
Abstract
A dramatic increase in the volume of research literature referencing social determinants of health (SDH) since the report of the World Health Organization Commission on the topic in 2008 has not been matched by expansion of policies and interventions to reduce health inequalities by way of SDH. This article argues that familiar hierarchies of evidence that privilege clinical epidemiology as used in evidence-based medicine are inappropriate to address SDH. They misunderstand both the range of relevant evidence and the value-based nature of standards of proof. A richer conceptual armamentarium is available; it includes several applications of the concepts of epidemiological worlds and the lifecourse, which are explained in the article. A more appropriate evidentiary approach to SDH and health inequalities requires “downing the master's tools,” to adapt Audre Lorde's phrase, and instead applying a multidisciplinary approach to assessing the evidence that adequately reflects the complexity of the relevant causal pathways. Doing so is made more difficult by the power structures that shape research priorities, yet it is essential.
The late poet and essayist Audre Lorde is probably best known for the observation that “the master's tools will never dismantle the master's house”, 1 delivered at a 1979 conference on feminist perspectives in humanities. Drawing on the historical imagery of slavery and its after-effects in the United States, she went on to say that the master's tools “may allow us temporarily to beat him at his own game, but they will never enable us to bring about genuine change.” Altogether too many researchers investigating the origins of health inequalities by way of the social determinants of health have been using the master's tools, with results that Lorde might have predicted. The connection to politics and power implied by the reference to the master's tools is explicated in the final section of the article.
The 2008 report of the World Health Organization's Commission on Social Determinants of Health attributed health inequalities to the “toxic combination of poor social policies and programs, unfair economic arrangements, and bad politics”2(Executive Summary)—language that is not often encountered in United Nations system documents. Since then, references to the term “social determinants of health” have multiplied in the scientific literature (Figure 1). Research interest has not, so far, been translated into effective policies and interventions. Political scientist Julia Lynch 3 (p656) observed in 2017 that “systematic efforts to reduce inequalities in the ‘fundamental causes’ of health have been vanishingly rare”; 1 the intervening years have seen little change in the situation. Although the underlying politics are complex, and well explored by Lynch 5 and others, an important explanatory variable arguably relates to the increasing insistence that health policy, and indeed public policy in general, must be evidence-based. Superficially, it is hard to disagree with this proposition, but the dominant interpretation of what it means for population health is derived from the movement toward evidence-based medical practice, which strongly privileges the methods of clinical epidemiology. Specifically, hierarchies of evidence with multiple randomized controlled trials (RCTs) at the top are routinely applied to the research literature, setting a formidably high standard of proof (the decision about how much evidence, and what kinds of evidence, are sufficient to support a particular course of action) and—unexceptionably in the case of many clinical interventions—controlling for all but one variable. When RCTs are not possible, emulation is seen as the best strategy: “Trials have their own limitations … but attempting to mimic the randomised trial one would hypothetically conduct to answer an important question would seem to be a good place to start” 6 (p797).
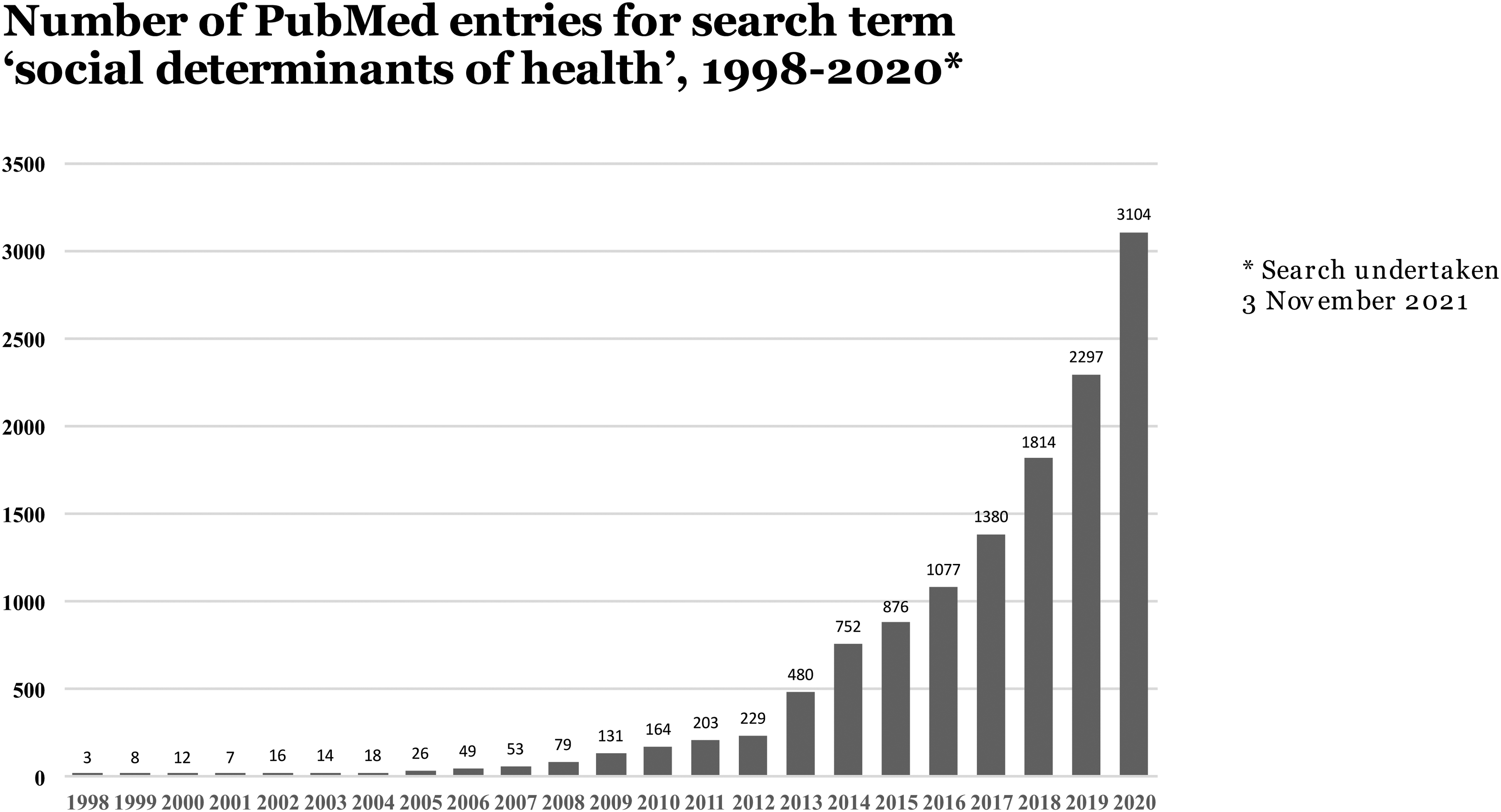
Increased frequency of references to social determinants of health in PubMed indexed literature, 1998–2020.
Other observers regard this approach as fundamentally misguided, functioning as an enabler of inaction through “epidemiological inertia”. 7 Sir Michael Marmot, who chaired the Commission on Social Determinants of Health, wrote with a colleague when the Commission's report was published: “If … you think the only evidence worth considering is that from randomised controlled trials, you can happily save time by not reading our report. …. It will not take long to assemble all the randomised controlled trials of the health effects of income redistribution in sub-Saharan Africa; or to conduct a systematic review of the effects on health equity of social protection mechanisms in Latin America; or the effect of trade agreements on life expectancy in low-income countries” 8 (p1096). In rich countries and poor alike, the health effects of macro-level policy choices and directions operate through multiple causal pathways, over long time periods, in contexts that are far too complex to be reduced to the tidiness of RCTs.
