
Abstract
Addressing racism within health systems and services is critical to addressing health vulnerabilities and promoting health equity for racialized populations. Currently, there is limited knowledge about the ways in which racism affects health services for adolescents. A scoping review was undertaken following the Joanna Briggs Institute Manual for Evidence Synthesis methodology and guided by the research questions: (1) What are the characteristics of the literature examining racism in health service use for adolescents? (2) What are the foci of the literature on systemic racism and health services for adolescents? A systematic literature search was conducted in April 2021 to identify all relevant published studies. The search identified 3049 unique articles, with a total of 13 articles included in this review. Multiple levels of racism were examined in the included articles across various health care settings. Five foci were identified: racism prevention, missed care, quality of care, racial bias, and experiences of racism. Our review indicates a current emphasis on interpersonal racism within this field of study, with emergent discussion of the impact of systemic racism. However, greater attention is needed that would investigate multiple forms of racism (institutional, interpersonal, internalized) in relation to specific contexts and adolescent populations.
At a time of growing awareness of health and social inequities, documenting the impact of discrimination across political, social, economic, educational, and health systems has been a growing focus for action.1–3 The increase in international activist movements, such as Black Lives Matter, Idle No More, and Stop Asian Hate, has served to remind leaders, policymakers, and scholars of the ongoing need to address the impacts of race and racism.4–7 As a socially constructed concept, “race” refers to power-based social relations through which individuals and groups are categorized according to their physical characteristics.4,8,9 Racism can be defined as an organized system of oppression, underpinned by deeply rooted societal beliefs about race, that creates a hierarchical categorization based on “race.”8,10 As a result, racism denies racialized populations equal opportunities and privileges.10–12 Members of Indigenous groups in countries colonized by European imperialization are racialized and continue to experience racism globally.13,14 Additionally, in societies built on white dominance, visible minorities made up of both citizens and newcomers from a diversity of ethnocultural backgrounds are racialized and subject to the impacts of racism.3,13,14,15
As a system, racism operates at multiple levels: internalized (incorporating ideologies into one's personal worldview), interpersonal (interactions between people), and structural or institutional (access to resources, services, or opportunities within society).8,10–12 Racism can also be enacted through racial biases and discrimination. Racial biases are negative associations about certain racial groups that consciously or unconsciously affect an individual's perceptions, attitudes, and actions. 16 Explicit racial bias refers to “beliefs that are known to the individual and can readily be expressed by self-report” (Ref. 17 , p. 2), whereas implicit bias includes the unconscious attitudes that influence an individual's behavior. 18 At the systemic level, racism can be manifested in social discourses, policies, and practices.8,10 Racial discrimination describes actions that are motivated by racial biases and the social inequalities that result from racism.19–21
The dominance and normalization of white cultures, norms, and values—referred to as whiteness—in many parts of the world grants white people with privileges and advantages based on the color of their skin.8,22,23 The ideology of whiteness manifests through a socially constructed racial hierarchy, often operating without being named or questioned, which places groups racialized as white at the top of this hierarchy. 8 This perpetuation and validation of whiteness occurs through white supremacy, the underpinning system that serves to sustain and promote the structure of racism.8,23 Previous literature documents the role of racism in shaping the structural disadvantages in educational and political access24,25 and social participation25,26 for racialized populations.
In health systems, racism is evidenced in the policies and practices of its institutions, actions of its service providers, and health outcomes of service users. Racism in the health care system is a pressing human rights and public health issue globally as it shapes equitable access to health services and treatment for racialized patients.27–29 In health care systems, racism continues to perpetuate and reinforce the system of white supremacy in the perceptions of pathologies following racial lines, 22 white health professionals holding the majority of leadership roles within the field, 5 and the Euro-centric lens applied to health care pedagogy and research. 8 In the absence of addressing racism in health systems, racialized groups will continue to experience health vulnerabilities.29–31 Confronting and addressing the impacts of racism within the health care system are therefore critical to promote health equity for racialized populations.
Racism in Health Care
As awareness has grown of the pervasive nature of racism across systems, more attention has been devoted to the interaction of racism and health. A growing body of research has examined racism as a social determinant of health, where racism is linked to unhealthy behaviors (ie, alcohol, tobacco, or drug use),32,33 diminished physical health (ie, over-stimulation of the body's physiological stress response, hampering proper immune system functioning), 29 and poorer mental health outcomes for racialized groups.26,33 Less studied is the manifestation of racism within health care systems and services.
During the life stage between childhood and adulthood, adolescents experience numerous physiological and psychological developments where adequate health care can critically shape their present and future well-being. 33 Adolescents are also especially vulnerable to racism as the developmental growth and identity formation that occur in this period rely on positive social interaction and support. 34 In this vein, racism in health care services for adolescents can have especially harmful impacts. Though less documented than with adult populations, racism and health has been explored with young people in terms of both health outcomes and experiences of racism when accessing or using health care services.32,35–37 If responses to racism when accessing or using health care in adolescence are similar during adulthood, then it can be predicted that such experiences will diminish adolescents’ trust in health care services and deter their use of health care both in the present and the future, imposing barriers to their long-term health and well-being.27,28,33,38 Thus, it is critical to further explore the experiences of racism in health care access and use for the adolescent population.
