
Abstract
Background:
Many governments encouraged generic use to enhance health equality and minimise health expenditure. The lack of knowledge and acceptance of generic medicines are the main barriers to their use.
Objectives:
This study aimed to assess population knowledge and perception towards generic drugs, identify their primary sources of information and examine which variables are independently related to their acceptance.
Design:
An observational cross-sectional study was performed targeting the Lebanese adult population.
Methods:
Overall, 385 patients participated in the study. Data were collected using a uniform survey from six public healthcare centres.
Results:
The participants reported a distrust towards generic drugs; they either said that they were not as effective as the brand (36.9%), were of less quality than the brand (38.5%) or had more side effects than the brand (38.4%). Around 52% said they would never buy a generic drug, and two-thirds (68.6%) preferred using a brand drug over a generic one. After adjusting for socio-demographics, a high income (odds ratio (OR) = 3.7), knowing that brands and generics have the same active ingredients (OR = 2.28) and that brands and generics were equally effective (OR = 6.46) were the strongest independent predictors for the willingness to buy generic drugs.
Conclusion:
A lack of knowledge and misperceptions about generic drugs limited the use of generic drugs, and therefore must be addressed.
Background
Pharmaceutical expenditures in Lebanon are considered one of the highest in the Eastern Mediterranean region since they account for over 25% of the total healthcare expenditure.1,2 Around 42% of the Lebanese population pay the total cost of health services and medications, while the remaining get 80% of their bills reimbursed by the Ministry of Public Health (MOPH) 6 months after. 3 To control the escalation of this spending, the Lebanese government and third-party payers encouraged the use of generics by implementing various policies, initiatives and strategies.4,5 In August 2015, the MOPH in Lebanon officially started implementing ministerial decision no.1295 by introducing drug substitution and a unified medical prescription form to promote generics. 6
Compared to their counterpart brands, generics are bioequivalent but generally 10%–80% less expensive. 7 Moreover, the food and drug administration stated that generics should be similar in the pharmaceutical form, safety, strength, route of administration and clinical use but could be different in some aspects, such as inactive ingredients, colour and shape.8,9 However, the use of generic medicines is restrained due to the limited knowledge and the negative perception of patients towards their quality, efficacy and safety. 10 Consequently, the perceived outcome of using generics to treat their conditions would be questioned (the nocebo effect). 11 Physicians in Lebanon reported a downward generic prescribing pattern primarily due to their perception and trust in brand medicines in addition to pharmaceutical companies marketing strategies such as gifts and samples provision.12,13 Moreover, the odds of acceptance to switch to generic drugs after initial treatment were reported to be higher among older Lebanese physicians with more experience. 14 However, in a recent study targeting pharmacists, only 52% suggested substituting to generics and were not supportive of the current strategy adopted. 6
Nevertheless, a study conducted in 2018 reported that after 12 months of switching from a brand to a generic drug, the same health outcomes were observed in terms of outpatient visits, urgent care visits, hospitalisations and medication discontinuation. 15 Therefore, community pharmacists play a significant role in clarifying patients’ concerns, promoting generic awareness and minimising their misconceptions. 16 After the implementation of the generic substitution policy issued by the MOPH, the attitudes of community pharmacists in Lebanon were examined and the practices were reported. 17 Community pharmacists stated that they faced many challenges in implementing the generic substitution policy since many patients did not accept it. 18 Accordingly, many strategies were adopted by the government and the order of pharmacists to clarify the misconceptions and lack of knowledge through continuous education programmes. 19
Healthcare professionals and pharmaceutical companies reported several limitations concerning the shortage of medications and late distribution channels. 20 Consequently, it is important to assess these misconceptions for professionals and patients to provide the optimal health option. A recent study reported some knowledge gaps in primary prevention and the general population’s misconceptions about the risk factors associated with these gaps. 21 Therefore, understanding the population’s knowledge and perceptions towards generics and evaluating their acceptance are essential to promote generic prescription and identifying predictors of their use.
Objectives
This study aimed to (1) assess population knowledge and (2) perception towards generic drugs, (3) identify their primary sources of information about generic drugs, (4) assess the acceptance of generics, (5) evaluate how the correlation between their knowledge and their socio-demographic variables and (6) to examine which variables are independently related to the acceptance of generic drugs.
Design
An observational cross-sectional study was performed between June and September 2017, targeting a sample of Lebanese adults in order to assess their knowledge and perception of generic drugs and factors affecting their acceptance to buy them. This study employed a questionnaire for data collection administered during face-to-face interviews.
