
Abstract
Community-based early detection and intervention for NDDs has increasingly received prominence in public health research. Despite diagnostic opportunities, limited awareness of child development, social support and standardised care pathways delays diagnoses and access to services. Engaging lived experiences builds trust, improves quality and access to care. However, there is limited synthesised knowledge on involving lived experiences, especially those of autistic individuals and their caregivers, in conceptualising community awareness to promote service utilisation. This scoping review reports on community-engaged research methodologies employed within community-based programs to build awareness to promote early identification and intervention
Lay Abstract
There is an increasing number of community-based programmes for recognising early signs of autism and increasing access to interventions. However, despite the same, limited awareness of child development milestones, lack of social support and difficulty in accessing care pathways lead to a delay in finding the right help. Engaging with people who benefit from health programmes – including beneficiaries, people with lived experiences and related stakeholders before implementation has been suggested to improve programme engagement. However, there is little condensed knowledge about how to engage people with lived experience, especially those who are autistic or are caregivers of autistic adults in building awareness and subsequently lead to programmes that help with detection and intervention. This particular scoping review reports on studies that have successfully done this and asks and answers (to an extent) critical questions about – what level of engagement currently exists, how to engage (approaches, methods and tools), and when to engage. Currently, lived expertise is largely included after research priorities are already set, for example, designing interventions that researchers feel the need for a benefactor or population. This often leads to mismatched priorities for beneficiaries and excludes them from the design of programmes that directly benefit them. This paper suggests that stakeholders need to come together to build a taxonomy that ethically and meaningfully engages lived experience at different stages of research, whilst acknowledging the level of engagement possible and using appropriate approaches, methods and tools while building programmes for early detection and intervention.
Introduction
Globally, an estimated 52.9 million children under 5 years have a developmental disability with – autism and intellectual disability, resulting in high costs to individual and family functioning (Baxter et al., 2015; Global Research on Developmental Disabilities Collaborators et al., 2018; Krishnamurthy, 2008). Researchers increasingly recommend task-sharing models that use community resources to address the gap between increased reporting of NDDs and the costs of availing detection and intervention services (Bhavnani et al., 2022). Community-based screening has been effective in identifying NDDs in low-resource settings (Stewart & Lee, 2017). Despite the implementation of community-based programmes, stigma related to disclosing concerns related to NDDs persists, with low awareness of child development, limited social support and inconsistent practices in care pathways resulting in delays in seeking timely care or interventions when they exist (Divan et al., 2021; Turnock et al., 2022). Furthermore, following the deinstitutionalisation of individuals with disabilities in the 1980s, understanding choice and agency among families of children with NDDs became essential to improve health outcomes (Dyer et al., 1990; Minihan & Dean, 1990; Stancliffe et al., 2000). In response, community-engaged research strategies, which are “the process of working collaboratively with groups of people affiliated by geographic proximity, special interests, or similar situations to address issues affecting their well-being” offer researchers opportunities to create an environment of trust and improve quality and access to care (Clinical and Translational Science Awards Consortium, Community Engagement Key Function Committee Task Force on the Principles of Community Engagement, 2011, p. 21).
Community engagement broadly aims to involve and incorporate the perspectives of those being impacted by research and its outputs (Luger et al., 2020; Ohmer et al., 2022). Actively involving community members in research processes assists in developing practices that serve the needs of the community in conjunction with researchers (Clinical and Translational Science Awards Consortium, Community Engagement Key Function Committee Task Force on the Principles of Community Engagement, 2011; Kok et al., 2016; Kwon et al., 2018; Yardley et al., 2015). This, however, has gained limited momentum in autism research and as put forth by Cullingham et al. (2025), such an approach needs to be “grounded in iterative action oriented research and practice”. Adams et al. (2024) outline three levels of engagement: (i) involvement (one-way sharing from lived experience experts (LEE) to the researcher), (ii) consultation (two-way communication and LEE have input on decisions), and (iii) partnerships (LEE and researchers share decision-making). While community-engaged research is new in the field of NDDs, it has been used to design mental health interventions (Edwards et al., 2024), communication aids (Zolyomi & Snyder, 2023) and for autistic individuals, and in building awareness through advocacy research (Schuck & Fung, 2024).
