
Abstract
The availability and accessibility of sexual and reproductive health (SRH) services for transgender individuals are crucial. This population is deprived of health care due to rejection, stigma, gender-based discrimination, confidentiality, and violence. This review attempts to provide readers with an account of the fundamental problems that the transgender population faces regarding experiences of SRH. This meta-synthesis review applied the Social–Ecological Model (SEM) to address trans individuals’ SRH factors. The databases were searched using “SRH” and “transgender” keywords. Fifty studies were finally selected. All studies were qualitative, including 36 semi-structured/ in-depth interviews, two focus group studies, and 12 interviews and focus group studies. The Social–Ecological Model application illustrates the impact of individual, interpersonal, institutional, and social factors on the condition of SRH among transgender individuals. This meta-synthesis reinforces multiple levels of factors that influence the SRH of transgender individuals. These include limited information, lack of awareness, low socioeconomic status, stigma and discrimination, and social deprivation. Interventions are urgently needed to provide better sexual and reproductive well-being for transgender individuals.
Sexual and reproductive health (SRH) is essential for general health and well-being. According to the World Health Organisation, SRH rights are essential to emphasize the needs of populations who may neither be aware of their right to health nor be able to access the services they need. 1 Accessing SRH care is a sensitive process for many individuals.
One of the most vulnerable populations is transgender people. Transgender individuals experience their gender identity as different from the sex they were assigned at birth. 2 According to the American Psychiatric Association, the term “transgender individuals” refers to “the broad spectrum of individuals who transiently or persistently identify with a gender different” from their sex assigned at birth. 2 Transgender patients have a variety of SRH needs. In particular, this population experiences pronounced barriers to SRH and rights due to bias, stigma, and discrimination within political, economic, social, education, and health care structures and institutions. Transgender people have delayed or avoided preventive health care and gender-affirming services out of fear of discrimination or disrespect.3,4 Numerous studies have addressed the factors correlated with perceived barriers to accessing SRH services. For example, individual variables, such as age, knowledge, and attitude, can be predictive of poor access to SRH facilities.5–7 Other variables, such as insecure family relations, poor health care provider and client interactions,8–10 and lower socioeconomic status, have been associated with poorer levels of access to SRH facilities. 5 Clearly, a comprehensive understanding of difficulties and their interactions with the surrounding environment requires an investigation of related factors. 11