Methods
Setting and participants
Non-probability convenience sampling was used to recruit participants from six public MOPH care centres across the six Lebanese governorates. Recruitment took place on any of the days the centres were open and at different times of the day. Participants were selected from each centre by proportional allocation according to the average number of patients seen in each centre annually. Beirut drug distribution centre accounted for 64% of the sample, 9% from Tripoli, 8% for each centre in Beqaa, Saida and Nabatieh, and 3% in Akkar drug distribution centre.
Epi info was used to calculate the required sample size, using the following equation

where Z is a standard normal variate (Z1 − α/2 = 1.96 at 95% confidence interval (CI)), d is the absolute accuracy or precision (5% margin of error), and p is the expected proportion of the population with a specific outcome and was set at 0.5 (the advised value if the proportion in the population is not known). This yielded a required sample size of 405 (5% refusal rate). Lebanese adults residing in Lebanon at the time of the study were included. Exclusion criteria were being older than 80 years old with any mental, cognitive or severe psychiatric disorders that made them non-eligible to be part of the study.
Study instrument
The questionnaire had closed-ended questions and consisted of three main parts: the first part covered the socio-demographic characteristics of the study participants, including sex, age, the governorate of residence, level of education, occupation and existing medical conditions (comorbidities). The second part was designed to collect data related to participants’ knowledge and perception of generic drugs. The third part assessed the participant’s acceptance of generic drugs. The second and third sections contained questions with three possible answers: yes, no and I am not sure. The survey was piloted on 15 volunteers after which questions with a lack of clarity or comprehensiveness were adjusted accordingly.
Data collection and management
Data collection was completed from 5 June 2017 to 7 July 2017. Six pharmacists working in the drug distribution centres collected data and received uniform training before the interview. During recruitment, an interviewer would approach people seeking medical care in the centres and provide information about the study. If the patient accepted to participate, the interviewer will register his answers using the questionnaire. To enhance the quality of data, face-to-face interviews were performed. The survey was available in English and Arabic to ensure that participants fully understood the survey’s language. Furthermore, a comparison with the national socio-demographics was performed after reaching 200 answers and afterwards for the whole sample to better reflect the general Lebanese population characteristics. Questionnaires were coded to ensure information confidentiality (pseudonymised data). Electronic data were stored in a password-protected computer file, and questionnaires were in a setting with restricted entrance. Once the retention period expires, data will be destroyed, as set by law.
Ethical considerations
This study used a survey for data collection without any type of invasive procedures or intervention. After reviewing the study protocol and questionnaire, no formal ethical considerations were required because the survey complied with the following Lebanese University ethical committee criteria: data were completely anonymous and non-identifiable; storage of data follow-up university general data protection regulation guidelines, and a written informed consent was obtained from each participant after explaining the study objectives on the first page of the questionnaire. However, legal approvals were taken from the local health regulatory authorities in the MOPH in Beirut. Participants were also informed that they could withdraw their participation at any point during the interview. Findings were considered for research purposes only, and no financial incentives were provided.
Statistical analysis
Statistical analyses were performed using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) Version 26.
To evaluate the national representativeness of the sample, we compared the distribution of socio-demographic characteristics between the sample and national data. Univariable relationships between two categorical variables or an independent continuous variable and a categorical dependent variable were assessed using logistic regression, producing crude ORs with 95% CI. The answers to the questions regarding knowledge, perception and socio-demographics were used as independent variables in a multivariate logistic regression that used willingness to buy generic drugs as the dependent variable. The variables age, sex, education and income were always included in the regression irrespective of statistical significance since these variables have previously been shown to be clinically important variables to adjust for. The knowledge and perception variables were only candidates for purposeful selection if they had p-values < 0.20 in univariable analysis. Whether or not a variable was added to the model was based on the likelihood ratio test with significance set at p < 0.05.
Two additional multivariate logistic regressions were done for the preference of brands over generics to switch from brand to generic, and the willingness to substitute the brand to its generic in correlation with the independent variables.
Results
In total, 405 people were approached, and 20 refused to participate (4.9%). The survey took an average of 15 min to complete. Table 1 shows the distribution of socio-demographic characteristics in the sample and when possible, compares this with the distribution in the general population to get an impression of representativeness.
Distribution of socio-demographic characteristics in the sample and the general population, Lebanon 2017.

