
Abstract
Children who have experienced adverse childhood experiences (ACEs) often present with emotional and behavioral characteristics that overlap with attention-deficit/hyperactivity disorder (ADHD), yet it remains unclear which trauma-related needs uniquely distinguish children with and without ACEs. Using data from 10,869 children receiving services in a statewide public mental health system, we compared children with ADHD and ACEs (ADHD + ACE) (n = 6,024) to those without ACEs (ADHD-only) (n = 4,845) on trauma-related emotional, behavioral, and risk behavior domains from the Child and Adolescent Needs and Strengths (CANS) assessment. Attachment difficulties, traumatic grief/separation, depression, oppositional behavior, self-mutilation, danger to others, poor judgment, and sexually reactive behavior independently predicted greater odds of ADHD + ACE classification. In contrast, attention/concentration difficulties and behavioral regressions were negatively associated with ADHD + ACE status, suggesting that when trauma-related emotional and risk behavior needs are jointly considered, ADHD-only profiles may be characterized by narrower attentional and behavioral regression concerns. Older age was also associated with higher likelihood of ADHD + ACE classification. Findings highlight a trauma-related dysregulation phenotype among children with ADHD + ACE and underscore the importance of trauma-responsive, developmentally informed, and dimensional assessment in mental health systems, rather than relying solely on attention when conceptualizing ADHD.
Lay Abstract
Many children live with both attention-deficit/hyperactivity disorder (ADHD) and difficult early life experiences, often called Adverse Childhood Experiences (ACEs). These can include different kinds of abuse, neglect, family violence, or other serious stressors. Because trauma can affect attention, mood, and behavior, it can be hard to tell when a child's struggles are mainly related to ADHD, trauma, or both. In this study, we looked at information from more than 10,000 children who were receiving services in a public mental health system and had an ADHD diagnosis. Using a widely used clinical tool (the Child and Adolescent Needs and Strengths, or CANS), we compared two groups: children with ADHD who also had documented ACEs, and children with ADHD without documented ACEs. We found that children with both ADHD and ACEs were more likely to have difficulties with attachment and relationships, grief and separation, depression, oppositional behavior, self-harm, harming others, poor judgment, and sexually reactive behavior. In contrast, when we considered all needs at the same time, attention, and concentration problems were more characteristic of children with ADHD without ACEs. Older children were also more likely to have both ADHD and ACEs. Overall, our findings suggest a distinct “trauma-related dysregulation” pattern within ADHD. This highlights the need for mental health systems to routinely assess trauma, to use dimensional and strengths-based tools, and to offer trauma-responsive supports rather than assuming that all challenging behaviors in neurodivergent children are “just ADHD.”
Adverse childhood experiences (ACEs), including physical, emotional, and sexual abuse, neglect, and exposure to violence, are common and have far-reaching consequences for development and long-term well-being (Brown et al., 2017). A substantial body of work demonstrates that ACEs are associated with emotional and behavioral difficulties, such as anxiety, concentration, impulsivity, and mood (D'Andrea et al., 2012; Felitti et al., 1998; Jimenez et al., 2017; Wang et al., 2020). Many of these characteristics resemble core features of attention-deficit hyperactivity disorder (ADHD), a neurodevelopmental condition characterized by persistent difficulties with attention, activity level, and impulse control that currently affects an estimated 7 million children in the United States (Armstrong, 2023; D'Andrea et al., 2012; Danielson et al., 2024; Posner et al., 2020).
The overlap between ACE-related responses and ADHD characteristics has led to concerns about under-recognition of trauma and treatment approaches that may not adequately address underlying needs (Armstrong, 2023; McDonald & Ingram, 2025; Siegfried & Blackshear, 2016). Trauma-exposed children often display behaviors, such as hypervigilance, emotional dysregulation, dissociation, and lack of concentration, that resemble ADHD symptoms (Courtois, 2004; D'Andrea et al., 2012; Ford, 2002; Herman, 2017; Ruiz, 2014). For example, intrusive memories, physiological hyperarousal, and difficulties with emotion regulation following trauma can appear as inattention, restlessness, or impulsivity in settings where children are expected to sustain focus (Harrison & Wilson, 2005; Ruiz, 2014). Conversely, trauma-related withdrawal or dissociation may be misinterpreted as inattentive presentation of ADHD (D'Andrea et al., 2012; Herman, 2017).
