
Abstract
Lay Abstract
Keywords
Many researchers and advocates have identified a population of autistic adults whose autism was missed in childhood, resulting in increased risk of negative psychosocial outcomes from lack of access to accommodations, and a positive sense of identity and community, among other factors (Lai & Baron-Cohen, 2015). Psychosocial factors related to delayed diagnosis include masking and camouflaging (Hull et al., 2017), which can lead to increased rates of mental health service need and use (Khudiakova et al., 2024). Additionally, experiences of burnout, rejection and isolation (Cook et al., 2021; Raymaker et al., 2020) may also contribute to increasingly high rates of mental health needs in autistic adults (Evans et al., 2024).
The research literature consistently shows that co-occurring psychiatric conditions occur among autistic adults at much greater rates than the general population (Fombonne et al., 2020; Hossain et al., 2020; Jadav & Bal, 2022). Studies suggest that between 28% and 66% of autistic adults also meet criteria for anxiety (Fombonne et al., 2020; Jadav & Bal, 2022; Lugo-Marín et al., 2019) and 28% to 58% of autistic adults also meet criteria for an affective/depressive/mood disorder (Hollocks et al., 2019).
Attending to the mental health of autistic adults is crucial, not only because all individuals deserve respect, dignity and supportive services but also because untreated mental health challenges can lead to increased hospitalizations, higher rates of unemployment and underemployment and elevated early mortality due to suicide and other causes (Oakley et al., 2021). Autistic adults experience disproportionate mental health challenges and an increased need for services compared to the general population. Although recent research indicates they may actually be overrepresented in adult mental health settings (Camm-Crosbie et al., 2019), the vast majority remain undiagnosed. Despite their presence in mental health services, autistic adults are not receiving adequate support (Roux et al., 2015). A lack of evidence regarding effective mental health interventions for autistic adults may play a role in this underutilization (Mazurek et al., 2023), along with other unique barriers to treatment (Brede et al., 2022). The mental health challenges facing autistic adults represent a significant global public health concern with substantial economic implications.
Beyond co-occurring psychiatric disorders, research on autistic adult mental health has predominantly focused on the presence of psychopathology (e.g., anxiety, depression) while giving considerably less attention to difficulties autistic adults face in achieving positive wellness outcomes such as life satisfaction, meaning, purpose and flourishing (Graham Holmes et al., 2020). Nearly 70% of autistic college students reported feeling left out “some of the time” or “often,” and 74% reported feeling isolated (Capriola-Hall et al., 2021). Qualitative studies of late diagnosed adults often find themes of lack of belonging (e.g., Grace et al., 2022). Overall quality of life for autistic adults is negatively impacted by stigma, depression, lack of social satisfaction, co-occurring physical health conditions, anxiety, general adversity, and other factors (Botha & Frost, 2020; Lawson et al., 2020; Park et al., 2019).
Despite some promising research, access to mental health treatment options for autistic adults’ remains limited (Capriola-Hall et al., 2021). Some studies suggest that over 50% of caregivers of autistic adults feel the autistic adult in their life has an untreated mental health need and 35% of autistic adults agreed with this (Schott et al., 2021). Cognitive Behavioural Therapy (CBT) adapted for autistic adults has demonstrated promising results in reducing mental health symptoms like anxiety. Several recommendations for adapting mental health therapies for autistic populations have been suggested (Table 1), but the systematic research with autistic adults is still sparse.
Selected Autism-Specific Therapy Adaptation Examples.

Note: 1. Structure & Session Format = Extended sessions, consistent structure, breaks, predictability; 2. Communication Modifications = Concrete language, visual aids, written materials, explicit explanations; 3. Sensory Accommodations = Sensory-friendly environment, reduced stimuli, sensory items; 4. Cognitive & Therapeutic Approach = Behavioural emphasis, emotion recognition, psychoeducation, individualized formulation; 5. Content Personalization = Special interests integration, individualized to person not diagnosis; 6. Support & Involvement = Caregiver/supporter involvement, collaboration with specialist services; 7. Therapist Factors = Autism training, understanding, neurodiversity-affirming approach, supervision; 8. Practical & Accessibility = Navigation support, materials, online options, addressing barriers.
Researchers have conducted limited research on group psychoeducation or psychotherapy, but it is another promising area. Studies suggest group interventions may improve quality of life, social relationships and mental health symptoms in autistic adults post-diagnosis (Cook et al., 2021). The sense of community and belonging that neurodivergent-specific settings can generate may be important components of group outcomes, as many autistic adults prefer neurodivergent-led services (Crompton et al., 2020; Hull et al., 2024).