Study Purpose and Research Questions
Racism is increasingly being recognized as a social determinant of health,29,33 and research on the ways in which racism affects the access and use of health services is also growing.27,38 There continues to be limited study, however, on the impact and experiences of racism within health services for adolescents. Examining the existing literature provides an analytical starting point to better understanding how racism is manifested in health services for adolescents. This scoping review was guided by the following research questions:
What are the characteristics of the literature examining racism in health service use for adolescents? What are the foci of the literature on racism and health services for adolescents?
As the first scoping review on this topic, to our knowledge, the aim of this review is to organize and summarize the literature on racism in health services for adolescents and to identify areas for further investigation.
Methods
Our review is reported in adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) statement 39 and PRISMA for Searching (PRISMA-S) extension. 40 Methodologically, this review was conducted in adherence to the Joanna Briggs Institute Manual for Evidence Synthesis, Chapter 11: Scoping Reviews. 41 The review protocol was registered on Open Science Framework on February 24, 2021.
Data Sources and Search Strategy
A systematic literature search was conducted in April 2021 by an experienced health sciences librarian (MK) to identify all relevant published studies. Searches were performed in the following bibliographic databases: Medline (1946-Present), EMBASE (1974-Present), and PsycINFO (1806-Present) via OVID; CINAHL (1936-Present), Alternative Press Index (1969-Present), Anthropology Plus (Inception-Present), and SocINDEX (1913-Present) via EBSCOhost; Scopus (1976-Present) via Elsevier; Dissertations and Theses Global (1861-Present) and Sociological Abstracts (1952-Present) via ProQuest. (See Supplementary File 1 for additional details about our search strategy.)
These databases were searched using a combination of natural language vocabulary and controlled terms (subject headings). Natural language terms were derived from three main concepts: (a) racism or racial discrimination; (b) health services access, utilization, quality, and services; and (c) adolescents. To increase search sensitivity, restrictions to publication date, language, and study type were not applied. Articles identified through database searches were exported in complete batches and duplicates were automatically removed upon import to the systematic review management software, Covidence. In total, 4000 articles were identified through database searches in April 2021, and 950 articles were removed through deduplication.
Other search methods were employed to retrieve additional evidence. These methods included hand searches of the reference lists and forward citation searches, using Scopus, of papers included in the scoping review. The team reviewed gray literature on this topic using a targeted website search (see Supplementary File 2 for the list of websites). These websites were searched using simple keywords, such as racism, health, and adolescents and by viewing the reports, publications, and news items available.
Study/Source of Evidence Selection
All articles identified through database searches were imported into the systematic review software, Covidence, to facilitate the title/abstract and full-text screening. The selection of sources followed the JBI guidance on population, concept, and context inclusion criteria.
Population
While the World Health Organization 34 defines adolescence as young people aged 10 to 19 years, existing literature suggests that most studies conducted with adolescents include participants aged 12 to 18. 12 To remain consistent with the existing literature and to align the age range with how health services and programs are organized and delivered within health systems such as in the authors’ context (Canada), this review included articles focused on young people aged 12 to 17 years. Articles with an age range beyond the 12 to 17 years were included provided the article disaggregated data for the target age group. Sources referring to “adolescents,” “young people,” or “youth” without identifying a target age range were also included in the review.
Concept
Included articles explored the concept of racism at any of the three conceptual forms or domains: institutional, individual, and internalized. In this review, we define racism as a hierarchical categorization based on race underpinned by an organized system of unequal power relations.8,42 Structural or institutional racism refers to processes that are embedded in social structures through policies and institutional practices that differentially neglect and disadvantage racial groups deemed as inferior, while providing privileges to racial groups deemed as superior.43,44 Individual-level, or interpersonal, racism refers to experiences of discrimination between individuals and is referred to in the literature as racial discrimination, perceived discrimination, and self-reported discrimination.33,45 Internalized racism describes the acceptance of negative assumptions and stereotypes by members of oppressed groups. 46
Context
This review included articles that focused on young people's access to and use of health care services. For the purposes of this study, we broadly defined health services to include acute health services (ie, hospitals, emergency care) and community or ambulatory health services (ie, preventative care, home care, rehabilitative care, diagnostic care, dental care).
Other Criteria
Articles were included if they were published in the English language. Primary or gray literature sources were included except for books, conference proceedings, and clinical trial descriptions. Timeframe or date of publication was not a criterion for inclusion/exclusion to capture as much of the relevant literature as possible.
Titles and abstracts were screened by two independent reviewers (SLP and GG) for assessment against the a priori inclusion criteria. All articles were independently classified as “include,” “exclude,” or “unsure” by both reviewers, including articles where abstracts were not available. Potentially relevant articles that were classified as “include” or “unsure” were retrieved for full-text screening. The full texts of selected citations were independently assessed in detail against the a priori inclusion criteria by the same reviewers (SLP and GG). Articles were classified as “include” or “exclude.” Reasons for exclusion of full-text articles that did not meet the inclusion criteria are reported in the PRISMA flow diagram (see Figure 1). Any disagreements between the reviewers at each stage of the articles selection process were resolved through a third reviewer (CH). Articles identified for data extraction were exported from Covidence to the reference management software, Excel 2019, in tabular format.