Consistent with the behavioral overlap between trauma and ADHD, existing research documents the high co-occurrence of trauma exposure and ADHD diagnoses (Burke et al., 2011; Burke-Harris, 2018; van der Kolk et al., 2005). Children with ADHD are more likely than their peers to have experienced maltreatment or household adversities (Biederman et al., 2013; Fuller-Thomson & Lewis, 2015; Sanderud et al., 2016). Children with trauma histories are also more likely to receive an ADHD diagnosis, underscoring the importance of distinguishing trauma-related symptoms from core ADHD features (Jimenez et al., 2017; Zhang et al., 2022). Yet despite this well-documented overlap, little is known about which trauma-related emotional, behavioral, and risk behavior needs uniquely differentiate children with ADHD who have ACE histories from those without such histories. Differentiating between ADHD and trauma-related profiles has critical implications. Standard ADHD interventions, including stimulant medication and behavioral modification strategies, may be insufficient or inappropriate when children's difficulties stem from trauma exposure (Mayes et al., 2008). Trauma-responsive care requires identifying specific trauma-related needs that co-occur with ADHD to ensure accurate assessment and appropriate intervention (Cassidy, 2015; Herman, 2017).
The Present Study
There is a significant gap regarding which specific trauma-related needs most clearly distinguish children with ADHD who also have ACE histories from those without such histories. Identifying these differentiating features could support more precise assessment, reduce misdiagnosis, and inform trauma-responsive care pathways for children with ADHD. The present study addresses this gap by examining a large, statewide sample of children diagnosed with ADHD to identify the trauma-related domains that uniquely differentiate those with ACE histories from those without ACE histories. Building on dimensional, strength-based assessment principles (Altschuler & Lyons, 2024), this study investigates whether specific emotional, behavioral, and risk behavior needs identified in prior trauma literature predict ADHD + ACE status above and beyond core ADHD characteristics. This approach allows us to determine whether ADHD with trauma exposure reflects a distinct phenotype.
Methods
Language and Positionality
We acknowledge variation in preferences for language in the neurodivergent communities more broadly and selected to use terms (e.g., ADHD diagnosis, neurodivergent, characteristics, and difficulties) consistent with the preferences identified by many neurodivergent individuals (Botha et al., 2023; Bottema-Beutel et al., 2021; Bury et al., 2023; Gernsbacher, 2017; Keates et al., 2025; Keating et al., 2023; Werkhoven et al., 2022). Although not the focus of the present study, we chose to use the term gender/sex when referencing this construct in our modeling specifications, which reflects expansive conceptualizations of gender/sex that highlight their multidimensional, complex, interactive, and dynamic nature (Hyde et al., 2019). Cisgender and transgender males/females were identified and included in the sample. Furthermore, we conducted this research from the lens of our lived experiences, such that the senior author has been diagnosed with ADHD and other neurodivergent conditions (Fletcher-Watson et al., 2019), while the lead author is a licensed mental health clinician with extensive experience diagnosing and providing therapeutic support to children with ADHD and ACEs.
Data Source and Sample
The Child and Adolescent Needs and Strengths Assessment (CANS) is an evidence-based, person-centered assessment that measures the functional wellness (dimensional needs and strengths) of children (Lyons, 2009, 2022). Developed from the Childhood Severity of Psychiatric Illness, the CANS was designed to assist mental health professionals in making treatment decisions by comprehensively assessing children in different stages of development and cultures with emotional and behavioral health needs, learning and developmental disabilities, and juvenile systems involvement (Lyons et al., 1999). Credentialed healthcare providers, such as mental health clinicians and social workers, can administer the CANS after completing a certification training that is renewed annually (Anderson et al., 2003; Dilly et al., 2007; Kisiel et al., 2017; Lyons, 2009, 2022; Spinelli et al., 2023). The CANS used in this study consisted of 150 items rated on four-point action levels from 0 to 3 across eight (8) domains. Those domains are “Traumatic/Adverse Childhood Experiences”, “Strengths”, “Life Functioning”, “Culture”, “Behavioral/Emotional Needs”, “Risk Behaviors”, “Transition to Adulthood”, and “Caregiver Resources and Needs”. The complete CANS manual is available upon request from the corresponding author. As an example, the “Sexual Abuse” item describes the child's experience of sexual abuse and is rated from 0 (“no evidence”) to 3 (“severe or chronic sexual abuse”) based on the frequency, severity, and consequences of the abuse.