Recognition of that complexity is exemplified by the system maps (diagrams of causal pathways) around which the important 2007 United Kingdom Foresight study of influences on obesity9,10 was organized, and obesity is used as an illustrative example at several points in this article. At the core of the basic full system map is a central “engine” consisting of three feedback loops involving energy balance. Around that central engine are mapped literally dozens of influences that operate through feedback loops both positive and negative. The report organized these influences into seven thematic clusters: physiology, individual activity, physical activity, food consumption, food production, individual psychology, and social psychology. 10 (Unfortunately, the full system map is far too complex to reproduce legibly at the scale possible here.) Variations on these maps illustrate, among other things, the strength of particular influences and the importance of considering separately for purposes of public health interventions the distinctive influences on the health of specific subpopulations such as children. A succinct statement of the consequences of such complexity for health inequalities policy is provided by David Byrne, a specialist in the study of complex systems: “If policy makers want to know how a complex social world works then one thing is as sure as the fact that the sun rises in the morning—experimental approaches in general and randomised controlled trials (RCTs) in particular are about as much practical use in providing that information as is a chocolate teapot for holding tea”. 11 (p44).
In considering such bodies of evidence, the choice of a standard of proof is not one that can be made on scientific grounds. This point has been articulated in literally decades of policy analysis on environmental issues12–15(Chapter 4). The best available scientific evidence 2 is obviously important, with appropriate recognition of uncertainties, but decisions about how to weight those uncertainties must be made (and if necessary contested) on the basis of the objectives that policy should be designed to advance. 19 “[S]ocieties regularly use different strengths of evidence for different purposes” and: “Choosing an appropriate strength of evidence for specific cases of potential hazards necessarily involves … trade offs between the consequences of being wrong in ‘establishing’ or ‘not establishing’ cause and effect” 13 (p262). Failure to acknowledge the omnipresence of this decision point in policy perpetuates the idea that too little is known about the causes of health inequalities and lends unjustified credibility to a fatalistic view that nothing works.
So, What to do? A Richer Conceptual Armamentarium for Studying Health Inequalities
The case for “diversifying the evidence base” for action on social determinants of health has been made by Marmot and Friel 8 (p1096) and many other authors. But what kinds of evidence are available? This core section of the article provides support for the argument of progressive health researchers 20 (p2) who, without referring to epidemiological inertia, state that “when the broader canon of evidence from the social sciences is included it provides a rationale for clear causal inference and policy action.” Considering this broader canon of evidence can provide a high-level roadmap to various concepts, literatures, and repertoires of research design that, taken together, can provide a compelling case for action on social determinants of health. Key examples of this broader canon are grouped here into two conceptual clusters: epidemiological worlds and lifecourse studies and perspectives. Most examples used here are from the Anglo-American contexts with which I am most familiar, but the insights into the causal mechanisms of health inequalities that they illustrate are broadly applicable. They are intended to lead to debate and evidence synthesis using more diverse cases, and as a side benefit to demonstrate the error of many researchers’ (and journals’) tendency to treat “theory” as a synonym for opinion or commentary. Theory is essential intellectual scaffolding for the responsible conduct of research and a fortiori for the development of policies and interventions although, as attested to by the transition over time in the focus of Nancy Krieger's work,21,22 it cannot be just epidemiologic theory.