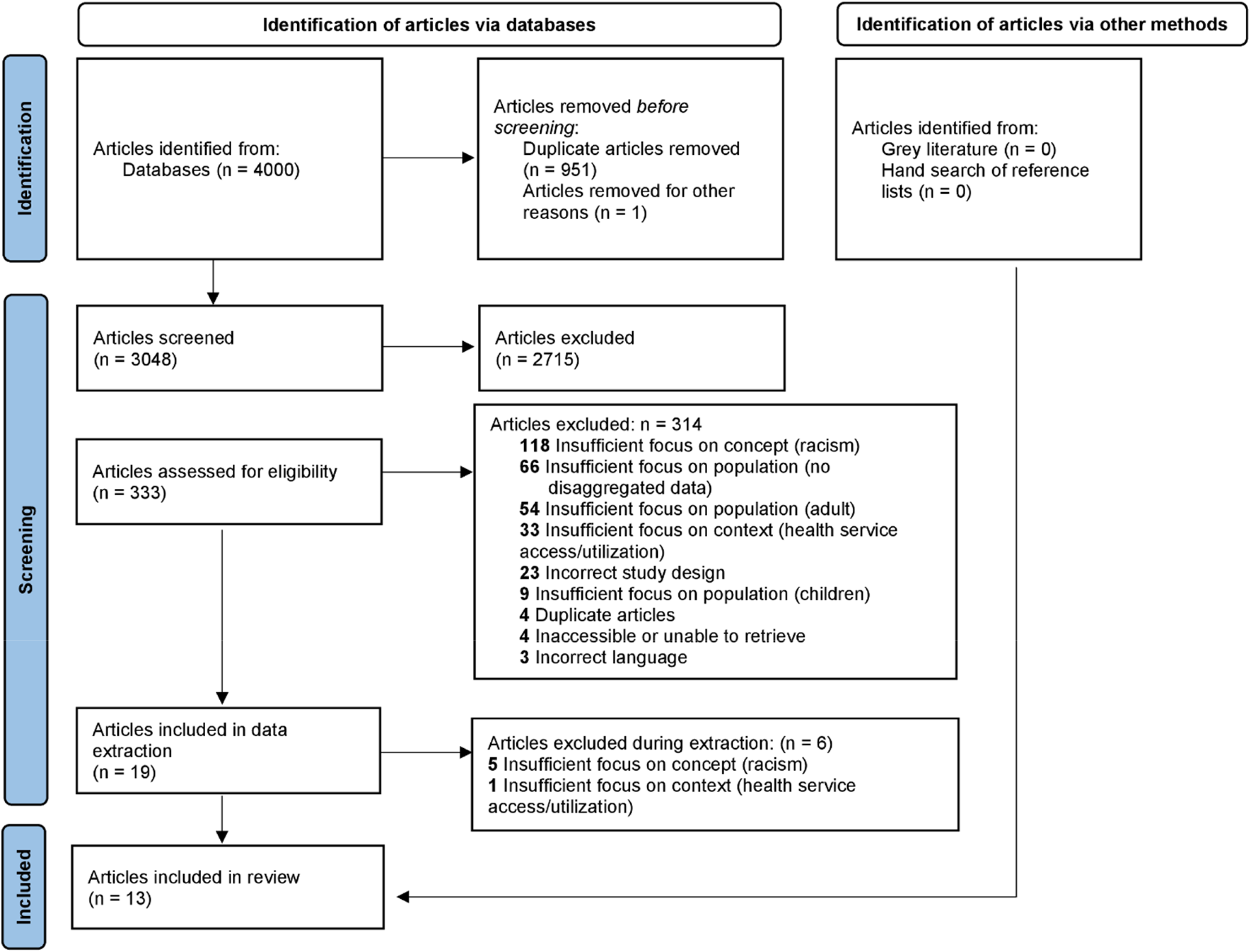
PRISMA flow diagram.
Data Extraction
Data were extracted from articles by two independent reviewers (MT and GG) using a data extraction tool developed by the study team. The data extraction tool was adapted from the standard JBI instrument for data extraction 41 and included specific details about the population, concept, context, study methods, and key findings relevant to the research questions and review objectives (see Supplementary File 3 for the modified data extraction instrument). The data extraction tool was iteratively modified as necessary during the process of extracting data to ensure the tool captured the breadth and depth of the data. Any disagreements between the reviewers were resolved through discussion with the study team.
Data Analysis and Presentation
The extracted data were summarized using descriptive statistics (ie, frequency counts) and qualitative content analysis. 47 Qualitative content analysis was used to classify the data into explicit categories rather than interpreting the data or identifying latent themes.47–49 The identified categories are presented as the foci of the literature.
