
Abstract
The specific learning difficulties (SpLD) network (SLDN) was established in 2022 to bring together UK researchers and stakeholders interested in SpLDs to better integrate research across different areas and to agree on research priorities. It was vital to include the views and experiences of people (and carers of children and young people) with SpLDs (here defined as dyslexia, dyscalculia, and dysgraphia) as part of the research priority-setting process. In this study, we analysed data from 145 participants (82 carers of a child or young person with an SpLD and 63 adults with an SpLD) from the UK (primary difficulty: 119 dyslexia, 14 dyscalculia, and 12 dysgraphia) on various issues around identification, labelling, support, mental health, and research priorities. Here, we present descriptive statistics separately for each SpLD where sample sizes permit. While not a population-representative survey, some key findings include: the high number of co-occurring SpLDs, high co-occurrence with other developmental traits, and high prevalence of mental health issues. Key priorities were around earlier identification and best ways to support SpLDs, and additionally, for dyscalculia, around increasing awareness. Suggestions for the next steps in the research priority-setting process include research based on co-production with people with lived experience of SpLD.
Lay Abstract
The specific learning difficulties (SpLDs) network (SLDN) was established in 2022 to bring together UK researchers and stakeholders interested in SpLDs to better integrate research across different areas and to agree on research priorities. It was vital to include the views and experiences of people (and carers of children and young people) with SpLDs (here defined as dyslexia, dyscalculia, and dysgraphia) as part of the research priority-setting process. In this study, we analysed data from 145 participants (82 carers of a child or young person with an SpLD and 63 adults with an SpLD) from the UK (primary difficulty: 119 dyslexia, 14 dyscalculia, and 12 dysgraphia) on various issues around identification, labelling, support, mental health, and research priorities. Here, we present descriptive statistics separately for each SpLD where sample sizes permit. While not a population-representative survey, some key findings include: the high number of co-occurring SpLDs, high co-occurrence with other developmental traits, and high prevalence of mental health issues. Key priorities were around earlier identification and best ways to support SpLDs, and additionally, for dyscalculia, around increasing awareness. Suggestions for the next steps in the research priority-setting process include research based on co-production with people with lived experience of SpLD.
There has been increased recognition of the importance of patient and public involvement in health and social care research, with UKRI committed to improved public involvement (https://www.ukri.org/news/shared-commitment-to-improve-public-involvement-in-research/). This participatory approach is valuable at all stages of research design, from formulating research questions themselves, to co-producing research designs, and disseminating research findings. The umbrella term, specific learning difficulties (SpLDs), maps onto the medicalised term specific learning disorder used in the DSM-5 (American Psychiatric Association & Association, 2013) where the deficit can be in reading (dyslexia), numeracy (dyscalculia), and writing (dysgraphia). However, this over-simplifies the nature of individuals’ skillsets, as boundaries between these specific difficulties are not clear cut, and biological, psychological, and social factors impact on functioning (Wissell et al., 2025). SpLDs are more relevant to the educational rather than medical context, with participatory research in the field of education often focussing on teachers and specific demographic groups of parents (Honingh et al., 2020). There has been relatively less involvement of people with lived experience of SpLDs in research co-production although we expect this to gain traction as neurodivergent people's voices and lived experience are increasingly viewed as valuable sources of insight (Sewell, 2022). Our aim then was to survey neurodivergent adults (and carers of children or a young person with SpLD neurotypes) on issues and views that could shape the direction of future research in the area of SpLDs.
The concept of SpLDs has evolved from a medical model in which weaknesses in these narrow academic skills were considered as impairments based on biological and cognitive causes, similar to the way in which neurodevelopmental conditions are considered to have causes in early brain development with effects on behaviour (Bourgeron, 2015). But the view is increasingly aligning with a social model of disability (Oliver, 2013) wherein the educational and social context are the key definers of what constitutes an SpLD and influence the negative assumptions people hold towards children and adults with SpLD neurotypes (see Riddick, 2001 for this perspective with regard to dyslexia). Within this framework, the importance of lived experience is especially valuable in helping to identify the socio-environmental limitations that make SpLDs disabling, and conversely, the educational and occupational support that enable people with SpLDs to flourish. Deficit-based conceptions of SpLD are often focused on specific cognitive processes with a view to intervening in these to improve achievement outcomes (Grigorenko et al., 2020). While intervention will assist some, for others, meaningful support can come through changes in societal (educational and occupational) and cultural factors to provide an inclusive learning/work environment for all.
Of the three SpLDs considered here, dyslexia is the most prevalent with the British Dyslexia Association citing a 10% prevalence in the UK (https://www.bdadyslexia.org.uk/dyslexia). A systematic review and meta-analysis of dyslexia prevalence in primary school children from middle- and high-income countries reported a worldwide prevalence of 7.1%, with a significantly higher rate in boys than girls (Yang et al., 2022). Difficulties with reading and spelling can negatively affect a child's self-esteem (Wilmot et al., 2023b) and can have a significant impact on educational and socio-economic outcomes (e.g. lower income; McLaughlin et al., 2012). There is much greater identification and support for dyslexia today than there was a generation ago (Kirby, 2020), and with the rapid advances in technology that can aid dyslexic learners (e.g. text to speech apps; Lerga et al., 2021; Svensson et al., 2021) there is a need to understand the current issues faced by adult dyslexics and carers of a child or young person with dyslexia today. Various recent studies have sampled stakeholder views on narrow issues, for instance, a Delphi study of parents on the barriers to dyslexia identification (Harding et al., 2023) and children and parents’ views around school struggles, self-esteem, and mental health (Wilmot et al., 2023b), but these were small scale and qualitative in nature. A priority-setting exercise in Scotland of stakeholders including those with lived experience, educational practitioners, and from health, social work, and charities, identified research questions that should be prioritised in the general field of learning difficulties (Ai Keow et al., 2019). However, the participants in this engagement exercise had a large range of neurodevelopmental differences that were not specific to reading and spelling. Dyslexia was represented, but an equally large proportion of participants reported on learning difficulties related to autism and attention deficit hyperactivity disorder (ADHD); there was minimal reporting of children and young people with dyscalculia and dysgraphia.