Epidemiological Worlds: Overview
The authors of a review article on urban environments and health 23 (p2079) wrote: “Rich and poor people live in very different epidemiological worlds, even within the same city.” However, they did not further theorize the concept, proceeding instead to a rather unimaginative exploration of various exposures and vulnerabilities related to urban planning decisions and infrastructure. The ensuing decade has not seen much analytical improvement, although many rich additions to an already substantial accumulation of empirical data about the metropolitan context. Notably, geographer Liam McGuire used cluster analysis of data across six domains to map no fewer than 10 distinct “cities” within Canada's Greater Toronto Area, with a population of roughly 6 million.24–26 These are collections of small areas (census tracts) that are often not contiguous but comprise distinctive epidemiological worlds defined by such criteria as income, housing characteristics and affordability, household composition, occupation, immigration status, education, and commuting patterns. In an unrelated but complementary micro-level qualitative study of one Toronto neighborhood, sociologist Laura Bisaillon and colleagues 27 identified the multiple elements of stratification associated with “being from a bad [impoverished, inner city] neighbourhood,” which is now exposed to gentrification pressures like almost all of central Toronto. These illustrations of how place matters for health are portals for further exploration; some of the connections with health outcomes are obvious, others less so.
This point is underscored and illuminated by the extensive environmental justice literature on ambient pollution exposures, 28 but also by such relations as those between (un-) healthy diet and residence in areas that have been characterized as food deserts, where sources of healthy foods are absent or inaccessible 29 ; food swamps, where unhealthy food options such as convenience stores and fast food outlets predominate 30 ; and food mirages, where healthy options may be accessible but unaffordable. 31 Some reviews find evidence of the impact of such place-based factors on diet, overweight/obesity, and such outcomes as diabetes to be equivocal 32 (but cf. 33 ). However, a valuable critical review related to diabetes pointed out the limitations of “over-simplistic definition of ‘exposure,’ ignoring other environmental attributes like the social environment; the focus on the residential neighbourhood only, not accounting for exposure to the food environment at work or in transit, and the lack of insight into individuals’ behavioral interactions with the food environment” 34 (p.266). Thus, the epidemiological worlds concept is much more than an argument for place-based explanations of health inequalities, as important as these are.
To understand this last point, consider the innovative “geo-ethnography” in which geographers 35 combined GPS tracking of participants with diaries of daily activity. They documented the journeys among home, nursery, school, work, and other necessary activities such as grocery shopping of lone mothers of young children in three U.S. cities, usually reliant on public transport, who had been forced into the predominantly low-wage, service-sector workforce by U.S. President Clinton's 1996 welfare cutbacks.36,37 The journey of two hours or more shown in Figure 2, which must be a composite because an actual journey might enable identification of the participant, presupposes: (a) the availability of public transport that runs on schedule, which is uncertain at best in much of North America, 3 and (b) a job with predictable and stable hours, which is far from the norm in a service sector characterized by growing precarity. It is useful to consider how such space-time trajectories affect the possibilities for such desiderata as healthy eating: Not only place and budget matter, but also time.
