
Abstract
Over the past 25 years, research has documented racial/ethnic differences and gaps in aspects of autism identification, including age of diagnosis and prevalence rates. A trend has been identified wherein Black youth are more likely than their peers to have autism with accompanying intellectual disability (ID). The present study used five years of data from the National Survey of Children's Health (2017–2021) and multivariable logistic regression to identify if there were racial/ethnic differences in the age of autism diagnosis, severity classification, and cooccurring psychiatric and developmental conditions while also accounting for a diagnosis of ID. The study's results demonstrated that when accounting for ID, Hispanic youth had higher odds of being diagnosed in infant or toddlerhood (ages 1–3) than in middle childhood (ages 6–9) compared to White youth. In addition, youth in the Black and multiracial/other groups had lower odds of being diagnosed during adolescence (ages 10–15+). The following article provides support for the presence of diagnostic gaps and implications for research and practice.
Lay Abstract
Autism is a condition that affects how children interact, communicate, and behave. Getting diagnosed early can make a big difference, allowing families to access services and support that help children thrive. However, not all children are diagnosed at the same age or in the same way, especially when it comes to children from different racial and ethnic backgrounds.
In this study, we looked at national survey data from over 4000 children with autism in the United States to explore whether race and ethnicity are linked to differences in when children are diagnosed, how severe their autism is rated, and whether they also have other conditions like attention-deficit/hyperactive disorder, anxiety, or depression. We also considered whether the child had been diagnosed with intellectual disability (ID), which can sometimes influence how and when autism is identified.
We found that Hispanic children were more likely to be diagnosed with autism during toddlerhood (ages 1–3). In contrast, Black and multiracial children were less likely to be diagnosed during adolescence compared to White children. This suggests that children of color may be diagnosed earlier if they have more visible challenges but may be overlooked if their needs are less obvious, especially during the teenage years, when diagnosis can still be necessary.
Our study also showed that Black children were more likely to be reported as having more severe autism symptoms, which could reflect how clinicians or families perceive autism when ID is also involved. In addition, Black children were less likely to be diagnosed with anxiety compared to White children, even though anxiety is common among youth with autism. This points to possible gaps in recognizing mental health needs in autistic youth of color.
Why this matters:
Our findings highlight that children of color may face unequal experiences when it comes to autism diagnosis, both in terms of timing and the way their symptoms are understood. These differences could mean some children are not getting the help they need, especially if they don't show more obvious signs early in life.
This research can help healthcare providers, educators, and policymakers better understand how race and disability interact to shape the diagnostic journey. By improving awareness of these disparities and promoting more culturally responsive screening and support practices, we can make autism services more equitable, ensuring that all children, regardless of race or background, receive timely and accurate diagnoses and the care they deserve.
Race/Ethnicity, Intellectual Disability, Diagnostic Characteristics, and Cooccurring Conditions Among School-Aged Youth with Autism: A Cross-Sectional Study
Autism is a neurodevelopmental condition marked by difficulties with social interaction and repetitive and restrictive behaviors, interests, and activities. Autism impacts social and behavioral functioning beginning during the developmental period and persists throughout the lifespan. Understanding autism remains a critical public health concern due to its increasing prevalence (Zeidan et al., 2022). Several campaigns have been developed to support the early identification of autism, and early intervention serves as an efficacious tool in mitigating the exacerbation of emotional and behavioral concerns associated with later diagnosis (Mandy et al., 2022; Raspa et al., 2015). Research over the past 25 years has documented racial/ethnic differences in aspects of autism identification, including age of diagnosis and prevalence rates (Mandell et al., 2002, 2009; Valicenti-McDermott et al., 2012). White youth are identified more frequently compared to Black and Hispanic youth (Baio et al., 2018). However, recent data from the Autism and Developmental Disabilities Monitoring, a program funded by the CDC, suggests that this gap may be narrowing, with autism rates being similar across White, Black, and Hispanic youth (CDC, 2023).
Notably, a trend has been identified wherein Black youth are more likely than their peers to have autism with accompanying intellectual disability (ID), a condition with impairment in cognitive and adaptive functioning (Ratto et al., 2016). ID is one of the many cooccurring conditions that can impact the trajectory of autism. Findings on the influence of cognitive ability on autism severity and age of diagnosis have been mixed. Generally, research has suggested that youth with lower cognitive abilities, frequently evidenced by a diagnosis of ID, are diagnosed earlier and with greater severity. In contrast, youth without cognitive impairments are diagnosed at later ages (Hagberg & Jick, 2017; Leader et al., 2022). The current study aims to determine if there are differences across ranges of diagnosis age, severity rating, and cooccurring psychiatric conditions based on race/ethnicity and cooccurring ID. In doing so, this study explores whether gaps in autism identification remain present when accounting for the cooccurrence of ID among youth of color.