There is less public awareness of dyscalculia compared to dyslexia, despite only a slightly lower prevalence across the lifespan (3%–7%) (Haberstroh & Schulte-Körne, 2019). As a consequence, underlying numeracy difficulties often go unnoticed, which can result in socio-emotional problems and lower academic attainment (Ohanele, 2023). A systematic literature review from 2015 to 2016 showed that dyscalculia is equally prevalent across sexes and that it often co-occurs with dyslexia (odds ratio [OR] of 12.25) (Haberstroh & Schulte-Körne, 2019). Of 2421 Northern Irish primary school children, 5.7% were identified as having dyscalculia, with around half of them having a language/communication difficulty, and a smaller proportion with additional neurodivergence and/or socio-emotional difficulties (Morsanyi et al., 2018). With regard to research priority setting in the area of dyscalculia, a relevant collaboration of 16 researchers with expertise in education, psychology, and neuroscience produced a list of 26 research priority questions for mathematical cognition (Alcock et al., 2016). There were six broad themes including the nature of mathematical thinking, identifying predictors and processes related to the acquisition of maths skills, supporting these skills, developmental tracking of competencies, interventions, and measurement. The authors themselves recognised that there was little breadth in the experience and knowledge of their participants (all researchers in narrow disciplines). It is therefore important to include a lived experience perspective in any research priority-setting exercise, including valuable insight from those whose lives are directly affected by research-informed changes to education policy.
Dysgraphia is little recognised and researched, but its prevalence in the USA has been estimated at 6.9% or 14.7% depending on the criterion used, with boys being 2 to 3 times more likely than girls to be classified as having dysgraphia (Katusic et al., 2009). Furthermore, 75% of those with written language difficulties also had reading difficulties. A similar prevalence has been reported in Norway (13% at the end of grade 5; Karlsdottir & Stefansson, 2002), South India (12.5% in 8–11-year olds; Mogasale et al., 2012), but lower in Turkey (1.8% in 7–11-year-olds; Büber et al., 2020). Besides higher co-occurrence with dyslexia, developmental dysgraphia also frequently co-occurs with developmental co-ordination disorder, attention deficit hyperactivity disorder, autism, and developmental language disorder (O’Donnell & Colvin, 2019). O’Donnell and Colvin (2019) interpret this overlap through a model of neuropsychological components including graphomotor skills, phonological processing/auditory working memory, semantics and syntax, pragmatics, and executive function which are shared to different degrees across the developmental traits. A scoping review of childhood (5–15 years) dysgraphia research focussed on children, carers, and educators found that of 77 studies published between 2015 and 2021, 87% pertained to children, with few focussed on the carers or teachers as participants (Kalenjuk et al., 2022). Most of the studies took a quantitative or mixed methods approach, and the main themes were around difficulties with handwriting and spelling, co-occurrence with other neurodivergence, and the use of new technology. Whether those with lived experience of dysgraphia would identify the same research topics as the worthiest of study is unknown.
The research aim of our study is to understand the views of those with direct experience of an SpLD, whether they are adult reporting on themselves or on a child or young person in their care with an SpLD. We ask a wide range of questions, both quantitative and qualitative in nature, mapping demographics, views around labelling and alignment with the neurodiversity framework, identification, support, challenges, co-occurring traits including mental health outcomes, family risk factors (i.e. genetic risk which has been a controversial research topic within the autistic community; Sanderson, 2021), and research priorities. While there are recommendations around the best age to assess for SpLDs there is no recent UK population-level data to indicate when this actually occurs. Age of identification arguably has relevance to both educational and emotional outcomes. Deficit-based models of SpLDs have predominantly focussed on cognitive and educational correlates (Grigorenko et al., 2020), but given significant increases in the population prevalence of mental health traits like depression (Moreno-Agostino et al., 2021), we deemed it vital to sample these in our study. For developmental dyslexia, reviews have highlighted the increased presence of internalising and externalising behaviours (Wilmot et al., 2023a) and associated emotional corelates (Livingston et al., 2018). Given the expected mechanisms for these associations, poor mental health is also likely to occur in dyscalculia and dysgraphia. Neurodiversity, a term that is primarily associated with autism (Kapp et al., 2013; Pellicano & den Houting, 2022) is a paradigm that recognises the natural variation in human brain function and emphasises differences in ways of thinking as positive (Alcorn et al., 2024). Behaviours that are not dominant in the population are classed as neurodivergent thus avoiding negative connotations associated with medical terms of disorder and impairment. We wished to assess how familiar our participants were with this term and whether they thought it relevant for SpLDs, and whether existing SpLD labels were acceptable. Our descriptive study (which was in no way hypothesis driven) was intended to inform the agenda of the specific learning difficulties network (SLDN) which is UK based and as such our participants were recruited from the UK. However, we expect that various findings will generalise to other countries, especially Western democracies with similar health and educational systems.
Methods
The online survey was designed by several of the study co-authors, one of whom was a carer of a neurodivergent young person with a SpLD (and also a speech and language Therapist with professional experience in supporting neurodivergent young people) and two principal investigators whose research expertise is in dyslexia. We are neuro-affirming in that we believe neurodivergent people should be included in any research about better representing and supporting their needs in society.
Thirty-eight questions were devised in line with the broad research aim of better understanding the lived experience of those with dyslexia, dyscalculia, and dysgraphia neurotypes. These questions tapped into SpLD identification/diagnosis, support, schooling, and views about the causes and language around SpLD. Demographic and health information was also requested so that altogether survey completion time was around 15 minutes. The questionnaire went through a number of revisions (for language use and content) based on feedback from several neurodivergent adults (dyslexic and ADHD) and from a mother of a young person with dyslexia. The survey was launched in June 2022 and ran until March 2023, with the link to the Qualtrics survey advertised on social media (e.g. X (then Twitter) and Facebook), various websites (SLDN, Dyslexia Scotland), the Edinburgh Learns newsletter (for headteacher distribution to schools), and via the University of Edinburgh's Volunteer Research Panel. Participation was voluntary with all responses optional, and information anonymised. A description of the study participants is given in the results. The research project was approved by the Philosophy, Psychology, and Language Sciences Ethics Committee (approval number 202-2122/2). Statistical analysis was done in R (R Core Team, 2021) using standard descriptive analysis packages.
