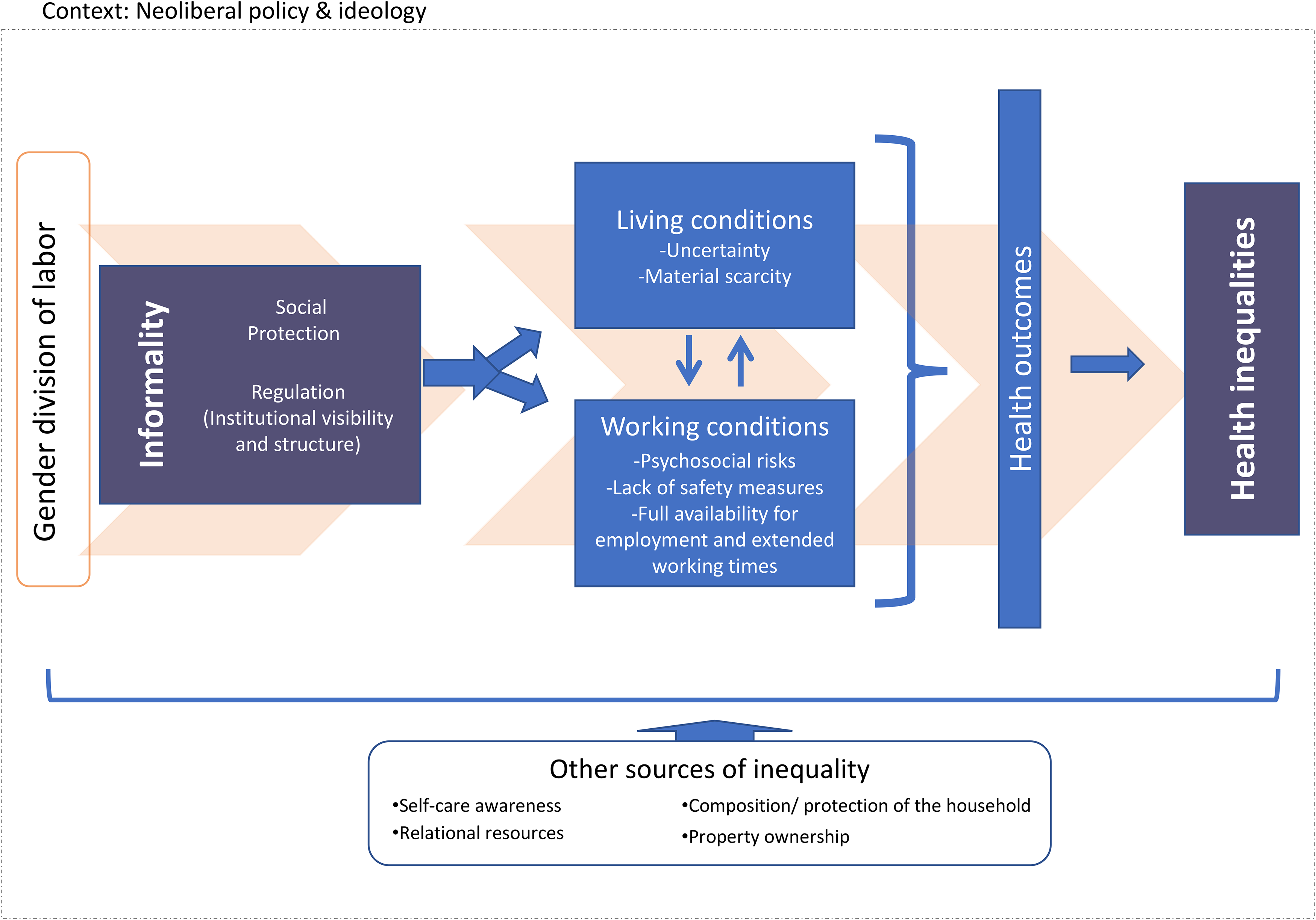
Synthesis of analytical concepts and findings.
Our results are in line with previous research showing the health-damaging effects of the different forms of insecurity experienced by non-standard workers. 50 Furthermore, our research develops a comprehensive and exhaustive view of the implications of poor employment conditions on specific domains of both living and working conditions. Our research results also go beyond the identification of risk factors in the working conditions of particular jobs (such as street vendors or waste pickers; see, for instance, 54) to focus on the common and broader implications of the core elements of the informal employment relationship, namely the lack of regulation and social protection.
However, beyond the observed commonalities derived from such features of informality, certain groups of workers with specific situations of informality are exposed to distinctive threats with differential effects on health. Informal dependent workers (salaried workers and homeworkers without contracts or with fee contracts, or domestic workers without contracts and family workers) are particularly exposed to employers’ abuses of power, which causes anguish and stress. For informal non-dependent workers (employers with fewer than five workers and non-professional self-employed workers), the need to reinvest resources and subsequent temporary indebtedness generates anguish. In turn, major sources of stress for informal employers are the difficulties in regularizing their situations and those of their employees.