This review aims to understand if these approaches can be scaled to support community programmes that promote service utilisation. Moreover, community engagement research methods are reportedly flexible and rely on case studies, qualitative inquiry or literature review (Luger, Hamilton & True, 2020). Thus, with the research question: “What community-engaged strategies are employed to involve lived experiences of autism and ID toward building awareness resources that lead to early intervention service uptake?” this review aims to report methodologies used in community-engaged research and programs to raise awareness through leveraging lived experiences to improve service utilisation for early identification and intervention.
Method
Protocol Registration
The protocol of the current review was created in adherence to PRISMA-ScR guidelines (Tricco et al., 2018) and was registered on the Open Science Framework (Malhotra et al., 2025; https://doi.org/10.17605/OSF.IO/XJRPA).
Search Strategy
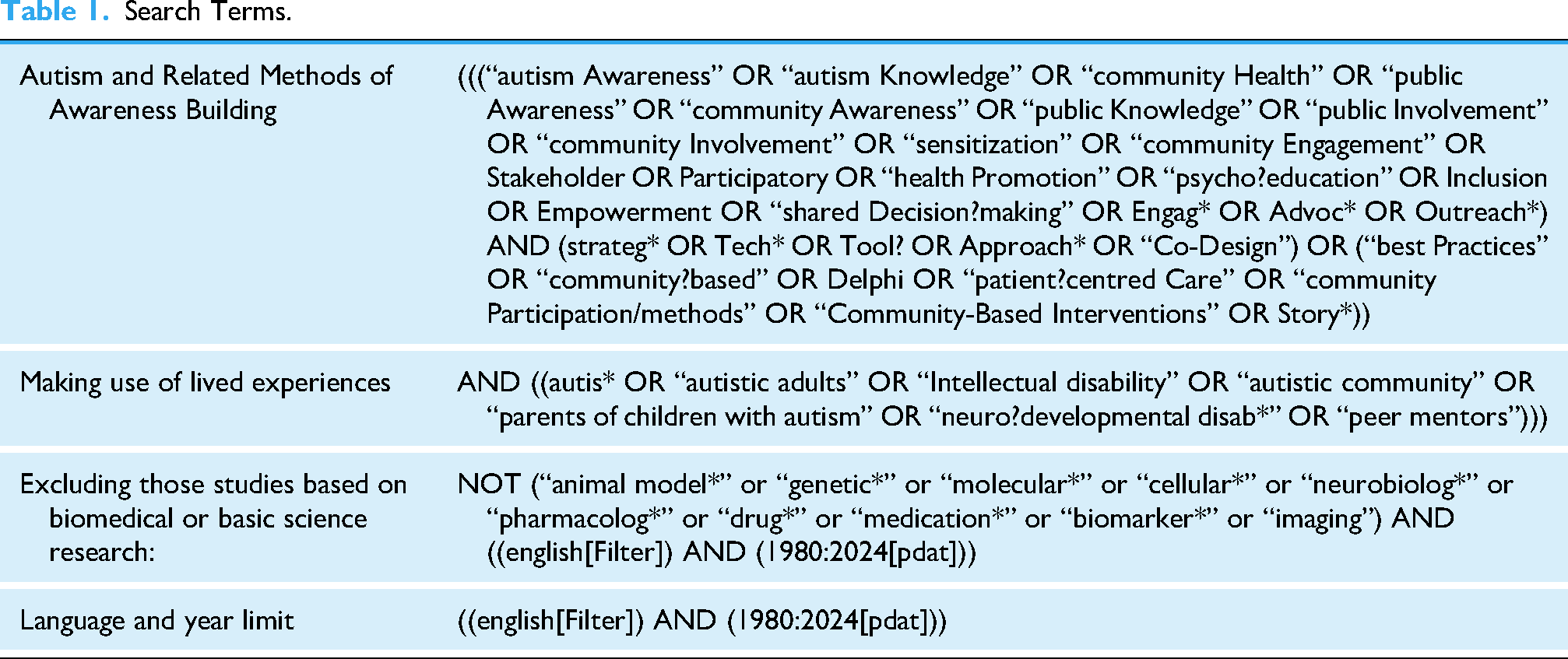
Four databases were selected (PubMed, Scopus, Web of Science, and Ovid for PsycInfo and PsycAPA articles) and helped to identify relevant keywords related to community awareness, community engagement and involvement methods, autism and intellectual disability. Initial results were saturated with information about biomedical and pure science studies, and hence, served as an exclusionary basis for further refining the strategy (Table 1). Full search terms for all databases are found in the supplementary section (Table S2 in the Supplementary materials).