Results
One hundred and sixty-six participants responded to having an SpLD, but of these, four did not answer more than a few questions, and 17 were not living in the UK, leaving an N of 145 for analysis. These included 78 participants from Scotland, 33 from England, and three from Wales with known locations. Sample characteristics are shown in Table 1, separately for participants with single and co-occurring SpLDs. Of the 116 participants who provided demographic information, only three were not born in the UK and 14 reported speaking more than one language; six from 108 participants reported being mixed race, African, or Asian Arab. Co-occurrence of SpLDs with other developmental traits is common; in our sample, 51 reported one other co-occurring neurodivergence, 16 reported two, four reported three, and two reported four (Figure 1 shows the frequency and type of co-occurring trait by SpLD). A single question on the presence of mental health issues was answered by 137 participants with 43% reporting mental health issues; free text responses indicated that these were predominantly anxiety and/or depression (see Table 1 for breakdown by SpLD).

The Frequency of Co-Occurring Neurodevelopmental Traits Observed within the Different Specific Learning Difficulty (SpLD) Groups. The Number of Participants within each Category is Depicted within the Bars.
Descriptive Statistics for Specific Learning Difficulty (SpLD) Type by Reporting Status (Self vs. Carer), Sex, School Type, and the Presence of Mental Health Problems.
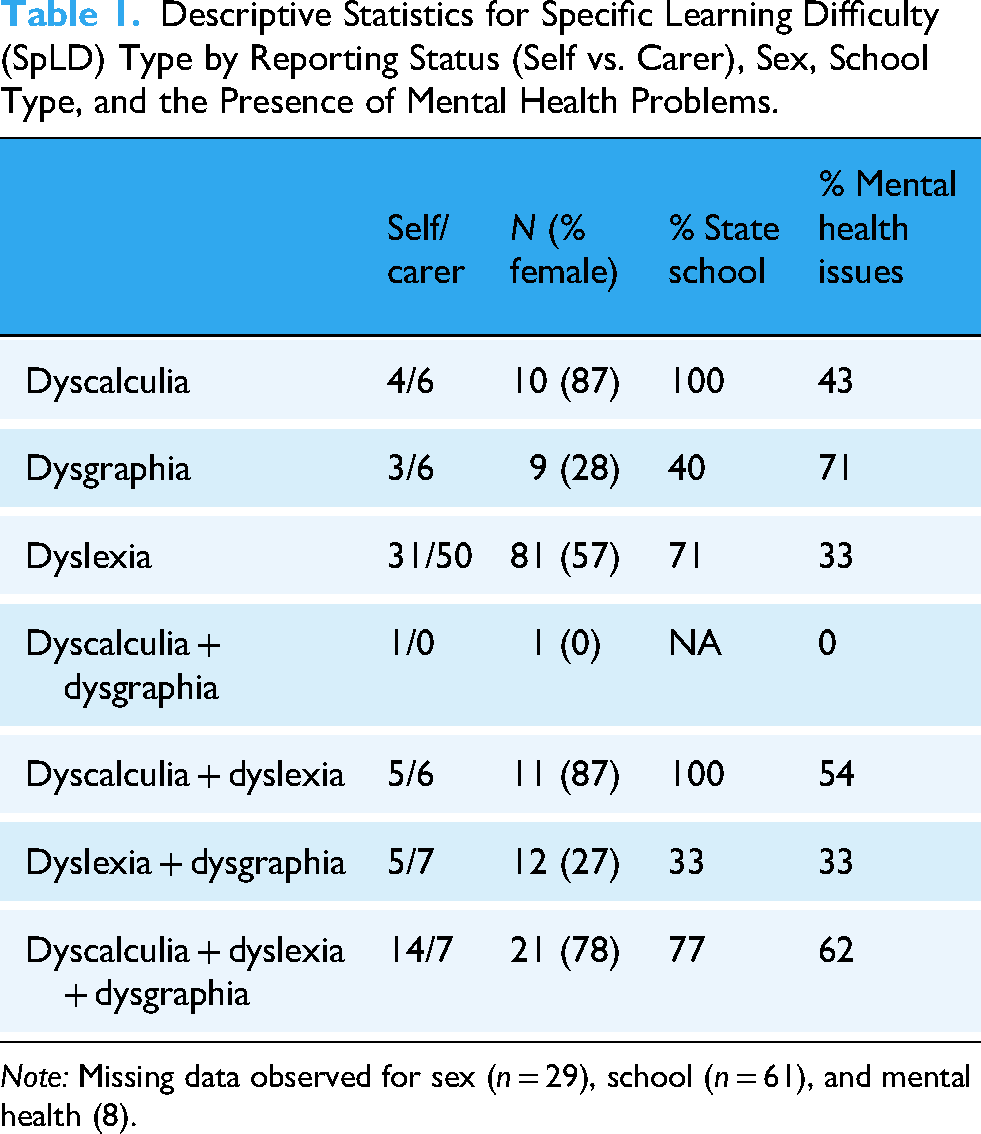
Note: Missing data observed for sex (n = 29), school (n = 61), and mental health (8).
In terms of who was involved in the identification of the SpLD, nursery/school was the major source for dyslexia, and a psychologist for dyscalculia and dysgraphia. Figure 2 shows the breakdown of identification sources separately by primary SpLD, with ‘Other’ responses mostly noting educational psychologists and private/specialist assessors. Table 2 shows the age of identification/diagnosis of the primary SpLD separately by self-report and carer report (of a child/young person). The median age was higher for dyscalculia identification than dysgraphia or dyslexia for both self and carer reports.
