
Abstract
Background:
Diarrhea is a significant global health concern, particularly among children, and its impact is particularly pronounced in countries with limited resources and ongoing conflicts, such as Yemen. Diarrheal diseases remain one of the leading causes of morbidity and mortality in children under the age of 5 years worldwide.
Objectives:
The aim of our study is to assess the treatment patterns and counseling of community pharmacists regarding the management of acute diarrhea in children in Yemen.
Design:
A simulation-based cross-sectional study was carried out targeting community pharmacy professionals in Sana’a city.
Methods:
A questionnaire and simulated client methods were used to assess the pharmacists’ evaluation of a case based on five indicators including the child’s age, diarrhea frequency, presence of fever, and blood or mucus. In addition, the pharmacists’ recommendations and counseling were also evaluated.
Results:
During the study, a total of 100 pharmacists were visited and evaluated using both a questionnaire and simulation. The results demonstrated that 43.0% of the pharmacists utilized all five indicators in the questionnaire, with a mere 3.0% using all five indicators in the simulation. Oral rehydration solution (ORS) alone was recommended by 42.0% of the pharmacists and in combination with other drugs by 47.0% in the questionnaire, and the rest (11.0%) recommended only other drugs; while in the simulation, 7.0% of the pharmacists referred the patients to clinic, only 6.0% recommended ORS alone, 47.0% gave ORS plus other drugs including antibiotics, and 40.0% dispensed only antibiotics. In regards to counseling, 89.0% of pharmacists reported that they would explain to the patient regarding the recommended medicine during the questionnaire, and only 36.0% gave any sort of explanation to the simulated client.
Conclusion:
In the current study, community pharmacists did not ask enough questions to accurately evaluate a child with acute diarrhea during the simulation. This finding has apparently differed from their responses in the questionnaire. Furthermore, the pharmacists failed to provide sufficient dietary advice, and their recommendation of ORS was inadequate.
Plain language summary
Diarrhea is a common health issue, especially among children, and it can have severe consequences, particularly in countries like Yemen. We conducted a study to assess how community pharmacists in Yemen manage and counsel on acute diarrhea in children. We used questionnaires and simulated client visits to evaluate their practices. We visited and evaluated 100 pharmacists, using both questionnaires and simulated client visits. The results showed that only 3% of pharmacists used all five indicators to assess the case during the simulated visits, compared to 43% who used all indicators in the questionnaire. When it came to treatment recommendations, 42% of pharmacists suggested using oral rehydration solution (ORS) alone, while 47% recommended ORS along with other medications in the questionnaire. However, during the simulated visits, only 6% recommended ORS alone, and 47% prescribed ORS with additional antibiotics. In addition, 40% of pharmacists solely dispensed antibiotics. Regarding counseling, 89% of pharmacists reported that they would explain the recommended medicine during the questionnaire, but only 36% provided any explanation to the simulated clients. Our study revealed that community pharmacists in Yemen did not ask enough questions or provide adequate dietary advice during simulated client visits for acute diarrhea. This differed from their responses in the questionnaires. Moreover, their recommendation of ORS was insufficient. These findings highlight the need for improved training and guidance for community pharmacists in Yemen regarding the management and counseling of acute diarrhea in children.
Keywords
Introduction
Diarrhea is a significant global health concern, particularly among children, and its impact is particularly pronounced in countries with limited resources and ongoing conflicts, such as Yemen. Diarrheal diseases remain one of the leading causes of morbidity and mortality in children under the age of 5 years worldwide. 1 Diarrhea in children is characterized by loose or watery stools occurring three or more times per day and can be classified into three subtypes: acute watery diarrhea, acute bloody diarrhea, and persistent diarrhea. 2 The main objective in managing acute watery diarrhea is to prevent and treat dehydration. Children in Europe under 3 years of age experience 0.5 to 2 instances of acute diarrhea per child every year, 3 while those in developing countries experience an average of three episodes annually. 2 The causative organism of acute diarrhea in children can be viral, bacterial, or protozoal,2,4,5 with viruses being the primary cause in most cases. Infection is often acquired directly from another infected person or through the consumption of contaminated food or water.