The sample distribution of gender (51.2% males) is like the distribution in the population (49.4% males). The mean age in the sample is higher than in the general population (44 years vs 28 years). In our sample, the Beirut governorate was over-represented (25.5% vs 9.3% in the population), while the North (15.1% vs 21.9% in the population) and Mount Lebanon (23.1% vs 34.8% in the population) were under-represented. Regarding education, 43.6% of people held a university degree, 25.4% had primary or intermediate education at most and 27.3% had a higher secondary diploma. The comparison with population data was not available for the type of occupation and income, but around half of the participants worked in a non-medical field (53.8%). In comparison, 35.1% were unemployed or inactive, and half earned more than 1000 US$ per month.
Knowledge of generic drugs
About half of people have used a generic in the past (47.0%). This and the answers to the knowledge questions are presented in Table 2. Overall, a third of the knowledge questions were answered with an ‘I am not sure’, indicating many people were not familiar with this topic. In addition, one in five people did not know the active ingredient is the same (19.4%) or were not sure the dosage in the generic would be the same as in the brand (19.4%).
Knowledge and perception towards generic drugs, Lebanon 2017.

Perception of generic drugs
Participants’ perception of generic drugs is presented in Table 2. There is quite a marked distrust towards generic drugs in about a third of people, they either think that generic drugs are not as effective as the brand (36.9%), are of less quality than the brand (38.5%) or have more side effects than the brand (38.4%).
Sources of information about generic drugs
Table 2 also shows that 59.4% of respondents had never received information about generic drugs. The 144 people who had received information about generic drugs answered that this information primarily came from pharmacists (55.6%, n = 80) and physicians (38.9%, n = 56), while a smaller number of people mentioned the media (15.3%, n = 22), friends or family (11.8%, n = 17) and nurses (5.6%, n = 8) (Figure 1).

Distribution of the sources of information related to generic drugs, Lebanon 2017.
Acceptance of generic drugs
Table 3 shows the acceptance of generics. In general, 51.7% (n = 199) say they would never buy a generic drug, and two-thirds (68.6%, n = 264) prefer using a brand drug over a generic drug. The acceptance of generic drugs also depends on the illness: 20.3% (n = 78) would accept generic drugs for infections, but more than double (44.7%, n = 130) would accept them for cancer treatment.
Acceptance of generic drugs, Lebanon 2017.
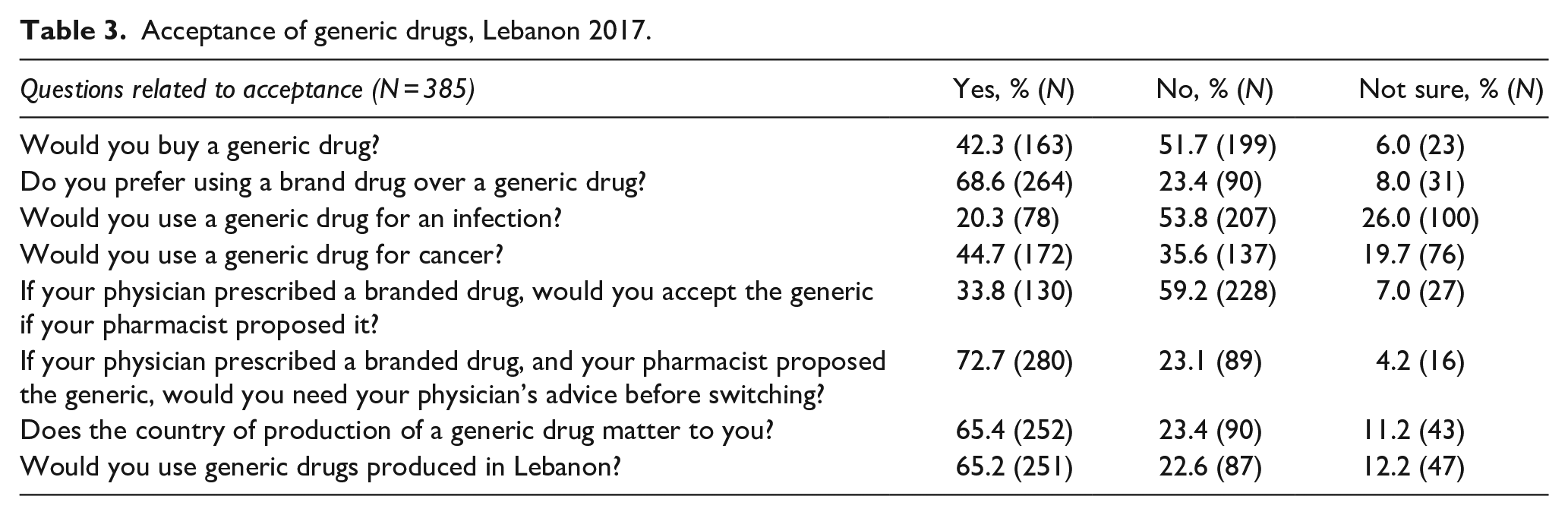
If their pharmacist would propose a generic when the physician prescribed the brand, 72.7% (n = 280) would want to ask their physician for advice before accepting. This hesitancy towards buying generic drugs seems heavily influenced by the fear of lower quality since far fewer people would refuse the generic if they were certain it was locally produced (22.6%, n = 87).