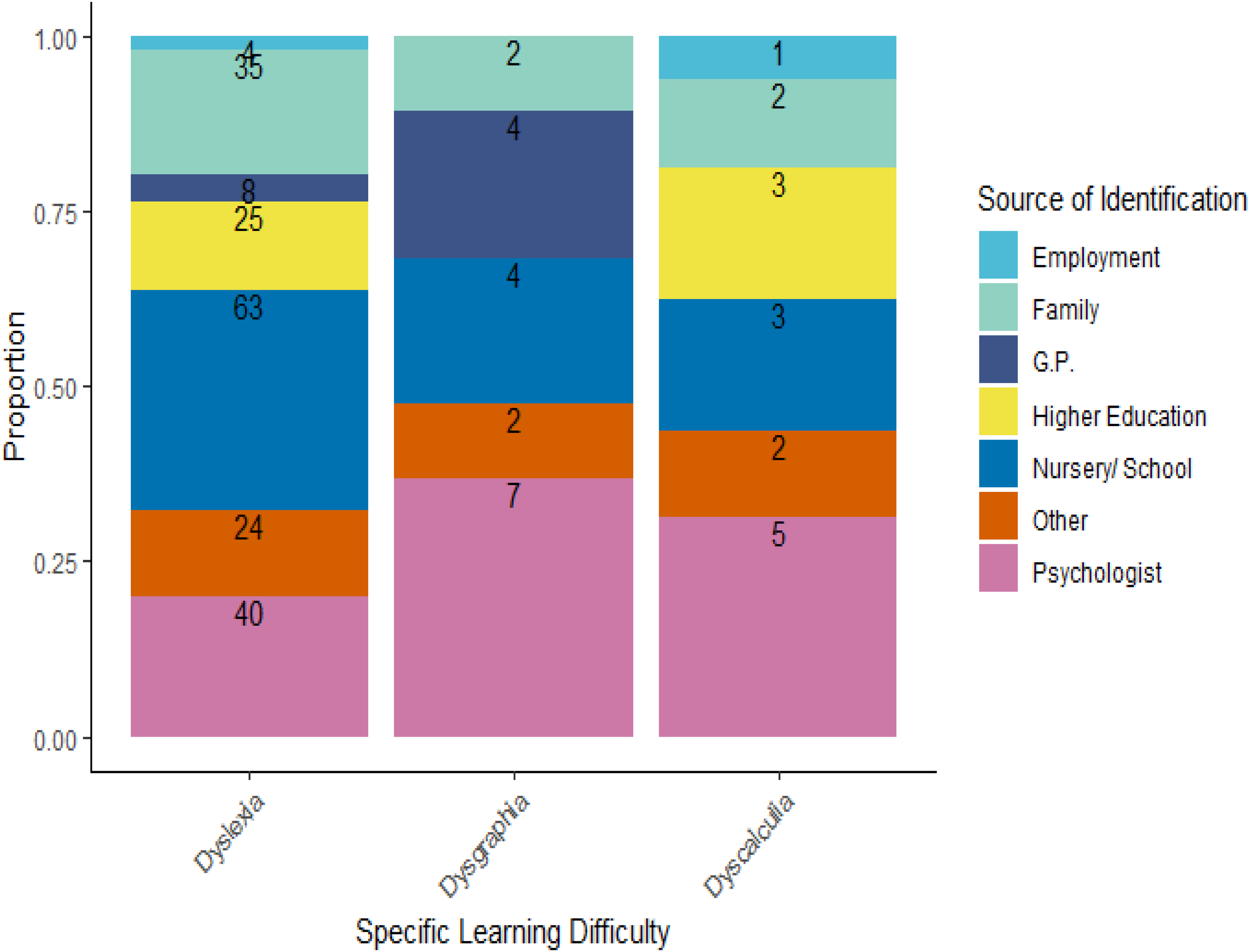
Distribution of Who was Involved in Identifying the Specific Learning Difficulty (SpLD). The Number of Participants Endorsing each Source Category is Indicated within the Bar. Note that Multiple Sources could be Endorsed.
Mean and Median Age of Identification/Diagnosis of the Primary Specific Learning Difficulty (SpLD) (Dyscalculia, Dysgraphia, and Dyslexia).

A question on the difficulty of getting identified/diagnosed with an SpLD was rated from ‘very easy’ to ‘very difficult’ on a 5-point scale. Fourteen percent of participants found formal identification ‘very easy’ or ‘easy’, 29% found it ‘somewhat easy’, 50% found it ‘somewhat difficult’ or ‘difficult’, and 22% found it ‘very difficult’. A chi-squared test with simulated p-values (due to low case membership for some categories) showed that there was no difference between self-reporting and reporting on a child/young person (p = 0.88). Given that the mean age of SpLD identification was 25 years in the self-report group versus 9 years in the carer group this suggested that there was no change over a generation in ease of being formally identified with an SpLD. Additionally, there was no significant difference in the responses between participants in England and Scotland (chi-squared = 2.076, p = 0.84). Note that group sizes were too small to test for differences across SpLDs. For all types of SpLDs, the most frequent difficulty in getting identified was that the school did not provide the right help. Other highly endorsed difficulties included: no one taking them seriously, being too ashamed to seek help, and the high cost of diagnosis. When asked what more could have been done around identification/diagnosis, two main themes emerged in the free text responses: (a) more accessible assessment and support, particularly at an earlier age, and (b) more accurate knowledge around SpLDs for teachers and parents.
When considering the primary SpLD, 77% of those with dyscalculia and 75% of those with dysgraphia reported that it was ‘somewhat hard’ to ‘very hard’ (most endorsed the ‘very hard’ category) to get support following identification/diagnosis versus 59% reporting such difficulties for dyslexia (where fewer endorsed the ‘very hard’ category). There was no difference between adult self-reporting and reporting on a child/young person (chi-squared = 5.467, p = 0.35) on this question. The types of difficulties faced when trying to get support following identification/diagnosis are shown in Figure 3. The ‘Other’ free text comments could be grouped into three main themes with the most dominant being ‘no or inconsistent support being offered’, then ‘others lack of understanding/awareness of the learning difficulty’, and ‘no difficulties’. The type of support reported as most helpful to the participants is shown in Figure 4. For dyslexia, the greatest support was clearly from technology and educational/employment support. With more varied support being reported for dyscalculia and dysgraphia. The free text of the ‘Other’ response mostly focussed on specific examples of technological/school support (e.g. touch typing, laptop use, and extra time in exams) for dyslexia, online and self-support for dyscalculia, and a comment about general counselling or there being no support for dysgraphia.

The Types of Difficulties Encountered when Trying to Get Support Following a Specific Learning Difficulty (SpLD) Diagnosis. The Number of Participants Endorsing a Category is Shown within the Bar.