On a more interpretative level, these experiences can be understood against the backdrop of underlying structural factors closely related to neoliberalism—which, in Link and Phelan's terms, 51 could be considered fundamental social causes of disease that modulate people's exposure to risk factors. First, among dependent informal workers, the informal employment relationship magnifies the power imbalance that characterizes the employer-employee relationship due to the lack of any protective legal structure to rely on and their specific difficulties in terms of collective organization and representation rights. 52 Second, workers remain increasingly exposed to risk in the absence of social policies articulated to counteract the increased pressures of the market. 53
The experience of informal non-dependent workers is marked by their situation of apparent freedom, one where the workers are often unprepared to operate within a competitive marketplace. 52 As a result, they are constantly threatened by poverty, 54 and socially are held responsible for their own failure or success 38 according to a narrative of opportunity and freedom underlying the presentation of autonomous informal workers as microentrepreneurs. 30 These conditions force non-dependent informal workers into situations of apparently self-imposed heightened workloads, which triggers a lack of time and of opportunity to rest. In this way, the article illustrates empirically the health effects of what have previously been theorized as systemic pressures to achieve and produce self-exploitation. 55
The empirical findings also suggested possible explanations for the lack of a protective effect of employment formality on women's health, as identified by Ruiz and colleagues. 9 These explanations refer to two types of dynamics: (a) the special incidence of precarious working conditions, low wages, and a lack of social protection among feminized activity sectors; and (b) the persistence of the gender division of labor. These situations, which affect the female working population as a whole and not only informal employees, could account for the generally poorer health conditions of working women relative to men and for the lack of differences between informal and formal female workers observed in quantitative studies. These findings are consistent with research in other countries suggesting that gender inequalities in health are rooted in wider processes of gender inequality, reflecting differential employment and working conditions, unequal earnings, and the burden of unpaid work falling on women.26,49
The blurring of the boundaries between formal and informal employment may not only be relevant among the female population, but also may be occurring because of neoliberal reforms promoting deregulation, flexibilization, and the resulting destabilization of labor markets. 30 In this sense, despite the particularly disadvantageous situation of informal workers, some of the harmful aspects of informality are not unique features of the informal employment relationship but may rather reflect the characteristics of the position these workers occupy within a secondary or peripheral segment of the labor market.10 The situation of women illustrates this point paradigmatically, with gender segregation leading to particularly poor employment and poor working conditions in female-dominated sectors, which adds to the higher overall workloads resulting from the unequal division of reproductive labor. Such factors would seem to hinder the protective effect of formality on physical and mental health.
Strengths and Limitations
Our study not only developed a comprehensive and systematic understanding of how workers perceived the relationship between informality and health across the different dimensions of living and working conditions, it also did so in the context of the Global South, which has been historically understudied. However, it has limitations that should be considered and be addressed in further research. Concerning the temporal relevance of the article, it must be noted that the lack of regulation and social protection is likely to have had specific detrimental health outcomes during the economic, social and health crisis triggered by the COVID-19 pandemic. While this study does not capture such developments, it provides an interpretative framework for understanding potential changes.
Other limitations concern the sample composition, namely its under-representation of the challenging-to-reach migrant population. Further research should delve into the specifics of informal migrant workers to identify how their informal employment position intersects with other inequalities derived from their non-legal residential status, racial discrimination, and limited support networks in producing damaging health outcomes. It is also necessary to deepen the knowledge of the differences among sub-types of informal workers (family workers, homeworkers, etc.), including how they benefit or are excluded from specific social policy resources and programs, and how this is perceived to affect workers’ health and well-being. Finally, incorporating the views and strategies of employers and other actors of the system could also be helpful in designing fine-tuned policies oriented toward the reduction of informal employment in the Chilean context.
Policy Implications
As a whole, this study sheds light on a problematic issue for public health and highlights the need to develop public policies supporting forms of employment that are more sustainable for the health and quality of life of workers. In the face of the empirical evidence showing the negative repercussions of informality on health, public policy should aim to guarantee the formalization of dependent workers by, among other possible measures, promoting inspection and control systems, increasing the incentives to employers, and abolishing fee contracts for public servants. Moreover, continued training for non-dependent workers should be implemented by public offices. In addition, by identifying intermediate steps in the process by which informal employment produces poor health, the results of the article enable the identification of possible points of intervention. These points include guaranteeing minimum or basic income to reduce income uncertainty and reinforcing occupational health and safety preventive culture and enforcement systems. The lack of protection for formal employment for women shows the relevance of establishing a gender-mainstreaming agenda that permeates every single policy, most importantly in the domains of employment and caregiving. Adopting a “health in all policies” approach that regulates and ensures living wages and universal social protection plans—alongside specific institutional support for the most disadvantaged groups of workers—can be crucial in mitigating the health inequalities that result from situations of informality.
Footnotes
Acknowledgments
This study was supported by a grant from the Comisión Nacional de Investigación Científica y Tecnológica de Chile, as part of Marisol E. Ruiz's doctoral thesis. The authors would like to thank Joan Beach and Alejandra Vives for their guidance and support of the research project from which this article stems, as well as the Research Group on Health Inequalities, Environment—Employment Conditions Network at Pompeu Fabra University for providing equipment and office space. The authors also are very grateful for the people who were interviewed in this study for sharing with us their time and life experiences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Agencia Nacional de Investigación y Desarrollo (former Comisión Nacional de Investigación Científica y Tecnológica de Chile), Beca Chile (folio 72130263); PRESSED project (CSO2017-89719-R, AEI/FEDER, UE); and Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (grant number 51NF40-185901).