Literature Review
Autism and Cooccurring Conditions
Autism has a heterogeneous presentation marked by varied levels of severity and support needs. Early interventions are considered critical in addressing autism due to the neuroplasticity of brain regions during the early developmental period, which supports growth across domains of functioning (Novak & Morgan, 2019). While the age of 24 months has been reported as the age at which autism can be reliably diagnosed, some youth experience delays in diagnosis for many reasons (CDC, 2025). First, some youths can function without their autism being detected until social demands exceed their capacities, such as those that begin to present in middle childhood and adolescence. Second, several conditions cooccur with autism, including attention-deficit/hyperactive disorder (ADHD) and ID, both of which can complicate the clinical presentation of the condition, influencing the age of diagnosis and severity classification (Hatch et al., 2023; Miodovnik et al., 2015; Shenouda et al., 2023; Thurm et al., 2019). A combination of impairments in intellectual (i.e. IQ <70) and adaptive functioning is conducive to a diagnosis of ID (Diagnostic and Statistical Manual of Mental Disorders, 2013). ID is a developmental disorder impacting thinking and reasoning, independent functioning, and generalization of skills across settings (Diagnostic and Statistical Manual of Mental Disorders, 2013). The estimated prevalence of autism with cooccurring ID is approximately 30% (Shenouda et al., 2023). Research suggests that having an IQ below the cutoff characteristic of ID is associated with an early diagnosis age (Shattuck et al., 2009). Further, racial differences have been seen in the cooccurrence of ID, with Black and Hispanic youth more likely to be identified with ID (Patrick et al., 2021).
ADHD and Behavior Problems
ADHD is a developmental condition that has impacts on executive functioning, impulse control, and attentional processes. This condition is marked by hyperactivity, inattentiveness, or both. The prevalence rate of ADHD cooccurring with autism is around 40% (Rong et al., 2021). Sometimes social and behavioral challenges are attributed solely to ADHD when there is cooccurring autism (Miodovnik et al., 2015). ADHD can present similarly to oppositional defiant disorder and conduct disorder due to the presence of externalizing symptoms and commonly cooccurring with each other (Dick et al., 2005). In the general youth population, racial/ethnic differences appear to be a salient factor in the diagnoses of these conditions, such that youth of color were less likely to be diagnosed with ADHD and more likely to be diagnosed with conduct problems (Fadus et al., 2020). Black youth were more likely to have concurrent ADHD and conduct disorder than White youth, and poverty and region were associated with this (Fadus et al., 2020). Further, Hispanic, Black, and youth from other racial backgrounds were less likely to have a diagnosis of ADHD (Visser et al., 2016). Overall, there may be an underdiagnosis of ADHD among Black and Hispanic youth (Coker et al., 2016). Behavior problems are also commonly cooccurring with both autism and ID. Behavior problems in autism have been linked to sleeping issues, hyperactivity, and internalizing symptoms (Hill et al., 2014). In ID, behavior problems are attributed to sleeping issues and chronic pain, which present as aggression in destructive behavior directed both toward self and others (Ageranioti-Bélanger et al., 2012). Given the high cooccurrence of ADHD among autistic youth and the racial disparities in its diagnosis, it is important to consider how externalizing behaviors may be differentially attributed across racial groups when autism is also present.
Internalizing Conditions
Internalizing symptoms and disorders such as anxiety and depression are also common cooccurring conditions associated with autism (Cai et al., 2018; Kerns et al., 2015; Williams et al., 2022). Anxiety can develop due to difficulties with social situations, sensory difficulties, alexithymia, intolerance of uncertainty, and cognitive inflexibility (Ozsivadjian et al., 2021; Spain et al., 2018; South & Rodgers, 2017). Depression in autistic youth can arise from experiences of victimization, such as bullying, which can impact self-esteem and lead to social isolation (Rai et al., 2018). These internalizing symptoms may be obscured by autism but are important to understand due to their association with self-injurious behavior (Pezzimenti et al., 2019; Stewart et al., 2006). Black, autistic youth were found to have more depressive symptoms than White youth, and this may be exacerbated by code-switching, the process of altering communication styles based on environment and contexts, as well as masking, the process of concealing autistic traits (Cage & Troxell-Whitman, 2019; Williams et al., 2022).