Search Terms.
Inclusion and Exclusion Criteria
Studies were included if they met the following inclusion criteria:
(a) Published since 1980, (b) involved relevant stakeholders, with a focus on autistic individuals and their caregivers in the conceptualisation of awareness strategies, (c) reporting on the use of awareness strategies toward the promotion of early detection or intervention services. Beginning of deinstitutionalisation in the 1980s which led to advocacy for the needs of individuals with NDDs, especially focusing on choice-making, and finally involving individuals with lived experience to inform interventions developed for them and their community (Dyer et al., 1990; Minihan & Dean, 1990; Stancliffe et al., 2000). Studies were excluded if (a) recipients of interventions were above 18 years, (b) not in English due to a lack of resources for translation, or (c) purely biomedical or pure science studies.
Study Selection
BM and SP searched all four databases which can be found in the supplementary file. Consensus was achieved in getting the same results, and all identified references were uploaded into the Covidence systematic review software (Veritas Health Innovation, n.d.). The abstract screening comprised 5 reviewers, namely BM, SP, MM, RM and SS. Since COVIDENCE considers inter-rater reliability by default, disagreements on including an abstract were resolved in consultation with the entire team, with BM and SP as the deciding vote. BM, MM, RM and SS then proceeded to screen the full texts of selected abstracts. The included full-texts were extracted by two reviewers charting data and a third reviewer checking for data accuracy.
Few studies had the same authors, but it was unclear if one study preceded the other to inform CE. However, upon clarification by BM through email correspondence to these authors, as well as discussions with RR, it was understood that these were independent studies.
Data Charting
The Population, Concept, Context framework was adopted to chart data (Peters et al., 2015). Furthermore, the review will refer to the definitions in the Stakeholder Engagement Navigator Tool (Kwon et al., 2018) designed to guide researchers on suitable stakeholder engagement methods for translational and clinical research. This included:
Approaches: Organising frameworks used to define and understand stakeholders’ roles in decision-making, as well as in the conceptualisation, conduct, and dissemination of research. Methods: Specific tools, techniques, and processes that are employed to achieve “high-level” engagement. This involved identifying and convening stakeholders, creating reciprocal relationships (to level the playing field), engaging in bi-directional communication, eliciting perspectives, and making collaborative decisions over time. Tools: Specific activities for gathering information, facilitating group discussions, brainstorming, etc., utilised by the research teams.
An extraction sample is shared in Table 2 for the study:
Example of an Extraction.

Community-Engaged Research to Translate Developmental Screening and Referral Processes into Locally-Relevant, Family-Centered Language (Magnusson et al., 2020).
Additional methods and tools not included in the engagement navigator – such as workshops, interviews, consultations, and community health events – were also considered for a comprehensive understanding of engagement practices.
Role of Funding Source
The funding source had no role in the design, execution, analysis or interpretation of this research.
Results
The search yielded 23,961 references, of which 8286 were duplicates, leaving 15,673 abstracts (Figure 1). The study selection process was visualised using a PRISMA 2020 flow diagram created with an online tool (Haddaway et al., 2022). After screening, sixty-six abstracts underwent full-text review, of which 50 studies were excluded as they lacked an awareness strategy or focus on service promotion. Sixteen studies across design research, public health, community psychology, child development, anthropology, technology and disability health were included for final synthesis.

PRISMA Flow Chart for engaging individuals with lived experience of autism and intellectual disability towards developing community awareness to promote service utilisation for early identification and intervention.
Population Characteristics
Stakeholder groups: All 16 studies included in this review reported engagement with multiple stakeholder groups.
