
Abstract
Current parent training programs for ADHD do not appear to improve the parent-child attachment relationship, even though the quality of this relationship significantly influences the child's socio-emotional development and wellbeing. This mixed-methods, single-arm feasibility study evaluated the potential of a novel ADHD parenting program that aims to improve the parent-child attachment relationship. The study used pre- and post-intervention surveys and a follow-up focus group to assess program outcomes with 21 parents of 6–11-year-old children with ADHD and four allied health clinicians. Quantitative data indicate significant improvements in parent-child closeness and reductions in parent-child conflict (as assessed by the Child-Parent Relationship Scale) but no changes in scores on the Parental Stress Scale 10 days post intervention. Qualitative analysis generated three themes: (1) “Acceptance, connection, compassion and empathy,” (2) “It's wonderful, just what we need,” and (3) “These ideas would help the program better meet our needs.” Findings converge to suggest that the program is acceptable and may hold potential benefits for the parent-child relationship. These promising findings support further development and testing of the intervention. Findings are being used to refine the program to better meet the needs of parents and enhance its acceptability before proceeding with a randomised control trial.
Attention deficit hyperactivity disorder (ADHD), which affects approximately 7.6% of children aged between 3 to 12 years (Salari et al., 2023), represents the most prevalent form of childhood neurodivergence (Francés et al., 2022). While children with ADHD have copious strengths, display and misunderstanding of their neurological differences can challenge the parent-child attachment relationship (Dekkers et al., 2021; Weyers et al., 2019; Wylock et al., 2023). For example, limited understanding of ADHD and traditional parenting approaches likely contribute to ADHD-associated parent-child relational conflict (Weyers et al., 2019) and attachment insecurity (Wylock et al., 2023); and negatively affect the emotional wellbeing of children and parents (Cheung et al., 2018; Ringer, 2020). They also likely contribute to the high levels of frustration, exhaustion (Laugesen & Groenkjaer, 2015; Laugesen et al., 2016), stress (Theule et al., 2013), and depression parents report experiencing (Cheung et al., 2018), which increases the risk they will respond to their children in negative ways (Harold et al., 2013). When the strengths of children with ADHD are not recognised and their differences are criticised, or they find themselves on the receiving end of constant direction and redirection (Barkley, 2015; Brown et al., 2025a), and sometimes hostility and maltreatment (Clayton et al., 2018), their emerging self-concept is compromised (Miller, 2017; Ringer, 2020). They are also more likely to develop anxiety (D'Agati et al., 2019; Meinzer et al., 2014), depression (Daviss, 2008; Meinzer et al., 2014), substance use (Charach et al., 2011; Lee et al., 2011), eating disorders, self-injury, and suicide (Balazs & Kereszteny, 2017).
To support children with ADHD and their parents, National ADHD treatment guidelines often recommend parent training, which tends to be behavioural-based (ADHD Guideline Development Group, 2022; National Institute for Health and Care Excellence (NICE, 2018)). A recent systematic review however found that while existing parent training programs may improve parental stress and self-efficacy in the short term, there is little evidence that they improve child health outcomes, parenting behaviours, or attachment quality for 6–11 year old children with ADHD (Brown et al., 2024). Notably, none of the studies included in this review examined whether these programs assist parents in helping their children develop the traits and skills necessary for living well with ADHD (Brown et al., 2024). These being: an understanding of ADHD (Ginapp et al., 2023), self-awareness (Becker et al., 2023; Miller, 2017), self-acceptance (Attoe & Climie, 2023; Beaton et al., 2022; Rasmussen et al., 2022), acceptance of disability (Botha & van der Westhuizen, 2023; Zapata & Worrell, 2023), self-compassion (Mattingly, 2024), and skills and compensatory strategies (Ginapp et al., 2023) that support adaptation and self-mastery (Rasmussen et al., 2022). Additionally, parents report that behavioural-based parenting strategies are difficult to apply and have limited efficacy (Brown et al., 2025a; Corcoran et al., 2017); potentially because they mask underlying attachment problems and leave already frustrated and anxious children feeling more vulnerable (Richards, 2013).