Taken together, many externalizing and internalizing symptoms can cooccur with autism, and these may present differently when an ID is present, which has been an understudied area of research. Many aspects of autism diagnosis and treatment can be impacted by understanding cooccurring conditions and how the intersection of race and disability shapes the lives of youth with autism. For instance, youth of color may be particularly susceptible to the dual processes of racism and discrimination based on ability. This dual discrimination can be compounded by challenges in social-emotional communication, causing the internalization of negative emotional states. Beyond the impact of internalizing and externalizing conditions, socioeconomic factors can contribute to the experiences of youth of color as they navigate getting a diagnosis of autism.
Racial Differences in Autism Identification and Treatment: Contributing Factors and Findings
One major contributor to disparities related to autism identification and treatment is socioeconomic status. A report by the CA.J. Drexel Autism Institute's Policy and Analytics Center and Life Course Outcomes Program noted that compared to youth without autism, autistic youth were more likely to live in low-income homes and poverty (The Intersection of National Autism Indicators Report: Autism, Health, Poverty and Racial Inequity—Drexel University, n.d.). Poverty is a powerful social determinant of health. While several government assistance programs have been developed to address economic disparities, poverty remains a large barrier to access to healthcare, particularly among Black and Hispanic youth (Dababnah et al., 2018; Zuckerman et al., 2014). For families with youth of color, navigating healthcare settings can be perceived as being met with discrimination based on race and class, as well as occurring within a community context with a limited understanding of autism (Stahmer et al., 2019). Parents below the federal poverty line were found to have less awareness of interventions that can support autism and the services received by their children (Longtin & Principe, 2016). This lack of knowledge can serve as a barrier to parents advocating for their child's health needs. Beyond resource availability, a lack of parental knowledge of mental health and psychiatric conditions may impact their ability to share concerns in these areas with healthcare providers. Altogether, socioeconomic status can particularly impact the lives of autistic youth of color.
Cognitive ability and race/ethnicity both have impacts on the differential identification of autism in youth of color when compared to White youth. Black and Hispanic youth are identified as having ID with autism at greater rates than White youth (Baio et al., 2018). In schools, Black youth are significantly more likely to have a special education eligibility classification of ID compared to other groups (Disproportionate Identification of Students of Color in Special Education—Learning Disabilities Association of America, n.d.). Black youth diagnosed at later ages had to have more autistic traits than White youth, who were more likely to have higher IQs and higher internalizing symptoms (Ratto et al., 2016). Finally, Black and Hispanic youth with mild and moderate autism were less likely to be diagnosed at later ages (Jo et al., 2015). Altogether, these findings suggest that autism without accompanying intellectual impairment may be less readily identified among Black and Hispanic youth, which may present in differences in diagnosis at older ages for these youth, such that they are underidentified (Jo et al., 2015; Ratto et al., 2016; Rosenberg et al., 2011).
Present Study
Research focusing on youth of color with autism is warranted due to an increased vulnerability of experiencing double marginalization based on race/ethnicity and dis/ability (Annamma et al., 2013). The present study seeks to identify if there are racial differences in the diagnosis age of autism and severity classification based on race and ethnicity, while also accounting for forever receiving a diagnosis of ID. Previous investigations have been limited in exploring the role of ID cooccurring with autism as a point of disparity in autism identification across race/ethnicity. Understanding how ID impacts diagnosis for youth of color is particularly relevant due to the higher prevalence of cooccurring ID, which is a documented predictor of autism severity and prognosis. This study addresses previous limitations in sample size by using a nationally representative dataset to clarify the role of ID in the age of autism diagnosis and autism severity. Additionally, this study expands on existing autism literature by focusing on the roles of race/ethnicity and cooccurring ID as they relate to the presence of internalizing and externalizing conditions. Multivariable and multivariate logistic regressions are used to quantify potential differences between groups given the discrete outcomes of the current study. The two research questions at the center of this study are: (1) Are there differences in age of autism diagnosis and severity of autism based on race/ethnicity and ever receiving a diagnosis of ID? and (2) Are there differences in receiving diagnoses of co-occurring internalizing and externalizing conditions based on race/ethnicity and a comorbid diagnosis of ID? There are two hypotheses guiding this study. First, youth who have ever received a diagnosis of ID will have higher odds of autism severity ratings of moderate or severe compared to mild. Secondly, youth of color will have lower odds of being diagnosed in later years than White youth due to a higher prevalence of cooccurring ID among youth of color, associated with a higher autism severity and earlier age of diagnosis.