Findings
Selection of Sources of Evidence
The initial search of databases identified 3048 unique articles. Title and abstract screening removed 2715 articles that did not meet the inclusion criteria. Of the remaining 333 articles, 314 were removed during full-text screening and a further 6 were excluded in the process of data extraction, yielding 13 eligible articles that were included in this review. The hand search of reference lists and gray literature search did not yield any additional sources of evidence for this review. This selection process is shown in Figure 1, Prisma Flow Diagram. Findings of this study are organized into two sections based on the research questions: (a) Characteristics of the Literature and (b) Foci of the Literature.
Characteristics of the Literature
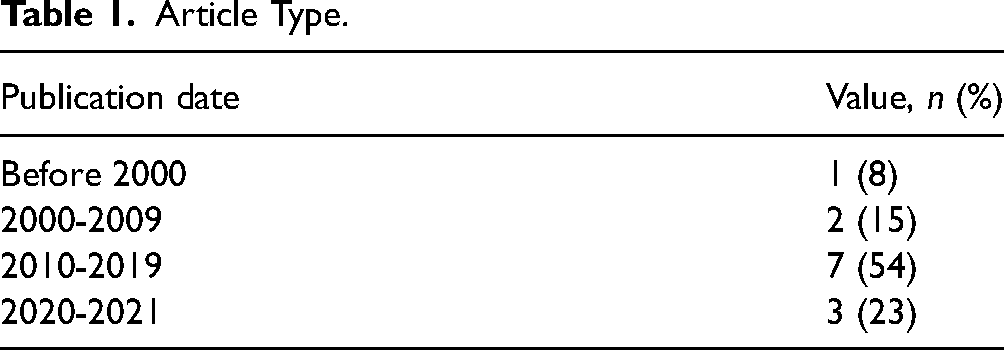
Included articles were published across four decades between 1979 and 2021 (median = 2017) (see Table 1). Articles were published in journals that spanned a range of fields of study, including clinical health (n = 3), social work/social services (n = 3), public health (n = 2), and psychology (n = 1). Included articles were split between empirical studies and discussion papers. Seven articles described primary research, 1 of which was a dissertation. The remaining 6 articles offered discussions of racism in health services. Of the empirical articles included in this review, quantitative and qualitative methodologies were equally applied, and one study employed mixed methods to collect data.
Article Type.
Population
Six articles did not provide an age range and instead used terms such as “youth” and “adolescents”.50–55 Of the 7 articles specifying age, youth ranged from 13 to 21 years old, with 14 to 16 years old being the most common range. Most of the articles (n = 8) focused on only one racialized group.50,51,53–58 Racialization refers to the process of being assigned to a particular group based on characteristics associated with race, 59 such as Asian or Black. By contrast, 5 articles explored more than one racial group at a time.20,52,60–62 Four records compared experiences of racism between racialized and non-racialized youth.20,60–62 Across all included records, focusing on African American and Black populations (these terms were used interchangeably in some American articles to refer to individuals whose ancestors were originally from