Research on neurodiversity-affirming mental health interventions for autistic adults is in its infancy, yet emerging evidence suggests these services may represent one of the most impactful supports available to this population (Chan & Doran, 2024). For example, therapies that incorporate developing a positive autistic identity and autistic community significantly increase mental health outcomes and reduce social anxiety in autistics (Cooper et al., 2023). Therapy from a neurodiversity-affirming perspective has been linked to higher ratings of well-being in autistic adults and produce better therapeutic outcomes (Kroll et al., 2024).
Researchers and autistic advocates have united in calling for studies that move beyond deficit-focused approaches to examine interventions that honor autistic ways of being while addressing genuine support needs (Dietz et al., 2020). This call reflects a paradigm shift from interventions historically designed to reduce autistic traits or promote conformity to neurotypical standards, towards approaches that affirm neurodiversity and prioritize the well-being, autonomy and lived experience of autistic individuals. Rather than framing autistic characteristics as deficits to be corrected, these approaches seek to reduce distress, remove systemic barriers and enhance quality of life. This shift aligns with broader movements in disability studies and public health that emphasize dignity, self-determination and inclusive support, moving beyond remediation towards genuine empowerment and equity.
This study addresses these critical gaps by examining two key questions: First, how do autistic adults respond to individual CBT specifically adapted for autism? Second, does participation in psychoeducation groups, which may provide the community connection and identity affirmation that individual therapy cannot, confer additional benefits for quality of life above and beyond psychotherapy alone? By investigating both individual and group-based interventions delivered via telehealth, this study offers vital insights into approaches that could transform mental health care for a population that has been historically underserved and misunderstood.
Research Questions
We sought to answer two research questions:
Do mood, anxiety, social relationships and quality of life improve over time for all participants, regardless of their participation in one or more psychoeducation groups? Will people who participated in at least one psychoeducation group demonstrate significant differences in their trajectories of change than those who did not? In other words, are there added benefits (or harms) of participation in peer-led psychoeducation groups for autistic adults?
Method
Participants
Participant demographic information can be found in Table 2. This study utilized a retrospective chart review design with a convenience sample of 460 adults seeking therapy from a telehealth organization specializing in autism-informed services. An operational team external to the research team randomly selected participants who had baseline data available within the electronic health record on all four outcome variables and had consented to having their clinical data used for de-identified research purposes.
Demographic and Clinical Characteristics of the Sample (N = 460).

The organization operates entirely online across eighteen states in the United States, with most sessions covered by private insurance carriers. Clients are primarily self-referred and complete a self-initiated HIPAA-compliant online intake, though occasionally a physician, psychiatrist, therapist or other professional may suggest participation. The organization's byline states “Online Adult Autism Therapy and Testing Services,” and all psychotherapy utilizes autism-specific DBT, ACT and CBT approaches. The only evaluations conducted are autism assessments.
Participants were not required to have or disclose formal diagnoses to receive services. Diagnostic information (e.g., anxiety, bipolar disorder, autism) was collected via self-report at intake, with individuals selecting applicable conditions through checkbox responses without limitation on the number of selections. Given the organization's explicit focus on autism-informed therapy for autistic adults, we operated under the assumption that most participants identified somewhere on the autism spectrum, regardless of formal documentation.
No self-reported conditions resulted in exclusion from psychotherapy services. Data regarding autism support levels were not systematically collected, consistent with our self-identification approach, though we assume the majority of participants would meet criteria for Level 1 autism support needs. Our sample comprised English-speaking autistic adults without apparent intellectual disabilities.
Individual Therapy and Psychoeducation Group Descriptions
For brevity, detailed descriptions of the neurodivergent-affirming individual therapy and the psychoeducation group can be found in Supplementary Materials.
Ethics Review and Informed Consent
All participants gave informed consent for the use of their clinical data for research purposes before we collected data. We stored this data in a HIPAA-compliant electronic database. The organization's internal 11-member institutional review board (IRB), consisting of autistic community members and advocates external to the organization, autistic psychologists internal to the organization and other researchers external to the organization who did not identify as autistic, both inside of and outside of the United States, reviewed an electronic submission of the project. It was approved. Extensive care and consideration was given to patient privacy, and all data was de-identified by staff members not associated with the study before being given to the team of investigators. As our population is vulnerable, especially in light of the recent political climate, for the protection of participants, the data is not uploaded to a shared database to enhance trust with the autistic community.
Participatory Methods and Positionality Statement
The research team brings diverse lived experiences and professional expertise to this work. Two of the three authors are neurodivergent: one author has attention-deficit/hyperactivity disorder (ADHD) and demonstrates traits across a broad autism phenotype, while another author also has ADHD. In addition to working with the autistic community professionally, and sharing overlapping traits, both neurodivergent authors have multiple close autistic relatives and friends, providing personal insight into the autistic community. The third author, while not neurodivergent, has specialized in neurodiversity-affirming care for many years, serves as an ally to the autistic community and directs therapeutic programmes serving autistic adults.