Including autistic individuals and caregivers, that is, Lived Experience Experts (LEE) Five out of 16 studies involved LEEs in different capacities; as advisors (n = 1) (Magaña et al., 2021) as participants (n = 1) (Gilbert et al., 2023) as co-researchers only (n = 1) (Ha et al., 2022), one study involved them in both an advisory and participatory capacity (Singla et al., 2024), and one involved LEE both as advisors and partners (Rutherford et al., 2021) Including caregivers Fifteen out of 16 studies included caregivers in different capacities; in a participatory role only (n = 5), (Gilbert et al., 2023; Grinker et al., 2015; Islam et al., 2018; Magnusson et al., 2020; Milgramm et al., 2022), as disclosers of autobiographical lived experience narrative in the form of video or other media (n = 2) (Codd et al., 2018; Johnson & Van Hecke, 2015), in a partnership role only (n = 2) (Brookman-Frazee et al., 2012; Peacock & Lin, 2012). The remaining six studies engaged caregivers in more than one capacity; as participants and partners (n = 2) (Wagner et al., 2023; Aabe et al., 2019), as advisors and partners (n = 2) (Rabba et al., 2020; Rutherford et al., 2021) as participants and advisors (n = 2) (Magaña et al., 2021; Singla et al., 2024)
Caregiver characteristics: fifteen of the 16 studies engaged caregivers, such as mothers, fathers, grandparents or families of children with NDDs; five studies involved mothers only (Aabe et al., 2019; Codd et al., 2018; Gilbert et al., 2023; Grinker et al., 2015; Wagner et al., 2023), two involved both mothers and fathers (Rabba et al., 2020; Singla et al., 2024), and one involved mothers and grandmothers (Magnusson et al., 2020). One study consisting of four programmes included mothers, fathers and grandmothers (Magaña et al., 2021). The study by Gilbert and colleagues also included unspecified female caregivers (Gilbert et al., 2023). Six did not report on the sex of the caregivers (Brookman-Frazee et al., 2012; Islam et al., 2018; Johnson & Van Hecke, 2015; Milgramm et al., 2022; Peacock & Lin, 2012; Rutherford et al., 2021). Only three studies reported the ages of the caregivers (26.1–54 years) (Gilbert et al., 2023; Islam et al., 2018; Singla et al., 2024).
Studies within HICs also focused on racial or ethnic minorities such as the Korean-American community in New York (Grinker et al., 2015), the local Somali community in Bristol, UK (Aabe et al., 2019), members from the black community in the USA (Johnson & Van Hecke, 2015) and caregivers from multiple communities were represented in one study.
Concept
All studies report on either approaches, methods, tools or all three, to engage relevant stakeholders. Based on these, they were also classified at the level of engagement they offer, as shown in Table 3.
Levels of Engagement.

Approaches
CBPR was the most frequently utilised approach, appearing in three studies (Aabe et al., 2019; Brookman-Frazee et al., 2012; Magnusson et al., 2020). One study used cultural adaptation in addition to CBPR and the Ecological Validity Framework across four programmes (Magaña et al., 2021). Out of 16 studies, two attempted to approach their objectives by keeping culture/cultural relevance at the fore, for example, by using cultural consensus (Grinker et al., 2015; Johnson & Van Hecke, 2015). Eight out of 16 other approaches included participatory action research (PAR) (Brookman-Frazee et al., 2012), Medical Research Council Framework (Rutherford et al., 2021), “Consulting End Users About Their Needs to Target the Needs of Potential Users” (Singla et al., 2024) identifying participants’ experiences (Gilbert et al., 2023) community involvement (Ha et al., 2022), patient-centredness (Codd et al., 2018) and Consolidated Framework for Implementation Research (CFIR) (Wagner et al., 2023). Three studies did not elucidate their approach to engage stakeholders (Islam et al., 2018; Milgramm et al., 2022; Peacock & Lin, 2012).
Methods
Half (8) of the studies used collaborative partnerships: including advisory boards (Rutherford et al., 2021), multistakeholder partnerships (Aabe et al., 2019; Rabba et al., 2020), community partnerships with campus researchers (Brookman-Frazee et al., 2012; Magnusson et al., 2020), advisory boards alongside multistakeholder partnerships including LEEs (Magaña et al., 2021), advisory boards and lived experience consultations (Singla et al., 2024), and lived experience consultations with community partnerships with campus researchers (Wagner et al., 2023).
Three studies utilised needs assessment/analysis (Gilbert et al., 2023; Grinker et al., 2015; Islam et al., 2018) and two sought feedback from stakeholders for strategy refinement (Grinker et al., 2015; Ha et al., 2022). Other methods included: Boot Camp Translation (BCT) in conjunction with active learning strategies (Magnusson et al., 2020), regional summits (Peacock & Lin, 2012), and ethnographic inquiries (Grinker et al., 2015). Two studies involved LEEs by using an autobiographical narrative (Codd et al., 2018; Johnson & Van Hecke, 2015).