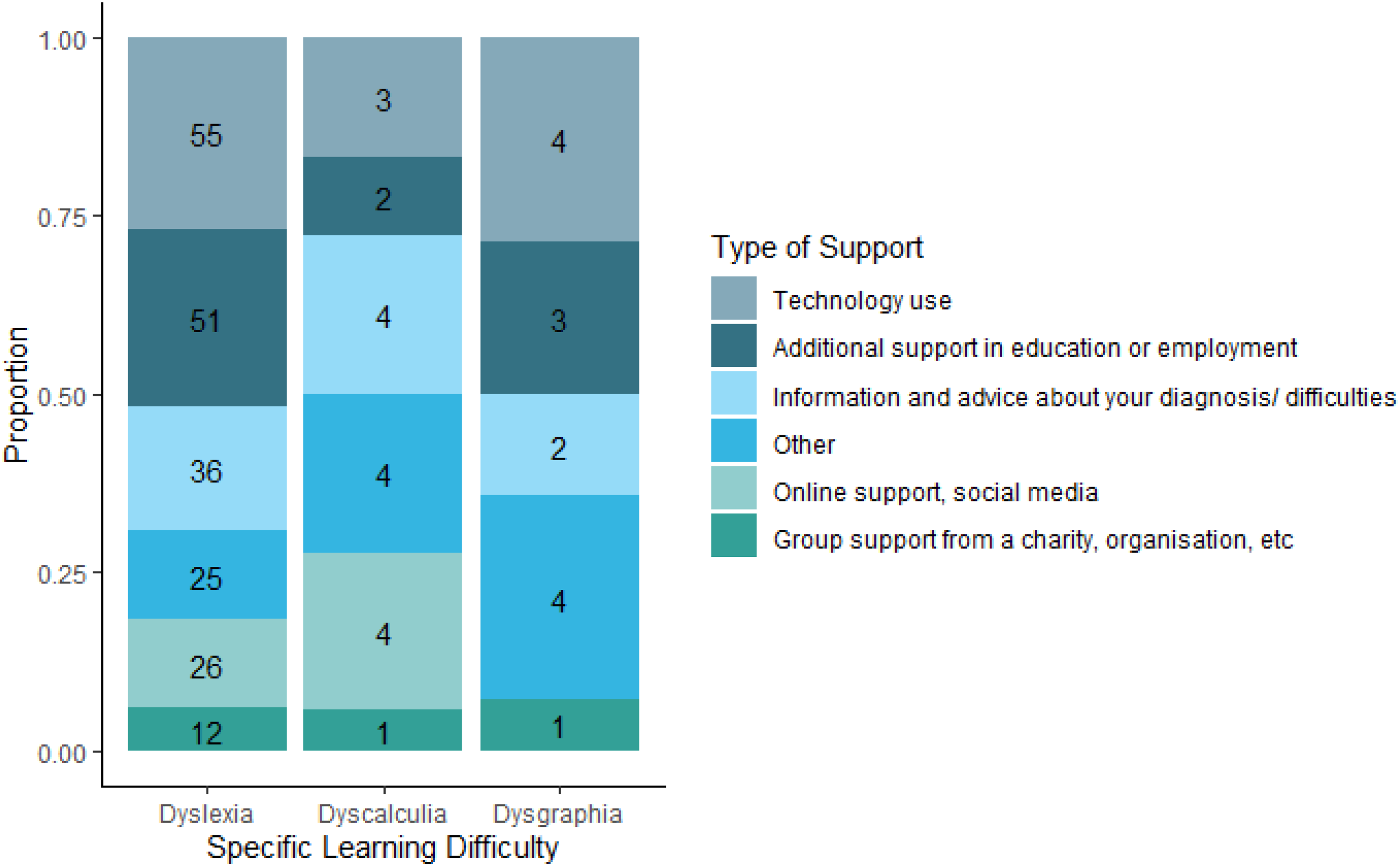
Distribution of the Type of Support Reported as Most Helpful for the Different Specific Learning Difficulties (SpLDs). The Number of Participants Endorsing each Category of Support is Shown within the Bar.
Of special interest to two of the authors who are geneticists, three questions around genetics were asked. The first asked about participants’ awareness of SpLDs being influenced by genes, the second around known family members who have an SpLD, and the third around whether they would want to know their own (or their child/young person's) genetic susceptibility to an SpLD. Figure 5 shows the responses to these separately by type of SpLD. There was overwhelming awareness of genetic inheritance for all SpLDs and reporting of family members with an SpLD. On whether they would like to know their own (or cared for person's) genetic predisposition to an SpLD, responses were mixed, with roughly equal numbers of participants answering yes and no for all SpLDs and a sizeable number not sure or requiring further information about this before making a decision for dyslexia and dysgraphia. No differences between adults self-reporting and reporting on a child/young person were observed for any of these questions (p > 0.05).

Responses to Questions About Genetic Predisposition to Specific Learning Difficulties (SpLDs). The Number of Participants Endorsing a Category is Shown within the Bar.
Three questions (Q1–Q3) were asked about terminology. Seventy-eight percent of 129 respondents were familiar with the term neurodiversity (Q1), with 66% agreeing that SpLDs should be talked about in terms of neurodiversity (Q2). The preferred word choice (disorder, difficulty, or difference; (Q3)) for those with dyslexia and dyscalculia was as a ‘learning difference’ (see Figure 6). In the free text ‘Other’ response there were comments that none were sufficient labels; that enabling focused language should be used (e.g. ‘supported learning’, ‘learning requirement’, and ‘diversely able’); and that there was a need to avoid negative connotations. Several dyslexic participants commented that the form of SpLD should be used, that is, ‘dyslexia’, and several participants (with dyslexia or dysgraphia as primary SpLD) preferred ‘disability’ as a label, one commenting that it gained them employment rights. No differences between adults self-reporting and reporting on a child/young person were observed for any of these questions (p > 0.05).

Word Choice Preference when Referring to Specific Learning Difficulties (SpLDs), Separately by Dyslexia, Dyscalculia, and Dysgraphia. The Number of Participants Endorsing a Category is Shown within the Bar.