There is a correlation between the knowledge of generic drugs and age, gender, income, and level of education. Table 4 shows the results of the univariate analysis between the knowledge questions and the answers to the socio-demographic variables. Every year of increasing age was associated with a lower chance of having received information (odds ratio (OR) = 0.98, 95% CI = [0.97–1.00]). There are no significant correlations with the gender of the participants. However, each 500 US$ increase in monthly income was associated with considering that both generic drugs and the brands have the same dosage (OR = 1.19, 95% CI = [1.03–1.37]) and active ingredient (OR = 1.25, 95% CI = [1.08–1.45]).
Correlation between knowledge and perception of generic drugs and socio-demographic variables.
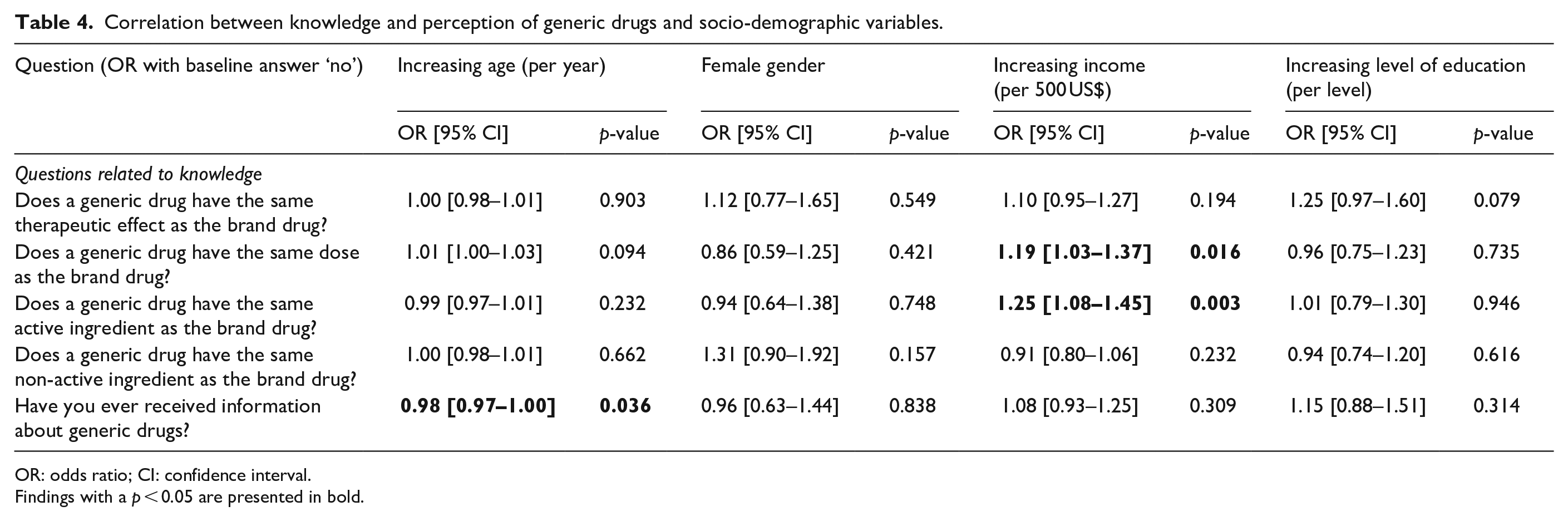
OR: odds ratio; CI: confidence interval.
Findings with a p < 0.05 are presented in bold.