The analytical sample included 10,869 children receiving mental health services in a public mental health system in a western state in the United States. From April 2023 to April 2025, incoming children were given the CANS by a team of trained professionals. ADHD diagnoses were determined by International Classification for Disease-10 (ICD-10) codes (F90.0, F90.1, F90.2, F90.8, or F90.9), rated by clinicians.
Adverse Childhood Experiences
The Traumatic/Adverse Childhood Experiences domain of the CANS consisted of items that identified whether or not the child had experienced ACEs. Items used were: “Sexual Abuse”, “Physical Abuse”, “Emotional Abuse”, “Neglect”, “Medical Trauma”, “Witness to Family Violence”, “Witness to Community Violence”, “Witness to School Violence”, “Natural or Manmade Disasters”, “War Affected”, “Terrorism Affected”, “Witness/Victim to Criminal Activity”, “Parental Criminal Behavior”, “Disruption in Caregiving/Attachment Losses”, and “Systems Involvement” (Lyons et al., 1999). Each item was rated on a four-point scale: 0 = “No evidence of any trauma of this type,” 1 = “Single incident of trauma occurred or suspicion exists,” 2 = “Multiple incidents or moderate degree of this trauma type,” and 3 = “Repeated and severe incidents with medical/physical consequences.” To classify ACE exposure, scores of 2 or 3 on any ACE item were coded as “Yes” (ACE present), and scores of 0 or 1 were coded as “No” (ACE not present). This classification ensured that suspicion alone (rating of 1) was not considered evidence of ACE exposure for the purposes of this study.
CANS Needs/Predictor Variables
The primary predictor variables for this study were CANS items from the Behavioral/Emotional Needs and Risk Behaviors domains that map onto trauma-related responses identified in prior research (APA, 2022; Badour & Feldner, 2013; Barlow et al., 2004; Bonn-Miller et al., 2011; Briscoe-Smith & Hinshaw, 2006; Courtois, 2004; D'Andrea et al., 2012; Ehring & Quack, 2010; Fuller-Thomson & Lewis, 2015; Gonzalez et al., 2019; Harrison & Wilson, 2005; Herman, 2017; Jeong et al., 2021; Jimenez et al., 2017; Kulkarni et al., 2013; Lilly & Lim, 2013; Lyons-Ruth et al., 2013; Plieger & Reuter, 2020; Ruiz, 2014; SAMHSA, 2014; Shonkoff & Garner, 2012; Siegfried & Blackshear, 2016; Thomas, 1995; Trickett et al., 2011; Tull et al., 2007; Wang et al., 2020; Zhang et al., 2022). Table 1 outlines those trauma responses and the research studies that identified the responses. The Behavioral/Emotional Needs items were (1) “Emotional and/or Physical Regulation,” (2) “Attention/Concentration,” (3) “Impulsivity,” (4) “Depression,” (5) “Attachment Difficulties,” (6) “Behavioral Regressions,” (7) “Somatization,” (8) “Anxiety,” (9) “Oppositional Behavior,” (10) “Anger Control,” (11) “Mood Disturbance,” and (12) “Traumatic Grief & Separation.” The variables in the Risk Behaviors Domain examined were (13) “Self-mutilation,” (14) “Danger to Others,” (15) “Sexual Aggression,” (16) “Judgment,” (17) “Intentional Misbehavior,” (18) “Sexually Reactive Behavior.” These items were selected to match the responses of childhood trauma exposure that have been identified in the literature. Each item was rated on a four-point action scale: 0 = “No current need; no need for action or intervention,” 1 = “History or suspicion of problems; requires monitoring or preventive activities,” 2 = “Problem is interfering with functioning; requires action or intervention,” and 3 = “Problem is dangerous or disabling; requires immediate and/or intensive action.”
Summary of Studies That Identified Trauma Responses.