The final survey question asked about research priorities (see Figure 7) and was answered by 114 participants (with multiple responses permitted). Participants reporting dyslexia or dysgraphia as the primary SpLD endorsed ‘earlier identification’ and ‘how to support’ as their two main priorities. Participants (or carers of a child/young person) with dyscalculia additionally endorsed ‘getting diagnosed’ and ‘raising awareness’ as equally important priorities. For all types of SpLD, the ‘causes of SpLD’ were less important. Four dyslexic responders gave ‘Other’ priorities which broadly aligned with ‘support’: ‘Recognition of where changes to teaching methods could benefit children with such difficulties without negatively impacting other children (or in some cases might actually benefit all children) to make inclusion easier for all’ and ‘coping mechanisms’; and ‘awareness’: ‘More awareness of learning difficulty that is caused by current educational practice. Society needs many different types of thinkers to be successful, we should embrace and encourage all neurotypes’ and ‘Helping people to make more of their specific skills and stop criticising them for their difficulties’.
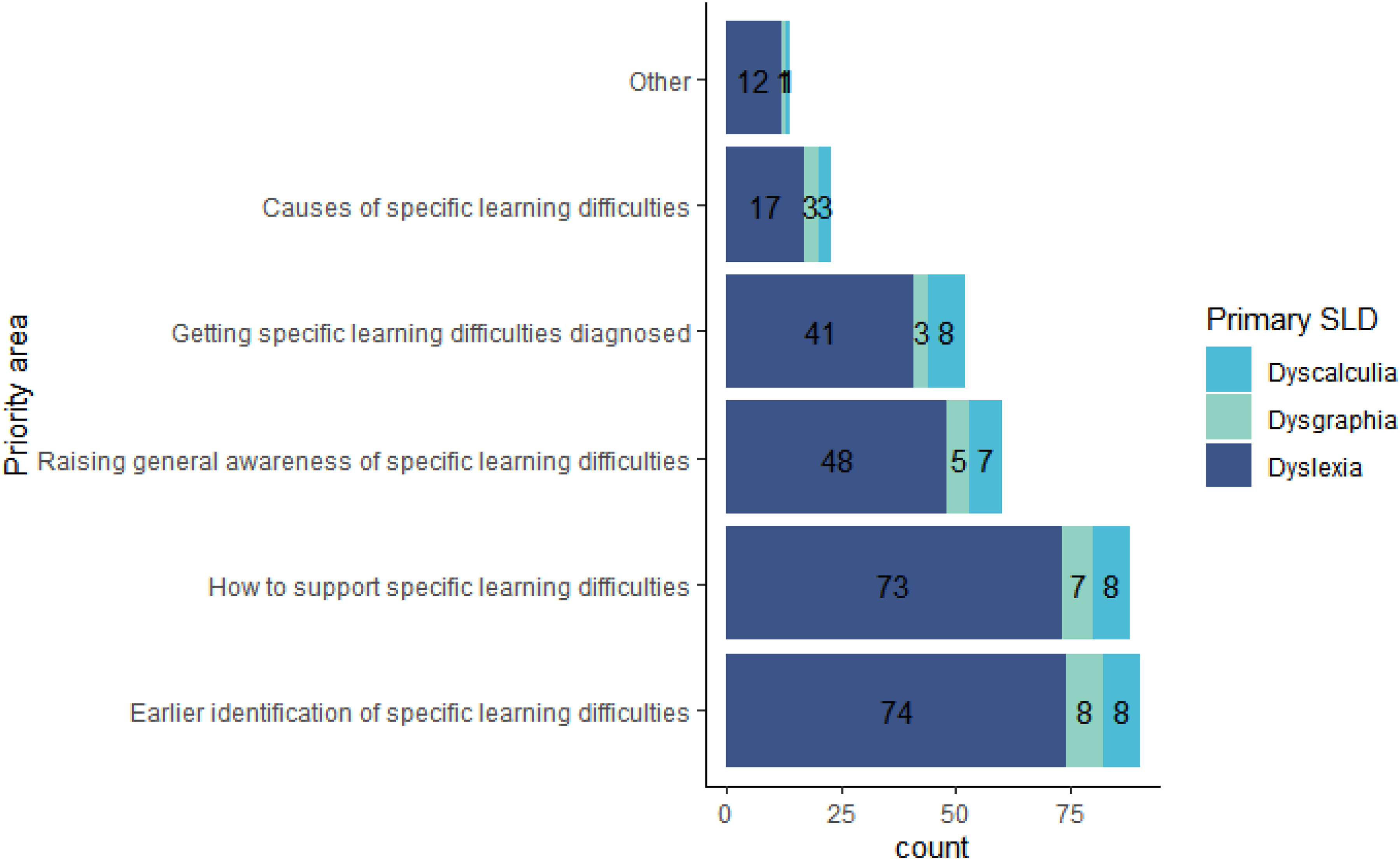
Endorsement of Research Priorities Separately by Specific Learning Difficulty (SpLD) (Dysgraphia, n=10; Dyscalculia, n=11; and Dyslexia, n=93). The Number of Participants Endorsing a Category is Shown within the Bar. Note that Multiple Categories could be Indicated.
Discussion
In line with the slightly higher reported population prevalence of dyslexia (∼10%) compared with dyscalculia (3%–7%) and dysgraphia (5%–10%) (Devillaine et al., 2021; Haberstroh & Schulte-Körne, 2019; Yang et al., 2022), and especially the greater awareness around it, the respondents in our survey primarily had dyslexia or cared for a child/young person with dyslexia. The findings, therefore, are more reliable for dyslexia, and in particular, for those without any co-occurring SpLD. Sample demographics also showed a bias towards female respondents, Scottish participants, monolinguals, and White British ethnicity which limits generalisability and potentially restricts the range of views. In sum, the responses indicated that improvements are needed in the areas of identification and support of SpLD, and research priorities in the field accordingly pertained to these areas. A worrying proportion of mental health issues were reported amongst those with all types of SpLD (especially dyscalculia and where it co-occurred with dysgraphia and dyslexia). The findings thus highlighted three key areas of importance that should be followed up with further public participation in research.