Qualitative data on the barriers and facilitators to accessing sexual and reproductive services of transgender individuals is limited, especially among the adult population. 11 This systematic review is based on the Social–Ecological Model (SEM), which recognizes the intertwined relationship existing between an individual and their environment. By using the SEM as an analytical lens, this systematic review explores the barriers and facilitators to accessing SRH services at the individual, interpersonal, institutional, and societal levels. Although there is a growing body of research and an increasing number of studies using qualitative methods, there has been no synthesis across that body of research to explore the implications of SRH and related factors in trans populations. This systematic review aimed to aggregate, interpret, and synthesise findings from qualitative studies about accessibility barriers and facilitators to SRH care among transgender individuals.
Methods
Search Strategy
The PubMed, Scopus, Medline, Web of Science, and ScienceDirect databases were searched from January 2005 to February 2021 for papers published in English using the following search terms: “sexual health” or “sexual risk” or “reproductive health” or “SRH” AND “transgender” or “transsexual.” References of the included studies were reviewed manually. The selection process of the studies is represented in Figure 1.
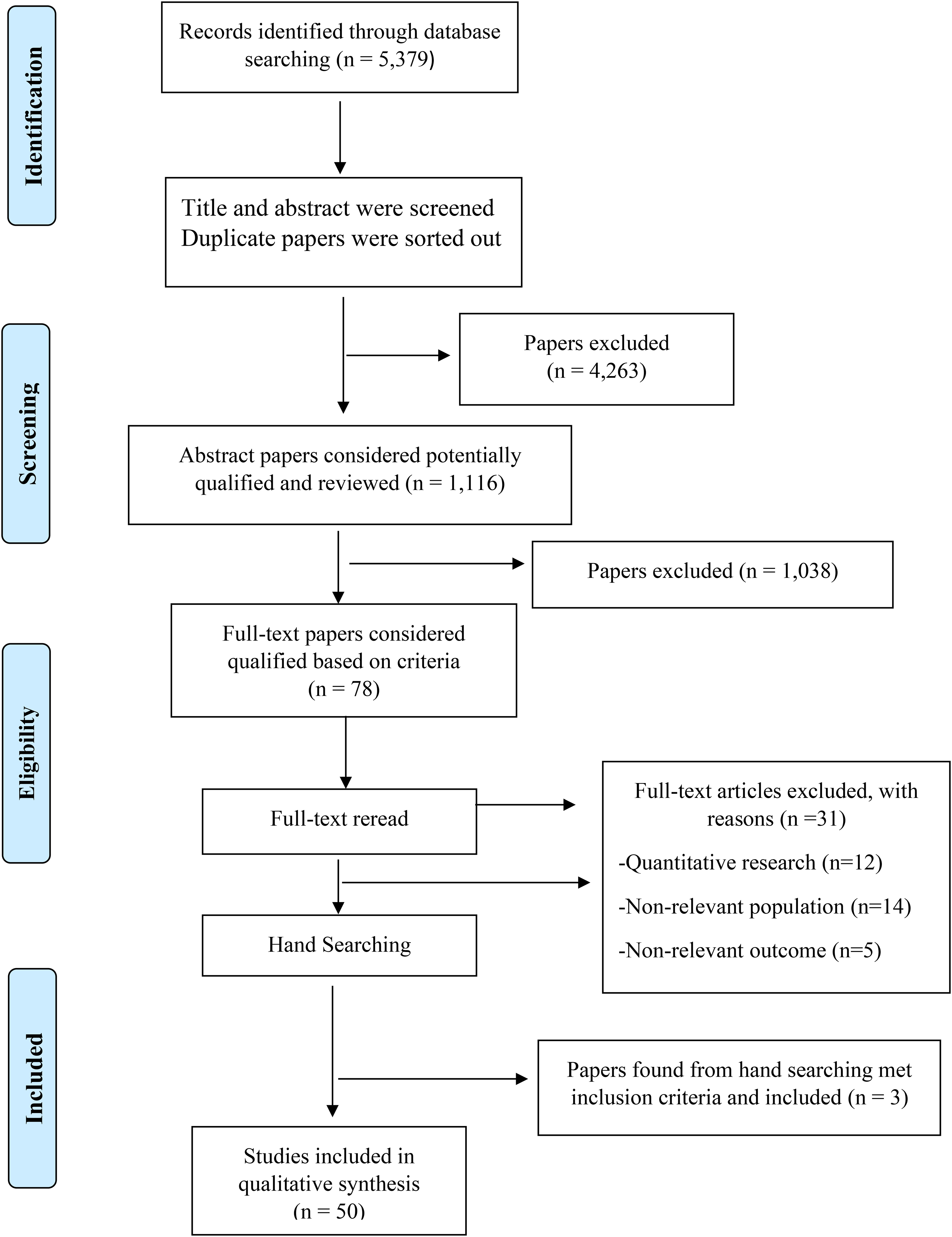
Flowchart of study selection.
Inclusion and Exclusion Criteria
The inclusion criteria for the literature were as follows: (a) qualitative articles, (b) the publication language was English, (c) a focus on the barriers and facilitators to accessing SRH care among transgender individuals in health care practices, or (d) a focus on the perspectives of health professionals working with trans individuals, and (e) availability of the full-text article.
Articles that were excluded: (a) focused on a specific medical condition (e.g., gender-affirmation surgery, assisted reproductive technology, or vaccination), (b) focused on a health difficulty (e.g., tobacco or substance use), or (c) were conference abstracts, editorials, and reviews. A flowchart of the study is presented in Figure 1. A total of 5,379 studies were retrieved from PubMed, Scopus, Medline, Web of Science, and ScienceDirect databases. After 4,263 duplicates were removed, 1,116 reports were screened for the titles and abstracts. From this screening, 1,038 citations irrelevant to the research topic were excluded. Based on the 78 remaining studies’ full-text reviews, 31 articles were excluded, including 12 studies involving quantitative research, 14 studies conducted in non-relevant populations that were not representative samples, and five articles with non-relevant outcomes. Hence, three more papers were found from a hand search that met inclusion criteria and was included in the review. Finally, 50 papers met the inclusion criteria, as summarised in Supplementary Table 1. The articles reviewed, published between 2005 and 2021, are characterised in Supplementary Table 2. All 50 studies were qualitative, including 36 (72%) semi-structured studies/in-depth interviews, two (4%) focus group studies, and 12 (24%) studies that were both interview and focus group. The majority of the studies were conducted in the United States (36; 72%), with two (4%) conducted in Asia, two (4%) conducted in Africa, seven (14%) conducted in Europe, and three (6%) conducted in Oceania. Regarding gender, seven studies (14%) included both transgender men and women, 10 (20%) included only transgender women, six (12%) included only transgender men, five (10%) included health care providers, five (10%) included both health care providers and transgender individuals, 16 (32%) studies included transgender individuals and other people on the sexual and gender minorities spectrum, and one (2%) included parents.