Tools
Six studies used interviews: two mentioned interviews (Codd et al., 2018; Magaña et al., 2021), two mentioned in-depth interviews (Aabe et al., 2019; Grinker et al., 2015), one reported using individual or group, semi-structured interviews (Rutherford et al., 2021) and one reported cultural consensus modelling interviews alongside unstructured interviews (Grinker et al., 2015). Grinker et al. (2025) also used free-listing, ranking and piles-sorting.
Five out of 16 studies reported using group formats to facilitate engagement; two studies employed small group discussions (Magnusson et al., 2020; Rutherford et al., 2021) with Magnusson et al. (2020) additionally using problem-based learning and teach-back strategies, and conference calls, and three studies used focus group discussions (Gilbert et al., 2023; Magaña et al., 2021; Wagner et al., 2023). One study reported using iterative participatory design workshops through individual and/or group meetings, engaging in knowledge translation sessions through group and individual meetings, alongside feedback cycles on the output developed in the study (Rabba et al., 2020). Other tools reported in five out of 16 studies included documenting an autobiographical video (Johnson & Van Hecke, 2015), personal communication (Brookman-Frazee et al., 2012; Rutherford et al., 2021), expert presentations alongside interactive discussions and logic model development (Peacock & Lin, 2012) and peer review and participation (Ha et al., 2022). Brookman-Frazee et al. (2012) additionally utilised a collaborative process committee as a tool.
Context
Fifteen out of 16 studies were from high-income countries: ten were from North America (USA and Canada), three from Europe (UK), and two from Australia. Only one study was based in an LMIC, in South Asia (Bangladesh).
Discussion
Lived experience involvement is increasingly considered a good research practice, with the UK's National Health Service requiring research applications to explain this across methodologies and disciplines (Wright et al., 2010). While this is an important approach, it can also lead to a tokenistic representation of service users if they do not fit in with the needs of the research. To ensure relevant representation, the global health community focussed on neurodiversity needs to consider the following questions toward fair and equitable community-engaged research: Whose lived experience is involved in building community-engaged awareness materials towards service uptake? How are people with lived experience involved? When is lived experience included in the research cycle and whose interest is prioritised?
Whose lived experience is involved in building community-engaged awareness materials towards service uptake?
Currently, as parents/caregivers are the first point of advocacy in autism and neurodevelopmental disabilities, this population is widely approached and involved in designing awareness efforts towards improving uptake of detection and intervention services. Autistic adults and children are also involved in studies. During our search, we did not limit ourselves to the global north. However, as with most public health studies, the studies included in the current review focussed on White, Educated, Industrialised, Rich and Democratic populations, which represent only 12% of the global population (Henrich et al., 2010). All but one study came from an HIC, with only four out of the 15 studies (Aabe et al., 2019; Grinker et al., 2015; Johnson & Van Hecke, 2015; Magaña et al., 2021) focussing on disadvantaged racial and ethnic communities in the USA, Canada, and England. Greater investment is needed to support LMIC-based researchers in conducting research in their local context, which goes beyond “parachute research” that is, “drop into a country, make use of the local infrastructure, personnel, and patients, and then go home and writes an academic paper for a prestigious journal” (The Lancet Global Health, 2018). For health to be truly global, equitable and representative, researchers need to build partnerships with LEEs, LMICs and LEEs in LMICs to bridge knowledge gaps, address disparities in health service provision, and lack of infrastructure and resources.
How are People with Lived Experience Involved?
Researchers’ have dominantly involved lived experiences to fit into their research question or programme requirements rather than as stakeholders who may drive research priorities. For example, Johnson and Van Hecke (2015) recorded an autistic child to improve content relevance for training inner-city church ambassadors on autism knowledge and attitude for an awareness session.
However, in the backdrop of the evolving neurodiversity movement, we see active involvement of LEEs in leading and partnering with academicians. LEE-led partnerships may be involved to serve as a bridge when cultural differences exist between researchers and the study population, as demonstrated by Magaña et al. (2021), Grinker et al. (2015) and Aabe et al. (2019). Advisement and feedback from LEEs with intersecting identities based in sex, culture, disability, immigration experiences may be involved to build relevant local adaptation of interventions and study materials to improve service utilisation, such as by Magnusson et al. (2020), and Singla et al. (2024), Rutherford et al. (2021), Rabba et al. (2020). LEEs may be involved as participants sharing their internal and subjective experiences shaping the resources that may be used by researchers to support community building, promoting services that lead to service uptake, as seen in the studies by Gilbert et al. (2023), Ha et al. (2022) and Johnson and Van Hecke (2015).