In response, we proposed a neuro-affirming, ADHD-specific parenting program to better meet the needs of 6–11 year old children with ADHD and their parents (Brown et al., 2025a). This program represents a paradigm shift from negative narratives and traditional behavioural-based parenting approaches. Grounded in Bronfenbrenner & Morris (2006) Bioecological model of human development, the program integrates principles of acceptance, realistic optimism and mental health recovery principles. It aims to empower parents to (1) understand and respond to their children with ADHD in a manner that promotes healthy attachment and respectful dialogue, (2) scaffold their children's ADHD traits, and (3) and guide their children in recognising and developing their strengths as well as the skills they may need to live an independent, well-adjusted and empowered life in a neurotypical world (Brown et al., 2025a). In doing so, the program hopes to assist parents to look beyond ADHD-related deficit assumptions and to mitigate the detrimental impact that neurotypical parenting approaches can have on these children and their families. In an initial qualitative exploratory study, parents expressed overwhelming support for this parenting program, expressing a desire to better understand their children with ADHD and for strategies that enable them to respond to their children in a manner that is validating, supportive and protective of attachment quality. They also described their preferences for program structure and delivery (Brown et al., 2025a). This feedback informed all aspects of program development.
The next phase of program development involved a mixed methods, single-arm feasibility study of the educational and parenting workshop components of the program that aligns with the second phase of the UK Medical Research Council's Framework for Developing and Evaluating Complex Interventions (Skivington et al., 2021). This feasibility phase plays a crucial role in intervention optimisation prior to investing in an outcome evaluation (Skivington et al., 2021). Through formative evaluation processes, we collected and analysed data to inform program refinements to improve acceptability and implementability (Tsiachristas & Rutten-van Molken, 2017).
Specifically, we piloted the draft education and parenting workshop components of the ADHD parenting program (henceforth termed program) three times over a six-month period. We aimed to: (i) examine whether program participation led to improvements in attachment quality and decreased parental stress, (ii) explore parent and clinician participants’ perceptions and experiences of the program and parenting approach, and (iii) their perceptions of areas of the program that could be improved and preferences for program structure and delivery.
Methods
Researcher Positionality
As a team, we situate ourselves within the neurodiversity paradigm and wish to improve the experiences and outcomes of children with ADHD and their parents. Several team members bring their lived experience of ADHD to this research: LEB who developed the parenting program as an advocacy initiative; MT and BM. To honour the cultural and linguistic preferences of the Australian ADHD community (which differ from Autistic community preferences), we use the words condition and symptoms and refrain from using identity first language. We consider ADHD a neurobiological difference that can cause significant disability; “A condition that needs to be embraced and supported by parents, schools and society in general so that individuals with ADHD can be empowered to live well with ADHD” (Brown et al., 2025a).
Participants
Parent and guardian (thereafter parent) eligibility requirements were as follows: No previous or current relationship with the research team, and one or more children with ADHD aged between 6–11 years. The parent's children with ADHD needed to be on stimulant medication to align with clinical guideline recommendations for the provision of multimodal treatment (ADHD Guideline Development Group, 2022; NICE, 2018), and because this class of pharmacological agent is considered the first line medication intervention due to its efficacy (Coghill et al., 2023). Parents whose children also had anxiety, depression, a specific learning disorder (i.e., dyslexia), or oppositional and defiant behaviour (which can be evoked from mismatched parental responses to ADHD symptoms) were eligible to participate. However, conditions where children require parental support and their parents require education and assistance that falls outside the scope of the current program (i.e., autism spectrum, bipolar disorder, conduct disorder, intellectual disabilities) were excluded. Parents self-reported all information on their children's diagnoses. This was not confirmed by additional assessments or medical records.