Variables related to the acceptance of generic drugs
After adjusting for socio-demographics, a high income (OR = 3.7 for income >2000 US$/month, 95% CI = [1.55–8.72]), knowing that brands and generic have the same active ingredients (OR = 2.28, 95% CI = [1.09–4.76]) and believing that brands and generics are equally effective (OR = 6.46, 95% CI = [3.63–11.49]) were the strongest independent predictors for the willingness to buy generic drugs (see Table 5).
Predictors of willingness to buy generic drugs*, Lebanon 2017.
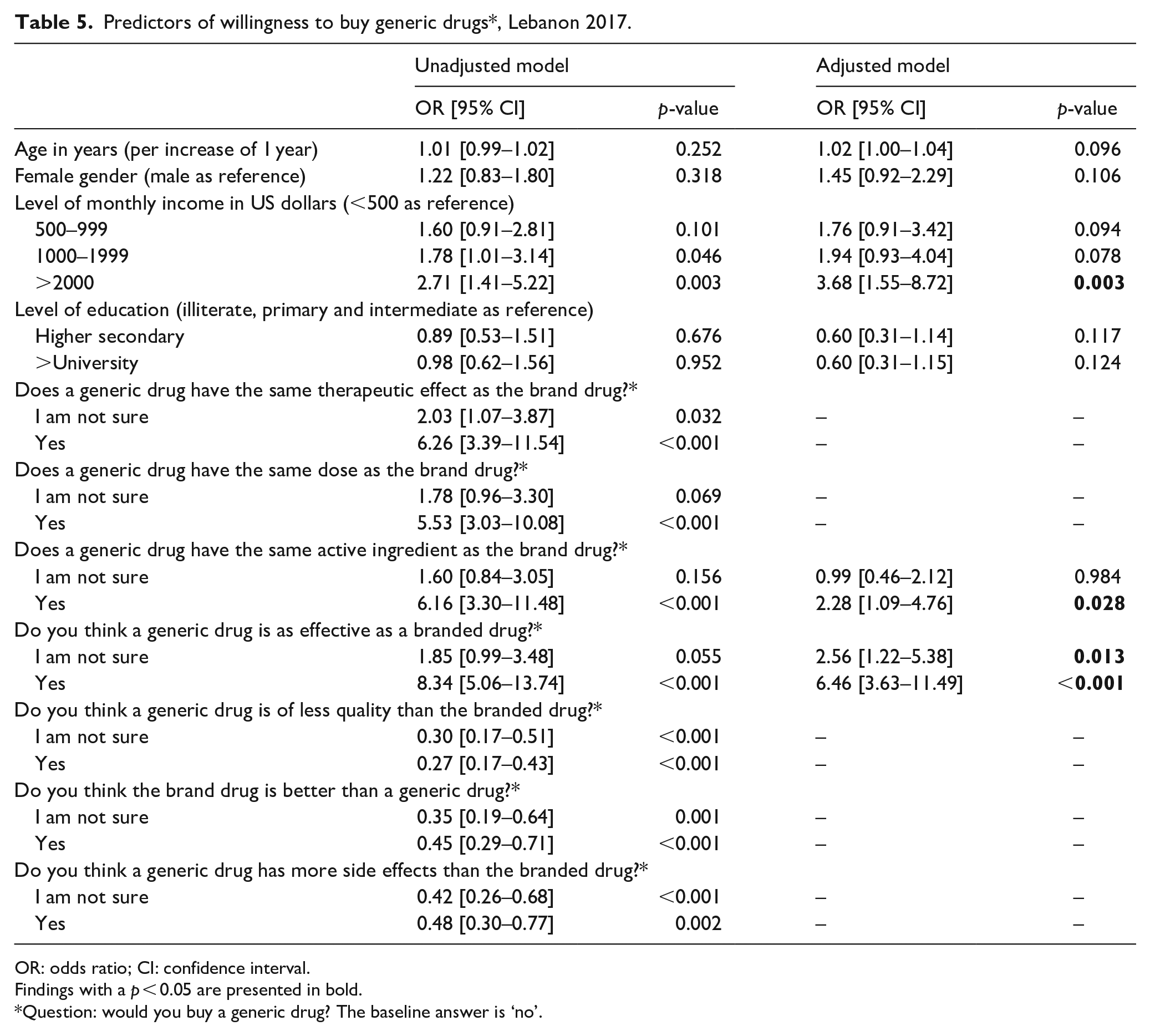
OR: odds ratio; CI: confidence interval.