This combination of lived experience, community connections and professional expertise fundamentally shaped our research approach, interpretation of findings and commitment to autistic input and oversight. Our positionality influenced our decision to prioritize community-based advisory boards and inputs when creating study design and to include autistic members on our IRB, emphasize real-world effectiveness over controlled conditions and focus on interventions that honour autistic ways of being rather than seeking to modify autistic traits. The neurodivergent authors’ personal understanding of masking, burnout and the search for affirming community informed our interpretation of why peer-led groups showed particular benefits for social relationships and quality of life. While our therapy protocols, assessment measures and IRB were overseen by autistic individuals themselves, we acknowledge that due to limitations of our organization in its early phases, this research was not a true emancipatory community-based co-production of knowledge.
Assessments and Measures
The World Health Organization’s Quality of Life Questionnaire
A modified version of the World Health Organization’s Quality of Life Questionnaire (WHOQOL-Bref) (WHOQOL Group, 1998) was used. Two neurodivergent psychologists modified the wording to be less ambiguous for use with a neurodivergent population based on theory and practice; these modifications were reviewed and approved by a team of autism specialists and an autistic psychologist/stakeholder. The WHOQOL-Bref was used due to its generic acceptability across several countries and cultures (Skevington et al., 2004) and emerging support for its use with adult autistic populations (Mason et al., 2022). It was modified for readability and to reduce items.
There is already a pre-existing adaptation of the WHOQOL-BREF for autistic individuals (McConachie et al., 2018), but it was not appropriate for the clinical needs of our population after informally surveying feasibility. The autism-adapted WHOQOL-BREF developed by McConachie and colleagues consists of the full 26-item WHOQOL-BREF in addition to an additional 9-item autism-specific module (ASQoL), creating a 35-item measure (McConachie et al., 2018). While this comprehensive measure represents important advances in autism research methodology, its length renders it impractical for routine clinical implementation in applied mental health settings.
Our modification approach differed fundamentally from the McConachie adaptation. Rather than adapting content to address autism-specific experiences, we adapted the measure's already-existing items for readability, usability and feasibility for real-world clinical practice with neurodivergent populations. Requiring participants to complete 35 quality of life items at each therapy session would be prohibitively burdensome for our population seeking therapeutic services and would likely result in assessment fatigue and reduced treatment engagement.
The adapted measure we co-created is currently undergoing psychometric validation and reliability testing. It consists of nine items, each evaluating a different aspect of life, including physical health, mood, anxiety, social relationships, work or school, family relationships, leisure activities/hobbies, living/housing situation and overall sense of well-being. Participants rated each domain using a 5-point Likert scale, with response options ranging from Very Poor to Very Good. Although this adapted version of the WHOQOL-Bref has not yet undergone formal validation or reliability testing and was selected for its ability to provide a quick and accessible assessment of quality of life for autistic adults in psychotherapy, as data was originally collected for continuous quality improvement and tracking psychotherapy outcomes, rather than clinical research. Our approach prioritizes treatment accessibility and participant burden reduction.
Design and Data Analysis
We used R (R Core Team, 2024) for all quantitative data analyses. The dependent outcome variables were drawn from the QoL measure described above and included four items: mood, anxiety, social relationships and overall quality of life. We measured outcomes at five time points: intake, session 4, session 8, session 16 and session 24. We were interested in determining if there were meaningful differences in these scores within subjects, over time and also in examining the additional impact of group participation. After careful consideration, we ultimately chose to run a cumulative linear mixed model (CLMM; Christensen, 2019; McCullagh, 1980; Tutz & Hennevogl, 1996) to avoid errors associated with treating an ordinal variable as continuous (Liddell & Kruschke, 2018). The CLMMs also have the additional benefit of being less vulnerable to the effect of missing data due to maximum likelihood estimation (Molenberghs & Verbeke, 2004). Very few studies with truly ordinal outcome variables actually treat their variables as such; as a result, there is no seminal piece or best practice to follow for reporting guidelines. We did our best to follow Meteyard and Davies (2020) when relevant.
Power Analysis
Based upon prior literature with linear mixed effects models, (Brauer & Curtin, 2018; Brysbaert & Stevens, 2018; Scherbaum & Ferreter, 2009; Snijders & Bosker, 2012) upwards of 900–2500 observations are likely sufficient to produce reliable estimates with a medium effect size. The present study consists of 2300 observations. As a result, we feel comfortable proceeding with the CLMM analysis.
Data Assumptions
Schmidt (2012) suggests only two assumptions must be met to run a CLMM: independence of observations and proportional odds. Similarly, Christensen (2019) also suggests proportional odds as the only assumption for CLMMs. We inspected residual plots for all four outcome variables (mood, anxiety, social relationships, quality of life) which all suggested no clear evidence of non-independence. When comparing models assuming proportional odds to models assuming non-proportional odds for all four variables, there was no significant difference between the proportional odds models and a model fit statistic, the Akaike information criterion (AIC), did not shift dramatically, suggesting that the proportional odds assumption is met.