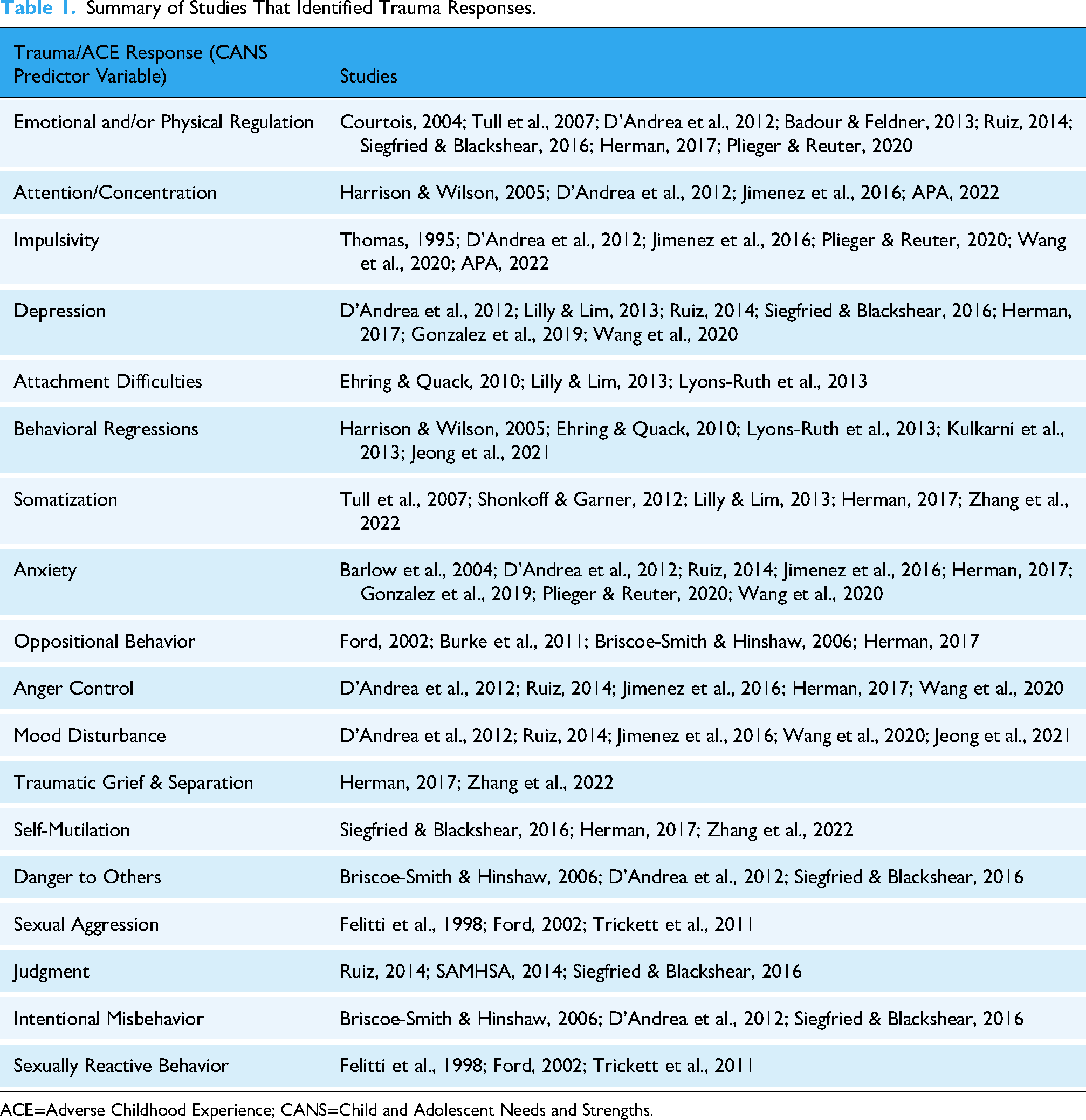
ACE=Adverse Childhood Experience; CANS=Child and Adolescent Needs and Strengths.
ADHD With ACE Versus ADHD Without ACE
We created two mutually exclusive groups based on ACE exposure among children with ADHD diagnoses. Group 1 (ADHD + ACE) included children with ADHD and a rating of 2 or 3 (“Yes”) on at least one ACE exposure item (N = 6,024). Group 2 (ADHD-only) included children with ADHD and ratings of 0 or 1 (“No”) on all ACE exposure items (N = 4,845).