Sixty-four parents expressed initial interest in the study via email and were sent study information; 23 were successfully recruited (female n = 21, male n = 2) and completed the consent form and pre-intervention survey. They comprised 22 biological parents (95.7%) and one adoptive parent (4.3%), aged between 30–39 years (n = 7), 40–49 years (n = 14), and 50 and over (n = 2); one of which identified as being an Aboriginal or Torres Strait Islander (4.3%). Eighteen parents (78.3%) had one child with ADHD and five (21.7%) had two children with ADHD. Twelve parents (52.2%) had completed an undergraduate bachelor's degree (in comparison to 20.3% of the Australian population) and four (17.4%), a postgraduate degree (in comparison to 8.1% of the Australian population; (Australian Bureau of Statistics, 2023). Fourteen parents (61.0%) had previously attended a parent training program, including Triple P (n = 11), 123 Magic & Emotion Coaching (n = 8), Circle of Security (n = 9), Incredible Years (n = 1), or another unspecified program (n = 5). Full demographic data is available in Appendix A (Supplementary File 1).
Regarding clinician recruitment, our aim was to recruit six allied health clinicians who work with children with ADHD (two per workshop). We recruited five clinicians, however, only four participated: two psychologists, one social worker, and one speech pathologist; all female (100%). Excessive time requirements and lack of availability were quoted as the reasons for declining our invitation. Clinician participants were aged between 20–29 years (n = 1), 30–39 years (1) and 40–49 years (n = 3). Their clinical experience ranged between 3–5 years (n = 3), 6–10 years, (n = 1) and over 10 years (n = 1). See Appendix B for demographic characteristics (Supplementary File 1).
Procedure
Participants were recruited from Perth, Western Australia, between late January and early June 2024; parents via Facebook and ADHD WA newsletter advertisements and clinicians via selective invite. No participant compensation was provided and the program was offered free of charge. Interested participants were sent information about the study, asked to provide written consent for participation, and emailed a link to the pre-program survey along with details about their allocated workshop date and location on receipt of a signed consent form. Ten days after the workshop, participants were sent a link to the post-program survey and an invitation for a focus group discussion. The survey needed to be completed prior to the focus group, which was conducted 14 days post workshop attendance, facilitated by MT and recorded. Parent focus groups were about 1–2 h and clinician focus groups were 30–60 min in duration. The study was approved by the Curtin University Ethics Committee (HRE2021-0090).
Intervention
The draft education and parenting workshop components of the program under investigation, including the underlying philosophy, theoretical framework, content and proposed delivery mechanisms were informed by a narrative review of the child development literature, an integrative review examining the impact of ADHD on brain maturation, composition, function and cognitive processes (Brown et al., 2025b) and the qualitative study discussed above (Brown et al., 2025a). The overarching aim and description of the program can be found in Appendix C (Supplementary File 1). Part A involved delivery of ADHD-related information, including how ADHD symptoms and underlying cognitive differences may influence a child with the condition. Part B involved describing the philosophy underlying the parenting program and providing parents with practical information aimed at fostering parenting skills. Program delivery was aided by PowerPoint slides, workshop activities, and lived experience scenarios (provided by the author and other parents and adults with ADHD). As ADHD is highly hereditary in nature (twin study estimates range between 77–88%; Faraone & Larsson, 2019), the needs of parents with ADHD were also considered and accommodated.
The program was delivered three times (to separate groups of participants). After each delivery, we slightly refined the program delivery mechanisms based on focus group feedback (see Appendix D, Supplementary File 1 for a description of the adapted versions). The program took place at Curtin University, and was presented by LEB with the support of an assistant who could provide individualised emotional support to participants if required. The first two iterations ran for 4 h and included a 20-min refreshment break. The third iteration was extended to 4.5 h and included a 30-min break.
Measures
We used two quantitative scales to assess changes in attachment quality and parental stress from the pre-program survey to the post-program survey. Parents who had more than one child with ADHD were asked to base their responses on their eldest child with ADHD.