Quality Assessment
The Critical Appraisal Skills Program (CASP) tool was used to appraise the 50 identified studies. 12 This tool was used because it is a method that systematically explores issues of rigor, credibility, and relevance of qualitative studies. 13 Initially, the authors (M.S. & Z.M.) appraised the studies independently. The authors adopted a three-point rating system developed by Duggleby and colleagues (2010) to determine quality scores. According to Duggleby and colleagues’ rating system, a study is rated using a score from 1 to 3 for eight-core questions. Thus, each article's quality scores can range from 8 to 24, based on Duggleby's rating system. “Weak” articles scored between 8 and 15, “moderate” between 16 and 23, and “strong” 24 (see Supplementary Table 3). After independently reviewing the 50 studies and discussing and comparing the results, there was a high rate of agreement in scores across the two authors. Several minor discrepancies in scores were resolved through discussion until a consensus was reached. The assessment of the quality of the studies demonstrated that all the studies were categorised as “moderate” to “strong” quality based on the scores assigned by the authors. The highest score was 23, and the lowest score was 18 out of a possible 24.
Analysis and Synthesis
Authors extracted, aggregated, interpreted, and synthesised findings from the included studies. This review was guided by the meta-ethnography method of Noblit and Hare (1988). Meta-ethnography is an inductive, interpretative process that involves integrating and synthesising across studies, resulting in novel interpretations and conceptual insights. 14 Following the proposed stages of meta-ethnography, the individual articles were read and reread. For each article, the themes relevant to the review's aims were recorded in a table, along with supporting original data. 14 Comparing and contrasting each study enabled clearer insight into the common and recurring concepts found across the research papers and the similarities and differences occurring within them. The final step in the analysis involved synthesizing the second-order translations to identify third-order constructs and present how the studies were related. Clear themes emerged that focused on different aspects of transgender individuals’ access to sexual and reproductive services. These findings brought together all 50 studies to construct an overarching understanding of the experiences of this population.
Results
Applying the Social Ecological Model for Transgender Individuals
The application of the SEM illustrates the complex relationships between society and the behaviour of transgender individuals, highlighting the effects on their SRH.
15
Some unique behaviors such as health seeking, which have a complex interaction with the environment, sometimes are not appropriate ascribed to an individual's behavior and may be ascribed to a new system. This review shows that factors influencing the health-seeking behaviors of transgender individuals can be categorized under the SEM. The SEM addresses the complexities and interdependences between socioeconomic, cultural, political, environmental, organizational, psychological, and biological determinants of behavior.
16
SEM is a well-established conceptual framework in public health that acknowledges the critical individual, interpersonal, institutional, and social factors. SEM also evaluates the impacts of such factors on risk assessment and usage of SRH services.
17
Therefore, it is hard to understand the difficulties of transgender individuals’ health without considering their environment. Poor SRH knowledge and practices among transgender people are a complex matter affected by personal, community, cultural, and regulatory factors. All these factors overlap and are affected by each other. Therefore, it is challenging to understand individuals’ reactions in the face of these complexities.
