
Abstract
In vitro fertilization (IVF) treatment often involves significant psychological distress, yet many current support models are limited in taking a preventative lens and one which considers neurodiversity. This paper discusses the literature regarding fertility and IVF treatment for Autistic and Attention-Deficit-Hyperactivity Disorder (ADHD) individuals and highlights Bancroft's Hope Affirm Thrive framework, a universal psychological support model integrating trauma-informed care and systematic neurodiversity screening and support for IVF populations. Hope Affirm Thrive employs a three-tiered model delivering psychoeducation, emotional regulation skills from Dialectical Behavior Therapy, trauma processing through Eye Movement Desensitisation and Reprocessing, and Schema Therapy interventions. Universal screening for Autism and ADHD traits enables proactive accommodation without requiring diagnosis. The framework was specifically adapted for Australian healthcare contexts and IVF treatment timelines and addresses identified gaps by providing preventive rather than reactive support. This framework provides a replicable template for neurodiversity-affirming, trauma-informed psychological support adaptable to other high-stress medical contexts beyond IVF.
Lay Abstract
Infertility treatment through in vitro fertilization (IVF) is not only physically demanding but may also be emotionally overwhelming. Research shows that up to three-quarters of women and more than half of men experience significant anxiety or depression during treatment, with nearly half of patients discontinuing IVF because they feel overwhelmed by the process. Despite this, psychological support is often reactive, limited, or not well integrated into fertility care. The Hope Affirm Thrive program was developed to address these gaps through a proactive, trauma-informed, and neurodiversity-affirming model of care. This program combines well-established therapeutic approaches including Eye Movement Desensitisation and Reprocessing (EMDR) Therapy, Schema Therapy, and Dialectical Behavior Therapy (DBT) skills while also screening for Autistic and Attention-Deficit/Hyperactivity Disorder (ADHD) traits. Many individuals, particularly women, remain undiagnosed until adulthood, and IVF stress often reveals previously unrecognised traits. By offering universal supports such as written information, visual schedules, and sensory accommodations, among other accommodations, to all participants, the program removes the need for diagnostic labels before accessing help.
Keywords
Positionality Statement
The framework was developed by Elizabeth Bancroft, a Clinical and Counselling Psychologist and EMDRAA Accredited Practitioner with lived experience of Autism and ADHD and a 13-year fertility journey. This dual positioning provided both clinical credibility and authentic understanding of patient experience. The second author, Liam Spicer is an Autistic and ADHD academic, psychologist, EMDR trainer and accredited schema therapist who has their own history of grief and loss related to recurrent miscarriages experienced by their neurodivergent wife, and subsequent IVF treatment. They therefore bring their own lived experience and professional insight to the paper.
Introduction
In vitro fertilisation (IVF) represents a monumental step in reproductive medicine, offering individuals and couples the possibility of biological parenthood where natural conception has not occurred, whether due to medical infertility, same-sex partnerships, or other circumstances requiring assisted reproductive technology. With approximately 1 in 6 people globally experiencing infertility and over 2.5 million IVF cycles performed annually worldwide, resulting in approximately 1 in 16 (since 1/0.063 = 15.873) Australian babies being conceived through IVF, this technology has become increasingly vital to modern family formation (Kotevski et al., 2025; Zegers-Hochschild et al., 2017). However, the emotional and psychological toll is significant and frequently underestimated. IVF involves a complex multi-stage process that typically spans several months (Kotevski et al., 2025; Zegers-Hochschild et al., 2017). The process begins with ovarian stimulation using hormone medications to encourage multiple egg development, followed by regular monitoring through blood tests and ultrasounds. The egg retrieval procedure involves surgically collecting mature eggs from the ovaries under general anesthesia. These eggs are then fertilised with sperm in a laboratory setting, and resulting embryos are cultured for 3–6 days. The embryo transfer involves placing at least one embryo into the uterus, followed by a waiting period to determine if implantation has occurred (Kotevski et al., 2025; Zegers-Hochschild et al., 2017). This cycle may be repeated multiple times, with each stage often presenting unique physical, emotional, financial, and psychological challenges.
Research has consistently demonstrated that individuals undergoing IVF face elevated rates of psychological distress, including anxiety, depression, adjustment disorders, and trauma-related symptoms, with studies showing that 76% of women and 61% of men experience significant anxiety symptoms, while 56% of women and 32% of men report significant depressive symptoms during fertility treatment (Rooney & Domar, 2018). Women describe the experience as “all-consuming,” likening it to a full-time job with no guarantee of success (Domar et al., 2012). This mental health burden has critical implications, not only for patient wellbeing, but for treatment outcomes, as psychological stress is associated with poorer adherence, reduced number of cycles completed, and higher dropout rates. This paper provides an overview and synthesis of the existing literature in this space and outlines a program which is trauma informed and neurodiversity affirming that has been developed to meet the needs of individuals undergoing IVF treatment.
Psychological Distress in IVF: Scope and Impact
The significance of psychological distress in fertility treatment cannot be overstated. Approximately 70.4% of people encounter trauma at some point in their lives (Benjet et al., 2016; Kessler et al., 2017), meaning many entering fertility treatments carry pre-existing trauma histories that may be activated by the IVF process. Such trauma exposure significantly impacts how individuals respond to medical procedures, interact with healthcare providers, and cope with treatment uncertainties (Nicolaidis et al., 2015; Schmoyer-Edmiston, 2023). Medical environments can trigger trauma responses through factors like invasive procedures, loss of control, and positioning (National Institute of Mental Health, 2025; Substance Abuse and Mental Health Services Administration, 2014a, 2014b). This necessitates a shift from traditional biomedical approaches to holistic, trauma-informed models of care.