The quality of the parent-child attachment relationship was measured using an original long-form version of the Child-Parent Relationship Scale (CPRS-LF; Driscoll & Pianta, 2011). CPRS-LF is a parent-completed scale containing 30 statements that correspond to three subscales. The conflict subscale (13 items) measures the extent to which a parent feels their relationship with their child is characterised by negativity. The closeness subscale (11 items) assesses the degree to which a parent feels their relationship with their child is characterised by warmth, affection and open communication. The dependence subscale (6 items) measures the extent to which a parent feels their child is dependent on them. Each statement is measured using a 5-point Likert scale (1: Definitely does not apply; 5: Definitely applies). For this sample, subscale internal consistency was: closeness (α = 0.80), conflict (α = 0.90), and dependence (α = −0.50).
Parental stress was measured using the Parental Stress Scale (PSS; Berry & Jones, 1995). The PSS contains 18 statements related to positive and negative aspects of being a parent. The degree to which each statement applies is measured using a 5-point Likert scale (1: Strongly disagree; 5: Strongly agree). Due to an administrative error, only the first 13 of the 18 scale statements were included in this study. The Cronbach's alpha score for internal consistency for the included items was 0.59.
Participant feedback on the program was collected via parent and clinician focus groups. Both Focus Group Moderator Guides are available in Appendix E (Supplementary File 1). Participants’ perceptions of the program were collected via three post-program survey questions (Appendix F, Supplementary File 1).
Data Analysis
Data gathered from each group of participants were combined due to the small sample size and program content consistency. All quantitative data were analysed using IBM® SPSS® software. First descriptive statistics were used to calculate frequencies of categorical, demographic variables. Next, pre-intervention to post-intervention changes in attachment quality and parental stress scores were analysed using paired samples t-tests. We report pre- and post-intervention means and standard deviations along with p values (Hedges & Olkin, 1985). Hedge's g is also reported for all analyses as a measure of effect size, with a g of 0.20 being considered small, 0.50 considered medium, and 0.80 considered large (Hedges & Olkin, 1985).
For qualitative data, the focus group transcripts were transcribed verbatim by LEB and managed using Nvivo. They were analysed using the reflexive thematic analysis steps proposed by Braun and Clarke (Braun & Clarke, 2006, 2012, 2021). To begin with, the focus group transcripts were read several times by LEB who made initial annotations to assist with data familiarisation, information processing, and later, initial code development. At the same time, LEB recorded reflexive notes and discussed her thoughts regularly with MT to support reflexivity. Codes were then collated and developed into initial themes by LEB in consultation with MT, using a thematic tree that underwent several iterations. Primarily an inductive approach to data analysis was used, however, to determine the program adjustments required to meet the needs of parents, a deductive approach was employed. The thematic tree was then discussed with MB and BM, which resulted in further refinements. A final assessment of the themes against the dataset was then conducted by LEB and MT to provide final confirmation (see Supplementary File 2 for thematic tree).
Results
Quantitative Analyses
Of the 23 parents who enrolled in the study, 91.3% (n = 21) participated in the program, for a pre-program attrition rate of 8.7% (n = 2). All the program participants completed the post-program survey, although one participant did not complete the CPRS or PSS scales. Four of the five clinicians (80%) participated in the program and completed the post-program survey; one withdrew for personal reasons.
As Table 1 shows, participation in the program was associated with significant parent-reported improvements in two aspects of the child-parent attachment relationship, with closeness increasing and conflict decreasing, both medium effect size. No significant changes in the dependence subscale or parental stress were noted (See Table 1).
Quantitative Data.