18
Based on this concept and the overview of primary studies, a unified system consisting of four levels (individual, interpersonal, institutional, and society) was developed. Each level illustrates the factors affecting transgender individuals’ SRH (Figure 2). These include:
Individual level: individual characteristics including those influencing behavior, such as knowledge, attitudes, skills, and beliefs Interpersonal level: the interpersonal interaction between the individual and their partner, friends, family, and health providers Institutional level: the organizational system covers the providers’ knowledge, discrimination, stigma, and social support Social level: the structural macro-system, which includes rules, policies, norms, and values
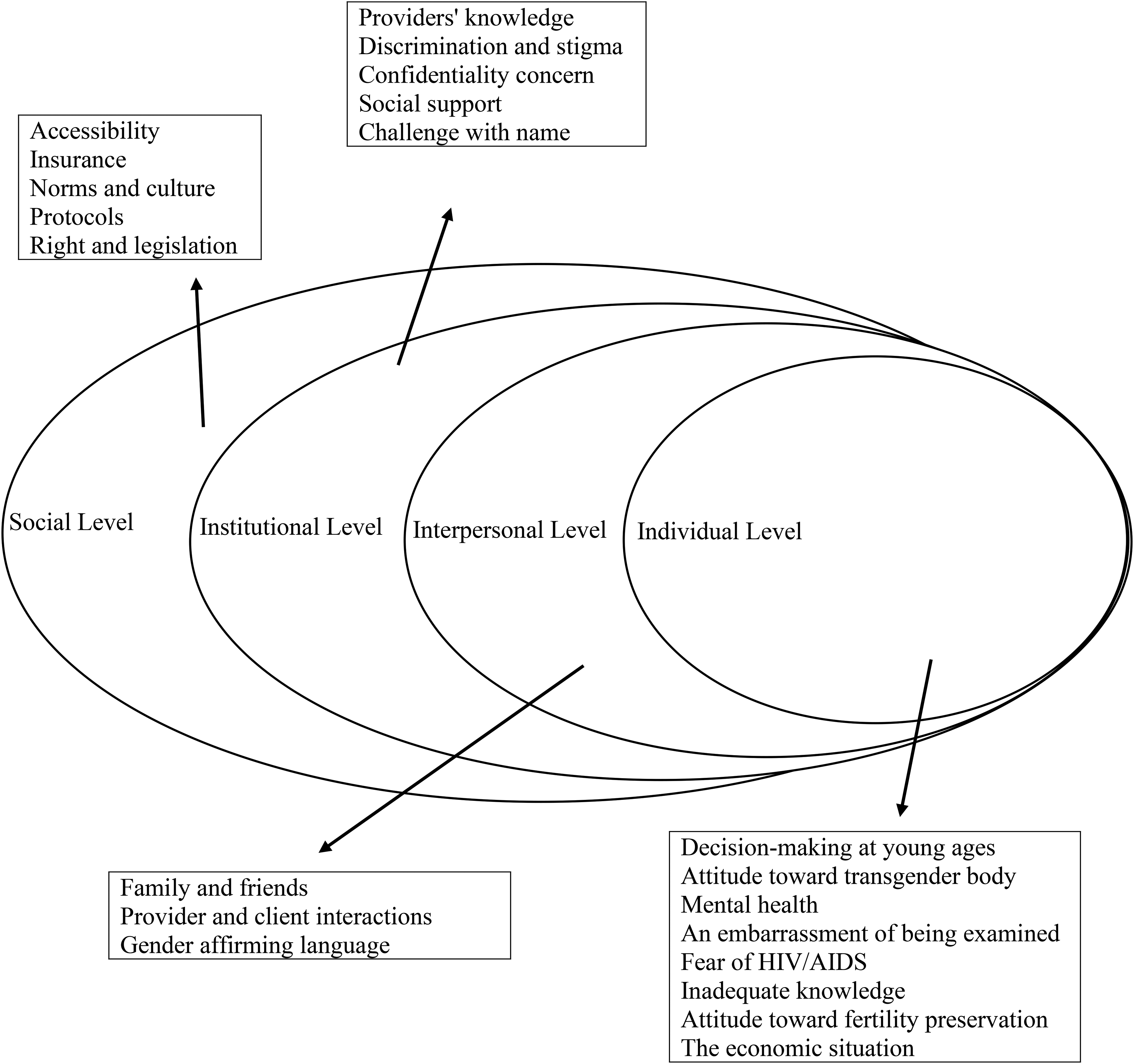
Ecological framework guiding the analysis of the barriers to the SRH of transgender individuals. Source: adapted from the centers for disease control and prevention (CDC), The social-ecological model, https://www.cdc.gov/nccdphp/dnpao/state-local-programs/ health-equity/framing-the-issue.html. (Retrieved December 13, 2016).
The SEM is applied in this meta-synthesis to offer a holistic understanding of the health-seeking behaviors of transgender individuals and their access to SRH care services.
Individual Level
Numerous factors form an individual's life. However, based on the present review, certain factors have been identified as significantly influencing SRH. Examples include decision-making at young ages, attitudes toward the transgender body, mental health, embarrassment of being examined, fear of HIV/AIDS, knowledge, attitude toward fertility perseveration, and economic situation.
Decision-Making at Young Ages
Five studies show that trans youth may be less likely to seek help from SRH services or follow providers’ advice if they feel their identity is disconfirmed or ignored by health care providers.6,19 Different children of the same age may have different maturity levels, and this issue affects their decision-making about using SRH services. No universal agreement exists as to when children reach decision-making competence. In the medical practice, it is not clear-cut whether a minor of a certain age is sufficiently competent for medical decision-making. 20 “I thought I knew everything at 14, do you know what I mean? But a decision like that is a huge decision” ( 6 , p. 7). It seems that the lack of adequate competence has a significant impact on their future fertility power and related matters. 19 Furthermore, some transgender individuals are too young to perceive some medical issues. 6
Attitude Toward Transgender Body
Reasons for low use of health services by this population may include misconceptions and conflicting perceptions of sexual organs and reproductive issues before and after transition. Both individuals and health providers may also be uncertain about the appearance of transgender bodies. One health care provider stated, “When it's clearly people who’ve made the journey, and so everything matches up if you like, that's fine. But it's when people are crossing over in between. You know, do they have a penis or not?” ( 6 , p. 5; 5 ; 7 ; 21 ). Many individuals described the challenge of talking about their bodies, especially with cisgender intimate partners. 21
Mental Health
Ten studies revealed that depression, alcohol consumption, and suicidal thoughts in transgender individuals on the one hand and misunderstandings of gender identity as an unstable mental state in health care providers, on the other hand, prevent transgender people from going to health care services.6,7,22,23 For example, one health care provider stated, “I think the DSM diagnostic manual for psychological therapy etcetera still regards trans . . . as a potential mental health issue.” Also, providers labelled transgender individuals “distressed, withdrawn, unhappy, and depressed” ( 6 , p. 6).