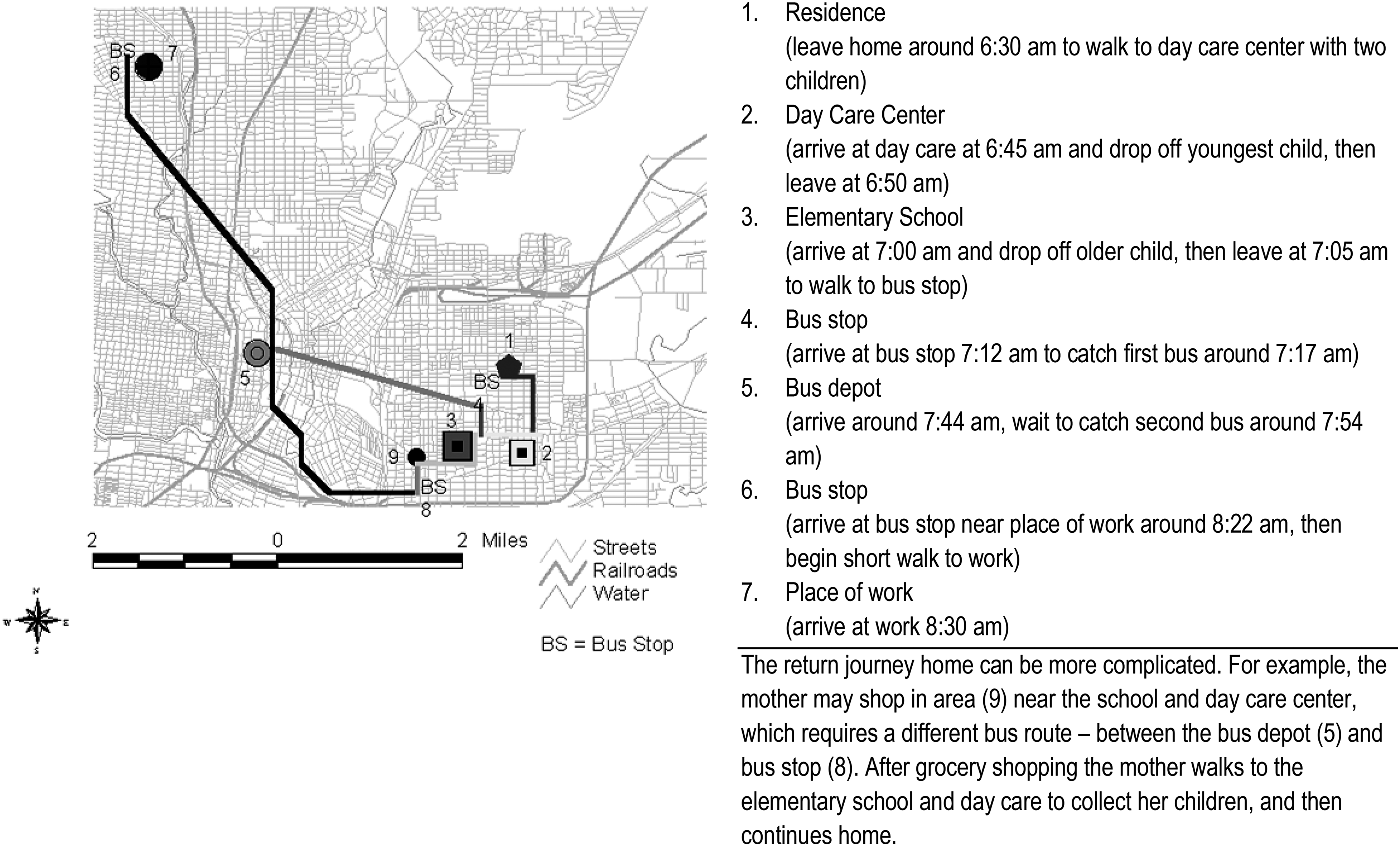
“Geo-ethnography” of a lone mother's hypothetical weekday journey to work in San Antonio, Texas (time two hours one way). Reproduced with permission from University of Toronto Press (https://utpjournals.press) from Matthews SA, Detwiler JE, Burton LM. Geo-ethnography: Coupling Geographic Information Analysis Techniques with Ethnographic Methods in Urban Research. Cartographica: The International Journal for Geographic Information and Geovisualization 2005;40:75–90; doi:10.3138/2288-1450-W061-R664. Copyright © University of Toronto Press.
In a related illustration, consider the epidemiological worlds described by Barbara Ehrenreich,39,40 an accomplished academic and journalist who went undercover with an imaginary, limited résumé in search of the kinds of jobs literally millions of women had to seek after the 1996 reforms. Employment conditions and precarity and housing availability and costs figure prominently in Ehrenreich's account, as they should for anyone serious about understanding health inequalities. Professional readers with relatively secure jobs may wish to consider the contrasts; readers in the expanding ranks of precariously employed instructors and research associates may wish to consider the similarities. Epidemiological worlds, then, are not only about places and their associated exposures and vulnerabilities, but also about how people live in and move among those places, and the resources that are (or are not) available to them as they do so.
Epidemiological Worlds: Intersectionality and Overdetermination
The concept of intersectionality originated in work by African-American legal scholar Kimberle Crenshaw 41 on the inadequacy of anti-discrimination doctrines that focused on race or sex, but not on the interaction of the two. Its contemporary relevance for health inequalities research is described by Kapilashrami and Hankivsky, two leading exponents of the concept 42 (p2589): Intersectionality “moves beyond examining individual factors such as biology, socioeconomic status, sex, gender, and race. Instead, it focusses on the relationships and interactions between such factors, and across multiple levels of society, to determine how health is shaped across population groups and geographical contexts.” Crenshaw herself observed recently that African-American women killed by U.S. police tend to be invisible, relative to African-American men, by virtue of the intersection of their race and gender. 43 Differential responses by European countries to refugees and asylum seekers depending on their country of origin are an example cited by Kapilashrami and Hankivsky; the treatment of Ukrainian as contrasted with Middle Eastern and North African refugees in the United Kingdom has dramatized such differences. As with the epidemiological worlds concept as a whole, the core axiom is that in the real lives of real people, perhaps in particular those navigating adversity, many things that affect their opportunities (or lack thereof) to lead healthy lives are going on at once. Health inequalities researchers and those designing policies and interventions to reduce them need urgently to take this on board.