Sub-Saharan Africa) occurred most frequently (n = 8),51–54,56–58,61 followed by 3 articles that focused on Asian populations,18,53,58 2 records focused on Hispanic populations,50,52 2 focused on Pacific Islander populations,20,60 and 3 focused on Indigenous populations that further subdivided into the Maori people of New Zealand20,60 and the Sami people of Norway 62 (see Supplementary File 4).
Concept
All levels of racism were examined in the included articles (see Figure 2). In some cases, racism was explored in relation to other forms of oppression. For example, 4 articles explored sexism,50,57,58,61 2 articles examined classism,50,61 and one article addressed colorism. 57
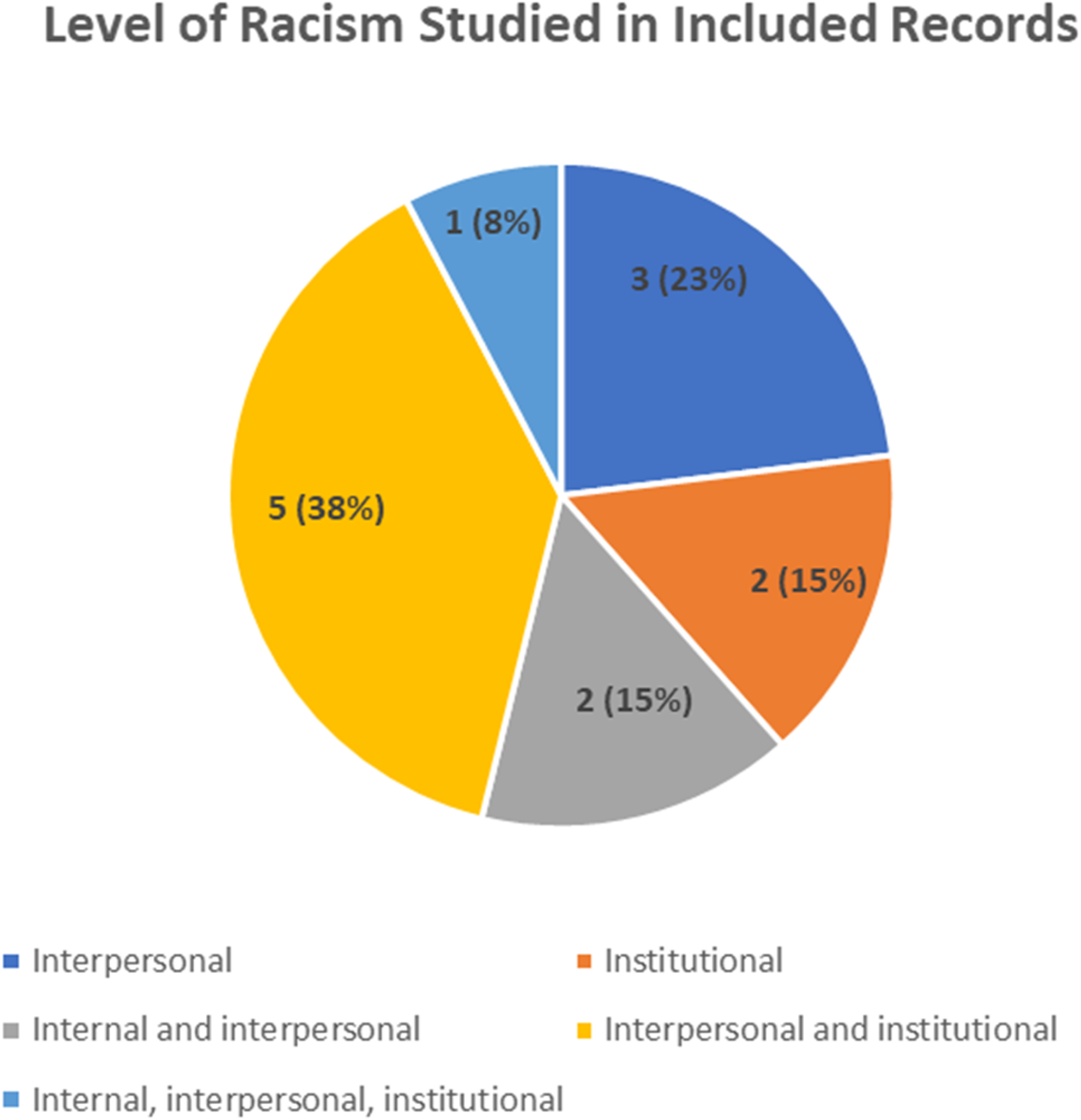
Level of racism.
Apart from 2 articles focused on racism prevention,56,58 the remaining 11 articles explored existing racism in health care services access and utilization. Racism was more often explored in terms of health care service utilization (n = 6),20,50,55–57,61 which refers to the experiences of using health services, compared to health care service access (n = 2),52,62 defined as the barriers or facilitators in accessing health services. An additional 5 articles discussed both access and use of health care services.51,53,54,58,60 Of the articles discussing health care service utilization, the majority examined treatment and care of racialized adolescents, in terms of both the quality of care and differences in treatment experiences compared to non-racialized youth.50,54,55,57,60,61
Context
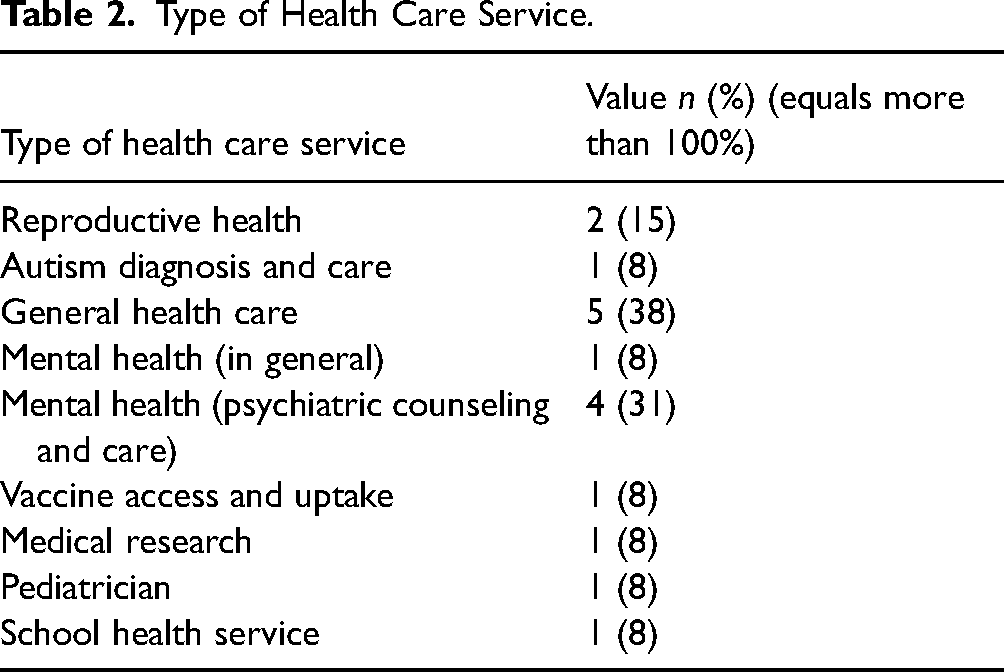
Three countries were represented by the articles included in this review: United States (n = 10), New Zealand (n = 2), and Norway (n = 1) (see Supplementary File 4). Racism was most commonly examined in general health care such as check-up visits with general practitioners (n = 5; 38%)20,53,60–62 including both general mental health care 52 and psychiatric counseling and care54,56,58,62 (see Table 2). Racism was explored in a variety of other health care settings but with less frequency, including reproductive health,50,57 autism diagnosis and care, 51 vaccine access and uptake, 53 medical research on vaccines, 53 pediatrician services, 55 and school health services. 62 Across these health care contexts, interpersonal racism between health practitioners and youth was most explored.20,57,61
Type of Health Care Service.