An Embarrassment of Being Examined
Some transgender individuals are embarrassed to be read by a doctor and consider the examination an unpleasant situation that causes them to feel distressed and disrespectful to themselves and their bodies, sometimes to a sense of torture.22–24 One participant said, “any kind of gynecological examination was problematic: Going to a doctor and saying it, then opening and showing your vagina is a degree of torture” ( 22 , p. 5). The examination rooms without appropriate brochures and additional information cause them to feel uncomfortable.9,20 Additionally, some doctors tend to examine transgender patients out of curiosity. These issues prevent creating an intimate atmosphere between the client and the provider and a reluctance to discuss the desired topics. 25
Fear of HIV/AIDS
Eleven studies revealed that the most critical obstacles preventing presence in health clinics are the fear of a positive HIV/AIDS test,24,26 misconception about HIV/AIDS and sexually transmitted infection (STI), 27 low perceived susceptibility to HIV/AIDS and STI, and anxiety about HIV/AIDS acquisition.20,28,29 Trans people are not biologically different from cisgender people, so it is better to understand the risk of HPV and other sexually transmitted diseases (STDs) and get the relevant tests. 30 HIV acquisition is high in the trans population, particularly in trans female, and this risk is exacerbated in racial/ethnic minorities.3,8,20
Inadequate Knowledge
Thirteen studies reported that transgender individuals described a lack of awareness about SRH as a reason why they didn’t access services. There was a perception that services were only for cisgender individuals and not available to trans individuals.9,20–22,27 Inadequate knowledge about STI due to diverse sexual relationships, not using condoms regularly, and inadequate skills in using condoms during an unprotected sexual relationship were the major reasons for not using SRH services.31–35 For example, “how to open a condom package and unroll a condom” ( 20 , p. 837).
Attitude Toward Fertility Preservation
There is limited research on the fertility status and experiences of trans people who use transition services.36,37 Youth trans individuals are concerned about the effects of gender-affirming hormones or surgery on their fertility and biological children's ability .38,39 Trans individuals have varying preferences about having children; some prefer being a biological parent, others prefer adopting children, and some have no interest in having children. 40 One participant said, “I’ve always wanted kids” ( 41 , p. 109). At the same time, another preferred to “save one of the kids from orphanages and give them a chance”. 36 Meanwhile, some parents may support their child's reproductive wishes or insist on preserving their child's fertility. 38 Also, transgender individuals may face family formation barriers. One participant said, “My partner and I have discussed and are unsure about having children in the future. We both have concerns about the implications of pregnancy that go with our gender identities” ( 36 , p. 4).
The Economic Situation
Seven studies reported that financial difficulties are one of the most significant obstacles to going to health centres.42,43 Having a secure job and financial security can reduce the risk of HIV/AIDS and other STDs.42,44 Low-income individuals, especially trans women, are more prone to prostitution and high-risk STDs.26,42,44 On the other hand, being excluded from family translates into a loss of financial support, forcing individuals to sell their bodies and resort to survival sex.42,45 Because of their identity, trans people have difficulty getting a home and a steady job. On some occasions, trans individuals lose their jobs after revealing their transgender identity and are forced into prostitution and exposed to sexual assault and violence due to financial needs.5,27,46
Interpersonal Level
The quality of interpersonal relationships has significant and long-term effects on individual decision of using health care services. The SEM's interpersonal interaction includes the trans relational variable, such as parents, intimate partners, peers, and health providers’ communication.
Family and Friends
Eleven studies described parents’ communication methods with their children and discussions involving SRH issues are some of the most important predictors of the individuals’ engagement with using health care services.7,9,20–22,25,29,31,45,47,48 One participant shared, “I see and affirm that this is who you are and am grateful that we have this level of trust that you’re sharing this information with me. I am happy that you feel free to live life as your truest self. Please tell me more about your identity so I can understand it better. I’m gonna do some research as well so we can have more transparent, better conversations about this. And most importantly, I love you” ( 8 , p. 8). Informed parents have a significant role in their child's decisions about their future fertility plan 19 and can help their children in the transition period.8,20,48 Furthermore, fear of family rejection and stigma created barriers for trans individuals in seeking services.9,20,22,28,29
Provider and Client Interactions
Almost all studies reported lack of proper communication between the health care provider and the trans person as one of the reasons why trans individuals avoid going to medical staff.5,28,44,47,49 Transgender individuals are not fully understood by the providers and find the environment judgmental and unpleasant, and also the interaction with the doctors is not based on honesty and transparency.8,9,32,45 Furthermore, they examine out of curiosity to explore the trans person's body.23,25,33 This unfriendly behavior is exacerbated especially when the trans person wants to receive treatment for STDs.27,44 On the other hand, the lack of a safe and trans-friendly environment, mistreatment, disrespect, harassment, humiliation, ignoring of trans people, use of insulting literature, and inappropriate treatment by providers prevent trans people from going to health care centers.5,23,24,33,42 Such behaviors prevent a sincere relationship with the staff, and eventually, the trans person becomes alienated and does not express their main problem and particular health need.23,39,50,51
Gender-Affirming Language
Two studies identified that the use of inclusive and precise language is considered when health care providers try to ask questions about the SRH of trans individuals.9,28 One participant said, “I ask my clients to define what parts [genitalia] are used [in sex acts] and how. I do not define it [sex] for them” ( 9 , p. 5). The care environment is more welcoming for trans individuals if health care providers use words that describe the body instead of using anatomical language. Not using gender-affirming literature by the physician due to the lack of knowledge of trans people in the medical literature fails to provide optimised care.5,9,25
Institutional Level
In the SEM, the providers’ knowledge, discrimination, stigmatised setting, confidentiality concerns, social support, and challenge with name- and gender-affirming services constitute the institutional level.