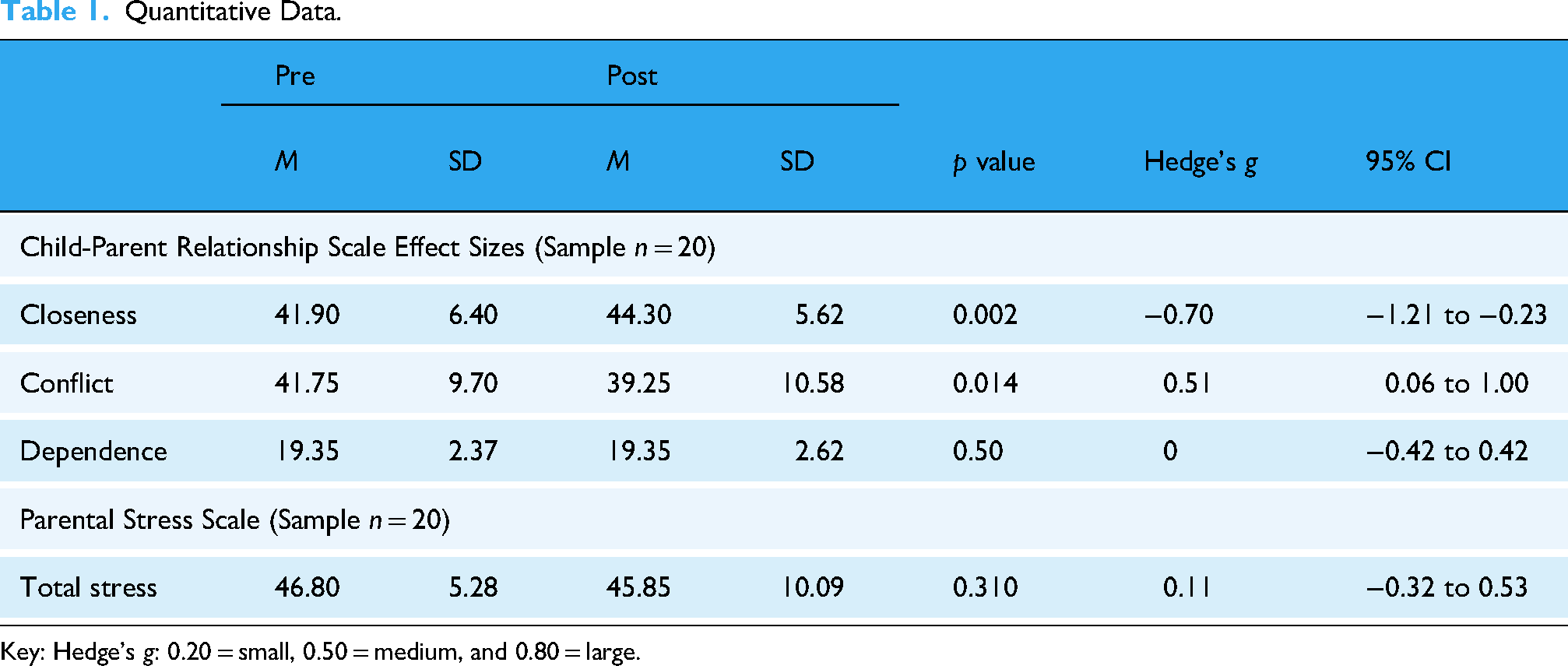
Key: Hedge's g: 0.20 = small, 0.50 = medium, and 0.80 = large.
All parents rated their experience participating in the program as good (n = 10, 47.6%), very good (n = 8, 38.1%), or excellent (n = 3, 14.3%). Twenty parents (95.2%) thought it would be beneficial if (1) a psychologist, nurse practitioner or social worker delivered the program and (2) they could access a program website containing the program content and other resources post-program completion. The clinicians rated the program as very good (n = 2, 50%) or excellent (n = 2, 50%). Three of the four clinicians (75%) indicated that they would consider delivering a manualised version of the program and continuing to support parents post program completion.
Qualitative Analyses
Fifteen of the 21 parent participants participated in a focus group (female n = 13). Reasons for non-participation included illness and unforeseen family needs. All four clinicians who attend the program participated in a focus group.