In this vein, a key challenge involves multiple sufficient causes of ill health, the importance of which has been described as follows: “Isolating social causes of disease” can be complicated “because some groups may be so disadvantaged that alleviating one adversity will not be enough to enable them to achieve good health. The bad health outcomes are ‘overdetermined’ by multiple, sufficient causes of disease” 44 (p27). Underscoring the limitations of research designs that control for all but a single variable, the cited authors point out that: “In a counterfactual analysis, removing only one of the sufficient causes would suggest that it was not a ‘cause’ at all, because the disease outcomes did not change … [C]hanging this one factor is not enough to improve health.” In an illustration that I have used to good effect in teaching, a case report on obesity in a five-year-old Mexican girl that is laudably attentive to social determinants of health 45 identifies multiple contributing factors including limited exercise time in school, unsafe conditions in available exercise spaces near the family's home, five hours of daily screen time, and excessive caloric intake associated with a corporate-driven nutrition transition that has been especially rapid in Mexico. Affordability of a healthy diet was not identified as a concern by the parents, although this would be a concern to literally billions of people worldwide 46 (Chapter 3). Most of the variables identified connect to macro-scale social conditions, and it is questionable whether a change in any single variable would lead to meaningful health improvement, on either an individual or a population basis. Coordinated intervention across multiple policy fields would be required—a kind of initiative that is usually impossible to assess by way of experimental or quasi-experimental methods, for both ethical and logistical reasons, even if necessary political and financial support could be mobilized.
Another example is provided by systemic or structural racism directed against African-Americans in the United States. 47 African-American men are imprisoned at a rate six times higher than white men. 48 The authors of a comprehensive inventory of the direct and indirect public health effects miss the point about multiple sufficient causes by arguing that: “Research into interventions, policies and practices that could mitigate the harms of incarceration and the post-incarceration period is urgently needed, particularly studies using rigorous experimental or quasi-experimental designs” 49 (p1464). Like hypothetical interventions addressing a single variable in the Mexican case, such interventions would not necessarily be without positive effect, but their effects are likely to be modest unless embedded in a larger effort to address underlying inequalities. Hyperincarceration of African-Americans is just one part of a much larger and darker picture, including a dramatic climb in overall incarceration prevalence relative to other purported democracies starting in the 1970s 47 (and, for extensive additional background, 50 ) and an historical background dating back to the Jim Crow era of attempting to re-establish an economic order predicated on the subjugation of African-Americans.47,51 Thus, the need is for “transforming and dismantling the policies and institutions that undergird the U.S. racial hierarchy” 47 (p. 768). Contemplating an experimental or quasi-experimental research design that would address this imperative demonstrates the salience of Byrne's point about chocolate teapots.
Epidemiological Worlds: Syndemicity
The concept of a syndemic was developed by medical anthropologist Merrill Singer52,53 in a long-term study of health outcomes in a deprived U.S. urban Hispanic neighborhood. Singer referred to a syndemic of
“Syndemics theory unites three core features. First, two or more diseases cluster together within a population—often this relationship is well documented epidemiologically, although often described as comorbidity or multimorbidity. Second, there is some type of biological, social, and/or psychological interaction of those diseases … Third, there are recognisable large-scale social forces that precipitate disease clustering in the first place,” reflecting macro-level social inequalities 56 (pp,213–214). For example, early data from the COVID-19 pandemic in Montréal, Canada, showed a clustering of cases in districts with the lowest median incomes and the highest proportion of residents self-identifying as Black, which tend to be the same places. 59 As in other similar contexts,60,61 the vulnerabilities in question are likely to have included front-line occupations involving disproportionate risks of exposure (e.g., in care homes or essential retail), unemployment (e.g., in hospitality) or both; heavy reliance on public transportation; and crowded housing conditions.
In addition to underscoring the important of overdetermination and multicausality, much syndemics research relies heavily on qualitative (interview-based, ethnographic) data to aid understanding of what philosopher of science Jon Elster 62 has called the texture of everyday life in situations of multiple, often interacting forms of deprivation and subordination. The concept of syndemicity thereby draws attention to the need for “multi-layered, multi-pronged and multi-sector responses as well as an assessment of the sociopolitical dynamics of health that promote disease clustering and interaction” 63 (p952). Contemporary population health research and policy are generally ill equipped to offer such interventions and perspectives, demonstrating the subversive importance of the syndemic concept.
Epidemiological Worlds: Risk Contagion
Political scientist Jacob Hacker 64 has described “the great risk shift” in U.S. public policy, as labor market changes and welfare state retrenchment combined to increase economic insecurity and to shift responsibility for dealing with it from employers and governments to individuals and households. Risk has been privatized, 65 as it has been to some degree in almost all high-income countries in parallel with economic globalization and neoliberalization (see 66 , and 67(Part A), among many other sources). A further dimension of this process, with special importance for population health, has been termed risk contagion: the process in which “risks amplify as they spill from one domain into another. Risk contagion captures the idea that risks stemming from one dimension are compounded when they trigger contingent risks in another dimension” 68 (p299). The paradigmatic example is the loss of access to health care and increased risk of illness-related downward mobility and financial hardship that are associated with job loss in the United States, with its distinctive reliance on employer-paid health insurance.
Countries, and in some cases sub-national jurisdictions, vary widely in the extent to which their policies and institutions work against risk contagion. 68 As one of the most straightforward examples, many high-income countries provide health care free, or nearly free, at point of use. Differential vulnerability to risk contagion drives both variations among societies and stratification within societies, and the associated health inequalities, thereby providing a valuable foundation for identifying potential interventions. The COVID-19 pandemic foregrounded this point by way of differences in “baseline” entitlement to paid sick leave among Organisation for Economic Co-operation and Development countries, which over the short term varied from zero to 100% of previous earnings. 69 Actual variation was somewhat less dramatic, both because of entitlements associated with collective agreements rather than mandated by governments and because of ad hoc measures implemented during the pandemic, but in jurisdictions such as the United Kingdom, many low-paid and precariously employed workers fell through the cracks. Canada's largest province, Ontario, never did require employers to pay workers who fell ill with COVID-19 or were self-isolating after a positive test.