Results
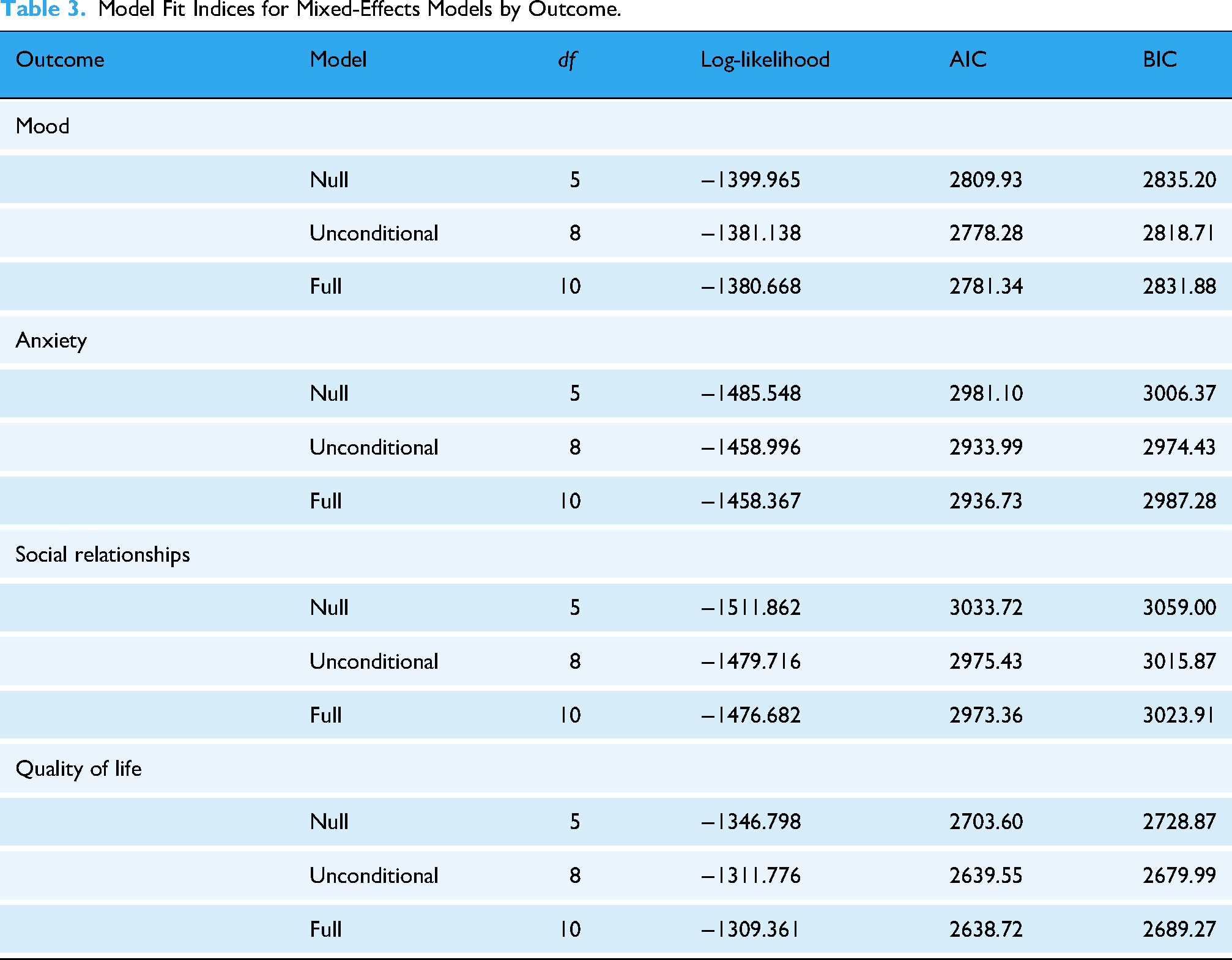
To examine whether psychoeducation groups provided added benefit, we compared model fit statistics (AIC/BIC) between null and full models. We first assessed overall improvement across all participants using unconditional models (Research Question 1), then tested whether improvement trajectories differed between group attendees and non-attendees using conditional growth models with time × group interaction terms (Research Question 2). All odds ratios used profile likelihood confidence intervals for more reliable estimates. All model fit statistics can be found in Table 3. Results of the CLMMs can be found in Table 4 with a visual representation on Figure 1. For ease of interpretation, the log-odds coefficient (b) was exponentiated to produce odds ratios. Research Question 1: Do mood, anxiety, social relationships and quality of life improve over time for all participants, regardless of their participation in one or more psychoeducation groups?