Three themes were generated from the data that reflected the language used by participants, the directness and limitations of the questions posed, and the aim of this study. The first theme, “Acceptance, connection, compassion and empathy,” provides insight into parents’ and clinicians’ responses to the parenting approach outlined in the program. The second theme, “It's wonderful, just what we need,” describes participants’ perceptions of the overall program and components that were highly valued. The third theme, “These ideas would help the program better meet our needs” summarises participants’ suggestions for improving the program.
Theme 1: Acceptance, Connection, Compassion and Empathy
Over three quarters of parents expressed positive thoughts about the parenting approach outlined in the program (no negative feedback was received), with the majority highlighting the importance of acceptance, connection, compassion and empathy and expressing the parenting approach aligns with how they want to parent their children. For example, Parent 6 stated, “I think it's a great approach… as opposed to a sort of standard… neurotypical kind of approach. It's designed for their diverse needs so you can adapt it to your child… [It's] not going to give them … negative self-feelings.” Parent 1 went on to explain: It's a child centred approach… You’re not trying to get a neurotypical child, like your child is never going to be neurotypical. So, it's acceptance of the reality that you're in. … You're coming from a different point of view, I guess. Connecting with the child and meeting them where they are at, as opposed to where you think they should be.
More than half of parents reported using this new parenting approach with positive results, although some found it difficult. For example, Parent 19 disclosed that her efforts connecting and collaborating with her son: “paid off because he was in a much better mood. … It's… nicer to be in the house when the dynamic changes.” However, she also highlighted that changing her approach to her son's meltdowns by listening with empathy felt “really clunky”: I struggled to keep myself regulated… It wasn't great, but I think he appreciated the effort… It was different [having me] listening more… as opposed to just saying this is what happened, needs to happen. … I think he appreciated that I asked questions.
There was also consensus among clinician participants about the benefits of the parenting approach outlined in the program. Clinician 1 endorsed the focus on the “attachment relationship; It moves away from trying to fix kids, to trying to understand and help them… [which minimises] the harm… that can come with not being understood.” Clinician 2 described it as: “an anxiety reducing style of parenting [that's likely to reduce] trauma and attachment trauma.”
Theme 2: It's Wonderful, Just What We Need
Overall, the parenting program was met favourably by nearly all parents and clinicians. “I found it was very, very informative. … It's a wonderful workshop” (Parent 13). Clinician 3 asserted the program, “was really wonderful, I received it gratefully. … [It focuses on] changing the relational dynamic [and the] longer term hopes and dreams and wishes that parents have for their children… What does my young person need to be an adult who lives a healthy, happy life to the best of their ability?” For Parent 19, the program was, “neuro-affirming. It didn't feel like… some other experiences I’ve had. [It's not about] teaching us how to get kids to follow societal expectations or rules.”
Several participants also expressed appreciation that the program was being developed, emphasising its important contribution. For example, Parent 18 asserted, “This is really good work, and it matters. … You can't possibly understand what impact this is going to have long term for the kids just in our little group,” and Parent 20 affirmed, the program will result in children with ADHD feeling “more supported and understood.” Furthermore, Clinician 2 stated she was “excited” and offered to, ‘do whatever is needed to help get this up and running.”
Both parent and clinician participants thought the program content was highly relevant and acceptable. For example, Parent 6 felt the program, “contains everything you need to know about ADHD.” Parent 7 expressed that she, “appreciated the… background [information on ADHD]; why they are the way they are, the differences in their brains and those types of things.” As per Parent 11, two thirds of parents also expressed that the program content had created a: “deeper understanding [and a] gear shift internally… Acceptance is probably the big part… you just have to accept and try not to react.” Parent 18 shared the program affected: “how I understand and how I make meaning from my child's behaviour.” Clinicians also felt that the content could help shift parent negative perceptions of their children. According to Clinician 4, the program made parents: “more aware of the potential impact of ADHD [and helped them] understand where their kid was coming from, which shifted their paradigm of what they think their child is doing and what their expectation of their child is.”