Providers’ Knowledge
One of the most critical factors in how the institutional level impacts the health system is health care providers’ knowledge. Almost all studies point to a lack of general and particular information in the developing field of SRH.5,6,9,19,21,27,34,52 Health care providers’ knowledge is not following recent medical world science and is outdated.35,44,53 The consultation methods are inadequate and unprofessional. 5 Some structural hurdles can be summarized as a lack of knowledge about fertility preservation 38 and the results of reproductive storage, a lack of knowledgeable and supportive staff with sufficient experience, and shortage of competent physicians to meet the special needs of transgender individuals.8,19,28,35,44 Preoperative and postoperative adaptation information is inferior. 23 Additionally, health care providers’ information is irrelevant or inconsistent with gender-affirmative needs.35,54 Moreover, informed health care providers have a significant role in trans individuals’ decisions about their fertility preservation. Health care providers have an encouraging or discouraging role in using health care services. 38 One participant said, “The medical staff helped provide specific advice about the process, e.g., how much sperm to store for future IUI/IVF procedures” ( 55 , p. 10).
Discrimination and Stigma
Every study reported various forms of discrimination, stigmatisation, and poor usage of SRH services.23,27,28,34 This occurs even in societies with progressive human rights policies. 33 High levels of stigma and discrimination, lack or poor quality of services and care in the public sector, and fear of discrimination prevent trans people from going to health service centers.5,24 Discrimination can be exacerbated in trans people of colour, particularly in trans women of color who are marginalised and experience high rates of violence and exclusion. 46 One participant stated, “Race, ethnicities, socioeconomic status, immigrant status—You have all of the different types of discrimination that are associated with those identities that would kind of compound and intersect with discrimination based on gender identity and gender expression in various ways, to hinder people's access to the care they need” ( 5 , p. 8). One of these studies demonstrated that health care providers consider a person's race and ethnicity in addition to gender identity. 5 Four studies reported transgender females with higher exposure to stigma and discrimination were more likely to engage in HIV risk acquisition than their peers.9,42,44,45
Confidentiality Concern
Five studies reported that lack of confidentiality from health care providers emerges as an important barrier to accessing SRH services.9,20,24,25,49,53 Studies have shown how confidentiality violations can create a barrier to testing and prevention for HIV/AIDS and other STDs among trans individuals.9,22,24 One participant stated, “In a certain clinic . . . they did some tests, and from that, someone opened their mouth and told everyone that certain friends were living with HIV and certain friends had STIs. So, because of this, many people don’t get tested or go for a check-up” ( 24 , p. 320).
Social Support
Social support is one of the most significant determinants of using health care centers.7,24,56 Studies have shown that trans people express their unique needs in supportive environments. 49 One participant noted, “Sometimes, just online, finding other people that encounter some of the same barriers that I do that—just being able to talk about it is usually helpful” ( 5 , p. 8). The essential support source is family, followed by friends and acquaintances. 45 The risks of HIV/AIDS and other STDs are reduced if supportive staff visit transgender individuals.9,42 Supporting adults and peers has a facilitating role in preventing HIV/AIDS and other STDs. 9
Challenge with Name
Six studies described trans people want a legal name for themselves,9,21,25 and they have numerous challenges in changing their identity. It is undesirable for them if providers use their chosen name inconsistently, use incorrect pronouns, or call them by the name of birth.32,42,57 Using the correct form of the name or neutral language creates self-confidence in the trans person and helps communicate with the medical staff. 9 As one participant shared, “Look, I don’t like being called Juan; I like to be called Berta because I feel like I’m Berta. She [the secretary] doesn’t understand. She [the secretary] said, ‘But your papers say that your name is Juan and to me, you are Juan because you are a man’” ( 24 , p. 319).
Social Level
In the SEM, accessibility, insurance, norms, culture, protocols, and regulatory factors constitute the social level.