In terms of viral pathogens, while Rotaviruses were previously considered the primary causative agents, noroviruses have emerged as significant viral pathogens and are now recognized as the predominant cause of nonbacterial gastroenteritis globally. Rotavirus infection accounts for 20%–60% of all diarrheal cases in both developing and developed nations and remains the leading cause of acute diarrhea among children under the age of 5 years. 6 In developing nations, Rotavirus is the leading cause of severe gastroenteritis in young children. Recent conservative estimates reveal that approximately 702,000 children die each year from Rotavirus disease, with up to 85% of these deaths occurring in low-income countries. 7 Diarrheal disease caused by unsafe water and inadequate sanitation is the leading cause of morbidity and mortality among children under five worldwide, especially in impoverished nations. 8
According to the World Health Organization (WHO) and United Nations Children’s Emergency Fund (UNICEF), there are about two billion cases of diarrheal disease worldwide every year, and 1.9 million children younger than 5 years die from diarrhea each year, mostly in developing countries. 9 Globally, acute diarrhea is the second leading cause of death, following pneumonia. Both the incidence and the risk of mortality from diarrheal diseases are highest among children under the age of 5 years, especially during infancy, with rates gradually declining thereafter. 10
Currently, Yemen is ranked 41 out of 189 countries with the highest number of deaths among children under the age of 5 years, with diarrhea being a major contributor to Yemen’s high child mortality rate. Diarrheal diseases pose a significant threat to the population in Yemen, especially among children under the age of 5 years. They are the second most common disease in Yemen and account for approximately 17.0% of reported annual deaths in this age group. Moreover, around 55% of the Yemeni population lacks access to proper sanitation facilities and relies on unimproved water sources for drinking water. 11 Yemen is an economically poor country compared to its neighboring countries, experiencing issues of overcrowding and inadequate infrastructure. As a result of resource shortages and a lack of proper planning, the healthcare system in Yemen is greatly impacted, negatively affecting the health of children. 12
Many patients seek treatment for common ailments such as diarrhea from community pharmacies. 13 However, the quality of management provided by community pharmacists for acute diarrhea in children has raised concerns and has been the subject of numerous published studies. 14 - 16 To appropriately evaluate a child’s acute diarrhea, healthcare practitioners should ask several key questions, including the child’s age, frequency and duration of diarrhea, accompanying symptoms (e.g. fever, vomiting, blood in the stool), recent medical and medication history, and feeding status.3,17 Certain studies have reported that pharmacists may conduct inadequate or incomplete assessments when evaluating children with acute diarrhea.15,16,18
WHO recommends the use of low-osmolarity oral rehydration solution (ORS) as the first line of management for acute diarrhea in children. However, some pharmacists do not comply with these recommendations and tend to dispense unnecessary or inappropriate products. 2 Studies have shown that there is a high degree of variation among pharmacists in the dispensing of ORS, ranging from 5% to 70%.18,19 Inadequate knowledge and insufficient training on the appropriate management of acute diarrhea are the primary reasons for the low dispensing of ORS by pharmacists. In addition, other factors such as prioritizing higher profits by selling more expensive products or dispensing antibiotics due to patient or parental pressure also contribute to this issue.18,19
According to the WHO guideline (2005), breastfeeding should be continued during rehydration therapy in breastfed infants with acute diarrhea. Recent studies have indicated that early refeeding after rehydration in older children leads to better outcomes than late refeeding.3,20 However, some studies have highlighted that pharmacists may not provide appropriate advice on feeding during consultations. For instance, one study found that only 12% of pharmacists gave appropriate advice on feeding,18,21 while another study found that 26% of pharmacists gave inappropriate dietary recommendations such as discontinuing milk or suggesting soda intake.15,22
While a questionnaire is a suitable tool for evaluating the knowledge of healthcare professionals on a given topic, such as the management of acute diarrhea, some researchers 16 have used additional methods, such as simulated clients, to assess their actual practices. In our study, we aim to use both the questionnaire and simulated client methods to assess the treatment patterns and counseling practices of community pharmacists regarding the management of acute diarrhea in children in Yemen. Furthermore, we will explore the impact of demographic factors on the practices of the pharmacists.