Women in most societies, if not all, are disproportionately vulnerable to contagious risks associated with economic insecurity, domestic violence, and the interaction of the two—a vulnerability that has been magnified in the context of the pandemic.70,71 As for the effects of racism, a U.S. campaigner against police violence said in the context of the COVID-19 pandemic: “There is danger lurking in every corner right now. We [African-Americans] are disproportionately dying from COVID-19, we are a disproportionate amount of frontline essential workers, we are a disproportionate amount of the people police are arresting due to social distancing regulations, we are obviously a disproportionate amount of people being killed by police, we are also being killed by vigilantes and threatened by white liberal women walking their dogs in Central Park”. 72 Here we glimpse the importance of risk contagion, syndemicity, overdetermination, and (often) intersectionality as conceptual lenses that should be used in combination to comprehend different epidemiological worlds, in particular those defined by multiple dimensions of deprivation and risk exposure.
Lifecourse Studies and Perspectives: Overview
Time matters, not only in people's daily experience but also over the longer course of their lives. Most simply, a lifecourse perspective “sees health state at any given point in life as a cumulative health profit-and-loss account” 73 (p96). Within the scope of this rather mechanistic formulation, considerable variation exists between “developmental” and “structural” perspectives, with the former emphasizing “critical and sensitive periods” and the latter focussing on “socially structured quantitatively and qualitatively different life experiences,” including those outside key developmental windows. 74 For purposes of this article, assessing the evidence for each perspective—and they should be viewed as complementary rather than competing—is less important than the general point that in “a socially partitioned world” 75 (p12.4), people accumulate over the course of their lives a variety of exposures, vulnerabilities, and opportunities that reflect the effects of partitioning. It is important to reject the fatalism that could be a consequence of a focus on early development; as important as it undoubtedly is, the temptation, especially in policy environments preoccupied with cost-effectiveness, may be to reduce the priority attached to policies and interventions aimed at compensating for negative effects of various forms of deprivation in the early years. In the extreme, such fatalism could manifest as “a model which says that ‘if they aren't okay by age 3, scrap them!’ …. What is needed instead is a pragmatic approach which draws upon the strength of each model” 76 (pp1087–1088).
One illustration of such a pragmatic approach is provided by the findings of a multidisciplinary research project (the Lifepath Consortium) organized around multiple lifecourse studies, which consistently demonstrated a health gradient related to socioeconomic position. 77 One of the Lifepath projects—a meta-analysis of cohort studies of 1.7 million people in high-income countries—found that low socioeconomic position, even using a crude, three-category, occupation-based measure, accounted for a reduction in years of life larger than hypertension, although smaller than lack of physical activity. 78 The limitations of the socioeconomic position measure, no doubt reflecting the limitations of the underlying data, mean this is likely to be an underestimate. The critical point is that socioeconomic position should be considered independently as a modifiable risk factor; “both socioeconomic adversity and 25 × 25 risk factors,” the cornerstone of the World Health Organization's largely individualized approach to preventing noncommunicable disease, “should be targeted by health strategies” 78 (p1234). A later Lifepath publication complemented the analysis of mortality data with “a biologically multi-layered approach,” including biological markers such as childhood obesity and a variety of blood biomarkers, similarly concluding that “socioeconomic disadvantage … is a determinant of poor health through biological embodiment beyond classic behavioural risk factors for non-communicable diseases” 79 (pp2,6).
Lifecourse Studies and Perspectives: The (Socio-)Exposome
The exposome concept originated as an advance in the epidemiology of chemical exposures in the natural environment, “complement[ing] the genome by providing a comprehensive description of lifelong exposure history” 80 (p24). Although some contemporary reviews maintain the focus on environmental epidemiology (e.g., 81 ), many others argue for a broad and inclusive definition of environmental exposures, including “the wider social, economic and psychological influences on the individual, for example: social capital, education, financial status, psychological and mental stress, urban-rural environment and climate” 80 (p24). The exposome can be thought of as a biological record of exposures over the lifecourse, and the broad definition of environment is what makes the exposome concept useful as a way of understanding how social disadvantage gets under our skin—what leading researchers describe as the “biography-to-biology transition” 82 (p1). Sociologists have therefore argued for the terminology of the socioexposome as a way of avoiding the tendency to “molecularise complex social phenomena” 83 (p107) that result from macro-scale inequalities and exercises of power.