Current fertility clinic care remains heavily biomedical, with limited integrated psychological support. Where offered, services are often siloed, optional, or require additional cost. Research shows 25–60% of infertile individuals report psychiatric symptoms, with anxiety and depression significantly higher than fertile controls (Pasch et al., 2012). Over 80% of IVF patients show high clinical risk for depression (Aimagambetova et al., 2020). Of significant importance to highlight, 40.2% of women discontinue IVF with 47.5% of that stressed subgroup feeling “too stressed to continue,” with psychological burden being the primary reason for treatment discontinuation (Domar et al., 2018; Verberg et al., 2008). The medicalisation of conception transforms an intimate process into clinical procedures, creating additional psychological burden through repeated invasive procedures, pregnancy loss, unexpected poor results, feeling dismissed by staff, and experiencing feelings of bodily betrayal when treatments fail (Greil et al., 2010).
Trauma Histories and Fertility Treatment
For many patients, IVF is not their first exposure to reproductive trauma. Prior losses, delayed diagnoses, medical dismissals, and societal stigma often precede treatment, compounding the psychological load and creating heightened risk for treatment-related trauma (Hillcoat et al., 2023; Swift et al., 2024). Research has highlighted significant associations between trauma and reproductive health outcomes. Childhood sexual and emotional abuse and neglect are strongly associated with later infertility and pregnancy loss (Swift et al., 2024). Furthermore, intimate partner violence shows a 35% increased risk of miscarriage (Morland et al., 2008a, 2008b, Spencer et al., 2023). Recent research by Rostvall et al. (2025) demonstrated strong associations between adverse childhood experiences and reproductive conditions like endometriosis.
The mechanisms are complex and multifactorial. Trauma may impact reproductive health through chronic stress and hypothalamic-pituitary-adrenal axis dysregulation affecting hormone production (Chrousos et al., 1998; Morris et al., 2012); inflammatory responses interfering with implantation (Hillcoat et al., 2023; Mor et al., 2011); behavioral factors like delayed healthcare seeking (Swift et al., 2024); and epigenetic changes influencing reproductive function (Binder et al., 2008; Serpeloni et al., 2017). Trauma history represents one of many contributing factors to infertility alongside genetic, medical, environmental, and lifestyle factors. Individuals should not feel responsible for fertility challenges, as these relationships involve multiple interacting variables (Pearlin et al., 1981). Further proposed mechanisms and associated factors for trauma-reproductive health associations include immune system dysregulation affecting endometriosis tissue elimination; pain sensitisation through central nervous system changes; persistent stress response activation; and psychiatric comorbidities altering pain perception (Rostvall et al., 2025). These findings emphasise the need for trauma-informed fertility care approaches. The intersection of reproductive trauma and medical treatment creates complex clinical presentations. Patients may experience dissociation during invasive procedures (Brand et al., 2012; Lanius et al., 2010), hypervigilance regarding medical communications (Kimble et al., 2014; Kimble et al., 2023), or avoidance behaviors interfering with treatment adherence (Boykin, 2022; Waichler, 2022). Traditional medical approaches prioritising efficiency and standardised protocols may inadvertently perpetuate trauma responses, highlighting the need for specialised, trauma-informed fertility care (Center for Health Care Strategies, 2022; Ravi & Little, 2017).
The Intersection of Trauma, Autism, and ADHD
Recent research reveals a complex intersection between trauma exposure and neurodevelopmental differences such as Autism and Attention-Deficit/Hyperactivity Disorder (ADHD) (Biederman et al., 2013), with individuals with ADHD showing 2.9 times higher relative risk for developing PTSD (Spencer et al., 2016), with rates reaching 10% compared to 1.6% in the general population (Antshel et al., 2013). Autistic individuals experience more severe PTSD symptoms compared to non-Autistic peers, with at least comparable rates of occurrence (Quinton et al., 2024). Furthermore, due to common adversities faced by Autistic and ADHD people including bullying, sensory stressors, being talked down to, continual changes in daily life, social exclusion, and other adversity across the lifetime, tailored trauma-informed and neurodiversity-affirming therapeutic support is required (Spicer et al., 2024). The co-occurrence of Autism and ADHD creates additional complexity, with estimates from some studies suggesting between 40% and 70% of Autistic individuals also identified as having ADHD (Antshel et al., 2016). People with ADHD demonstrate elevated risk for trauma exposure due to impulsivity, risk-taking behaviors, and reduced HRV variability with sympathetic nervous system dominance, making stress regulation more difficult (Dekkers et al., 2016; Rukmani et al., 2016). Some research demonstrates certain shared similarities in stress system functioning between ADHD, Autism, and PTSD, including in the hypothalamic-pituitary-adrenal axis (Kushki et al., 2013; Song et al., 2024), emphasising the importance of accurate diagnosis, appropriate support, and affirming treatment models. The intersection of these differences with other identities such as race, gender, sexuality, and socioeconomic status among other differences may also create compounded vulnerabilities. Therefore there is a need for intersectional approaches that acknowledge power structures associated with discrimination and trauma to achieve better outcomes for multiple marginalised individuals (Cobbaert et al., 2024; Mallipeddi & VanDaalen, 2022). This emerging discussion in the literature underscores the critical need for trauma-informed, neurodiversity-affirming approaches in clinical practice that recognise the heightened vulnerability and complex presentations at these intersections.
Fertility and Autism/ADHD
The intersection of trauma, Autism, and ADHD becomes particularly relevant in fertility care, where women are significantly underdiagnosed. The Autism diagnosis for women without intellectual disability occurs later than men, often not until adulthood (Bargiela et al., 2016; Gesi et al., 2021), with ADHD also frequently going unrecognised until adulthood (Young et al., 2020), coinciding precisely with fertility treatment seeking. Research has identified distinct social factors that impact on Autistic females with common presentations involving sophisticated masking and camouflaging strategies (Hull et al., 2017), which comes at significant psychological cost and often breaks down under extreme stress (Bernardin et al., 2021; Lai et al., 2017). This may be one of the factors as to why many women first seek diagnosis during challenging life events like fertility treatment.