Methodology
Study area and period
A study was carried out in community pharmacies located in the capital city of Yemen, Sana’a, for a period of around 2 months started at the beginning of June 2023.
Study design and population
Using a cross-sectional study design, the research was divided into two parts: a structured self-administered questionnaire and simulated client method. Each pharmacy was visited twice; the first visit involved giving the questionnaire to the pharmacy professional, and the second visit involved applying the simulated client method.
Inclusion and exclusion criteria
During the data-collection period, pharmacy professional working in community pharmacies were included, whereas those employed in hospital-based or primary healthcare center pharmacies were excluded from the study.
Sampling technique
The study employed a convenient sampling technique to select 100 community pharmacies. The capital city was divided into four areas, and 25 community pharmacies in each area were visited. In case a pharmacy declined to participate, the next pharmacy was approached.
Data collection instrument and procedures
To assess the treatment patterns and counseling practices of community pharmacists regarding the management of acute diarrhea in children, a questionnaire survey and simulated client methods were utilized. The pharmacy professional was given a questionnaire during the first visit to answer the questions, and later the same pharmacy professional was visited by a simulated client.
Questionnaire
The study employed an anonymous, structured, and validated questionnaire that was adapted from literature. 16 The investigators obtained verbal permission from the pharmacy professional to answer the questionnaire and participate in the study. To ensure clarity and ease of understanding, the questionnaire was pretested on 10% of pharmacy professionals in a pilot study. Ten pharmacists completed the questionnaire and reported no difficulties in understanding or answering the questions. To facilitate the simulated client method, the pharmacies were divided into four groups (A, B, C, and D), with each group consisting of 25 pharmacies, and the questionnaire was distributed by the four investigators.
The questionnaire was divided into three sections (appindex 1). The first section covered demographic characteristics of the community pharmacists such as age, gender, qualification, country of graduation, experience, and job status. The second section assessed community pharmacists’ knowledge and attitudes about the management of acute diarrhea in children, including questions about ORS. The third section evaluated community pharmacists’ practices for the management of acute diarrhea in children, including questions about recommended drugs or products, evaluation of the child’s case using five indicators (child’s age, onset, duration or frequency of diarrhea, presence of blood or mucus in stool, and fever), counseling regarding the recommended product, and dietary advice.
Simulated client
The same four investigators who distributed the questionnaire also conducted the simulated client visit, but they visited different groups of pharmacies compared to those they visited during the questionnaire distribution to prevent the possibility of pharmacy professionals identifying the simulated client. For instance, if investigator 1 visited group A pharmacies during the questionnaire, they would visit group B pharmacies during the simulation. The simulated client visits were conducted at the same time and day that the questionnaire visits were done, 3 weeks later, to ensure that the same pharmacist who completed the questionnaire would attend to the simulated client.
To ensure that the simulated clients visited the same pharmacist, they carried a paper with the demographic data of the pharmacist and comments on their physical characteristics written by the investigator who visited the pharmacy during the questionnaire visit.
During the simulated client visit, the client entered the community pharmacy with a scenario of a 2-year-old sibling or nephew suffering from acute watery diarrhea without any accompanying symptoms. The simulated client only said “my brother/nephew has diarrhea” upon entering the pharmacy and provided further information only upon request. The information provided upon request included the age of the child (2 years), absence of fever, vomiting, blood or mucus in stool, and occurrence of four episodes of diarrhea since yesterday.