Model Fit Indices for Mixed-Effects Models by Outcome.
Cumulative Link Mixed Model Results Predicting Changes in Mood, Anxiety, Social Relationships and Quality of Life Over Time by Group Participation.

Note. OR = odds ratio. b represents the log-odds coefficient. SE represents the standard error.
Mood
All Participants Combined. In the unconditional model (i.e., without accounting for group status), mood scores increased over time for everyone, regardless of their participation in one or more psychoeducation groups (b = 0.34, SE = 0.06, p < 0.001). The odds ratio of 1.41 (95% CI [1.26, 1.58]) means that with each additional time point, participants had 41% greater odds of reporting a higher mood rating, regardless of whether they participated in a psychoeducation group. The overall odds ratio (OR = 1.41) is not a simple average of the subgroup odds ratios from the conditional growth model reported below because it comes from a separate, unconditional model that does not account for group status or interaction effects. Instead, it reflects the general trend across the entire sample, which can result in different ORs due to differences in group sizes, variance and model structure. It is still reported as this number captures the overall within-subject change over time across the entire sample and offers a broad picture of whether or not participants’ mood increased over time, regardless of whether they participated in a group or not. This is further broken down by subgroups below.
Individual Therapy Only. Looking only at the subgroup of individuals who participated only in individual therapy, and who did not participate in a group, we found a significant increase in mood over time (b = 0.33, SE = 0.07, p < 0.001). The odds of reporting a higher mood rating for individuals only participating in individual therapy increased by a factor of 1.38, or approximately 38%, with each additional time point (95% CI [1.199, 1.595]).
Individual Therapy and Group Participation. Looking only at the subgroup of individuals who engaged in both individual therapy and a group, we found a significant mood increase over time (b = 0.38, SE = 0.10, p < 0.000). For ease of interpretation, the log-odds coefficient (b) was again exponentiated to produce odds ratios. The odds of reporting a higher mood rating in those participating in both individual therapy and a group increased by a factor of 1.46, or approximately 40%, with each additional time point (95% CI [1.204, 1.762]).
Anxiety
All Participants Combined. In the unconditional model (i.e., without accounting for group status), anxiety scores increased over time (representing an increase in their satisfaction with levels of anxiety/decreased anxiety) for everyone, regardless of their participation in one or more psychoeducation groups (b = 0.41, SE = 0.06, p < 0.001). The odds ratio of 1.50 (95% CI [1.34, 1.68]) means that with each additional time point, all participants had 50% greater odds of reporting lower anxiety ratings, ignoring group status. Please see the note above regarding interpretation of this odds ratio. This is further broken down by subgroups below.
Individual Therapy Only. Looking only at the subgroup of individuals who participated only in individual therapy, and who did not participate in a group, we found a significant increase in reduction of anxiety over time (b = 0.37, SE = 0.07, p < 0.001). The odds of reporting a better anxiety rating for individuals only participating in individual therapy increased by a factor of 1.44, or approximately 44%, with each additional time point (95% CI [1.26, 1.66]).
Individual Therapy and Group Participation. Looking only at the subgroup of individuals who engaged in both individual therapy and a group, we found a significant increase in reduction of anxiety symptoms over time (b = 0.49, SE = 0.10, p < 0.001). The odds of reporting lower anxiety in those participating in both individual therapy and a group increased by a factor of 1.63, or approximately 63%, with each additional time point (95% CI [1.341, 1.97]).
Social Relationships
All Participants Combined. In the unconditional model (i.e., without accounting for group status), social relationship scores increased over time for everyone, regardless of their participation in one or more psychoeducation groups (b = 0.45, SE = 0.06, p < .001). The odds ratio of 1.57 (95% CI [1.40, 1.76]) means that with each additional time point, participants had 57% greater odds of reporting higher satisfaction with their social relationships, regardless of whether they participated in a psychoeducation group. Please see the note above regarding interpretation of this odds ratio. This is further broken down by subgroups below.
Individual Therapy Only. Looking only at the subgroup of individuals who participated only in individual therapy, and who did not participate in a group, we found a significant improvement in social relationship scores over time (b = 0.36, SE = 0.07, p < 0.001). The odds of reporting better social relationship satisfaction for individuals only participating in individual therapy increased by a factor of 1.43, or approximately 43%, with each additional time point (95% CI [1.241, 1.643]).
Individual Therapy and Group Participation. Looking only at the subgroup of individuals who engaged in both individual therapy and a group, we found a significant increase in reduction of anxiety symptoms over time (b = 0.63, SE = 0.1, p < 0.001). The odds of reporting lower anxiety in those participating in both individual therapy and a group increased by a factor of 1.88, or approximately 88%, with each additional time point (95% CI [1.542, 2.289]).