With regard to the participant demographics, there was greater representation of those who attended or whose child/young person attends a state versus private school although a significant number of participants did not report school status. Dyscalculia was being identified at a later age in both self and carer reports compared to dysgraphia and dyslexia. For children/young people, the reported median age of identification/diagnosis for dyscalculia was 14 years versus 8 years for dysgraphia and dyslexia. The later identification of dyscalculia is likely due to its lower awareness among educators (Van Herwegen et al., 2024) and general acceptance by the public that some people are just ‘bad at math’ (Numeracy, 2020). Our finding highlights a pressing need for better awareness of dyscalculia and tests that can identify the need for numeracy support at the primary school level. In England, a phonics screener is used to identify children at the end of the first year of primary school who may have difficulties with phonic decoding (https://www.gov.uk/education/phonics), a core feature of dyslexia but not its only indicator. The screener has shown validity against a range of standardised reading tests, but teachers trained in assessing/teaching phonics can identify children as well as the screener; supporting the argument that resources directed to teacher training is preferable given educators’ resistance to the screener's statutory use (Duff et al., 2015). A dyscalculia screener could be a good step to help earlier identification of children with numeracy difficulties (https://discovery.ucl.ac.uk/id/eprint/10158637/; Van Herwegen et al., 2022). But better teacher training around maths difficulties might also be sufficient to identify dyscalculia earlier. The ADD UP toolkit can assist parents and educators to spot dyscalculia and mathematics learning difficulties and includes guidance for seeking support (UCL, 2024). At the very least, children who demonstrate difficulty with concepts of number and quantity at preschool/first year of school or with a family history of dyscalculia (Haberstroh & Schulte-Körne, 2019) could be flagged for support or for standardised testing.
Mental health issues were present in all SpLD groups containing at least 10 participants, ranging from 33% for dyslexics without any other SpLD to 62% for participants with all three SpLDs. These estimates are higher than those reported in the population survey of the Mental Health of Children and Young People in England, 2023 where roughly one in five 8–25 years old had a probable mental health issue; the 2017 report indicated that the most prevalent disorder (8.1%) in 5- to 19-year-olds was of the emotional type (Newlove-Delgado et al., 2023). Given that anxiety and depression were the most common mental health issues reported by our participants, the difference from the population estimate is particularly concerning; and reasons for this could be probed in public participation events. Studies in other countries (e.g. Germany and Hungary) have also shown greater levels of anxiety and depression or emotional problems in late childhood and adolescence (Piko & Dudok, 2023; Visser et al., 2020). In Australian dyslexic adults, lower mental wellbeing has been reported (Wissell et al., 2021) and in Finland, mental health problems in adulthood were higher for those with SpLDs (reading and maths) than those without (Aro et al., 2019). Our findings thus highlight the urgency for more studies on coping; preliminary studies, for instance, suggest sex differences in the coping styles of dyslexics (Alexander-Passe, 2006).
Identification of dyslexia mostly took place in the education system (i.e. nursery/school) whereas a psychologist was the primary source for identifying dyscalculia and dysgraphia. This difference likely stems from the heightened public and educator awareness around dyslexia (especially teachers’ understanding of its early indicators). In England, there is a standardised phonics screener which ensures all early primary teachers understand the phonological indicators of reading difficulties. In Scotland, the Addressing Dyslexia Toolkit is a free online resource that educators are encouraged to use to support, assess, and monitor literacy difficulties. Many undergraduate and postgraduate teaching degrees will include some content on dyslexia whereas dyscalculia content is typically not part of the curriculum. With less public and educator awareness about dyscalculia, the early signs of numeracy problems may be missed by parents and teachers; and potentially get picked up by psychologists as part of assessment for co-occurring traits. In the UK, dysgraphia is identified/diagnosed by educational psychologists or a specialist assessor because it takes different forms (motor, sensory, perceptual, and dyslexic) that can be difficult to judge based on handwriting difficulties alone. The lack of a nationally agreed definition also makes its identification more difficult. Within the UK, the four nations use largely similar dyslexia definitions based on the Rose report and British Psychological Society, with expected revisions in line with a new Delphi study of dyslexia where a consensus definition was espoused (Carroll et al., 2024). Dyscalculia definitions within the nations also align with the definition agreed by dyscalculia working groups of the SpLDs Assessment Standards Committee and British Dyslexia Association (https://www.sasc.org.uk/media/215bhkbr/dyscalculia-maths-difficulties-assessment-sasc-nov-2019.pdf). The impact of not having nationally agreed definitions of SpLDs extend beyond confusion in identification and resulting support but will affect the translation potential of research which requires homogenous samples in which to study, for instance, causes, prevalence, and interventions (MacKay, 2009).
Half of the participants rated the process of obtaining a formal identification of an SpLD as being somewhat difficult or difficult, with a further 22% finding it very difficult. This was similar for those reporting on themselves (who were older) and those reporting on their child or young person. This suggests that there has been no improvement in the process of SpLD identification over the last generation. In particular, there was dissatisfaction with schools for not providing the right help. However, 43% of respondents found the process to be very easy, easy, or somewhat easy. To understand what schools should be doing, future public involvement should focus on those who had positive experiences to identify the procedures that they followed and that could be implemented more widely. Consulting with Dyslexia Friendly Schools (Riddick, 2006) would be another useful way to document their processes, particularly with regards to implementing policies around identification. In England, a formal diagnosis of an SpLD is required to obtain additional support in school whereas in Scotland this is not required. Nevertheless, the reported ease of identification did not differ between countries. A recent Delphi study identified a lack of teacher training and funding in schools and local authorities as the main barriers to dyslexia diagnosis and support, as viewed by parents (Harding et al., 2023), which aligns with the findings of our survey.
With regard to support following identification of an SpLD, those with dyscalculia and dysgraphia as their primary learning difficulty, reported it being harder to get support than those with dyslexia. Again, this can be linked to lower teacher awareness and training around numeracy and handwriting difficulties which is consistent with the free text responses that others lacked understanding of the learning difficulty. Other difficulties encountered were: a lack of information was available or that they did not know who to contact, both related to a failure of procedure in the education setting. Another main theme of the free text responses was that support was not offered or that it was inconsistent, again comments that link to the school setting. In terms of the most valuable support, technology was highly endorsed and so, too, was support in the educational/employment environment. This highlights a pressing need for educational practices to be improved in terms of making families aware of the support available and systematically offering it to those in need.