Analytical Approach
Analyses were conducted in R Version 4.4.1. We first examined descriptive statistics and group differences between ADHD + ACE and ADHD-only children on demographic variables. Age differences were evaluated using analysis of variance (ANOVA), and categorical demographic variables (gender/sex, race, and ethnicity) were compared across groups using chi-square tests. Next, we compared ADHD + ACE and ADHD-only groups on each of the 18 CANS trauma-related Behavioral/Emotional Needs and Risk Behaviors domains using bivariate ANOVAs. These bivariate tests were used descriptively to characterize the overall pattern and magnitude of group differences across domains rather than as primary inferential tests. Our primary inferential analysis was a single multivariate logistic regression model predicting ADHD + ACE status (1 = ADHD + ACE, 0 = ADHD-only) from all 18 trauma-related CANS domains entered simultaneously, with age, gender/sex, and race included as covariates. This approach, which has been used in prior work examining ADHD and ACE/trauma exposure (Bomysoad & Francis, 2020; Crouch et al., 2021; Khanijahani & Sualp, 2022; Walker et al., 2021), allowed us to identify domains that uniquely differentiate ADHD + ACE from ADHD-only while adjusting for co-occurring needs.
We assessed multicollinearity using variance inflation factors (VIFs), which ranged from 1.00 to 1.22, indicating very low multicollinearity and supporting the inclusion of all domains in a single model (Kutner et al., 2004; O’Brien, 2007). Because the trauma-related domains reflect clinically distinct constructs that are assessed independently in the CANS, we did not perform dimension-reduction techniques, and instead prioritized interpretability of individual domains for clinical decision making. Model fit indices (pseudo-R2) are reported to describe variance accounted for in ADHD + ACE status. Given the large sample size and the number of bivariate comparisons, we focus on the pattern and direction of effects and on the multivariate model when drawing substantive conclusions, rather than on isolated p-values from the bivariate tests.
Results
Table 2 presents demographic information for children with ADHD-only and ADHD + ACE. Children with ADHD + ACE were, on average, older than children with ADHD-only (M = 11.3 vs. 10.2 years), and this difference was statistically significant, F(1, 10,867) = 287.4, p < 0.001. Gender/sex distributions also differed by group, χ2(3) = 19.1, p < 0.001, with a somewhat higher proportion of cisgender females and transgender youth in the ADHD + ACE group, although cisgender males comprised the majority in both groups. Race was significantly associated with group status, χ2(5) = 43.3, p < 0.001; for example, children categorized in “other” or multiracial racial groups were somewhat less likely to be in the ADHD + ACE group. Ethnicity was not significantly related to ADHD + ACE status, χ2(1) = 0.0, p = 0.973. These findings suggest that demographic characteristics, particularly age, gender/sex, and race, are important to consider when examining ADHD with and without ACE exposure.
Demographic Characteristics of Children With ADHD With and Without ACEs.

Note. ACE=adverse childhood experience; ADHD=attention-deficit/hyperactivity disorder; AFR = African American; ASN = Asian; EUR = European; HSP = Hispanic; NAT = Native American; NSP = non-Hispanic; PAC = Pacific Islander; RCO = Other; SXF = Cisgender Female; SXM = Cisgender Male; TSF = Transgender Female; TSM = Transgender Male.
Table 3 summarizes group differences across the 18 CANS trauma-related Behavioral/Emotional Needs and Risk Behaviors domains. Across nearly all domains, children with ADHD + ACE had higher mean scores than children with ADHD-only, indicating more needs among those with ACE exposure.
CANS Trauma-Related Domains by Group.

Note. *** = p < 0.001.
ACE=Adverse Childhood Experiences; ADHD=Attention-Deficit/Hyperactivity Disorder; CANS=Child and Adolescent Needs and Strengths.