Methods
Data
Secondary data analysis was conducted using the 2017 through 2021 years of the National Survey of Children's Health (NSCH) (Bureau, n.d.). The NSCH is a cross-sectional, nationally representative, self-administered survey of youth aged 0–17 years to gather information about physical and mental health, health care access utilization, and the functioning of American families across contexts. The NSCH is funded by the Health Resources and Services Administration Maternal and Child Health Bureau. The survey was administered online or through paper formats and contained pertinent questions about child development and other aspects of special health needs. Sampling weights were adjusted to account for the multiple years included in the current analysis. The subsample that was selected for the present study consisted of youth with current autism, measured by a question asking if the child currently had autism, ASD, Asperger's disorder, or PDD.
Participants
Sample characteristics are included in Table 1. The total number of youths included in this analysis was 4245. Of the sample, 50.6% were white, 41.6% were diagnosed between ages 1 and 3, and 46.4% were rated as having mild autism. The age of youth included in the sample was within the range of 5–17, with a mean age of 11. The median age of autism diagnosis was 5 years old. The multiracial/other category consisted of races collapsed into one due to limited sample size, and included 160 Asian, 35 American Indian, Alaska Native American, Native Hawaiian, or Other Pacific Islander youth, and 315 youth who were of two or more races. We recognize that this group is heterogeneous and that such categorization may obscure important subgroup differences. The Black, White, and Multiracial/other categories consist of non-Hispanic youth and will henceforth be referred to as such. To provide additional context for the age of autism diagnosis, we examined the age distribution at the time of survey completion across racial/ethnic groups. Age was categorized into three brackets (coded 1 through 4): 1 = 0–5 years, 2 = 6–11 and 3 = 12–17 years. A chi-square test indicated that the distribution of age varied significantly by race/ethnicity (χ² (12) = 25.22, p = .0138), with some groups having higher representation in younger or older age bands.
Demographic Characteristics Among Youth with Current Autism, Age 5–17 (N = 4245).
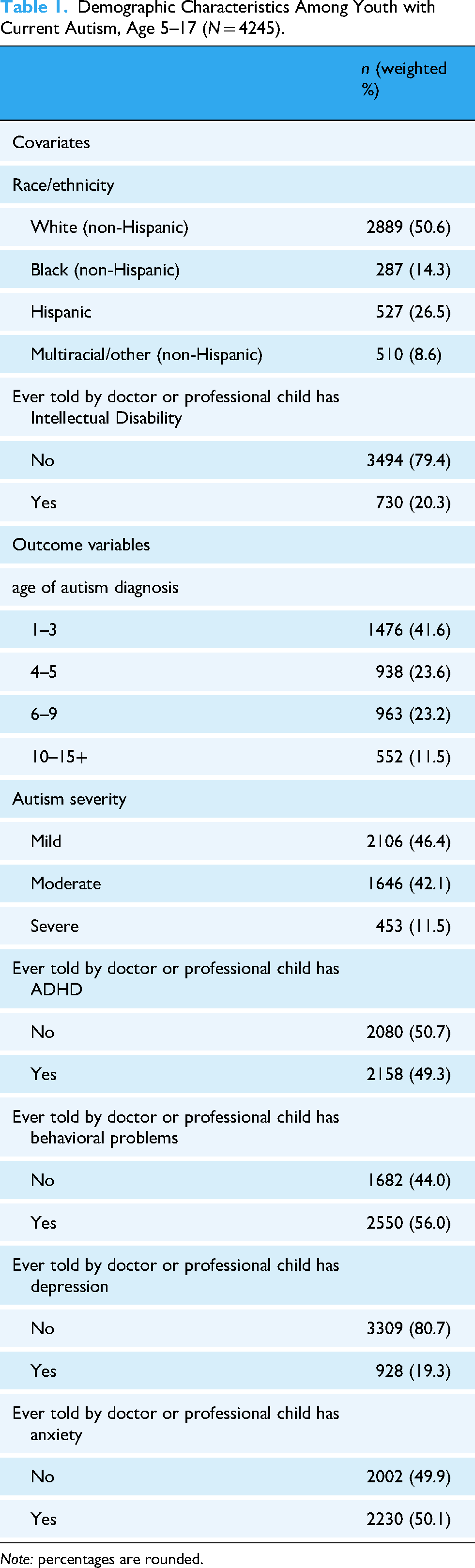
Note: percentages are rounded.