Autistic women experience significantly higher rates of co-occurring reproductive disorders including polycystic ovarian syndrome (PCOS), endometriosis, and menstrual irregularities (Ingudomnukul et al., 2007; Simantov et al., 2022), meaning they may be overrepresented in fertility populations. However, Autistic and ADHD individuals face additional challenges in fertility settings that standard protocols fail to address, including sensory overwhelm from medical environments, difficulties with complex multi-step treatment protocols and time management demands, communication barriers with providers, and social demands of group sessions (Chapman & Botha, 2023; Dundon, 2024; Nicolaidis et al., 2015; Ptacek et al., 2019). The complex medical and emotional demands of fertility treatment may reveal previously unrecognised Autistic and/or ADHD traits as individuals navigate these challenges. Multiple factors contribute to higher concentrations of Autistic and/or ADHD individuals in healthcare settings: 74% of individuals who are Autistic have at least one medical comorbidity (Khachadourian et al., 2023) (Lai et al., 2019), approximately 40% also present with ADHD (Rong et al., 2021), up to 80% carry psychiatric diagnoses (Lugo-Marín et al., 2019), and Autistic and/or ADHD individuals demonstrate markedly higher healthcare utilisation rates (Zerbo et al., 2015). Additionally, “neurokin” connections whereby neurodivergent individuals such as those who are Autistic and/or ADHD seek practitioners with similar differences may lead to higher rates of neurodivergent clients in affirming practices (League of Autistic Psychologists and Affirming Colleagues, n.d.; Paynter, 2025).
This paper provides a comprehensive description of the Hope Affirm Thrive framework, including its theoretical foundations, development process, core components, and implementation considerations. The framework was developed through clinical work with IVF patients and is informed by lived experience of the primary author. While full outcome evaluation is planned for future research, this paper focuses on framework description to enable replication, adaptation, and further investigation.
Framework Development and Components
Framework Development Process
The Hope Affirm Thrive framework was developed through systematic integration of clinical practice insights, evidence-based therapeutic approaches, and lived experience perspectives between January and August 2024 in Perth (Boorloo), Western Australia. Development was guided by three complementary theoretical frameworks: the Knowledge-to-Action framework (Graham et al., 2006), which structured progression from evidence synthesis to implementation planning; the Ecological Validity Model (Bernal & Sáez-Santiago, 2024; Bernal et al., 1995), which ensured cultural and contextual adaptation across eight dimensions including language, content, methods, and healthcare context; and the Medical Research Council framework for complex interventions (Skivington et al., 2021), which guided phased development from evidence identification through feasibility testing to planned evaluation which will be the subject of future work in this field.
The framework was developed by Elizabeth Bancroft, a Clinical and Counselling Psychologist and EMDRAA Accredited Practitioner with lived experience of Autism and ADHD, and a 13-year fertility journey. This dual positioning provided both clinical credibility and authentic understanding of patient experience. Development occurred within the Australian private practice context, characterised by significant psychology workforce shortages, partial Medicare rebates creating affordability barriers, and IVF costs of $10,000–$15,000 per cycle necessitating group-based intervention design for accessibility. The second author, Liam Spicer is an Autistic and ADHD academic, Psychologist, Eye Movement Desensitization and Reprocessing (EMDR) trainer and accredited Schema therapist that has their own history of grief and loss related to recurrent miscarriages experienced by their neurodivergent wife, and subsequent IVF treatment. They therefore bring their own lived experience and professional insight to the paper.
Prior to framework development, clinical observations from 1:1 therapy practice revealed consistent patterns among IVF patients presenting for psychological support. Women aged 32–45 years at various stages of IVF treatment commonly reported inadequate clinical support and communication, significant information gaps, emotional isolation, advocacy challenges, need for trauma-informed care, and critically, the absence of preventive support. Patients frequently expressed desires for support before something had gone wrong rather than waiting until everything escalated, highlighting a clear need for preventive rather than reactive psychological intervention.
Clinical consultations consistently revealed patients experiencing sensory overwhelm during medical procedures (bright lights, multiple people present, invasive examinations), difficulty processing complex medical information delivered verbally in time-pressured consultations, and significant distress with unpredictable scheduling and routine disruptions inherent to IVF protocols. These presentations, consistent with Autism sensory and ADHD executive function profiles, informed the decision to incorporate systematic autism and ADHD screening.
This decision was further supported by population prevalence estimates suggesting substantial unrecognised Autism and ADHD in adults, particularly women who are historically underdiagnosed (Botha et al., 2023; Sedgewick et al., 2022), research documenting differential impacts of chronic stress and medical trauma on autistic and ADHD individuals (Kinnaird et al., 2019; Lever & Geurts, 2016), and clinical gap identification revealing that standard reproductive healthcare lacks protocols for identifying and accommodating neurodivergent patients despite potential benefits of tailored support that are in line with the fundamental principles of the neurodiversity affirming movement (Chapman & Botha, 2023; de Visser et al., 2025).