Since the simulated clients were investigators in the study, they had adequate knowledge about the subject. However, they were additionally trained on how to interact with pharmacy professionals before conducting the visits. Upon leaving the pharmacy, the simulated clients completed a form that included information on whether they interacted with the same pharmacist as the one who completed the questionnaire, information on referral, use of evaluation indicators, drugs recommended, drug counseling, and dietary advice.
Data analysis
After completing all the questionnaires and simulation data collection, data were analyzed using Statistical Package for Social Sciences software (SPSS, version 24, SPSS, Chicago, IL, USA). Descriptive and inferential analyses have been applied. Chi-square test and Fisher’s Exact test were used for associations’ significance (P < 0.05). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 23
Results
Demographic data
A total of 100 pharmacists completed the questionnaire and were visited during the simulation. It is noteworthy that the pharmacy professionals (pharmacists and pharmacy technicians) encountered by the simulated patients were the same individuals who were interviewed. The majority of pharmacy professionals (84.0%) were male, with 77.0% of them being under the age of 40 years. The most common job title among the pharmacy professionals was pharmacy staff (85.0%). Only 35.0% of pharmacy professionals had more than 5 years of experience. In addition, the data indicate that majority of pharmacy professionals held a bachelor’s degree (74.0%). More detailed demographic data can be found in Table 1.
Demographic data of the pharmacists.

Evaluation of the case
Regarding history taking and the use of the evaluation indicators, 43.0% of the pharmacy professionals reported using all the five indicators in the questionnaire, while 40.0% used at least three indicators, and 17% used two or fewer indicators. However, during the simulation, only 3.0% of the pharmacy professionals employed all five indicators, 9.0% used at least three indicators, and 88.0% used two or less indicators. It is worth noting that all pharmacy professionals asked about the age of the child. Investigating a statistical difference between the questionnaire and simulation regarding the use of these evaluation indicators, the analysis showed no statistically significant difference (P = 0.43). More detailed can be found in Figure 1.
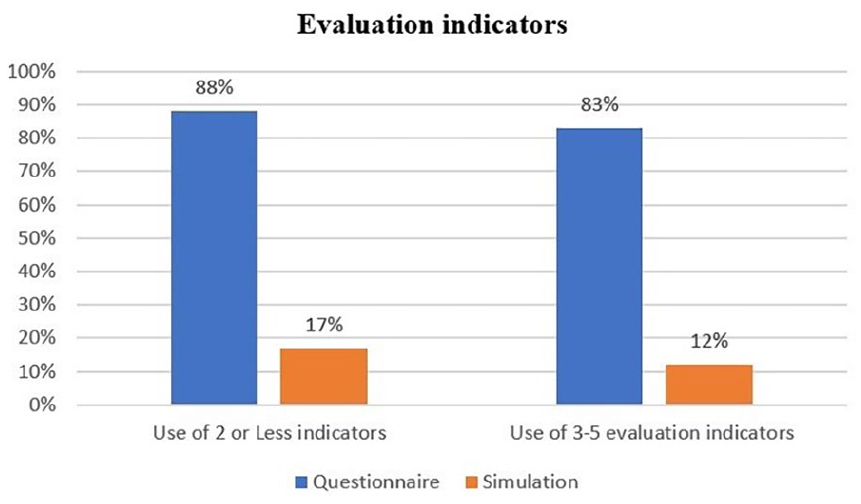
Comparison between questionnaire and simulation regarding the use of evaluation indicators.
Drugs recommendation
Data from the questionnaire reveal that 42% of pharmacy professionals gave ORS alone, while 47.0% prescribed ORS in combination with other drugs, including antibiotics. On the other hand, 11.0% of professionals chose to administer only other drugs. During the simulation, 7.0% of the pharmacy professionals referred the patients to a clinic, 6.0% gave ORS alone, 47.0% provided ORS along with other drugs, including antibiotics, and 40.0% dispensed only antibiotics (Figure 2). The other products used are metronidazole, loperamide, kaolin, and antibiotics (septrin, nifuroxazide, nitazoxanide). However, only three pharmacy professionals (3%) opted to give loperamide, indicating a relatively low usage rate. Similarly, probiotics were recommended by four pharmacy professionals (4%).