To identify which trauma-related domains uniquely distinguished ADHD + ACE from ADHD-only, we estimated a multivariate logistic regression model including all 18 CANS domains and covariates for age, sex, and race (Table 4). Multicollinearity was low (VIF range = 1.00–1.22), supporting the inclusion of all predictors in a single model. The overall multivariate logistic regression model was statistically significant, χ2(27) = 2344.42, p < 0.001, and accounted for approximately 21% of the variance in ADHD + ACE status (pseudo-R2 = .21). In the multivariate model that included all 18 trauma-related domains and demographic covariates, several domains showed robust positive associations with ADHD + ACE status. Traumatic grief/separation was strongly associated with ADHD + ACE classification (β = 1.19, odds ratio [OR] = 3.29, 95% confidence interval [CI] [2.99, 3.63], p < 0.001), indicating that children with greater traumatic grief and separation-related needs were more than three times as likely to be in the ADHD + ACE group. Attachment difficulties were also strongly associated with ADHD + ACE status (β = 0.71, OR = 2.03, 95% CI [1.84, 2.23], p < 0.001), doubling the odds of being in the ADHD + ACE group. Sexually reactive behavior showed a similarly large unique association (β = 0.96, OR = 2.62, 95% CI [2.08, 3.31], p < 0.001). Elevated depression (β = 0.36, OR = 1.44, 95% CI [1.29, 1.60], p < 0.001), oppositional behavior (β = 0.25, OR = 1.28, 95% CI [1.13, 1.45], p < 0.001), self-mutilation (β = 0.33, OR = 1.39, 95% CI [1.24, 1.56], p < 0.001), danger to others (β = 0.28, OR = 1.32, 95% CI [1.19, 1.47], p < 0.001), and judgment problems (β = 0.26, OR = 1.29, 95% CI [1.16, 1.44], p < 0.001) were also uniquely associated with a higher likelihood of ADHD + ACE classification. In contrast, two domains were negatively associated with ADHD + ACE status in the multivariate model. Attention/concentration difficulties were associated with lower odds of ADHD + ACE classification when controlling for other needs (β = −0.33, OR = 0.72, 95% CI [0.53, 0.97], p = 0.032), suggesting that more prominent attentional concerns may be relatively more characteristic of ADHD-only presentations when trauma-related domains are jointly considered. Behavioral regressions were also modestly negatively associated with ADHD + ACE status (β = −0.13, OR = 0.88, 95% CI [0.79, 0.98], p = 0.018). Other domains (e.g., emotional/physical regulation, anxiety, somatization, anger control, mood disturbance, sexual aggression, and intentional misbehavior) were not uniquely associated with ADHD + ACE status in the multivariate model once covariates and co-occurring domains were controlled.
Multivariate Logistic Regression Predicting ADHD + ACE Versus ADHD (Adjusting for Age, Sex, and Race).
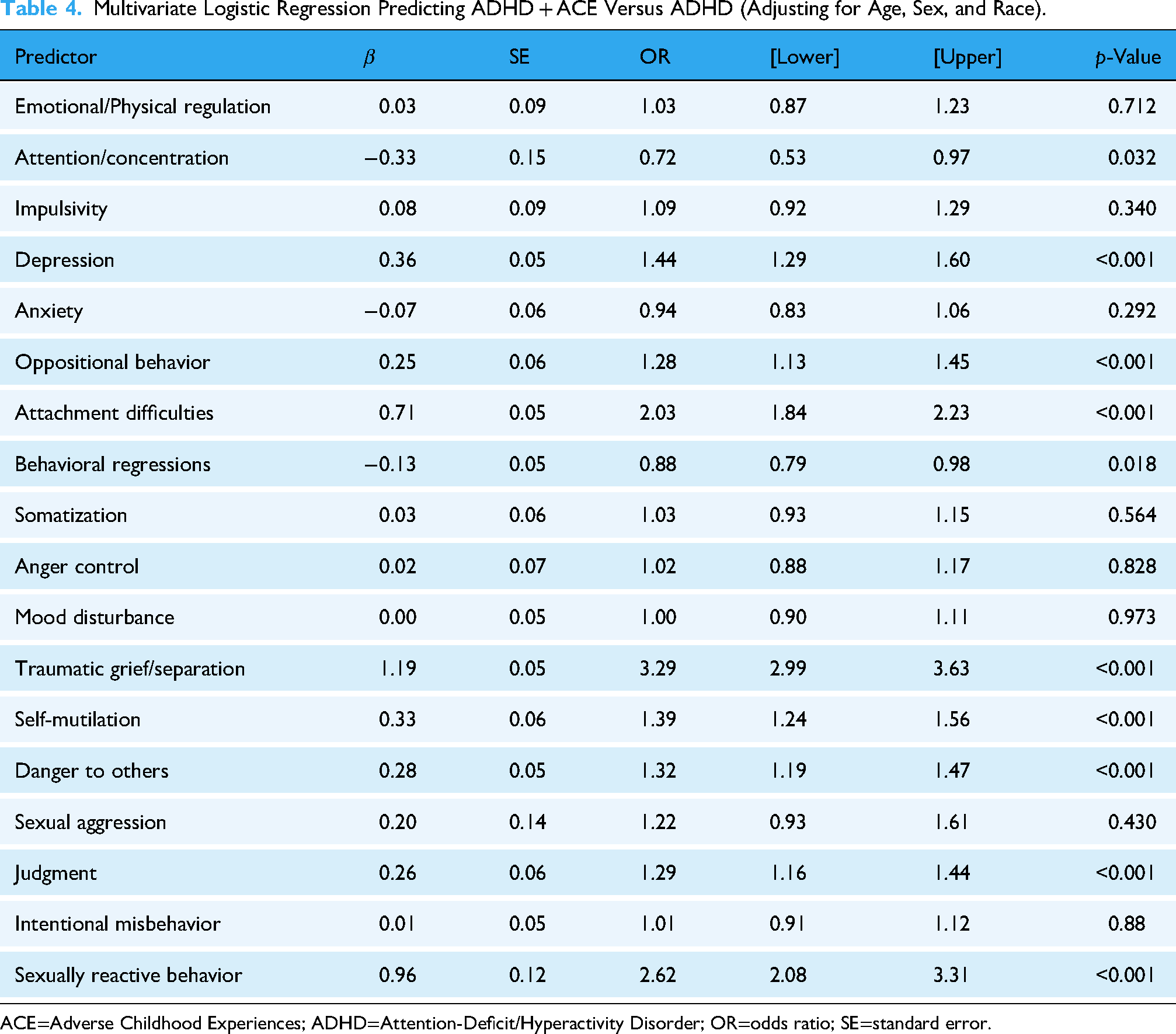