Foci of the Literature
Using qualitative content analysis, the included articles were examined, and the findings summarized to identify major foci in the literature examining racism in health service access and use. Five foci were identified: racism prevention, missed care, quality of care, racial bias, and experiences of racism.
Racism Prevention
Of the 13 included articles, 2 (15%) discussion articles focused on racism prevention in health care practice.56,58 These articles did not discuss racism that had already occurred in health services and instead took a proactive approach to minimizing these occurrences. The context of both articles was mental health, written from the perspective of therapists. Both articles focused on practitioner strategies to minimize the perception of racism and address past experiences of racism in therapeutic encounters with Black or African American youth. As such, these articles identified therapeutic care as possible environments where systemic racism is perpetuated and focused their discussions on prevention strategies as well as the lived experiences and contexts of racialized patients.
The level of racism discussed in the articles differed. Friedman 56 highlights internalized racism in cross-racial therapeutic dyads, where the therapist represents the majority white population and the patient is part of a racial or ethnic minority, by stating that white therapists must address their unconscious bias. By contrast, Venable and Guada 58 focus on culturally competent therapeutic treatment to redress historic and current instances of institutional racism against African Americans in the health care system. Venable and Guada point out that mistrust of therapeutic care is common among African American patients due to past psychiatric abuses, which must be acknowledged by the therapist.
Missed Care
In some cases, experiences of racism prevented youth and/or their families from receiving necessary treatment and care.51,52,54,55 Two (15%) articles highlighted gatekeeping, where health care professionals impeded racialized patients’ access to mental health treatment by delaying specialist referrals or dismissing pathologies without a referral.52,54 In cross-racial treatment, racialized youth reported that their health care needs were dismissed or minimized by non-racialized health professionals; this, in turn, limited their access to treatment.54,55 For example, Nguyen-Truong et al. 55 discussed a family's interaction with a pediatrician wherein their experience of racism was dismissed, which prevented the adolescent children from receiving timely mental health care. Compared to their non-racialized counterparts, 2 (15%) articles reported that Black or African American participants also experienced longer wait times for diagnostic services and delays in diagnoses,51,54 preventing timely treatment. Evans and Gusmano 53 suggested that historic instances of targeted malpractice against African Americans significantly reduced current uptake of recommended preventative care, specifically related to the HPV vaccine.
Quality of Care
Over half (n = 7, 54%) of the included articles reported that racism affected the quality of care for racialized adolescents.20,50,54,55,57,60,61 For some, this occurred through misdiagnosis or inappropriate medical treatment.54,57 For example, Lewis and colleagues 54 describe the role of racism in the misdiagnosis or absence of diagnostic care among Black youth presenting with extreme psychopathological symptoms, which affected quality of care and psychiatric health outcomes among these youth. In the context of reproductive health care, African American and Latina youth have reported being indiscriminately offered contraceptive advice and methods regardless of the reason for their visit or their personal needs.50,57 A conversation analysis of teenage white and Black patients and pediatricians found that Black youth received significantly less health promotion advice and guidance than their white peers. 61 Pope also reported shorter pediatrician appointments with racialized patients and the use of obstructive communication such as conversation domination, closed-ended questions, and power-oriented interruptions during those visits. 61
Neglecting the long history of racism in health care was also cited as shaping treatment and care for racialized adolescents.50,53 For instance, racialized individuals were encouraged to receive health services designed for non-racialized patients that did not consider their historical situatedness. Evans and Gusmano 53 describe African American mothers’ experiences with the HPV vaccine for their adolescent sons, where participants felt that the vaccine initiative was a tool of continued systemic oppression within health care. The authors point out that the vaccination initiative did not consider the historical context of institutionalized health care racism enacted against African American populations (ie, the Tuskegee syphilis study), nor adjust its approach to vaccine uptake accordingly.
Racial Bias
Nearly half (n = 6, 46%) of the included articles highlighted racial bias in health care access or use among racialized adolescents.50,52,54,55,57,61 These articles described health professionals’ assumptions about adolescents’ health-related behaviors and needs, based on racial stereotypes or narratives. A range of health contexts were described in these articles, including mental health and psychiatric care,52,54 reproductive health,50,57 and general pediatrics.55,61 Health care professionals commonly drew on racial stereotypes as a basis for their assumptions. For instance, adolescent participants of a qualitative study of African American females’ reproductive health experiences reported service providers making assumptions about the young women's sexual activity. 57 Similarly, a study from the perspective of child welfare caseworkers found that when making mental health referrals for youth, they relied on deeply rooted stereotypes of racial minority norms to assume parents’ disinterest or inability to provide care to their children. 52 In other cases, health professionals concluded that pathologies were exaggerated by racialized patients, such as the case described by Nguyen-Truong et al. 55 where a pediatrician suggested that parents were hyper-emphasizing the psychological impacts of a racist incident on their children. Lewis et al. 54 likewise concluded that “(Psychological) symptoms that would be recognized as pathological in white children…were ignored in black children” (p. 54), in part due to assumptions of behavioral manipulation by the adolescent patients.