Analytic Plan
Several variables of interest were first subjected to data manipulation through recoding in the present analysis. Analyses were conducted using Stata 9.4 software (Copyright © [2023] SAS Institute Inc). The covariate of race/ethnicity was constructed by determining which children were of Hispanic, Latino, or Spanish origin, and a separate category of Hispanic across all races was developed. The other racial categories were White, Black, and Multiracial/other, the latter consisting of Asian, American Indian, Alaska Native American, Native Hawaiian or Other Pacific Islander, and children of two or more races. The covariate ID was measured with a binary question of “Has a doctor, other health care provider or educator ever told you that this child has ID (formerly known as mental retardation)?” Examples of educators are teachers and school nurses with binary responses of yes or no. Age of diagnosis, the first outcome variable, was measured using the survey question, “How old was this child when a doctor or other health care provider first told you that they had autism, ASD, Asperger's disorder, or PDD?.” Ages were divided into four categories representing developmental stages: 1–3 being infancy–toddlerhood, 4–5 school entry age, 6–9 middle childhood, and 10–15+ adolescence. The second outcome variable, autism severity, was rated as mild, moderate, or severe based on caregiver reports. Two multivariable multinomial logistic regressions with sampling weights were used to test the first research question of the predictor variables of race/ethnicity and ID on the outcome variables of the age of diagnosis and autism severity. To address the second research question, separate multivariable regression models were conducted for each of the following binary outcome variables: whether a healthcare provider had ever told the caregiver that the child had (1) ADHD, (2) anxiety, or (3) depression. These conditions were analyzed individually to preserve the distinct diagnostic profiles and behavioral presentations of each. A binary question also assessed behavior problems, but an educator was included as a possible source of information on who told the caregiver. Before conducting the logistic regressions, chi-square tests were run to test the bivariate relationships between the variables of interest. Listwise deletion was used to address missing data.
Results
A preliminary analysis was conducted to determine if youth of color were more likely to ever be diagnosed with ID when compared to White youth. Results of this binary logistic regression showed that Black (OR: 2.10, CI [1.327–3.332]) and Hispanic youth (OR: 2.14, CI [1.244–3.691]) were over twice as likely to ever be diagnosed with ID. Table 2 includes the results of the analysis to answer Part 1 of the first research question: an analysis of race and ID on the age of autism diagnosis. Race/ethnicity and an ID diagnosis were significant predictors in the age of autism diagnosis (ages 1–3, 4–5, 6–9, and 10–15+). Multiracial/other youth had lower odds than White youth of being diagnosed between ages 6–9 (OR: .53, CI [0.341−0.825]) and age 10–15+ (OR: .422, CI [0.245–0.728]) compared to being diagnosed between ages 1 and 3. Hispanic youth had lower odds than White youth to be diagnosed between ages 6–9 (OR 55, CI: [0.332–0.921]) than diagnosed between ages 1 and 3. Black youth had lower odds than White youth to be diagnosed between ages 10–15+ (OR: .523, CI [0.276–0.990]). Across the entire sample, youth with a diagnosis of ID had lower odds of being diagnosed with autism between ages 6 and 9 (OR: 0.59, CI [0.360–0.958]) and between ages 10–15 (OR: 0.28, CI [0.148–0.530]) than between ages 1 and 3, compared to youth without ID, controlling for race/ethnicity.
Autism Age of Diagnosis by Race/Ethnicity and Intellectual Disability.
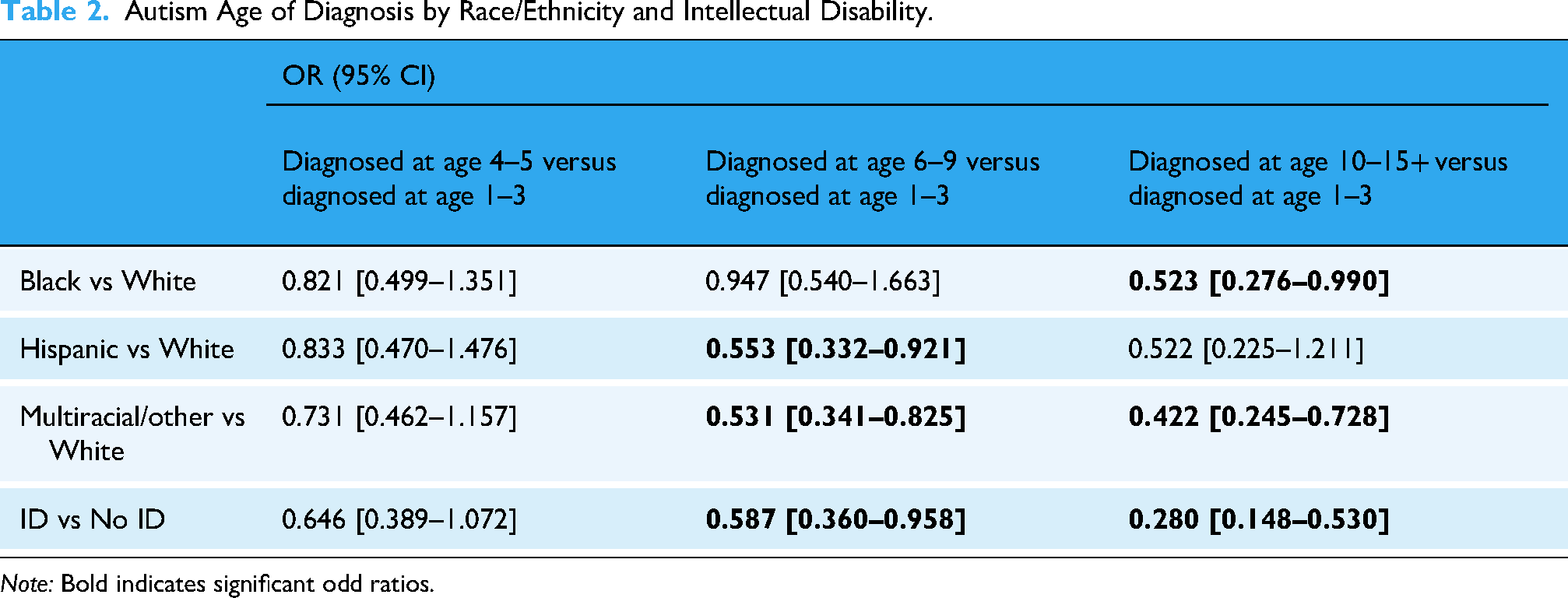
Note: Bold indicates significant odd ratios.
Table 3 includes the results of Part 2 of the first research question: an analysis of race, ID, and rating of autism severity. Race/ethnicity and ID were also significant predictors of autism severity rating. Black youth, compared to White youth, had higher odds of being rated as moderate (OR: 2.21, CI [1.415–3.449]) and severe (OR: 4.05, CI [2.153–7.620]) compared to mild. Multiracial/other youth had higher odds of being rated as moderate (OR: 1.62, CI [1.119–2.357]) compared to mild. Finally, Youth with ID had higher odds of being rated as moderate (OR: 3.30, CI [2.095–5.192]) and severe (OR: 11.43, CI [6.605–19.795]) autism compared to youth without ID.