ACE=Adverse Childhood Experiences; ADHD=Attention-Deficit/Hyperactivity Disorder; OR=odds ratio; SE=standard error.
Discussion
This study examined which trauma-related emotional, behavioral, and risk behavior needs uniquely differentiate children diagnosed with ADHD who have adverse childhood experiences (ADHD + ACE) from those without ACE exposure (ADHD-only) in a large, statewide public mental health system. Consistent with extensive literature documenting overlap between trauma responses and ADHD characteristics (Szymanski et al., 2011), children in the ADHD + ACE group showed higher needs across nearly all CANS trauma-related domains at the bivariate level. However, the multivariate model revealed a more specific pattern: only a subset of domains—particularly attachment difficulties, traumatic grief/separation, depression, oppositional behavior, and multiple risk behaviors (self-mutilation, danger to others, judgment problems, and sexually reactive behavior)—independently predicted ADHD + ACE status after accounting for demographics and co-occurring needs. Together, these findings support a trauma-related dysregulation phenotype among children with ADHD and ACE histories. Where prior work has typically focused on ACE counts or broad comorbidities among youth with ADHD, this study extends that literature by pinpointing specific trauma-related domains on a widely used functional assessment that distinguish ADHD + ACE from ADHD-only presentations within a public mental health system. This pattern suggests that ACE exposure is not simply associated with greater overall severity among children with ADHD, but with a particular constellation of attachment disruption, grief-related distress, mood disturbance, and risk behaviors that differentiates ADHD + ACE from ADHD-only when co-occurring needs and demographics are held constant.
Collectively, the demographic patterns in our results underscore that trauma and ADHD coexist within developmental and sociocultural contexts that shape how difficulties emerge, are interpreted, and are ultimately labeled within systems of care. Our findings indicate that ADHD + ACE status is patterned by broader developmental and sociocultural factors, including age, gender/sex, and race. Older children were more likely to be in the ADHD + ACE group, consistent with developmental research indicating that both cumulative adversity and recognition of complex trauma presentations increase with age among youth with ADHD (Boodoo et al., 2022). Gender/sex patterns reflected known disparities in ADHD diagnosis, with males more frequently identified overall (Martin, 2024), while cisgender females and transgender youth were somewhat more represented in the ADHD + ACE group. Racial differences paralleled literature on inequities in access to services, provider bias, and structural determinants shaping both trauma exposure and diagnostic processes (Mikhail et al., 2018).