Findings with a p < 0.05 are presented in bold.
Question: would you buy a generic drug? The baseline answer is ‘no’.
Table 6 shows that after adjusting for socio-demographics, believing that brands and generic are equally effective predicts that there is no preference for the brand version (OR = 0.23, 95% CI = [0.11–0.48]), while believing that the brand is better predicts a strong preference for the brand (OR = 59.2, 95% CI = [23.7–147.91]).
Predictors of a preference for branded drugs over generic drugs*, Lebanon 2017.

OR: odds ratio; CI: confidence interval.
Findings with a p < 0.05 are presented in bold.
Question: do you prefer brand drugs over generic ones? The baseline answer is ‘no’.
Table 7 shows that after adjusting for socio-demographics, the willingness to substitute a brand for a generic drug is increased by a higher level of education (OR = 2.15, 95% CI = [1.13–4.07]) and by believing that the generic is as effective as the brand drug (OR = 4.44, 95% CI = [2.61–7.55]). The willingness to substitute is decreased in groups who believe the brand is better than the generic (OR = 0.33, 95% CI = [0.20–0.54]).
Predictors of willingness to substitute brand for generics, Lebanon 2017.

OR: odds ratio; CI: confidence interval.
Findings with a p < 0.05 are presented in bold.
Question: if your physician prescribed a branded drug, would you accept the generic if your pharmacist proposed it? The baseline answer is ‘no’.
Discussion
An extensive set of studies explored the patients’ recognition and perception of towards the use of generic drugs in contrast with brands.1,2,4 Several studies reported a lack of knowledge among many participants.5,6 In a recent study conducted in Iraq in 2021 on the general population, they believed that generic drugs have less efficacy (53.5%), lower quality (57.1%), and lower safety (46.3%) when compared to their brand counterparts. 8 A high percentage of the Lebanese population answered the knowledge-related questions with ‘I am not sure’, reflecting a lack of understanding and knowledge about generic drugs. A comparable finding was reported in a study conducted in Bulgaria, where most participants answered either ‘Don’t know’ (46%) or ‘Not sure’ (43%) when asked about the differences between branded and generic drugs. 9 In addition, a high percentage of the study participants stated that generic medications might be of a lower quality (38.5%), efficacy (36.9%), and produce more side effects (34.6%) in comparison to their branded counterparts. These results are in accordance with reports from the literature.16,22 Therefore, strategies should clarify misconceptions to increase generic drugs’ use, given that both generic and branded drugs must fulfil safety and efficacy criteria before receiving marketing authorisation.
The primary source of information about generic drugs in this study included pharmacists (55.6%), physicians (38.9%), and social media (15.3%). Other studies in different settings reported that doctors and pharmacists were considered equal sources of information.7,10 However, access to pharmacists is easier in a low- to middle-income country like Lebanon, which can facilitate their role in clarifying misinformation and providing explanations in patient-friendly language. 23 Providing the appropriate information to the Lebanese population is vital because knowledge about these medications is essential for improving the acceptance of generic medicine. Insufficient information is one of the main barriers to the wider use of generics.21,24 Therefore, empowering pharmacists’ role and encouraging them to clarify any misconceptions about generics is crucial to optimise the population’s knowledge and, as a result, increase generic use.
Moreover, when assessing the acceptability of generic medicines, 68.6% of the participants preferred the brand over the generic in accordance with other studies.6,15 Only 33.8% accepted the use of generic drugs when proposed by their pharmacist and 72.7% would want to ask their physician for advice before accepting. Generic substitution is an important strategy adapted to decrease the overall medication cost. The findings of this study were higher in a study held in Portugal where 88.7% would accept generic substitution based on their physician’s recommendation and 64.5% would do the same based on the pharmacists’ advice. 25 In other terms, this might indicate that the physicians’ preference will affect the patient’s acceptance of generic substitution. However, pharmaceutical companies could have influenced physicians’ prescribing behaviour, which could indirectly affect their patients, by encouraging them to use a more expensive brand instead of an equally effective, lower-cost generic.19,26 Hence, promoting generic prescribing, substitution and guiding the patients through simple methods would increase the acceptability of generics. These methods include pamphlets and medical brochures provided in pharmacies and health clinics.