When is Lived Experience Included in the Research Cycle and Whose Interest is Prioritised?
In the current review, studies utilised lived experience at the
Co-production of global research with representation from the Global South and marginalised identities can help build relevant programmes and services which align with community priorities and lead to service uptake.
Partnerships of this kind offer deep and meaningful engagement with the community. Combining the researcher's expertise and lived experience enriches the process and outputs for all stakeholders. Considering the subjectivity of community-engaged research, researchers should reflect on the choices made in the research design, including which population was involved, how they were recruited, and how these choices impacted data collected and dissemination (Wright et al., 2010).
For example, Aabe's co-researcher reflects within the study reported: I felt reassured that her lived experience would be critical to bridge the gap between myself, an unknown researcher, and Somali parents affected by autism.
The review also brings forth questions on methodology toward building these partnerships and involving community members. Our findings corroborate with our introduction, that is, community-engaged methodologies are flexible in nature. However, studies with different nomenclature often report on the same process. For example, the process of Singla et al. (2024) consulting with end users, that is, final beneficiaries throughout the research is resonant of community-based participatory research (CBPR) as an approach (Collins et al., 2018). Building a taxonomy of approaches, methods and tools across fields such as design research, public health, community psychology, child development, anthropology, technology and disability health, can help researchers determine the level of engagement throughout the research cycle. An example of such a taxonomy based on this review is exemplified in Table S5 attached in the supplementary file.
Limitations
While the stakeholder navigator tool helped conceptualise current practices using approaches, methods and tools, these definitions are still susceptible to diverse interpretation based on one's lived experience or career exposure. The authors note that the current review does not consider grey literature or published reports about public and community engagement. Additionally, the current review is set within the context of Neurodevelopment and Autism in South Asia: Treatment and Evidence (NAMASTE) programme and is focused on service utilisation for early identification and intervention. Future research may benefit from identifying engagement practices to include lived experiences for community awareness for a variety of outcomes such as inclusion and intervention development as per community priorities.
Conclusions
In the current review, studies have reported on different strategies, which the current review has classified as approaches, methods and tools. Equitable decision-making is facilitated by using CBPR, involving lived experience advisors and experts, and the lived experiences of primary caregivers improve the design of research studies, enrich participant recruitment, research activities and dissemination activities. Researchers may benefit from building a taxonomy of community-engaged research strategies based on levels of engagement and corresponding methodologies (approaches, methods and tools) to answer critical questions underlying power sharing within community engagement.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330261432270 - Supplemental material for Community engagement with individuals with lived experience of autism and intellectual disability to promote awareness and service utilisation for early identification and intervention: A scoping review
Supplemental material, sj-docx-1-ndy-10.1177_27546330261432270 for Community engagement with individuals with lived experience of autism and intellectual disability to promote awareness and service utilisation for early identification and intervention: A scoping review by Bhavya Malhotra, Sweta Pal, Manya Mishra, Riya Mitra, Sanjna Shukla, Kathy Leadbitter, Jonathan Green, Gauri Divan, Reetabrata Roy and in Neurodiversity
Footnotes
Abbreviations
Ethical Approval and Informed Consent
No ethical approval was required, considering it was a scoping review and did not involve direct participation of human subjects.
Author Contributions
Bhavya Malhotra contributed to conceptualisation, data curation, investigation, methodology, visualisation, project administration, and writing–original draft preparation; Sweta Pal contributed to conceptualisation, investigation, methodology, and writing–review and editing; Manya Mishra contributed to data curation and investigation; Riya Mitra contributed to data curation and investigation; Sanjna Shukla contributed to data curation and investigation; Kathy Leadbitter contributed to supervision and writing–review and editing; Jonathan Green contributed to supervision, and writing–review and editing; Gauri Divan contributed to conceptualisation, supervision, and writing–review and editing; Reetabrata Roy contributed to supervision and review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the NIHR (NIHR134702) using UK international development funding from the UK Government to support global health research. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the UK government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data are available in the manuscript and supplementary files.
Community Involvement
The first author (BM) identifies as a neurodivergent individual with lived experience of ADHD.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.