A recent review 84 argued the importance of an exposome perspective, with the relevant exposures including endocrine-disrupting chemicals, in explaining the widespread increase in obesity. Also relevant are demonstrations that aspects of social advantage and disadvantage (the external exposome) can affect biological responses to fast food meals. “Thus, even if an individual living in affluent Bel-Air, Los Angeles, eats food from a multinational fast-food outlet at the same per-week frequency as a low-income individual from South Los Angeles, the biological buffering of those meals will almost certainly differ” 85 ( p329). Fast food is a key element of dietary transitions to high levels of ultra-processed food, which are implicated in rising overweight and obesity rates. 86 It will be interesting to see whether future research supports the hypothesis that the aspects of the external exposome related to social disadvantage affect biological responses in other contexts—for instance, the roughly half of all household food purchases in Ireland, Germany, and the United Kingdom (excluding restaurant purchases) that were found to consist of ultra-processed foods in a European study. 87
Lifecourse Studies and Perspectives: Stress, Allostatic Load, and Weathering
The physiology of responses to chronic stress, an exposure that is (like many others) unequally distributed across populations, is central to many exposome studies of biography-to-biology transitions, although much of the relevant science actually predates the widespread diffusion of the exposome concept. Stress gets under our skin in multiple ways that affect health. 4 Most simply stated, the fight-or-flight response that reflects successful evolutionary adaptation to threatening situations becomes maladaptive when the threat is prolonged or repetitive, as with the multiple stressors associated with poverty. 90 Allostasis refers to the process of adaptation during such exposures, and allostatic load refers to the wear-and-tear resulting over time from such repeated adaptation. It is usually measured using multiple biomarkers, which can be aggregated to generate a single allostatic load score. 92 A body of research too large to review here shows an association between higher allostatic load and a variety of variables, including not only position within social hierarchies and psychological adversity in childhood 93 but also such material factors as living in a deprived neighborhood. 94 Notably, one of the Lifepath studies, of a British cohort, found that “higher allostatic load at 44 years old was a significant predictor of mortality 11 years later,” reflecting “early-life socio-economic position, adverse childhood experiences and young adulthood health status” 79 (p6).
“Weathering” is a term that originally referred to “the cumulative impact of repeated experience with social or economic adversity and political marginalisation” among African-Americans 95 (p826). The quoted study used an index of allostatic load based on national survey data to assess the interacting physiological effects of being Black, female, and poor. An elegant demonstration of how to tell a lifecourse story using cross-sectional data, it found that probability of a high allostatic load, as calculated from risk thresholds for each of 10 biomarkers, increased with age for all groups, with higher scores among women, people living below a poverty threshold, and Black people. “In each age group the mean score for Blacks was roughly comparable to that for Whites who were 10 years older” 95 (p831). The effects of weathering are among three mechanisms by which structural racism was argued to “operate as a fundamental cause” of higher COVID-19 burdens among older African-American and Latinx adults in the United States—a consequence of their lifelong exposure to structural racism's manifestations interacting with other, material factors. 96 However, weathering has applications to many populations other than those affected by racism in the United States: Accumulated adversities mean that the exposed populations “put miles on the clock more quickly than other people,” as I once heard a workshop participant describe the process. Stated simply, social disadvantage—in particular, the experience of multiple forms of social disadvantage 97 —wears people out over time in biologically measurable ways.
Are such measures as allostatic load scores needed before taking action to remedy social disadvantages that affect particular populations, such as (to give just one example) successive generations in an urban district in Scotland ravaged first by deindustrialization and then by selective austerity 98 ? One should hope not. 89 Rather, research that addresses phenomena at the level of individual bodies, or even individual molecules, contributes to understandings of mechanism that often are arguably as comprehensive as those related to many pathogens, although the mechanisms are more complicated and multicausal. Such evidence must be considered in combination with what is known from social science about macro-level trends like those shaping nutrition transitions and rising economic insecurity. Where there are gaps in the evidence base, and there will almost always be such gaps, the question becomes one of choice of a standard of proof, as noted earlier.
Why “the Master's Tools”: The Politics of Evidence and Method
The inventory of concepts, literatures, and repertoires provided here is not exhaustive, and none is a magic bullet for understanding where health inequalities come from and how to reduce them. As suggested by the example of the obesity system map, they represent elements of an explanatory narrative that must be combined as appropriate to the relevant context. For example, anthropologist David Himmelgreen and colleagues 99 propose a combination of syndemicity and lifecourse theoretical perspectives for investigating the relation between food insecurity and diet-related chronic diseases. Given what is known about the influence of environment, broadly defined, on responses to diet, 85 it would be useful to incorporate the concept of the exposome into such research designs. Recognizing the importance of “methodologic pluralism”, 100 the need is therefore for a non-hierarchical “portfolio of evidence” 101 that draws on findings from multiple disciplines, which are quality controlled using the criteria that are appropriate to those disciplines rather than according to criteria specific to the single discipline of clinical epidemiology. Rather than guarding against bias, hierarchies of evidence organized around RCTs or approximations of them actually introduce bias: “[C]hoosing certain research strategies and standards of proof means the big questions …. probably will not be studied in ways that demonstrate the effectiveness of larger-scale, contextual interventions, and even the small questions will be asked in ways that seriously circumscribe the set of possible answers” 102 (p1682). As an alternative to the systematic reviews that are a mainstay of the evidence-based medicine movement, the method of realist review 103 and its later refinement as narrative review—“a scholarly summary along with interpretation and critique” 104 (p2)—should be the preferred approach to synthesis.