Autism Severity by Race/Ethnicity and Intellectual Disability.

Note: Bold indicates significant odd ratios.
Table 4 includes the results of the second research question: an analysis of race, ID, and cooccurring conditions. For ADHD, race/ethnicity was a significant predictor for the multiracial/other group, with this group having lower odds of being told they have ADHD compared to White youth (OR: 0.61, CI [0.439–0.858]). For behavior problems, there were no racial/ethnic differences; however, youth with ID had higher odds of being told that they have behavior or conduct problems (OR: 2.37, CI [1.570–3.577]). There were no racial/ethnic differences or differences based on having an ID for depression. However, Black youth had lower odds of being diagnosed with anxiety than White youth (OR: 0.446, CI [0.294–0.677]) and multiracial/other youth (OR: 0.533, CI [0.381–0.745]). There were no differences based on having an ID.
Internalizing and Externalizing Conditions by Race/ Ethnicity and Intellectual Disability.

Note: Bold indicates significant odd ratios.
Discussion
This study aimed to explore how race/ethnicity and co-occurring ID influence age of autism diagnosis, severity, and cooccurring conditions, it aligns with findings from previous studies that autism with cooccurring ID has higher odds of being rated as severe as opposed to mild and moderate, and higher odds of behavior problems (Ben Itzchak et al., 2008; Mayes & Calhoun, 2011). The results of this analysis add to the current literature by showing that when accounting for ID, Black and multiracial/other youth had higher odds of being diagnosed as moderate than mild. Further, Black youth had four times higher odds of being reported by parents as having autism rated as severe when compared to White youth. This may be due to several reasons. First, Black parents may rate their child as more severe due to the accompanying stigma and shame impacting perceptions (Dababnah et al., 2018; Rivera-Figueroa et al., 2022). One explanation for the higher caregiver-reported severity among Black youth may be related to how autism is clinically framed during diagnosis. Black children with autism may be more likely to be identified by clinicians when they also have cooccurring ID, a pattern supported by our findings and previous research (Maenner et al., 2023). If caregivers are introduced to the autism diagnosis alongside an ID diagnosis, this combined framing may influence their perception of the condition as more serious or disabling. Additionally, caregiver may interpret the label of ID as indicating greater developmental challenges overall, which may affect their interpretation of severity. This aligns with previous research that shows Black youth are significantly less likely to engage in subspecialty visits, including within the psychological/psychiatric domains (Broder-Fingert et al., 2013). This finding may reveal gaps in knowledge or access to mental health support. Our findings indicate later autism diagnosis among non-White youth with cooccurring ID may reflect a complex interplay of developmental, social, and structural factors. During adolescence, youth are increasingly engaged in identity development and may become more aware of both racialized and behavioral differences from peers (Stewart et al., 2006; Umaña-Taylor et al., 2014). For non-White adolescents, these differences may be attributed by themselves or by others (e.g. teachers, caregivers) to racial, cultural, or personality traits rather than neurodivergence (Turnock et al., 2022; Williams et al., 2022). Additionally, adolescents from marginalized racial/ethnic backgrounds may engage in impression management or camouflage behaviors to avoid further stigmatization, making it more difficult for researchers to detect autistic traits (Cage & Troxell-Whitman, 2019; Shtayermman, 2009; Stewart et al., 2006; Williams et al., 2022). These intersectional dynamics may delay identification and diagnosis, particularly among those without ID who may already present with less obvious support needs. In addition to