Experiences of Racism
Patient experiences of racism refers to racialized individuals’ perceptions of accessing or using health care. Four (31%) articles discussed participants’ alienation from both general and specific health care services following interpersonal and institutional experiences of racism.53,55,58,60 Specifically, these articles highlighted participants’ mistrust of the health and medical systems 53 and dissatisfaction with health care services. 60 Patients also shared their perception of receiving less respect from health professionals or receiving “unfair” treatment when accessing or using services.20,55,57 Although past examples of systemic racism in health care are well known, only 2 (15%) of the 13 included articles53,58 drew a direct connection between systemic and historical racism in health care and diminished trust of the healthcare system.
Discussion
Previous research has established that racism is a critical determinant of health outcomes for adolescents. 12 The findings from this scoping review contribute to current knowledge about racism by systematically identifying and summarizing existing literature pertaining to racism in health services for adolescents. Examining the ways in which racism may shape health outcomes through health services is critical to identify opportunities for changing practice and service delivery. In addition, our review provides insights on how racism has been studied across time, the foci within the literature to date, and knowledge gaps that can be addressed in future research.
The findings from our review map how racism in health services for adolescents has been studied across 4 decades. Most of this literature was published within the past decades, with limited scholarly discussion occurring prior to 2010. This finding is congruent with the results of a scoping review exploring barriers to accessing mental health services for Black youth within the Canadian context. 63 Coupled with other systematic reviews completed in the field of racism,12,64 our findings indicate that the increase in scholarly work aimed at understanding racism may be a response to societal demands aimed at dismantling social injustices that have been amplified in more recent years. As social movements striving for Black liberation and Indigenous sovereignty gain traction, it is possible that the literature on impacts of racism on health services and systems, including for youth, will also increase.
The dearth of literature between the late 1900s and early 2000s may be explained by the evolving ways in which racism is conceptualized. During the data screening stage of our review, we excluded articles that did not explicitly indicate racism. It is important to note that many articles reported racism in their results but did not explicitly indicate racism in the objectives or research questions and thus were not included in our review. While many of the excluded articles documented significant disparities for racialized youth, these disparities were not investigated in relation to racism. It is possible these excluded studies attempted to communicate the impacts of racism on health disparities, albeit largely without using the terms, concepts, and language employed in more recent scholarship on racism. Although much academic investigation focuses on differences in health service access or use according to race, it often stops short of naming racism as culpable even when implicated.65–67
For example, Breland-Noble 68 documents mental health disparities for Black adolescents through historical and perceptual barriers. Specifically, Breland-Noble 68 explores historical barriers causing mistrust of the health care system among Black adolescents, and offers clinical directions rooted in culturally responsive training and treatment. The current shift in focus toward an anti-racism praxis, as opposed to culture-based training, may explain the emphasis on culturally responsive training in Breland-Noble's 68 study. An anti-racism approach addresses issues of disparity from the perspective of structural oppression and racial power hierarchies.22,69,70 The shift in focus from culture to racism has identified issues of oppressive structural conditions that create vulnerabilities for racialized groups.
Similarly, Cuffe et al.’s 71 study illuminates the different health care treatment of adolescents based on race and gender. While this study explores race as a factor in the treatment of psychiatric disorders for adolescents, the emphasis remains on issues of race and not racism. Put differently, the focus rests on what (the racial differences that exist in health care) and overlooks why (the stereotypes, prejudices, or discrimination associated with these racial differences). This focus on race reflects the agenda of advancing the socially constructed notion of biological differences due to “race,” rather than the differences stemming from racism as a social determinant of adolescent health. These findings illuminate the ever-changing nature of scholarly discourses on the topic of racism in health care and may clarify the dearth of past literature included in this review.
Furthermore, this review found that racism in health care services was commonly manifested through the quality of treatment and care received by racialized adolescents. Importantly, the trend across articles reporting the impact on quality of care for racialized youth aligns with previous research establishing associations between racism and health outcomes for this population.12,63,64 In a systematic review of mental health service utilization for Black youth, Planey et al. 72 identified clinician factors as significant barriers in accessing and utilizing mental health services. Clinician-related factors included Black teens having negative past experiences with providers and fears of receiving inequitable treatment when compared to their white counterparts, and clinicians not responding to the unique needs of Black youth—all of which affected quality of care. 72 In several studies, health care providers were viewed as gatekeepers to treatment52,54 and directly contributing to (in)equitable care and treatment based on antecedent racial biases.50,54,57,61 The impact of health care provider bias on provider-patient interactions and clinical judgment are well-documented in the literature.27,73,74 In this way, our review indicates a current emphasis on interpersonal racism in the extant literature.