Another aspect of the program that was highly valued were the lived-experience scenarios provided throughout: “I think [they] resonated with a lot of people and… made everything very real” (Parent 10). “They made it incredibly relatable” (Clinician 4). The value placed on the lived experience scenarios was also highlight by participants concerns about how they could be offered when delivering the program at scale. As Parent 1 reflected, “I think lived experience is very important. Because [the presenter] weaved it in and out, [I’m wondering] how would that be done [in the final version]? Cause you still want to keep that lived experience… going forward?”
Participants also reported that they found the activities and facilitated discussions contained in the workshop component of the program helpful. This was especially the case for parents who attended the third iteration of the program as more time was allocated for this purpose. Parent 18 shared that the listening with empathy activities helped her to: “understand what my response should be in order to get to where I want us to be.” She also stated she was: Really glad that we not only did the role plays, but… also debriefed the role plays. … Having that modelled was… really powerful and helpful to refer back to in future. … [I also found] the unstructured discussion that we had towards the end… incredibly powerful and almost uplifting. [Knowing] I'm not alone in, in these kinds of challenges.
Along with the positive feedback, participants highlighted the need for the program to cater: “to different learning styles… [ensuring] that there are multiple ways and multiple opportunities to learn, relearn, question, revise and recall all this… information… over time and in different situations” (Clinician 3). This was particularly evident when it came to the information on ADHD. Parent 13 explained that her husband (Parent 12), “Really appreciated the first part… [Learning] about what it is and the changes in the brain,” however, she “felt it was really heavy.” A couple of parents also acknowledged, “Trying to keep [parents] attention in such a long presentation is going to be very difficult” (Parent 7), as is meeting everyone's individual needs. “It's very tricky to put [everything] in a workshop… I guess that's where there may need to be extra information” (Parent 13). As a result, some participants advised tweaking the delivery of some information to better facilitate parent's ability to retain and apply the foundational knowledge and the parenting approach.
Another suggestion related to increasing the time allocated for workshop activities and discussions, to enable parental connections and supportive interactions. As per Parent 11, who attended workshop 2 where less time was allocated for discussion: Like all kinds of education, it's not like it… drops in and then all the sudden life's different. … I would have loved heaps of examples of ways to scaffold [your child], instead of having to still do the work of trying to figure out what that looks. … [I would have also appreciated] talking [with other parents] about the challenges we face. … What works for you?
Theme 3: These Ideas Would Help the Program Better Meet Our Needs
To better facilitate information transfer, translation and consolidation, and increase the time frame that could be allocated to the workshop component of the program, nearly half of the participants suggested providing the information on ADHD pre-workshop attendance, in a manner that enabled parents to “learn at your own pace” (Parent 1). Suggested delivery mechanisms included online modules, pre-reading, and/or videos; “Then when you come in, you could recap the important bits and then the workshop is about … practical strategies and really getting hands on into… the meaty stuff” (Parent 1). In a similar manner, Parent 7 felt it would be beneficial to “come equipped with… background knowledge and then be able to apply that in the understanding of the parenting principles.” Parent 20 also felt the provision of a program workbook “to scribble notes down would be handy.” In regards to maintaining and extending the lived experience scenarios, along with the use of videos, Parent 7 acknowledged: “The lived experience can come from the participants in the room.” As per Clinician 2, clinicians also have lots of stories they can use, which according to Clinician 1, could be supplemented with “memes or… cartoons, pictorials or comics.” Other ideas to improve the program included the provision of more information on attachment theory and the social model of disability and using AI to help parents with knowledge application in the moment (Clinician 3). Some parents and one clinician also felt it would be beneficial if the program could support them advocate for their child at school.