Quality of Life
All Participants Combined. In the unconditional model (i.e., without accounting for group status), quality of life scores increased over time for everyone (b = 0.49, SE = 0.06, p < .001). The odds ratio of 1.63 (95% CI [1.446, 1.847]) means that with each additional time point, participants had 63% greater odds of reporting higher quality of life satisfaction, regardless of whether they participated in a psychoeducation group. Please see the note above regarding interpretation of this odds ratio. This is further broken down by subgroups below.
Individual Therapy Only. Looking only at the subgroup of individuals who participated only in individual therapy, and who did not participate in a group, we found a significant improvement in quality of life scores over time (b = 0.40, SE = 0.00, p < 0.001). The odds of reporting better quality of life for individuals only participating in individual therapy increased by a factor of 1.49, or approximately 49%, with each additional time point (95% CI [1.48, 1.49]).
Individual Therapy and Group Participation. Looking only at the subgroup of individuals who engaged in both individual therapy and a group, we found a significant increase in quality of life over time (b = 0.68, SE = 0.11, p < 0.001). The odds of reporting better quality of life in those participating in both individual therapy and group increased by a factor of 1.97, or approximately 97%, with each additional time point (95% CI [1.61, 2.40]). Research Question 2: Will people who participated in at least one psychoeducation group demonstrate significant differences in their trajectories of change than those who did not? In other words, are there added benefits (or harms) of participation in peer-led psychoeducation groups for autistic adults?
Mood
A CLMM with a logit link was used to examine whether changes in mood over time differed significantly between those who participated in a psychoeducation group and those who did not. The main effect of group therapy participation was not significant (b = 0.04, SE = 0.30, p = 0.880), suggesting that members of both groups had baseline values that were roughly the same for mood. This information increases confidence that interaction effects are not solely due to group differences at baseline. The interaction between time and group therapy (b = 0.06, SE = 0.12, p = 0.592) was not significant (Table 4); odds ratios are not reported due to non-significance of this finding. This suggests that the rate of change did not differ significantly between those who did and did not attend a psychoeducation group, indicating that attending the group did not add any statistically significant value or harm for our sample.
Anxiety
A CLMM with a logit link was used to examine whether changes in anxiety over time differed significantly between those who participated in a psychoeducation group and those who did not. The main effect of group therapy participation was not significant (b = −0.33, SE = 0.30, p = 0.261), suggesting that members of both groups had baseline anxiety scores that were roughly the same. This increases confidence that interaction effects are not solely due to group differences at baseline. The interaction between time and group therapy (b = 0.11, SE = 0.12, p = 0.328) was not significant (Table 4); odds ratios are not reported due to non-significance of this finding. This suggests that the rate of change did not differ significantly between those who did and did not attend a psychoeducation group, indicating that attending the group did not add any statistically significant value or harm in reducing anxiety for our sample.
Social Relationships
A CLMM with a logit link was used to examine whether changes in anxiety over time differed significantly between those who participated in a psychoeducation group and those who did not. The main effect of group therapy participation was statistically significant (b = −0.74, SE = 0.30, p = 0.015), suggesting that, at baseline, those in the psychoeducation group condition reported lower social relationship scores than those in individual therapy only. The interaction between time and group therapy (b = 0.25, SE = 0.12, p < 0.05) was significant (Table 4). The odds of reporting a higher social relationship satisfaction rating for participants who attended a psychoeducation group compared to those who did not increased by a factor of 1.29, or approximately 29% (95% CI [1.023, 1.614]) with each additional time point. This suggests that participants who attended a psychoeducation group experienced greater increases in social relationship satisfaction over time compared to those who did not. However, it is important to note that those who attended the group also had a lower social relationship score to start compared to those who did only individual therapy. Participating in a group was associated with added benefits that are meaningful in improving social relationships over time for autistic adults.
Quality of Life
A CLMM with a logit link was used to examine whether changes in quality of life over time differed significantly between those who participated in a psychoeducation group and those who did not. The main effect of group therapy participation was not significant (b = −0.34, SE = 0.29, p = 0.249), suggesting that baseline quality of life scores did not differ significantly between groups. The interaction between time and group therapy (b = 0.28, SE = 0.10, p = 0.006) was statistically significant (Table 4). The odds of reporting a higher quality of life rating for participants who attended a psychoeducation group compared to those who did not increased by a factor of 1.32, or approximately 32%, with each additional time point. This suggests that participants who attended a psychoeducation group experienced greater increases in quality of life compared to those who did not; participating in a group was associated with meaningful added benefits in improving quality of life for autistic adults.
Discussion
The present study examined quality of life outcomes among autistic adults receiving individual CBT and neurodivergent-led psychoeducation groups. Our findings provide important insights into effective mental health interventions for this population, which highlight the importance of community as a core component of mental health interventions.