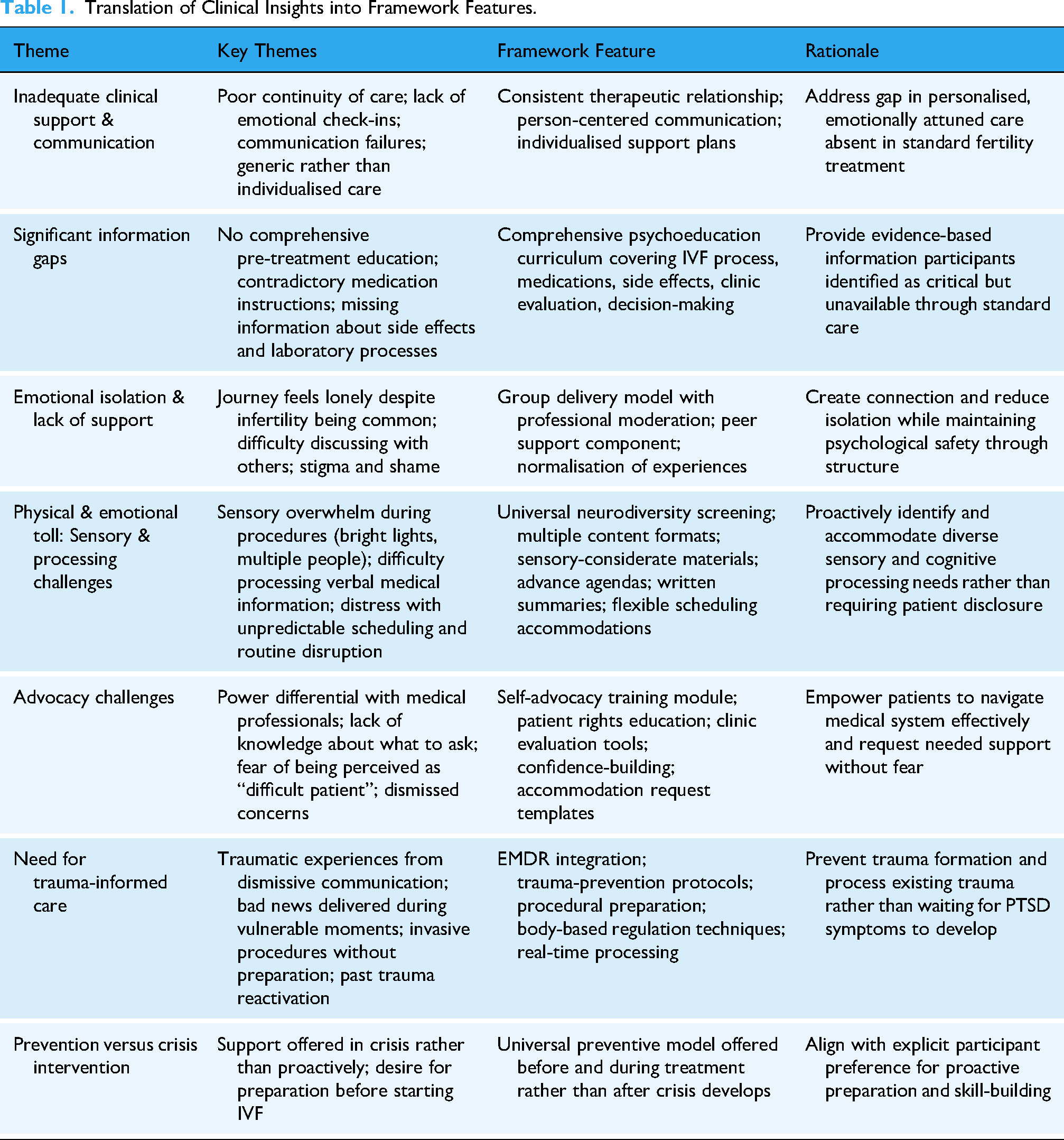
Table 1 presents the translation of clinical insights into specific framework features, demonstrating how each identified gap or need observed in practice was addressed through concrete program components. This practice-to-framework translation process ensured the intervention directly responded to patient-identified priorities rather than clinician assumptions about needs.
Translation of Clinical Insights into Framework Features.
Content Development
Content development drew on clinical training (EMDR Association of Australia Accredited Practitioner, Schema Therapy, Dialectical Behavior Therapy (DBT)), lived experience of Autism, ADHD and fertility treatment, clinical experience, literature review, and completion of Fertility Society of Australia and New Zealand START training in March 2024 ensuring medical accuracy. Existing evidence-based protocols for EMDR (Shapiro, 2018), DBT (Linehan, 2014), and Schema Therapy (Young et al., 2003), were adapted for fertility contexts. The comprehensive program includes four core psychoeducation modules covering IVF processes, emotional regulation and stress management, self-advocacy and medical system navigation, and grief and resilience, with bonus lessons on trauma, miscarriage, and deciding when to stop treatment. Materials include participant workbook, DBT skills training handouts adapted for IVF scenarios (distress tolerance for two-week wait, emotion regulation during hormonal fluctuations, interpersonal effectiveness with medical providers), EMDR protocols for procedural anxiety and grief processing, Schema Therapy assessment and mode work tools, self-advocacy toolkit with clinic evaluation checklists and accommodation request templates, and comprehensive screening protocol materials. All materials incorporate universal design principles including multiple formats, chunked information, visual supports, plain language, consistent structure, and mobile-friendly formatting.
Screening Protocol
The screening battery includes Comprehensive Autistic Trait Inventory (Hull et al., 2019), Ritvo Autism Asperger Diagnostic Scale Revised (Ritvo et al., 2011), Adult ADHD Self-Report Scale (Kessler et al., 2005), Executive Skills Questionnaire Revised (Barkley & Murphy, 2006), and broader psychological assessment measures such as the Depression, Anxiety, Stress Scale -21 items, Lovibond & Lovibond, 1995), Impact of Events Scale Revised (Weiss & Marmar, 1997), Young Schema Questionnaire -Revised (Young et al., 2003), Adverse Childhood Experiences Questionnaire (Felitti et al., 1998), Rosenberg Self-Esteem Scale (Rosenberg, 1965), Self-Compassion Scale (Raes et al., 2011), Brief-COPE (Carver, 1997), PTSD Checklist for DSM-5 (Weathers et al., 2013). All measures are completed online through Novopsych, an Australian secure assessment platform providing automated scoring, normative comparisons, and clinical threshold identification. Completion requires 60–90 min.
Screening results are communicated using neurodiversity-affirming frameworks emphasising traits as variations in cognition and functioning rather than pathology, practical implications for IVF experience, and no diagnosis requirement for accommodations. Screening data informs program delivery adaptations (format preferences, pacing, communication style), individualised accommodation planning (sensory supports, executive function aids, information processing modifications), psychoeducation content tailoring, referral decisions, and program evaluation examining differential response patterns.