In the context of these demographic differences, we found that the most robust predictors of ADHD + ACE status—traumatic grief/separation (OR = 3.29), attachment difficulties (OR = 2.03), and sexually reactive behavior (OR = 2.62)—point to disruptions in relational security, affect regulation, and interpersonal boundaries that are characteristic of complex trauma (Luyten et al., 2020). These domains capture difficulties in navigating loss, distress, and threat cues, which may produce behavioral expressions that resemble or amplify ADHD-related challenges (D'Andrea et al., 2012; Herman, 2017). Elevated depression, oppositional behavior, self-mutilation, danger to others, and impaired judgment further indicate a broader pattern of emotional dysregulation and risk-taking that often emerges in the context of chronic adversity and disrupted caregiving (Briscoe-Smith & Hinshaw, 2006; Gonzalez et al., 2019). Importantly, these associations persisted even when controlling for attention, impulsivity, and other core ADHD-related characteristics, suggesting that they represent distinct markers of co-occurring trauma rather than simply reflecting generalized severity among children with ADHD.
In contrast, attention/concentration difficulties and behavioral regressions were negatively associated with ADHD + ACE status in the multivariate model. Although both groups exhibited high levels of inattention descriptively, the adjusted findings suggest that when trauma-related needs are jointly considered, attentional difficulties may be relatively more characteristic of ADHD-only presentations. In other words, among children with ADHD, greater trauma-related dysregulation appears to be associated with a shift away from profiles dominated by inattention toward profiles marked by attachment and grief difficulties, mood symptoms, and risk behaviors. This pattern aligns with dimensional conceptualizations emphasizing attention as a core feature of ADHD across developmental stages and diagnostic subtypes (APA, 2013; CDC, 2015; Pena et al., 2020). Behavioral regressions may similarly reflect developmental or environmental processes that are less tightly linked to ACE exposure once broader trauma-related dysregulation is considered. These findings highlight the importance of examining how ADHD symptoms and trauma-related dysregulation diverge and interact, rather than evaluating individual behaviors in isolation.
Findings from this study have several implications for trauma-responsive, developmentally informed assessment in youth mental health systems. First, they underscore the importance of routinely and comprehensively assessing trauma among children with ADHD diagnoses, particularly when there are prominent attachment difficulties, traumatic grief/separation, mood disturbance, and risk behaviors, as these patterns may signal co-occurring ACE exposure rather than ADHD-only presentations. Second, interpreting ADHD-related behaviors within a developmental framework is critical, as older youth may show more differentiated symptom profiles in which trauma-related dysregulation becomes more apparent alongside—or in some cases instead of—core attentional difficulties. Third, dimensional assessments such as the CANS are well suited to this task because they capture a broad range of needs and strengths, support nuanced clinical formulation, and align with trauma-informed and strengths-based models of care. Finally, these findings caution against assuming that all behavioral dysregulation in children with ADHD reflects the neurodevelopmental condition itself. When trauma-related dysregulation is present, trauma-focused interventions—not solely stimulant medication and behavioral modification—are needed to address the underlying drivers of functioning and to more accurately tailor care.
These results should be interpreted in light of several limitations. The sample was drawn from a single public mental health system, which may limit generalizability to other service settings or populations. ACE classification relied on CANS ratings and may not capture all forms of adversity. The study's cross-sectional design precludes conclusions about causality or developmental timing, and unmeasured factors may also shape ADHD + ACE profiles. Future research should incorporate longitudinal trajectories and other domains that buffer against trauma. Finally, we did not apply dimensionality reduction techniques (e.g., factor analysis) to the trauma-related domains. Although such approaches may yield higher-order constructs, they can also obscure clinically meaningful distinctions between specific needs. Future work could examine both individual domains and empirically derived composites to balance clinical interpretability with parsimony.
Taken together, the present study identifies a specific constellation of trauma-related needs—centered on attachment disruption, traumatic grief, mood disturbance, and risk behaviors—that uniquely differentiates children with ADHD who have ACE exposure from those without ACEs. These findings challenge approaches that treat ADHD-related behaviors as homogeneous and underscore the necessity of trauma-responsive, developmentally informed, and culturally attuned assessment practices in youth mental health systems. Recognizing the trauma-related dysregulation phenotype within ADHD can guide more precise diagnosis and intervention, reduce misidentification, and support the tailoring of care for children whose attentional or behavioral difficulties emerge within the context of adversity.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to colleagues at the Center for Innovation in Population Health at the University of Kentucky, particularly our biostatistician colleague Dr. Xiaoran Tong for his assistance with data preparation and Dr. John Lyons for providing access to the data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.