A significant correlation was observed between receiving information about generic and increasing age (p = 0.036). This correlation could be explained by the fact that the majority of the sample was young, and as a result of increasing age, they tend to prioritise their profession and families over their own health. 27 Moreover, stating that a generic had the same dose and active ingredient as the correspondent brand was correlated with the increase in income (p = 0.016 and 0.003, respectively), which was previously reported in the literature. 28 These findings are in accordance with a systematic review conducted in 2015 in Brazil, where people with lower income had more negative perceptions towards generics associated with lower use. 29 An accessible list of the available generics should be provided to promote generic use by encouraging the engagement of specific groups, such as those with higher income and better knowledge about generic drugs, to influence other groups in the community.
When evaluating the predictors in correlation with the willingness to buy generics, it was noted that people with a high income had 3.7 higher odds of buying them, in accordance with a study conducted in the United States where people with lower income used fewer generics. 28 Furthermore, people who stated that both generics and brands are effective had a 6.46 times more chance to buy them together, with those reporting that they both have the same dose (OR = 2.2, 95% CI = [1.05–4.59]). The findings emphasise the importance of providing good knowledge and its direct effect on the purchasing behaviour of the patients. More particularly, it should focus on maximising the knowledge of people with low income and highlighting other incentives including the price and the common availability of generics.
In addition, 77% lower odds for the brand’s preference over the generic were significantly correlated with thinking that they both have the same effectiveness. Nonetheless, people stating that the brands are better than generics had almost 60% more odd to prefer the brand. These results could be interpreted by the fact that people favoured the brand medicine for perceiving higher effectiveness due to the extended clinical and pharmacovigilance period. A study conducted in 2016 concluded that labelling a placebo tablet as a brand appeared to have a treatment benefit even in the absence of an active ingredient compared to the generic labelling due to the perceived better effectiveness. 30
Finally, when assessing the predictors of the acceptance of the substitution to generics, a higher acceptance was reported for university graduates in contradiction to a study from Bulgaria where the higher the level of education, the less they accept generic substitution. 9 In addition, people thinking that the generic is as effective as the brand had a 4.44 higher willingness to substitute to the generic alternative. Therefore, it is recommended to encourage pharmacists to suggest generic substitution by targeting those with a lower level of education to ameliorate their knowledge of the efficacy of generic drugs to facilitate their access to lower-cost medicines.
This study has limitations. It surveyed only one stratum, which may affect the extrapolation of the findings to the entire population. However, we conveniently sampled the participants after following proportional allocation from different centres and comparisons to the general population characteristics to increase the study’s external validity. This study also has strengths. Recall bias was minimised by providing sufficient time for the interviewees to answer the questionnaire. In contrast, interviewer bias was controlled by giving appropriate training to pharmacists collecting data across the different centres in Lebanon. The findings from this study may not reflect the current situation in Lebanon affected by the economic crisis, shortage and high cost of medicines. Therefore, further investigation should be done to assess people’s knowledge and perception towards generic drugs following the crisis.
Conclusion
A lack of knowledge and negative perceptions about generic drugs were noted after interpreting the participants’ responses. These misconceptions might lead to the limitation of the use of generic medicines in Lebanon, and therefore must be addressed. Accordingly, it is essential to empower patients with adequate information about the effectiveness and safety of generics and the advantages of their use through educational campaigns in different clinical settings. In addition, all healthcare professionals, especially physicians, should be actively involved in patient counselling and education, with a clear positive stance towards generics.
Supplemental Material
sj-docx-1-map-10.1177_27550834221147789 – Supplemental material for Knowledge, perception and acceptance of generic drugs in the general Lebanese population: A cross-sectional survey among adults
Supplemental material, sj-docx-1-map-10.1177_27550834221147789 for Knowledge, perception and acceptance of generic drugs in the general Lebanese population: A cross-sectional survey among adults by Georges Hatem, Rana Itani, Roula Ajrouche, Nour Abbas, Rita Farah, Mathijs Goossens and Sanaa Awada in The Journal of Medicine Access
Supplemental Material
sj-pdf-2-map-10.1177_27550834221147789 – Supplemental material for Knowledge, perception and acceptance of generic drugs in the general Lebanese population: A cross-sectional survey among adults
Supplemental material, sj-pdf-2-map-10.1177_27550834221147789 for Knowledge, perception and acceptance of generic drugs in the general Lebanese population: A cross-sectional survey among adults by Georges Hatem, Rana Itani, Roula Ajrouche, Nour Abbas, Rita Farah, Mathijs Goossens and Sanaa Awada in The Journal of Medicine Access
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.