Despite, the current emphasis on interpersonal racism, there is emergent discussion of systemic racism. The studies identified through this review were conducted in Western countries (the United States, New Zealand, and Norway), contexts in which the racist beliefs of the health care providers may be shaped by their socialization within societies rooted in structural injustices such as white supremacy.22,75,76 For example, Evans and Gusmano 53 noted that the long history of medical racism against Black populations was strategically and systematically neglected in the structure of examining HPV vaccine uptake among African American adolescents. The findings suggest a need to recognize and redress the impacts of racism and white supremacy as belief systems that have shaped institutions, including health care.4,77
Several gaps in the literature emerged from the findings of this review. While our review identified literature on the presence of systemic barriers, knowledge about the nature, extent, and influence of institutional racism on health care access and utilization for racialized adolescents remains nascent. Future research is needed to better understand and to intervene on the impacts of racism on health care systems, including adolescent health services. Furthermore, to adequately address the instances of interpersonal racism documented in this review, greater attention to identifying and examining the degree to which institutional racism shapes health care providers’ interpersonal racism in service delivery is warranted.
Given the importance of racial bias, strategies such as anti-racism training may be useful to explore in addressing racial bias among health care providers. Additionally, anti-racism initiatives that consider the context of care and the experiences of specific racialized groups may be particularly promising. For example, racism may affect care differently for Black adolescents in the United States compared to Indigenous youth in New Zealand. Delgado and Stefancic 80 highlight the concept of differential racialization in the study of race and racism. In this perspective, Delgado and Stefancic 80 emphasize that various racial groups experience different origins, struggles, and histories of racism according to shifts in societal interests over time. Exploring the unique experiences of racism also necessitates understanding the contexts within which racism occurs. The majority of the articles in this review were conducted in the United States. It will be valuable for future research to explore how these experiences may differ across geopolitical borders. The foci and gaps in the existing literature base speak to the need for future research to account for context and nuance in the study of racism and adolescent health.
Limitations
There are two main limitations in this study. Critical appraisals of the individual studies were not conducted in this review; therefore, the strength of relationships across study outcomes was not reported. Future research in this field may consider conducting a systematic review to identify and explore the strength and significance of associations between racism and health care access and utilization across the existing literature base. While this review included records published globally and without restrictions to language, only articles in the English language were included in the final review due to feasibility reasons; three articles written in French and Portuguese were excluded.
Conclusion
The findings of this scoping review delineate the characteristics and foci of the literature on racism and health services for adolescents. The review provides evidence to support further study of racism as a determinant of adolescent health through its role in shaping health services and systems. To increase understanding of the pathways by which racism affects health services and to guide the development of evidence-based strategies for intervening on these pathways, there is a need for studies that investigate multiple forms of racism (institutional, interpersonal, internalized) and that incorporate robust measures of these forms of racism in relation to specific contexts and adolescent populations.
Supplemental Material
sj-docx-1-joh-10.1177_27551938231162560 - Supplemental material for Racism in Health Services for Adolescents: A Scoping Review
Supplemental material, sj-docx-1-joh-10.1177_27551938231162560 for Racism in Health Services for Adolescents: A Scoping Review by Carla Hilario, Samantha Louie-Poon, Mischa Taylor, Gurjeet K. Gill and Megan Kennedy in International Journal of Social Determinants of Health and Health Services
Supplemental Material
sj-docx-2-joh-10.1177_27551938231162560 - Supplemental material for Racism in Health Services for Adolescents: A Scoping Review
Supplemental material, sj-docx-2-joh-10.1177_27551938231162560 for Racism in Health Services for Adolescents: A Scoping Review by Carla Hilario, Samantha Louie-Poon, Mischa Taylor, Gurjeet K. Gill and Megan Kennedy in International Journal of Social Determinants of Health and Health Services
Supplemental Material
sj-docx-3-joh-10.1177_27551938231162560 - Supplemental material for Racism in Health Services for Adolescents: A Scoping Review
Supplemental material, sj-docx-3-joh-10.1177_27551938231162560 for Racism in Health Services for Adolescents: A Scoping Review by Carla Hilario, Samantha Louie-Poon, Mischa Taylor, Gurjeet K. Gill and Megan Kennedy in International Journal of Social Determinants of Health and Health Services
Supplemental Material
sj-docx-4-joh-10.1177_27551938231162560 - Supplemental material for Racism in Health Services for Adolescents: A Scoping Review
Supplemental material, sj-docx-4-joh-10.1177_27551938231162560 for Racism in Health Services for Adolescents: A Scoping Review by Carla Hilario, Samantha Louie-Poon, Mischa Taylor, Gurjeet K. Gill and Megan Kennedy in International Journal of Social Determinants of Health and Health Services
Footnotes
Acknowledgments
This research was supported by an internal grant from the Intersections of Gender Signature Area at the University of Alberta.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Intersections of Gender University of Alberta (grant number UOFAB VPRSF Hilario).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.