Accessibility
Inaccessibility is referred to as a barrier to reaching SRH facilities. Studies have revealed that public health services are free or low in cost. However, they have some difficulties like low quality, inconvenient geographical locations, and long waiting hours.24,56 One participant explained, “So it's about a two-and-a-half-hour drive to the closest place that might have reproductive health care that is competent for trans people” ( 5 , p. 7). Additionally, these conditions are exacerbated in rural areas.28,51 Lack of trans-oriented clinics with competent staff and lack of budget and facilities are other barriers to accessing SRH services. 9 One participant said, “What's missing is all that concerns everyday health, like getting tested and how to get hold of a good gynecologist? How can you get it all, and not only all that is considered exotic about transgender, but all the other stuff that all people need?” ( 27 , p. 324). The accessibility to the health care system is associated with disparities among racial/ethnic populations, and this situation is exacerbated in black trans individuals compared to white.9,51 Seven studies reported that disparities in the health care system are identified not only in developed countries but also in low-income societies that are associated with discrimination.51,58 The transgender population in low- and middle-income countries faces more challenges in accessibility to SRH services. 33
Insurance
Three studies reported lack of insurance coverage or exclusions as another barrier to fertility preservation, gamete retrieval, and gender-affirming health care.5,19,38 One participant shared, “pay out-of-pocket for those services” ( 5 , p. 6). Even transgender patients with health insurance have difficulty obtaining care, and most policies exclude coverage for gender-confirming interventions and surgeries. 5
Norms and Culture
Cultural attitudes and beliefs about transgender people have been mixed with misconceptions and transphobic ideas.5,20 The consequences of transphobic behaviors were the most significant reasons why transgender individuals found it difficult to access SRH services. 8 This contributed to a perception among trans individuals that they were incompetent to seek SRH services. A participant said, “we were told by homophobes and transphobic people all the time that we are not worthy” ( 5 , p. 9). Trans women, particularly trans women of color and those who are marginalized, experience high rates of violence and exclusion. 46
Protocols
Lack of consistently applied protocols was cited as a barrier to accessing SRH care, especially for young individuals at puberty. 19 The development of protocols for maintaining transgender individuals should be transgender-inclusive and holistic.49,51
Right and Legislation
Reducing health inequalities is a fundamental goal for the general population and essential for gender-minority groups.53,58 In general, the prevailing political climate prevents effective communication around the SRH axis, and transgender individuals continue to experience inequalities in accessing health and social care services. 27 One participant noted, “Of 11 candidates, I think at least nine have spoken out against people like me, this is no way to live, having government leaders who speak out against who I am as a person and whose policies deny me my rights” ( 20 , p. 839). On the other hand, some religious centers exacerbate this situation by stigmatising this population, affecting their health. Politicians and other stakeholders should have strong strategies to support transgender individuals’ SRH services.38,40
Discussion
This meta-synthesis used the meta-ethnography method of Noblit and Hare (1988) to systematically analyze and synthesize qualitative data from 50 qualitative studies. To our knowledge, no previous literature review has focused on barriers and facilitators to accessing sexual and health services by trans people based on SEM. This review shows that factors influencing the health-seeking behaviors of transgender individuals can be categorized under the SEM as individual, interpersonal, institutional, and social factors. In examining these issues through the lens of the SEM, it appears that such factors are prevalent across all trans individuals’ experiences, from the individual to the societal level. Most of the included studies primarily focused on the negative experiences with only limited reference to some successful experiences. Future research would benefit from exploring the positive experiences or aspects that transitioning and embracing gender identities has on transgender individuals because this is also important in understanding.
Transgender individuals, like other people in society, should have equal rights to access SRH services. Poor SRH knowledge and practices among this population are a complex matter affected by personal, community, and regulatory factors. All these factors overlap and are affected by each other. Therefore, it seems that the problems of trans people should be studied and analyzed in their living environment, according to cultural, social, and economic conditions. This model can guide politicians, medical staff, families, and society to identify and solve problems because it can identify weaknesses and complexities in the SRH field. According to the culture and context of their community, influential people can identify problems at each level and take action to resolve them. By incorporating these levels in qualitative studies, barriers and also facilitators to accessing SRH services are more readily understood.
Furthermore, recommendations are generated that consider the interdependence of these levels and inform the choice of intervention to improve access to SRH services for transgender population. The results indicate that transgender individuals are mostly a hidden population, and we have little information about their stress level and coping mechanisms. For that reason, further research is needed to overcome these barriers regarding the emotional well-being of trans individuals and their families.
Information Empowerment
Limited information and lack of awareness seem to be the essential hurdles for accessing SRH services.20,44 Consequently, considering that trans individuals do not have enough information about SRH or they are too young or immature to understand these types of issues, it is essential to empower their awareness and knowledge by disseminating accurate information and supporting this population against irreversible decisions and vulnerability to risky conditions such as HIV/AIDS and other STDs. 9 It is worth mentioning that raising the community's awareness and knowledge, especially among parents, peers, and medical staff, is also crucial in increasing the use of SRH services by trans people.