To return to the example of obesity, in many high-income countries, it exhibits a pronounced socioeconomic gradient. Indicating the extent of the problem, in England both children 105 and adults 106 living in the most deprived decile of small local areas are twice as likely to be obese as those living in the least deprived decile. The prevalence of obesity more than doubles during the first six years of schooling and the gradient becomes steeper. Obesity's multiple negative health consequences make it an important contributor to the overall burden of health inequalities. The complex range of causal pathways implicated in rising obesity levels10,84 indicates a need not only for direct redistribution of resources, to ensure affordability of healthy diets, 107 but also for initiatives including regulating or restructuring highly profitable and powerful enterprises in the food, beverage, and restaurant industries108,109 and changing planning priorities to render built environments more activity-friendly. All this will require “tackl[ing] the inequitable distribution of power, money and resources”—one of the three principles of action that were identified by the Commission on Social Determinants of Health.
Hierarchies of evidence and standards of proof drawn from clinical epidemiology are the master's tools when they serve the interests of beneficiaries and defenders of those unequal distributions, by providing apparently convincing evidence that not enough is known about how to reduce health inequalities. This disregards the value-driven nature of the choice of standards of proof and is deceptive in the same way that claims to be following the science were deceptive in the context of the COVID-19 pandemic; the relevant science in fact involved a plurality of methods, which could be and were cherry-picked, as in the case of face coverings. 110 What accounts for the continued prevalence of such methods and perspectives in population health research? “Biomedical individualism” 111 that is inimical to multidisciplinary, system-level understandings of health outcomes tends to dominate the environments in which such research takes place, but that dominance demands explanation even while providing it. Immediately after David Byrne's observation about chocolate teapots, he continued: “A second and cynical level of understanding might reflect on the fact that in many circumstances the last thing policy makers want is a truthful and accurate account of how a complex social world works so methods which utterly fail to provide that account may have considerable value after all” 11 (p44).
In further exploring this question, it is important to heed Elster's warnings about the difficulties of explaining social phenomena with reference to the interests of their beneficiaries—that is, of functional explanations. Elster argued that most such explanations fail in social science because of the lack of a demonstrable feedback loop between outcomes and antecedent conditions analogous to that provided by natural selection. 5 In other words, the fact that a particular phenomenon has benefits for the rich and powerful, however one defines them, does not explain its survival and persistence; more is needed. In this case, most individuals working within organizations such as universities adapt with striking facility to the conditions that influence who succeeds and advances—and those conditions often reflect incentives or reinforcements generated by external actors. When those external actors are concerned to defend existing interests and distributions, the effect is to provide a plausible account of the feedback loops that Elster considers essential, although the mechanism of selection is artificial rather than natural.
Katherine Smith's114,115 important interview-based documentation of how funding agencies in the United Kingdom shape researchers’ priorities, and the extent to which researchers engage in self-censorship in order to preserve their relationships with funders and state agencies, is a case in point from a jurisdiction where securing external funding is often critical to careers. 6 A “senior academic” interviewed by Smith commented: “You run yourself like a small business. […] I say the ESRC [Economic and Social Research Council] and the MRC [Medical Research Council] are my bosses – they are effectively … I have to watch what they want, I have to fulfill their expectations … I have to live up to whatever they ask me to do”114(p159, ellipses in original). As an illustration of how this process can operate, in early 2022, it was reported that a Conservative Cabinet secretary had vetoed a potential candidate for the executive chairmanship of the ESRC, the government agency that funds social science research, on political grounds. 120 So when funding agencies are captives of biomedical individualism, indifferent or hostile to macro-scale changes of the kind envisioned by the Commission on Social Determinants of Health, or commanded by government ministers or foundation trustees, those priorities shape the direction of research. As such mechanisms elevate into positions of power within research institutions those individuals and specialisms whose priorities are congruent with external demands, they affect the career trajectories of early-career researchers and indeed the content of curricula, thus completing the feedback loop and having an intergenerational impact.
Much more can and should be said about the politics of knowledge production in population health (cf. 121 ), a field of study that unfortunately remains terra incognita to many population health researchers. It would be interesting, for example, to continue with the obesity example by way of qualitative research on the experiences of investigators who have tried to adopt and promote whole-system approaches to addressing the inequality dimensions of obesity. Such observations in turn need to be situated with reference to a broader policy environment that is, in most of the world where population health research takes place, relentlessly hostile to the broadly egalitarian policy agendas implied by taking seriously the reduction of health inequalities.5,122,123 Anthropologist Kaveri Qureshi's 124 ethnography of health inequalities policy in the United Kingdom's New Labour government underscores the extent to which this can be true even of nominally left-of-center governments, as does the complete elision at this writing (early 2023) of health inequalities from the policy agenda of Britain's Labour party, now in opposition. Downing the master's tools will encounter formidable challenges within the research enterprise, as elsewhere. Doing so in both research and policy analysis is nevertheless necessary to change the discourses and priorities of multiple research domains and policy fields in order to make them more receptive to meaningful reductions in health inequalities, but it will not be sufficient. Against a background of rising economic inequality that threatens potentially irreversible changes to the political terrain throughout much of the world, even in the shrinking universe of formally democratic polities, positive outcomes are uncertain at best.
Footnotes
Acknowledgements
I am grateful to the postgraduate students in my Newcastle University module on Advanced Social Determinants of Health for many discussions that sharpened the analysis presented here, and to my colleague Duika Burges Watson for alerting me to the importance of the exposome concept.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and authorship of this article. Funding for open access publication was provided by Newcastle University.