Evaluation Mechanisms
Current feedback collection relies on post-session verbal check-ins, ongoing feedback channels via email or text, and real-time accommodation adjustments. Verbal approaches were prioritised recognising that Autistic and ADHD individuals often find written questionnaires create additional executive function demands, however the option for different forms of feedback are provided. More formal evaluation mechanisms including mid-program check-ins, post-program interviews, brief session surveys, and longitudinal follow-up are planned for implementation once sufficient participants complete the full program and move beyond active IVF treatment. This systematic development process, guided by established frameworks (Bernal & Sáez-Santiago, 2004; Bernal et al., 1995; Graham et al., 2006; Skivington et al., 2021), informed by patient voice, refined through iterative testing, and grounded in evidence-based practice and lived experience, demonstrates rigorous research-to-practice translation positioning the framework for both immediate implementation and ongoing evaluation.
Theoretical Foundations
The Hope Affirm Thrive framework integrates multiple evidence-based therapeutic modalities specifically adapted for fertility treatment contexts. Each modality addresses distinct aspects of the IVF psychological experience while functioning synergistically within the comprehensive program.
Neurodiversity-Affirming Approach
The framework operationalises neurodiversity-affirming principles (Leadbitter et al., 2021; Shaw et al., 2025) by framing individual differences as natural human variation rather than pathology. Universal screening enables identification of Autistic and ADHD traits without requiring diagnosis or diagnostic disclosure, reducing barriers associated with stigma, diagnostic access inequities, and difficulty articulating needs. Program materials offer identity-first language options (Autistic person versus person with Autism) respecting diverse preferences. Accommodations including advance session agendas, written summaries of verbal content, multiple content formats (video, written, visual), sensory considerations (lighting preferences, movement breaks), and executive function supports (reminders, task breakdowns, visual schedules) are built into standard delivery rather than requiring individual requests. Clinician training emphasises direct literal communication, validation of diverse emotional expression styles, and recognition that traits such as detail-orientation and sustained focus can be assets during structured IVF protocols. This approach contrasts with standard fertility care where accommodations are rarely offered unless patients self-identify and advocate, creating barriers for those unaware of their Autism and/or ADHD or uncomfortable with disclosure. Table 2 operationalises neurodiversity-affirming principles by contrasting standard fertility care practices with Hope Affirm Thrive's approach, providing concrete examples of how abstract principles translate into specific practices. These operationalised principles guide all aspects of program delivery and clinician training.
Operationalization of Neurodiversity-Affirming Principles in Relation to Standard Fertility Care and the Hope Affirm Thrive Program.

Trauma-Informed Care
Fertility treatment involves inherently vulnerable experiences including invasive medical procedures, repeated grief and loss, lack of control over outcomes, and potential for medical trauma from dismissive communication or unexpected bad news (Braverman et al., 2024; Greil et al., 2010). The framework applies trauma-informed principles (Substance Abuse and Mental Health Services Administration, 2014a, 2014b), by emphasizing safety (predictability through advance agendas, choice in participation format), trustworthiness and transparency (clear explanations of processes, collaborative decision-making), peer support (group format normalising experiences), collaboration and mutuality (power-sharing in treatment planning), empowerment and voice (self-advocacy skill-building), and cultural humility (neurodiversity-affirming, responsive to diverse backgrounds). Rather than waiting for trauma symptoms to develop, the framework takes a preventive approach through pre-treatment preparation for potentially distressing procedures, real-time processing of difficult experiences using EMDR techniques, and proactive skill-building for emotional regulation during high-stress periods.
Eye Movement Desensitization and Reprocessing
EMDR, an evidence-based therapy for trauma (Shapiro, 2018), is adapted for multiple IVF applications beyond post-traumatic stress disorder treatment. Protocols target procedural anxiety (desensitisation of fears related to egg retrieval, embryo transfer, injections), grief and loss processing (failed cycles, pregnancy losses, cumulative losses), negative cognitions about fertility (beliefs such as “my body is broken” or “I’m failing as a woman”), and resource development (building internal safe place, nurturing figures, and protector figures accessible during stressful medical procedures). The Recent Events Protocol (Jarero & Artigas, 2017) processes distressing clinic interactions in real-time, preventing trauma consolidation. Flash Technique manages overwhelming emotions during ongoing treatment without requiring detailed trauma narrative, making it suitable for preventive intervention (Manfield et al., 2021). Emerging research demonstrates EMDR's promise in fertility and grief contexts (Bal & Ucar, 2024; Spicer, 2024).
Schema Therapy
Schema Therapy (Young et al., 2003) addresses core beliefs and emotional patterns activated by infertility. The Young Schema Questionnaire-Revised identifies schemas commonly triggered by fertility struggles including Defectiveness and Shame (body perceived as broken), Failure (inability to achieve pregnancy interpreted as personal failure), and Unrelenting Standards (harsh self-criticism about not meeting expectations). Mode work helps participants recognise when operating from Vulnerable Child mode (helpless, hopeless), Angry Child mode (rageful at body, medical system, or partner), Demanding Parent mode (punitive self-criticism), or Healthy Adult mode (balanced, compassionate, problem-solving). Limited reparenting and imagery rescripting techniques provide corrective emotional experiences, while mode dialogues may facilitate greater compassion, insight, and behavioral change.
Dialectical Behavior Therapy
DBT skills training (Linehan, 2014) provides practical strategies for managing IVF's emotional intensity. Distress tolerance skills including TIPP (Temperature, Intense exercise, Paced breathing, Paired muscle relaxation) reduce acute anxiety before procedures, while ACCEPTS (Activities, Contributing, Comparisons, Emotions, Pushing away, Thoughts, Sensations) helps tolerate the two-week wait after embryo transfer. Emotion regulation skills address hormonal mood fluctuations, differentiation of emotions from hormone effects, and reducing shame through Check the Facts and non-judgmental stance. Interpersonal effectiveness skills (DEAR MAN, GIVE, FAST) support advocacy with medical providers and maintaining relationships during stress. Mindfulness practices cultivate present-moment awareness and acceptance of uncertainty. All skills are specifically contextualised for fertility scenarios with examples and practice opportunities relevant to IVF experiences.