Comparison between questionnaire and simulation regarding drug recommendation.
Furthermore, a statistical analysis was conducted to investigate any differences between the questionnaire and simulation regarding the use of ORS alone or in combination with other drugs. Fisher’s Exact test indicated a statistically significant difference (P = 0.046), as illustrated in Table 2.
Difference between questionnaire and simulation in overall ORS recommendation.

Fisher’s Exact test.
Educational advices
While 89.0% of pharmacy professionals reported that they would explain the recommended medicine to the patient during the questionnaire, only 36.0% actually provided any sort of explanation to the simulated client.
Regarding dietary advices, more than half of the pharmacy professionals (53.0%) advised increasing fluid intake in the questionnaire. Only 5.0% advised continuing normal feeding, while 33.0% provided more than one advice. In addition, 2.0% advised withholding milk, and 7.0% advised reducing food intake until child be okay. However, during the simulation, only 20.0% of pharmacy professionals provided appropriate dietary advice, while 16.0% offered inappropriate advice. Surprisingly, 64.0% of professionals did not provide any advice regarding the diet.
Other information
When the pharmacy professionals were asked whether they would recommend antibiotic to a child with diarrhea, 25 pharmacy professionals (25.0%) answered yes, while the remaining suggested other drugs either with or without ORS. Among the study sample, septrin was the most frequently recommended antibiotic by 46.0% of participants. When the pharmacy professionals were asked about the reason for choosing a particular product for managing diarrhea, 42.0% reported that it works better, 32.0% stated that it is recommended by the WHO, mentioned that it works faster, and 12.0% selected more than one option.
In regard to the question “How often do you recommend the use of ORS?,” 39.0% of pharmacy professionals reported recommending ORS all the time, while 61.0% recommended it occasionally. In addition, 83.0% of pharmacy professionals reported keeping enough stock of ORS, with 27.0% agreeing that ORS can be used as a complete management for watery diarrhea.
A comprehensive explanation regarding the use of ORS sachets includes instructions on how to mix the salt and store the solution, how long the solution can be used after preparation, and how and when to give the solution to the child. During the simulated visits, out of the eight pharmacy professionals who recommended ORS, only two (25.0%) provided the simulated patients with a complete explanation on how to use the sachets. Four pharmacy professionals (50.0%) did not provide any explanation at all regarding the product’s usage. The remaining two pharmacy professionals (25.0%) gave an incomplete explanation.
Regarding the function of ORS, only 30.0% of the pharmacy professionals correctly identified its purpose as replacing fluid and electrolytes lost. When the pharmacy professionals were asked about the quantities of salt, sugar, and water in ORS packs, only 7.0% provided the correct answer, while 25.0% gave an incorrect answer, and 68.0% did not provide an answer. When investigating pharmacy professionals’ awareness of new osmolality ORS, only 22.0% of them were aware of it, and 13.0% reported having it in stock. In response to the question “Do you stock zinc supplements for children?,” 66.0% of pharmacy professionals reported having this supplement in stock.
Association between demographic characteristics and the number of evaluation indicators
The association between the demographic characteristics (gender, age, qualification, country of graduation, and years of experience) and the number of evaluation indicators was explored. No statistically significant association was found between any of the demographic variables and the number of evaluation indicators used in the questionnaire interview (P > 0.05). However, Fisher’s Exact test indicated a statistically significant association (P = 0.022) between the number of evaluation indicators used and gender in relation to the simulation client visit (Table 3). It is important to note that no significant associations were observed with other demographic variables.
Association between gender and number of evaluation indicators used.

Fisher’s Exact test.