individual-level factors such as impression management or camouflaging, broader systemic barriers may also contribute to delayed or missed autism diagnosis among minoritized adolescents. Research has shown that Black and other non-White youth with behavioral differences are more likely to be misdiagnosed with externalizing conditions (e.g. conduct disorder or oppositional defiant disorder) or internalizing disorders (e.g. anxiety, depression) rather than being evaluated for autism or other neurodevelopmental differences (Emerson et al., 2016; Lauritsen, 2013). This phenomenon, often referred to as diagnostic overshadowing, reflects clinical bias in which mental health or behavioral challenges are foregrounded, potentially obscuring underlying neurodevelopmental conditions (Berg et al., 2018). Moreover, existing disparities in access to mental health services, coupled with stigma and mistrust of medical institutions, may further reduce the likelihood of appropriate evaluation for non-White adolescents.
Strengths and Limitations
Two strengths of this study are that it uniquely addresses the influence of race/ethnicity, ID, and autism to add to the current literature. Also, a nationally representative data set that included data across 5 years was used to enhance the robustness of statistical analysis that can be conducted on a sample of school-aged youth with autism. The use of logistic regression helps quantify the differences that are present between whites and youth of color. However, some limitations should be acknowledged. First, some research demonstrates that ID does not always lead to an earlier diagnosis, with moderate cases being diagnosed as early as possible. Moderate cases of autism have been found to be linked with an earlier diagnosis of autism than severe or mild cases (Lauritsen, 2013). This may be due to difficulty in discerning when autism is also present with ID, since both conditions are associated with developmental delays in social functioning. The diagnosis of ID within this sample of youth with autism is lower than national estimates of youth with an autism cooccurring ID. This sample had a weighted percentage of cooccurring ID at 20%, whereas national estimates are over 30% (Baio et al., 2018; Maenner et al., 2023). This means that this sample may not have adequately captured the impact of cooccurring ID on the outcome variables. Further, autism is known to have a distribution of cognitive abilities. As a secondary data set, the current analysis did not capture whether disparities are present across cognitive ability levels, such as borderline intellectual functioning or above-average IQ. The responses to the included predictors were based on parent reports, which are susceptible to recall bias. In addition, the severity variable was based on the caregiver's report of whether their child's condition was mild, moderate, or severe. While this approach reflects caregiver perceptions, it does not rely on a standardized or clinician-administered severity scale. The subjectivity may be shaped by contextual factors such as stress, socioeconomic status, and access to mental health services, which overall limit the comparability across groups. Finally, the racial category of multiracial/other is heterogeneous due to the category collapsing to account for small cell counts. Even with these limitations in mind, the findings of this study provide added perspective on racial differences in autism prevalence and cooccurring internalizing and externalizing conditions.
Implications for Research and Practice
A notable finding of this study is that youth within the Black and Multiracial/Other categories had lower odds than White youth of being diagnosed during adolescence (ages 10–15+). Further, Hispanic youth had lower odds than White youth of being diagnosed during middle childhood (ages 6–9) compared to infant–toddlerhood (ages 1–3). A preliminary analysis in this study demonstrated that Black and Hispanic youth are more likely than White youth to be diagnosed with cooccurring ID, which is concurrent with existing research (Maenner et al., 2023). These findings provide initial support for diagnostic gaps experienced by some youth of color, such that when accounting for ID, they may have lower odds of being identified in middle childhood and adolescence.