Universal Design Principles
The framework incorporates universal design (Centre for Excellence in Universal Design, 2020) ensuring accessibility for diverse cognitive and sensory profiles. Multiple means of representation provide information through video, audio, written, and visual formats. Predictability and structure reduce anxiety through consistent session formats and advance agendas. Flexible engagement options include camera-off participation, chat versus verbal contribution, and asynchronous content review. Clear expectations with explicit norms and step-by-step instructions reduce ambiguity. Information chunking prevents overwhelm through brief segments and frequent breaks. Sensory considerations include lighting control, volume adjustment, and fidget-friendly environments. Communication redundancy reinforces key information through multiple channels and written summaries. These features benefit all participants while being particularly essential for neurodivergent individuals. Table 3 details the universal design features integrated throughout the program, demonstrating how each feature benefits all participants while being essential for neurodivergent individuals. This dual benefit structure exemplifies the universal design philosophy that accessibility improvements enhance experiences for everyone, not only those with identified disabilities or differences.
Universal Design Features and Their Benefits for Participants.

Integration of Modalities
The framework's strength lies in integrating these approaches rather than applying them separately. EMDR processes trauma while DBT skills provide in-the-moment regulation. Schema work addresses underlying beliefs while EMDR reprocesses the emotional charge attached to those beliefs. Neurodiversity-affirming accommodations ensure all interventions are accessible. Trauma-informed principles create safety enabling engagement with challenging material. This integration creates comprehensive support addressing multiple dimensions of IVF psychological experience simultaneously.
Program Structure and Tiered Model
The Hope Affirm Thrive framework employs a three-tiered structure enabling participants to match intervention intensity to their needs, resources, and readiness.
Tier 1: Hope Starter (Psychoeducation Foundation)
This foundational tier provides comprehensive IVF education and preparation delivered through four core modules covering IVF medical processes and terminology, emotional regulation and stress management basics, self-advocacy and medical system navigation, and grief and resilience frameworks. Bonus modules address trauma in fertility journeys, miscarriage navigation, and deciding when to stop treatment. Content is delivered through self-paced online modules with live group sessions for question-and-answer opportunities and peer connection. Duration is approximately four weeks with 4–6 h total engagement. This tier is appropriate for all IVF patients seeking preparation and information, those early in treatment wanting preventive support, and individuals preferring educational rather than therapeutic intervention.
Tier 2: Affirmed Support (Skills Training)
Building on Tier 1, this tier adds intensive DBT skills training and EMDR through eight weekly live group sessions teaching distress tolerance for procedure anxiety and waiting periods, emotion regulation for hormonal fluctuations and grief, interpersonal effectiveness for medical advocacy and partner communication, and mindfulness for uncertainty tolerance. Skills practice homework and accountability through cohort engagement are included. Duration is eight weeks with approximately 16 total hours. This tier suits individuals experiencing significant distress requiring active skill-building, those struggling with emotional regulation during treatment, people wanting structured group support and peer connection, and patients identified through screening as potentially benefiting from enhanced support.
Tier 3: Thrive Experience (Comprehensive Therapeutic Support)
The most intensive tier includes all Tier 1 and 2 components plus group EMDR intensive sessions for trauma processing (past trauma, medical trauma, grief and loss, negative cognitions), Schema Therapy work addressing core beliefs and emotional patterns, and Resource Therapy techniques for accessing internal strengths. An in-person full-day EMDR workshop option is available for Perth participants. Duration is eight to ten weeks with approximately 22 total hours. This tier is appropriate for individuals with trauma histories requiring processing, those with complex grief or significant psychological distress, people wanting individualised therapeutic support beyond group programming, and patients for whom Tier 2 skills training is insufficient.
Universal Components Across All Tiers
All participants regardless of tier receive comprehensive screening at intake (Autism, ADHD, mental health, trauma history, coping patterns), individualised accommodation planning based on screening results, access to self-advocacy toolkit and resource library, crisis support and referral pathways as needed, and ongoing needs assessment with flexible tier movement (participants can step up or down based on evolving needs).
Delivery Format
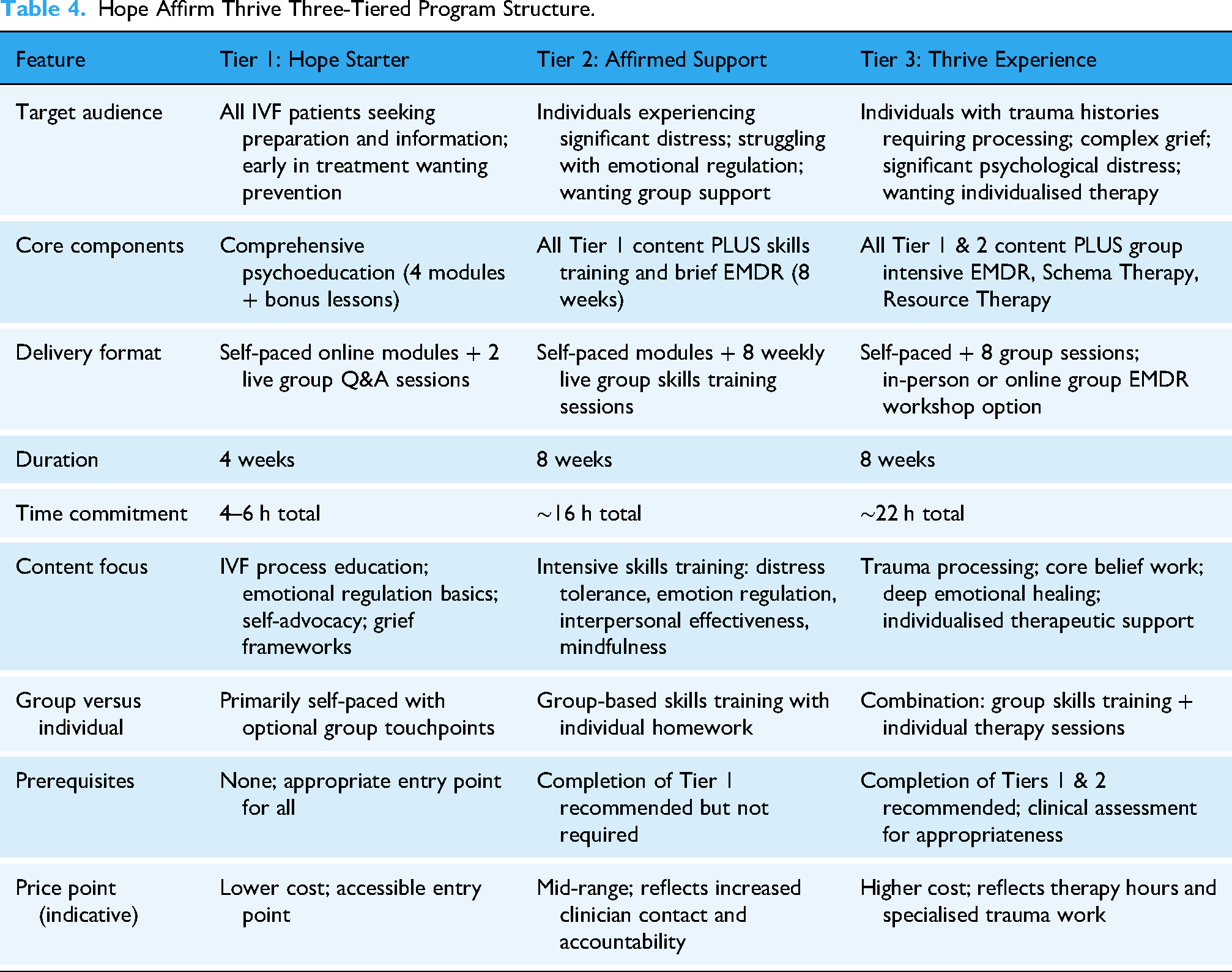