Association between demographic characteristics and the choice of recommended product
The association between demographic characteristics and the choice of recommended product was also examined. No statistically significant association was found between any of the demographic variables and the choice of recommended product, both in relation to the questionnaire interview and the simulation client visit (P > 0.05).
Discussion
The results revealed a significant concern regarding the inadequate history taking in actual practice by pharmacy professionals. While 83% of pharmacy professionals indicated their preference for asking 3–5 indicators to evaluate children with diarrhea during the questionnaire, 88% of them relied on two or fewer indicators during the simulated practice scenario. This discrepancy between questionnaire knowledge and actual practice evaluation is consistent with findings from other studies involving simulated clients.15,16,18,24,25 Accurate evaluation, recommendation of ORS alone, and providing correct instructions on fluid and food intake are crucial for appropriate management of acute “watery” diarrhea in children. 16 These evaluation indicator questions play a crucial role as they assist pharmacists in assessing the risk of dehydration and determining whether a child requires a referral or not.
According to the WHO, 2 ORS is recommended as an essential component for managing acute diarrhea in children. During the questionnaire, 42 pharmacy professionals (42%) agreed to administer ORS alone, but in the actual practice, only six pharmacy professionals (6%) dispensed it as a standalone treatment. This percentage aligns with the findings of a study conducted in Nigeria. 16 The low rate of ORS recommendation during actual practice highlights the urgent need for an educational campaign to promote the use of ORS among pharmacists and other healthcare professionals.
Kaolin, available as a kaolin-pectin suspension, was the most commonly recommended agent as a monotherapy by the pharmacists in both the questionnaire (22%) and the actual practice (17%). However, during the simulation, many pharmacy professionals reported that kaolin had been out of stock in their pharmacies for several months. If kaolin had been available in those pharmacies, we would have expected a higher number of pharmacy professionals to inappropriately dispense it during the actual practice. It is worth noting that both the WHO and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines do not recommend the use of kaolin for managing diarrhea in children.3,17
While filling the questionnaire, when the pharmacy professionals were asked if they would prescribe antibiotic to a child with acute diarrhea, 25 pharmacy professionals (25.0%) expressed their willingness to prescribe antibiotics. However, during the actual practice, 40 pharmacy professionals (40.0%) administered antibiotics (septrin, metronidazole, nifuroxazide, nitazoxanide). Comparing our findings to a previous study conducted in Yemen, 25 where pharmacy professionals directly dispensed antibiotics to 75.5% of simulated clients reporting diarrhea, our study observed a decrease in antibiotic dispensing by community pharmacists. This decline in antibiotic dispensing could be attributed to stock shortages resulting from the prevailing political situation.
Despite its potential benefits for treating diarrhea in adults, loperamide is not considered safe or effective for children under the age of 2 years, according to the WHO.17,26 Therefore, it is recommended to avoid administering loperamide to young children. In our study, only three pharmacists chose to give loperamide, indicating a relatively low usage rate among the pharmacists.
In the current study, the recommendation of probiotics, which have the potential to reduce the duration of diarrhea, was made by only four pharmacy professionals (4.0%). This contrasts with other studies15,27 where probiotics were frequently suggested by community pharmacists. Furthermore, as part of their management approach, three pharmacy professionals (3.0%) provided the simulated client with lactose-free milk.
Counseling patients on the appropriate use of medication is a significant responsibility of community pharmacists. A study conducted in Kuwait revealed that patients often have high expectations for pharmacists to provide them with education regarding the proper use of their medicines. 28 In our study, the majority of pharmacy professionals (89.0%) expressed their intention to explain the recommended product to the patient during the questionnaire interview. However, only 36.0% of the pharmacy professionals provided counseling to the simulated client regarding the recommended product. These findings align with a study conducted in Ethiopia. 24 During the questionnaire interview, more than half of the pharmacy professionals opted to provide appropriate dietary advice, which included recommendations to increase fluid intake, continue normal feeding, or both. However, in actual practice, only 20 (20%) pharmacy professionals provided the simulated client with advice to increase fluid intake, while 16 (16%) pharmacy professionals offered inappropriate dietary guidance. These findings align with similar studies conducted in Ethiopia and Nigeria.17,24 While pharmacy professionals in our study demonstrated satisfactory knowledge across various aspects during the questionnaire, they exhibited limited questioning and inadequate counseling during the actual practice. This observation suggests that some pharmacy professionals may rely more on their personal experience rather than the knowledge they possess. 29 The disparity between the information gathered from the questionnaire and the simulation highlights the potential limitations of using questionnaires alone as a reliable method to assess pharmacists’ real-world practice.