There was strong agreement (66%) that SpLDs should be talked about in terms of neurodiversity. Indeed, when asked for their preference in labelling SpLDs (disorder vs. difficulty vs. difference), participants preferred the term specific learning difference, which fits naturally into the neurodiversity framework (as highlighted by others (Sewell & Smith, 2020). Although it is possible that endorsement of this label was primed by the presentation of the definition of neurodiversity just prior to the question. The free text responses offered alternate suggestions of enabling language, like diversely able, yet others preferred the use of dyslexia, for instance, or disability, the latter ensuring legal rights in employment. Given that almost half of the respondents did not prefer ‘difference’, further work in this area is needed before advocating for a widespread change in terminology, and especially because our volunteer sample is not population representative. A Delphi study (Kirby et al., 2024) of dyslexia experts (researchers, practitioners, stakeholders) rejected the statement that ‘neurodiversity is a better term to use than dyslexia’, potentially because the label neurodivergent lacks the specificity that is needed to implement adjustments in education and employment settings. However, a narrative synthesis of the SpLD literature within the neurodiversity context has highlighted the potential for learning interventions informed by learning strengths and differences approach as a useful adjunct to a deficit-led remediation route (Sewell, 2022). Qualitative research focussed on practitioners/assessors is needed to better understand the concerns around the integration of SpLDs within the neurodiversity framework. Our study did not ask about the specific labels of dyslexia, dyscalculia, and dysgraphia, nor about preference for identity– versus person– first language, but it is clear that there was a leaning towards fostering a culture of acceptance of SpLDs as a difference in brain functioning which could positively impact children's self-esteem. Whether people with lived experience of SpLDs see value in specific labels will need investigating in the future. Qualitative research of dyslexic adults’ experience of their dyslexia, educational intervention, and public perceptions did not align with ‘anti-labelling’ arguments (Macdonald, 2010). Additionally, the future study of labels needs to consider how shifts away from these labels might affect relevant charities (e.g. British Dyslexia Association) and the impact they have made to increase public awareness of SpLDs.
Earlier identification and how to best support people with SpLDs were the two top priorities, with the causes of SpLD being ranked least important. This is in line with autistic adult community priorities around autism where research seen to directly impact people's daily life (e.g. mental health and identification) was most strongly endorsed whereas causes (including genetic and biological) were least endorsed (Cage et al., 2024). Interestingly, in our survey, the questions about genetics showed strong awareness of the genetic inheritance of SpLDs but mixed responses as to whether participants would want to know their own (or children's) genetic predisposition. It may be that participants recognise genes as causes (or associated factors) of SpLD so do not feel that further research is needed in this area. Yet knowledge about the risk factors of SpLDs may be valuable in future to identify children with SpLDs earlier, which was one of the top-ranked priorities. Geneticists who research human behaviour (including two of the authors) are only too familiar with the history of eugenics, so we speculate that others might also hold concerns over the use of such sensitive data especially as it applies to socially valued characteristics. A recent report on genomics and education has been published by the Nuffield Council on Bioethics and Nuffield Foundation, and outlines the opportunities and challenges in this sphere (Meaburn, 2025). Further qualitative research (e.g. in-depth interviews with interpretative thematic analysis) is needed to delve deeper into the motivations of participants’ preferred research priorities. Focus groups or Citizen's Juries which incorporate lay communication of how basic science in SpLDs can be translated to practice would serve as a useful way to evaluate whether research priorities are shaped by a lack of understanding of some of the research areas.
The top-ranked priorities echoed the difficulties around identification and support noted for all SpLDs in previous survey questions, and for those with dyscalculia, getting diagnosed and raising awareness were also priorities. These latter two priorities were ones of a practical nature that could be improved through increased education and funding around dyscalculia. The two top priorities require increased research to inform practice. In order to make the prioritised research as relevant as possible to those with lived experience of SpLD, research co-production needs to happen to formulate the specific research aims and hypotheses. Given that half of the participants in our survey reported at least one co-occurring developmental diagnosis/trait, future public involvement should include people with experience of single and multiple SpLDs, with and without other co-occurring developmental and/or mental health behaviours. Extra effort should be directed toward engaging those with dyscalculia and dysgraphia who were underrepresented in our study. This highlights the great value of high-profile charities like Dyslexia Scotland and the British Dyslexia Association (who helped with our participant recruitment) in heightening awareness of dyslexia, and the urgent need for equivalent in dyscalculia and dysgraphia. In future, we would recommend having people with lived experience of SpLDs being involved in the questionnaire design to better direct the content and improve the readability and organisation of questions to minimise questionnaire response attrition. Specifically, for the SLDN, our follow-on work will be to run focus groups with stakeholders aimed at narrowing down 10 research priorities identified by a James Lind Alliance Priority Setting Partnership on learning difficulties (Ai Keow et al., 2019). These results will also be made available to lobby funders and to direct research where it is most needed by neurodivergent learners.
Conclusion
The neurotypes of dyslexia, dyscalculia, and dysgraphia were sampled in our study to gain a more current perspective of neurodivergent adults and parents/carers of neurodivergent children or young people with lived experience of these SpLDs. Key findings included: substantial co-occurrence of SpLD neurotypes; high co-occurrence of SpLDs with other developmental traits; and high reporting of mental health issues. Key priorities were around earlier identification of SpLDs and how best to support them. For dyscalculia, an additional priority was around increasing awareness. To progress the research priority setting agenda, research-based co-production will require collaboration between people with lived experience of SpLDs, education practitioners and assessors who are involved in the identification of learning needs and in providing support and educational/workplace adjustments, and researchers whose work addresses SpLD identification procedures and evaluating support.
Footnotes
Acknowledgements
Authors’ Contributions
ML and SP conceived the research. ML, RM, MM, and SP designed/created the questionnaire. AYM and ML performed statistical analysis. ML drafted the article and all authors reviewed and edited the article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Biotechnology and Biological Sciences Research Council, MRC Harmonised IAA (grant numbers BB/T000813/1, MR/X502716/1).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Consent was not obtained to publicly share the data, but the analysis code is available on request.