Research supports the effectiveness of group psychological interventions for women undergoing fertility treatment, with meta-analytic evidence demonstrating significant reductions in depression, anxiety and fertility stress, alongside improved pregnancy rates (Warne et al., 2022). The framework was therefore designed for group delivery (eight to ten participants per cohort) to provide peer support, normalise experiences, increase cost-effectiveness, and address Australian psychology workforce shortages. However, initial implementation adapted to individual format due to enrolment constraints. Both group and individual formats maintain therapeutic integrity with appropriate modifications. In-person delivery options are available in Perth for participants preferring face-to-face engagement, particularly for EMDR intensive workshops, while telehealth options serve regional and rural Australia. Table 4 summarises the three-tiered program structure, presenting an at-a-glance comparison of target audiences, core components, delivery formats, and time commitments across tiers. This structured presentation facilitates program understanding and supports replication by other practitioners or clinics.
Hope Affirm Thrive Three-Tiered Program Structure.
Comprehensive screening at intake (Autism, ADHD, mental health, trauma, coping) Individualised accommodation planning based on screening Access to self-advocacy toolkit and resource library Crisis support and referral pathways as needed Flexible tier movement (step up or down based on needs)
Implementation Considerations
Barriers to Uptake and Lessons Learned
Initial implementation revealed significant systemic barriers to program uptake with important implications for future dissemination. Despite multi-channel marketing efforts, all referrals originated from existing practice networks with zero engagement from fertility clinics or women's health providers. This pattern suggests fundamental challenges in operating psychological support as an external referral service rather than embedding within fertility clinic workflows. Multiple factors likely contributed to limited uptake. Fertility clinics may prefer internal counselling services to maintain revenue, have established referral relationships with other providers, have concerns about coordination with external providers, lack systems for routine psychological referral, or have insufficient staff time to explain external programs during brief medical consultations. The separation between medical (fertility clinic) and psychological (private practice) services creates gaps, with patients primarily identifying with medical treatment and viewing psychological support as peripheral. Fertility specialists and women's health providers may lack awareness of the intersection of Autism and/or ADHD with fertility challenges, understanding of trauma-informed care principles, or familiarity with preventive psychological support models.
Patient-level barriers include substantial out-of-pocket costs despite Medicare rebates (typical gap of $100 per session) when already spending $10,000–$15,000 per cycle on medical treatment, time burden when IVF already requires frequent medical appointments, stigma around seeking psychological support, lack of awareness that psychological support during IVF exists or is beneficial, and timing challenges when marketing reaches patients at various treatment stages.
These barriers are not unique to this program but reflect systemic challenges in integrating psychological support into medical care. Successful implementation requires embedding psychological services within fertility clinics as routine standard of care rather than external referral, implementing universal screening of communication and sensory preferences during fertility clinic intake as normal protocol like bloodwork, providing subsidised or bulk-billed access through partnership funding or insurance integration, conducting provider education at fertility clinics about neurodiversity and trauma-informed care, and reframing psychological support as optimising treatment outcomes rather than optional add-on. Different implementation models may suit different contexts including large fertility clinics employing in-house psychologists implementing the framework, smaller clinics partnering with nearby psychology practices for contracted services, telehealth-only models with fertility clinic partnerships, and public hospital settings integrating into existing mental health pathways.
Clinical Implementation Requirements
Minimum clinician qualifications include registration as psychologist or equivalent mental health professional, training in trauma-focused modalities (EMDR or similar evidence-based trauma therapy), familiarity with DBT principles and skills training delivery, and understanding of Schema Therapy concepts (formal training recommended but not essential). Recommended qualifications include specialised training in fertility counselling or reproductive mental health and registration with the Australia and New Zealand Infertility Counsellor's Association (ANZICA), personal or professional familiarity with IVF processes, training in neurodiversity-affirming practice, and experience with group therapy facilitation.