Main Findings
Participants showed statistically significant improvements across all measured domains, aligning with a growing body of evidence supporting the efficacy of appropriately adapted psychotherapy for autistic adults (Cooper et al., 2018; Spain et al., 2015). This finding is particularly encouraging given the well-documented challenges autistic adults face in accessing effective mental health services (Vohra et al., 2017). The most striking findings emerged in the social relationships and quality of life domains, where participants in psychoeducation groups demonstrated significantly steeper improvement trajectories compared to those receiving individual therapy alone (OR = 1.29 for social relationships, OR = 1.32 for quality of life). This pattern aligns with research highlighting themes of isolation and lack of belonging among late-diagnosed autistic adults (Hymas et al., 2024) and suggests that group interventions may specifically address unmet needs for social connection. Notably, those who attended groups had significantly lower baseline social relationship satisfaction, indicating both greater room for improvement and possible self-selection based on recognizing this need.
Mood and anxiety improvements occurred at similar rates regardless of group participation, suggesting that individual therapy may be sufficient for addressing these symptoms. This finding supports previous research demonstrating the effectiveness of adapted CBT for anxiety and mood concerns in autistic populations (Spain et al., 2015), while highlighting that improvement in social connection and quality of life may require additional interventions.
Clinical Implications
The effectiveness of brief psychoeducation groups is particularly noteworthy. Over one-third of participants (35.2%) attended only a single session and demonstrated meaningful benefits. This suggests that even low-intensity group interventions can produce significant effects, consistent with findings that peer support and shared identity can be powerful therapeutic factors for marginalized populations (Bottema-Beutel et al., 2020). For autistic adults who face substantial barriers to care, including long waitlists, financial costs and sensory challenges in clinical environments, brief telehealth-delivered group interventions represent a potential approach to improving outcomes.
These findings have implications for treatment planning and referral practices. Clinicians should consider group interventions especially for clients presenting with social isolation or expressing lack of belonging. The neurodivergent-led format may provide unique benefits through shared understanding and reduced communication barriers, consistent with research showing that autistic adults often prefer services delivered by neurodivergent clinicians and experience improved rapport with other autistic people (Crompton et al., 2020; Milton et al., 2022). However, it remains unclear whether these benefits stem specifically from neurodivergent leadership or simply from any psychoeducation group participation, as this study lacked a neurotypical-led comparison group.
Theoretical Contributions
This study advances the limited evidence base for autism mental health interventions in several ways. The real-world clinical context strengthens external validity, as findings reflect how autistic adults actually engage with telemental health services in community settings rather than artificially controlled research environments. Our findings support neurodiversity-affirming approaches that position autistic individuals as active agents in their care rather than passive recipients (Chapman & Botha, 2023). The demonstrated success of neurodivergent-led groups aligns with double empathy theory (Milton, 2012), which proposes that communication and mutual understanding improve when people share similar neurotypes; this framework may help explain the additional benefits observed in our study, though additional research comparing neurodivergent-led versus neurotypical-led groups is needed to isolate this specific mechanism. The differential impact of intervention types on distinct well-being domains suggests that comprehensive care for autistic adults may require multi-modal approaches targeting both individual symptoms and broader psychosocial needs.
Limitations
Several limitations should be considered when interpreting these findings. The non-randomized design prevents causal inferences about intervention effectiveness. Baseline differences between groups introduce potential confounding. While this pattern may reflect appropriate self-selection, with individuals recognizing their need for connection, it could also indicate that observed benefits simply reflect greater room for improvement or higher motivation among group participants rather than specific group effects. The absence of a neurotypical-led comparison group further limits our ability to determine whether benefits stem from neurodivergent leadership specifically or from any psychoeducation group format. Additional factors may have contributed to community building beyond self-disclosure of diagnoses. While our groups incorporated psychoeducation, skill-building and peer support elements, we did not systematically measure which components drove improvements. Future research should examine specific mechanisms and group processes that facilitate belonging and connection.
The modified WHOQOL-Bref has not undergone formal validation, limiting confidence in measurement precision. While modifications were reviewed by autism specialists and autistic stakeholders, comprehensive psychometric evaluation is needed and currently underway. The convenience sample from a single telehealth organization may limit generalizability, as may the predominantly female-assigned-at-birth sample and lack of data on racial and ethnic diversity. Participants were primarily speech-using adults unlikely to meet intellectual disability criteria, limiting applicability to the broader autism spectrum. High missing data rates (approximately 25%) may have biased results despite the robustness of CLMMs. The majority of participants (61.1%) did not engage in psychoeducation groups, which could reflect positive treatment effects in individual therapy reducing perceived need, or barriers to group engagement including social anxiety, sensory sensitivities or scheduling constraints.