Relationship Empowerment
Transgender individuals may face lifelong difficulties from social marginalisation, rejection from family, depression, substance abuse, and bullying to intimate partner violence, leading to weaker SRH conditions. Furthermore, there is a need for increased social support for SRH. Attitudes about risky and safe relationships also need to be addressed, especially within sexual relationships. For example, prevention programming could reframe perspectives around intimacy and promote the use of condoms. These targeted programs for trans individuals decrease the risk of HIV/AIDS and other STIs. Moreover, suppose the relationships between family, peers, health care providers, and trans individuals are based on knowledge, respect, understanding, and non-judgment. In this case, negative consequences such as rejection from family, dismissal from work, and reluctance to seek health care can be avoided to a large extent.27,59 The results of this review showed trans individuals’ desire to access information related to their health and well-being from knowledgeable and well-respected health professionals. The results suggest that we can hope to manage relationships by enhancing families’ knowledge about affected individuals.
Community Empowerment
Stigma and discrimination are the most prominent barriers deterring trans individuals from seeking health services. This review's findings demonstrated that strong social stigma and discrimination against trans individuals contributed to trans’ reluctance to seek appropriate treatment. In general, we recommend that health care providers communicate with trans people non-judgmentally, avoid assumptions about sex and gender identity, and focus more on patients’ health. With their negative and stigmatized attitudes and denial of treatment to trans individuals, health care providers neglect their duty to safeguard all patients and violate the trans individuals’ equal rights to health. Meanwhile, the fear of disclosing their gender identity to health professionals has limited access to health care, which could undermine the accuracy of diagnoses and treatments’ effectiveness. Their negative experiences with health care providers further affect their future use of SRH services. The World Health Organization guidelines on HIV/STI prevention and treatment for transgender people (2011) state, “Legislators and other government authorities should establish antidiscrimination and protective laws, derived from international human rights standards, to eliminate discrimination and violence faced by transgender people, and reduce their vulnerability to infection with HIV, and the impacts of HIV and AIDS”. 60 This review highlighted the importance of removing obstacles faced by transgender people in accessing health services and combating stigma in health care settings. Also, there is evidence that requiring health care providers to undergo a sensitivity training program can improve their knowledge and attitudes toward a stigmatized community.
Social Empowerment
Social deprivation is the greatest challenge to the health and well-being of transgender populations. The underlying social exclusion mechanisms that undermine the right to health in health settings and broader society must be addressed. The results of this review demonstrate that there is a lack of good, available, accessible, and affordable SRH services for transgender people. Many health services are unsuccessful in meeting the multiple health needs and priorities of the gender-minority identities. These vulnerable people would like to access acceptable, affordable, and accessible SRH services that treat HIV/AIDS and STDs and cover other conditions like treatment and transition surgeries care, reproductive health, and mental health with full insurance coverage.
Study Limitation
Although the SEM addresses the complexities of the health-seeking behaviors of transgender people and offers strategies to improve their access to health care, this model also has limitations. It fails to show how factors at each level influence SRH behaviors. The model's complexity also reflects the practicalities and difficulties of developing appropriate interventions. 16 This meta-synthesis included all moderate- to high-quality studies, but most were of reasonable quality. Thus, more studies examining the SRH of transgender individuals are needed to increase knowledge and understanding of this population. This review reveals different layers of barriers and facilitators that prevent or improve transgender individuals from seeking SRH services. In this review, we focused on studies from 2005 to 2021. We may have lost some older information due to having an updated and in-depth look at the subject. The other limitation of the review is that most studies were mainly from the United States and Europe, and there are limited data from Asia and Africa. This review only included studies published in English. Therefore, we may have missed studies on this topic in non-English language journals. Looking at the concepts with an intersectionality lens, it must be noted that there are geographical and cultural differences between different nations, hence some of the interpretations cannot be extrapolated to other populations given the existing differences. Moreover, utilising background information from other cultures to support current findings in this study might not be fully logical due to the same differences.
Conclusion
The results demonstrate that the transgender population faces some barriers and facilitators to accessing SRH services across four levels mentioned in the SEM: individual, interpersonal, institutional, and social. Each level manifested the barriers and facilitators to accessing SRH services among this population. Furthermore, based on ethical principles, these individuals have the same rights as cisgender persons to benefit from SRH care. The review's findings provide potentially valuable insights for politicians and other stakeholders to support transgender individuals’ SRH.
Supplemental Material
sj-docx-1-joh-10.1177_27551938231187863 - Supplemental material for Barriers and Facilitators to Accessing Sexual and Reproductive Health Services Among Transgender People: A Meta-Synthesis
Supplemental material, sj-docx-1-joh-10.1177_27551938231187863 for Barriers and Facilitators to Accessing Sexual and Reproductive Health Services Among Transgender People: A Meta-Synthesis by Mina Saadat, Afsaneh Keramat, Shayesteh Jahanfar, Ali Mohammad Nazari, Hadi Ranjbar and Zahra Motaghi in International Journal of Social Determinants of Health and Health Services
Footnotes
Acknowledgments
Shahroud University of Medical Sciences supported the present study as a Ph.D. thesis. As a result of this, acknowledge the research deputy for grant No. IR.SHMU.REC.1398.234.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.