Training requirements for framework implementation include thorough review of all program materials and theoretical foundations, familiarisation with local fertility clinic practices and referral pathways, training in neurodiversity screening interpretation and accommodation planning, supervision or consultation during initial implementation (recommended minimum six sessions with experienced fertility psychologist), and ongoing professional development in trauma-informed care and neurodiversity. Resource requirements include secure telehealth platform with recording capability for asynchronous module access, screen-sharing and breakout room functionality for group delivery, secure file storage for participant materials and screening data, reliable internet connection and backup technical support, and private space for individual sessions when needed. Time requirements per participant include intake and screening review (1.5 h), Tier 1 (approximately 4 h total), Tier 2 (approximately 16 h total), and Tier 3 (approximately 22 h total).
Discussion
Framework Contributions
The Hope Affirm Thrive framework advances fertility psychology through several key innovations. First, it provides universal rather than reactive support, offering proactive preparation to all patients before a crisis rather than waiting for problems to emerge. This aligns with patient-expressed preferences from formative research and shifts from crisis management to prevention. Second, systematic neurodiversity screening enables identification and accommodation of Autistic and ADHD traits without requiring diagnosis or disclosure, addressing a significant gap in standard fertility care. Third, trauma-informed principles and EMDR integration recognise fertility treatment as potentially traumatic and offer evidence-based processing. Fourth, tiered accessibility with multiple entry points allows participants to match intensity to needs and resources. Lastly, and important to note it is informed by both clinical and lived experience allowing appropriate adaptations and considerations that will be explored in the future more directly in clinical research. The framework demonstrates how trauma therapy can be extended beyond post-traumatic stress disorder to stress regulation and preventive contexts, how neurodiversity-affirming principles can be operationalised in medical settings, and how universal psychological support can be integrated into medical procedures. It provides a replicable model for comprehensive psychological care applicable beyond fertility treatment.
Adaptability to Other Medical Contexts
While developed specifically for IVF populations, the framework principles are adaptable to other high-stress medical contexts sharing similar characteristics including prolonged uncertainty and lack of control, repeated medical procedures with cumulative stress, potential for medical trauma from invasive procedures or poor communication, need for navigation of complex medical systems, benefit from advocacy skills and self-efficacy, cyclical stress and grief processing, potential for unidentified neurodivergent needs complicating medical adherence and distress, and gap between medical focus and psychological support. Applicable contexts include assisted reproductive technology more broadly (donor egg or sperm procedures, surrogacy, fertility preservation for cancer patients), perinatal care (high-risk pregnancy, neonatal intensive care experiences, pregnancy after loss), chronic illness management (diabetes, autoimmune conditions requiring ongoing medical management), gender-affirming care (hormone therapy, surgical procedures, navigation of medical systems), organ transplant (prolonged waiting, complex medical procedures, uncertainty), and cancer treatment (chemotherapy, radiation, survivorship).
Adaptation would require context-specific psychoeducation, identification of context-specific stress points and trauma risks, modification of self-advocacy toolkit for relevant medical specialists, and cultural and demographic considerations for target populations. Core principles of universal neurodiversity screening, trauma-informed preventive approach, evidence-based modalities, tiered intensity matching needs, patient-informed design, and integration into medical care rather than separate referral would remain consistent.
Limitations and Future Directions
Implementation limitations include single-site development in Perth private practice (generalisability concerns regarding Australian healthcare context, urban setting, private practice selection bias), referral pathway constraints (all participants from existing networks, lack of fertility clinic engagement suggests findings may not represent broader IVF population), and delivery format discrepancy (framework designed for group delivery but implemented individually, leaving group dynamics, peer support mechanisms, cost-effectiveness, and scalability untested). Critical future research directions encompass multiple interconnected domains. Rigorous outcome evaluation through randomised controlled trials is essential, comparing the framework to standard care and waitlist control with adequate sample sizes, multiple sites, active control conditions, and longitudinal follow-up. Screening validation requires larger samples to assess Autistic and ADHD trait prevalence in IVF populations, with control groups of non-IVF fertile individuals, diagnostic follow-up for those screening positive, and investigation of mechanisms linking Autism and/or ADHD and fertility if elevated prevalence is confirmed. Mechanism research should examine which program components are most beneficial, whether certain participants respond differently, what mediates outcomes, and how screening and accommodation impact engagement.
Implementation science must test embedded-in-clinic models versus external referral, develop and evaluate provider training programs, conduct cost-effectiveness analyses, and identify strategies for clinic buy-in and culture change. Adaptation studies should test the group format as originally designed, develop adaptations for diverse cultural groups, create modifications for other medical contexts, and explore lower-intensity digital interventions. Equity research is crucial to ensure accessibility for culturally and linguistically diverse populations through translations and cultural adaptations, address socioeconomic barriers through subsidised access, expand rural and regional access through telehealth models, and include same-sex couples, single parents by choice, and gender diverse individuals. Finally, neurodiversity-specific research should develop fertility-specific neurodivergent support protocols, investigate sensory accommodation impacts on procedure distress, and explore how Autistic and ADHD traits interact with fertility treatment experiences and outcomes.
Conclusion
The Hope Affirm Thrive framework represents systematic, theory-driven development addressing critical gaps in fertility psychological support. Future research should prioritise rigorous outcome evaluation with adequate sample sizes, control groups, and longitudinal follow-up to establish effectiveness. Implementation research is equally critical to identify strategies for overcoming systemic barriers and achieving sustainable integration into fertility care. With systematic evaluation and thoughtful implementation, the Hope Affirm Thrive framework has potential to transform psychological support for fertility patients, ensuring that emotional well-being is prioritised alongside medical treatment throughout the challenging IVF journey regardless of outcome.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Elizabeth Bancroft is the developer of the Hope Affirm Thrive Program and delivers this program commercially in her clinical practice which constitutes a potential conflict of interest. Liam Spicer has no financial or commercial interests in the Hope Affirm Thrive Program and reports no conflict of interest.
Lived Experience Disclosure
Both authors bring lived experience of IVF experiences and neurodivergence to this paper, aligning with the Australian National Autism Strategy Action Plan and principle of “nothing about us without us” (Department of Social Services, 2025).