Educational programs and professional development workshops have been identified as effective approaches to enhance the knowledge and practice of community pharmacists. 30 Specifically, in the context of managing acute diarrhea in children, Pham et al. 31 have found that educational interventions resulted in improved questioning skills and increased dispensing of ORS by pharmacists. However, it is worth noting that factors such as working hours and the work environment can pose significant obstacles to pharmacists’ access to education. 29
In the current study, we analyzed the association between demographic variables and the number of evaluation indicators used during questionnaire interview as well as the choice of recommended product. The significant association was found between the number of evaluation indicators used and gender in relation to the simulation client visit. The data revealed a significantly higher proportion of females than males (31.2% vs 8.3%, P = 0.022) who utilized approximately 3–5 evaluation indicators. Several factors could potentially explain this discrepancy. First, it is possible that the females in our study had prior experience in evaluating diarrhea cases, providing them with a better understanding of the indicators and their application. Moreover, females may have demonstrated stronger communication skills during the evaluation process, allowing them to effectively utilize multiple indicators. This could be attributed to their tendency to be more eager, studious, and detail-oriented than males. Such characteristics may have contributed to their higher engagement and information-seeking behavior. Furthermore, it is worth considering that the observed performance difference could be influenced by individual variations within each gender group. It is plausible that the female group consisted of individuals who were particularly skilled or motivated in using evaluation indicators, while the male group may have comprised individuals with diverse abilities and interests.
Our study, similar to any other research, possesses its own set of strengths and limitations. The primary strength lies in the utilization of both a questionnaire and simulation to evaluate the knowledge and practices of pharmacists regarding the subject matter. The simulated client method provides us with a more accurate and authentic representation of pharmacists’ actual practices. As for limitations, it is important to note that the outcomes of this study were limited to the management of acute diarrhea in a convenience sample of pharmacy professionals within the capital city (Sana’a). Consequently, caution should be exercised when generalizing these findings to other diseases or different regions within Yemen. Our study provides valuable insights within the defined research setting and can serve as a foundation for future research and exploration. Future studies that employ more diverse and representative sampling methods would be beneficial to validate and extend our findings to a broader population.
Recommendations
The findings of this study emphasize the urgent necessity of implementing educational programs aimed at enhancing the management of acute watery diarrhea among community pharmacy professionals in Yemen. It is crucial to conduct professional development workshops to improve their knowledge in this area. Furthermore, it is recommended to conduct further studies that encompass other governorates in Yemen and assess the knowledge and practice of pharmacy professionals regarding other diseases. This will contribute to enhancing the overall quality of pharmaceutical care provided by community pharmacy professionals.
Conclusion
In our study, it was observed that the community pharmacy professionals did not ask an adequate number of indicator questions to effectively evaluate and manage a child with acute diarrhea. In addition, they did not provide sufficient dietary advice, and less than half of them recommended ORS for managing acute diarrhea in children. Moreover, they inappropriately administered other medications to the simulated clients who presented a scenario involving a 2-year-old child with acute watery diarrhea lasting for 1 day.
Footnotes
Appendix 1
Acknowledgements
The author would like to express gratitude to the Deanship of Scientific Research, Qassim University, for funding the publication of this project. In addition, heartfelt thanks are extended to all the community pharmacists who willingly agreed to participate in this study.