Fewer youth of color being diagnosed at later ages may generally point to diagnostic gaps being filled in terms of early intervention. However, it presents a concern for youth with lower support needs presentations that may present with symptoms when they are older. While youth with lower support needs are often diagnosed at later ages, the results of this study provide preliminary evidence that youth of color may be underidentified at later ages. This is a critical period of diagnosis due to increased social demands during the transition into middle and high school that may lead to autism symptoms becoming more apparent (Berg et al., 2018). These findings suggest room for missed diagnoses of youth of color without ID, which can lead to psychosocial difficulties impacting overall well-being due to a lack of adequate interventions and support (Joseph, 2022). Understanding contributing factors and consequences of racial/ethnic disparities in autism diagnostic characteristics carries important implications for clinical research and autism identification and treatment practices. The negative impact of differences in the quality of family-healthcare relationships, lower reporting of autism-related developmental concerns, and inconsistent use of developmental screeners unduly impact access to equitable care for youth of color (Collins et al., 2017). In addition, socioeconomic factors present a salient element as the burden of poverty is disproportionately experienced by families of color.
Access to early intervention has been widely identified as a priority for global research in developmental disability, improving several outcomes for children with autism (Sapiets et al., 2021). Early intervention's positive impact on child development includes improvements in adaptive skills, sleep, parental health, and self-efficacy (Landa, 2018). There has been evidence that indicates that young children with autism benefit from direct intervention as well as from parents who have received coaching and support to implement child-responsiveness engagement strategies (Dawson et al., 2010). Training and guidance provided to parents can enable them to support their children's development within their everyday routines and activities (Dawson et al., 2010; Jeong et al., 2021). This research supports the idea that the combination of interventions implemented by both the parent and clinician is important to promoting developmental growth (Development et al., 2000). These positive outcomes are made possible when early diagnosis is achieved. Despite the evidence supporting the effectiveness of early intervention, research suggests that racial minorities often face barriers that hinder their access to these services. Limited availability and reduced utilization of early intervention services within marginalized communities can result in late diagnosis and delayed treatment for children with autism. Consequently, parents from these communities often struggle to provide optimal support and intervention for their children (Rivera-Figueroa et al., 2022). Without timely and appropriate intervention, children from marginalized communities are left to experience the full extent of their condition with more significant challenges in their developmental progress and may not benefit fully from available resources. These implications of late diagnosis extend to impacting parents’ well-being and self-efficacy to fully support their children's development. These disparities in access to timely diagnosis create a cycle of disproportionate care for racial minorities. In addition, future research with larger sample sizes should disaggregate the Multiracial/Other category to better capture the unique diagnostic experiences of distinct racial and ethnic groups.
Conclusion
The results of this study suggest that the amount of Black and Hispanic youth identified as having a cooccurring ID is significantly higher than White youth, which may mean cases with lower support needs or no cognitive impairment are underdiagnosed. This aligns with the findings of a prevalence study by Shenouda and researchers (Shenouda et al., 2023). These findings point to the need for continued research to further understand how the presence or absence of ID may impact diagnostic characteristics. Additionally, a critical examination of how socioeconomic factors can contribute to the observed disparities is necessary to promote equity in early identification and access to intervention services for youth of color. Efforts should be directed toward increasing awareness and knowledge about ASD within these communities, reducing cultural and linguistic barriers to diagnosis, and expanding the availability of culturally sensitive and community-based early intervention programs. By addressing these systemic challenges, we can ensure that all children, regardless of their racial or ethnic background, have equal opportunities to receive timely diagnoses and access the early intervention services that can significantly impact their developmental trajectories. Moreover, these barriers are not unique to autism but reflect a broader pattern of systemic inequities in mental health and developmental care pathways. Future research should continue to investigate how structural racism, access limitation, and provider bias intersect with adolescent development to shape diagnostic trajectories for autistic youth of color. In addition, providing support and resources for parents within marginalized communities is essential to alleviate their burden and enhance their ability to actively engage in their children's development.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330251353629 - Supplemental material for Race/Ethnicity, Intellectual Disability, and Diagnostic Characteristics Among School-Aged Youth with Autism: A Cross-Sectional Study
Supplemental material, sj-docx-1-ndy-10.1177_27546330251353629 for Race/Ethnicity, Intellectual Disability, and Diagnostic Characteristics Among School-Aged Youth with Autism: A Cross-Sectional Study by Naomi M Ruffin and Philip Sanusi in Neurodiversity
Footnotes
Ethics Considerations
The present study was conducted using deidentified, publicly available data sets which under U.S. federal regulations for human subjects (45 CFR Part 46) does not require IRB review.
Author Contributions
All authors contributed to the study conception. Naomi Ruffin and Philip Sanusi performed material preparation, data collection, and analysis. The first draft of the manuscript was written by Naomi Ruffin, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The analysis of secondary data that was conducted in the present study was conducted with data collected from the U.S. Census Bureau website. ![]()
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.