For simplicity, initial models did not include covariates (e.g., age, sex assigned at birth) or non-linear change patterns, potentially obscuring confounding or complex trajectories. We ran four separate models rather than multivariate approaches, which does not account for correlations among outcomes and increases Type I error risk. However, this approach provided clear, focused understanding of domain-specific effects. Future work should employ more complex modelling approaches including relevant covariates, non-linear terms and multivariate or Bayesian frameworks.
Future Directions
Future research should address these limitations through several avenues. Randomized controlled trials are needed to establish causal relationships between interventions and outcomes, with careful attention to controlling for baseline differences and selection effects. Future studies should also investigate optimal timing and dosing of group interventions, as well as factors that influence group participation decisions among autistic adults seeking mental health services. Given the preliminary nature of these findings, replication studies across diverse service settings and populations will be crucial for establishing the generalizability and robustness of observed effects before recommending widespread implementation of these intervention approaches.
Additionally, research examining the specific mechanisms through which neurodivergent-led groups produce benefits (e.g., identity affirmation, social modelling or community belonging) or which autism-specific adaptations are most helpful in individual therapy would inform the development of more targeted interventions, in addition to utilizing neurotypical-led or non-explicitly affirming psychoeducational groups as a comparison group.
Future studies should also prioritize recruiting more diverse samples, including greater racial and ethnic diversity and broader representation across the autism spectrum and including individuals with different support needs and communication styles. Also, research examining the cost-effectiveness of combined individual and group interventions would inform healthcare policy and service delivery decisions.
Finally, future studies should incorporate relevant covariates to control for potential confounding influences. Further studies can explore more complex trajectories of change over time by including non-linear terms (e.g., quadratic or cubic effects) to capture potential curvilinear patterns in outcomes, by using more complex Bayesian approaches to run one model as opposed to four separate models, and to investigate heterogeneity in response patterns by employing latent transition analysis (LTA) or related mixture modelling.
Conclusion
This study provides preliminary evidence that autistic adults can achieve meaningful improvements in quality of life, mood, anxiety and social relationships through neurodiversity-affirming mental health interventions delivered via telehealth in real-world clinical settings. The demonstrated effectiveness of autism-adapted individual therapy for mood and anxiety, combined with the additional benefits of neurodivergent-led psychoeducation groups for social relationships and quality of life, addresses critical gaps in mental health access for this underserved population. The telehealth delivery model overcomes substantial barriers including sensory sensitivities to clinical environments, transportation challenges and geographic isolation from autism-informed providers, with particular promise for reaching rural and underserved communities. By demonstrating that brief, peer-led interventions can produce meaningful benefits in authentic service delivery contexts, these findings provide actionable guidance for clinicians, researchers and healthcare systems committed to advancing mental health equity for autistic adults.
Expected scores for Mood, Anxiety, Social Relationships and Quality of Life over time by treatment group in autistic adults receiving telehealth services.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330251408867 - Supplemental material for A Pilot Study of Telehealth-Delivered Autism-Adapted CBT and Neurodivergent-Led Groups: Preliminary Evidence for Mood, Anxiety, Relationship and Quality of Life Improvements in Autistic Adults
Supplemental material, sj-docx-1-ndy-10.1177_27546330251408867 for A Pilot Study of Telehealth-Delivered Autism-Adapted CBT and Neurodivergent-Led Groups: Preliminary Evidence for Mood, Anxiety, Relationship and Quality of Life Improvements in Autistic Adults by Kelly M. Whaling, Glen Veed and Rachel Loftin in Neurodiversity
Footnotes
Acknowledgments
The authors thank the autistic stakeholders, community members and psychologists who contributed to study design, IRB oversight, and review of early findings: Drew Carson, Jessica Monahan Pollard, Kris Guin, Lindsey Nebeker, Melanie Penner, Katherine Pang, Hannah Infinger, Nicole Russell and Michelle Gaines. The authors also thank Emily Goldman, Annabelle Raine, Byrne Hollander, our engineering and operations staff and our therapists, many of whom are autistic and share their lived experience in practice. Finally, the authors are grateful to the clients who participated.
Ethical Approval and Informed Consent
This study was reviewed and deemed exempt by an international IRB with autistic and non-autistic members. All participants provided informed consent.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: All authors were employed by Prosper Health, the organization where data was collected, during study implementation and manuscript preparation. K.W. and R.L. occasionally served as backup co-facilitators for psychoeducation groups.
Data Availability Statement
Participants were never informed that their data might be shared beyond the direct research team or organization. Even in aggregated and de-identified form, releasing these data may violate the trust participants placed in us and the ethical commitment we hold to the autistic community. To honour their autonomy, privacy and data sovereignty, individual-level and de-identified datasets will not be publicly shared. Only summary or aggregate results may be provided in response to inquiries, and always in a manner that safeguards participant confidentiality and respects the community's right to control how their information is used.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.