Discussion
This study examined the potential efficacy, feasibility and acceptability of a novel, neuro-affirming ADHD parenting program and sought lived-experience feedback to inform ongoing program development. Our findings indicate that the program potentially holds benefits; the most being for the primary microsystem that influences child development, the parent-child attachment relationship. Results from both our quantitative and qualitative data indicate that the program led to an increase in parent-reported parent-child closeness and decreased parent-child conflict, although only short-term outcomes were measured and parental stress and child dependence remained unchanged. Further, captured under our first theme, “Acceptance, connection, compassion and empathy,” clinicians reported that the program's parenting approach aligns with attachment theory, and nearly half of parents shared examples of the positive effect using the parenting approach had on their relationship with their child. These findings are important as improving the quality of the parent child attachment relationship may positively influence a child with ADHD's emerging self-concept, self-esteem (Keizer et al., 2019; Storebø et al., 2016) and mental health outcomes (Mikulincer & Shaver, 2012).
In regards to program feasibility and acceptability, quantitative and qualitative findings indicate participants viewed the program positively. In the post-program survey, all parents and clinicians rated their experience participating in the program positively. Further, nearly all parents and all clinicians expressed positive thoughts about the program during the focus groups as captured under the theme, “It's wonderful, just what we need.” As expected, refinements to the program are still required, as indicated by almost 50% of parents rating the program as good rather than very good or excellent.
Lastly, participants provided suggestions that would enable us to better facilitate the transfer, translation, consolidation and application of the foundational knowledge and parenting approach contained in the program. These included providing parents preworkshop with information on ADHD in a manner than enables them to learn at their own pace i.e., via online modules, as well as a program workbook. Additionally, parents voiced a need to maintain and extend the lived experience scenarios contained in the program, and expressed a desire for the program being delivered in a manner that facilitates richer microsystem and mesosystem support for parents, which would have a flow on effect for their children. Specifically, parents highlighted a desire for (1) facilitated parental connection during program delivery, which could potentially help combat the dominant negative macrosystem influences (i.e., ADHD-related stereotypes and narratives) that can influence child and parental wellbeing, and (2) guidance on how to advocate for their children within the mesosystem school environment.
Together our findings converge to indicate that this parenting program is worthy of further development. The findings are being used to refine the program to better meet the needs of parents, including those with ADHD, and to enhance its acceptability prior to further piloting and evaluation in a randomised control trial. The incorporation of lived experience input remains a priority.
Limitations and Directions for Future Research
While this study provides valuable information that can be used to continue developing the program, findings of potential program benefits, including its impact on the parent-child relationship, remain largely exploratory due to the lack of a control group. Results for the dependence outcome should also be interpreted with caution given that the dependence subscale of the CPRS-LF demonstrated poor internal consistency in this sample. The CPRS-LF, although unvalidated, was chosen for use as it was the only scale we could find that examined aspects of the parent-child relationship we were interested in. While a new short-from version of the scale is available; little work has been done to validate the scale. While preliminary results from limited studies appear promising (Driscoll & Pianta, 2011; Rinaldi et al., 2023; Zabidi et al., 2023), further research is required to validate the scale prior to it being used in a randomised control trial. Alternatively, a new parent-child attachment relationship rating scale will need to be developed and validated moving forward. Secondly, while no significant changes in parental stress were reported, these results may have been impacted by an administrative error that led to the omission of five scale items. Future studies are needed to explore the potential impacts of the program on parental stress.
Of further consideration is that we did not conduct member checking of the qualitative data which may have generated additional information on parental experiences. Equally, while significant improvements in some outcomes where noted, parents likely require more time to apply the learnings from the program, however, a longer follow up period was beyond the scope of this feasibility study. Lastly, we excluded children who were on non-stimulant medication (i.e., atomoxetine) and did not examine the influence previous participation in a parenting program had on findings. Future research that involves a rigorous randomised trial comparing outcomes for parents who receive the program and their children (whether they are on stimulant or non-stimulant medication), to those randomised to a control condition, with a longer follow-up period is needed to determine whether the program is efficacious and holds potential benefits for child development, the parent-child attachment relationship and reductions in parental stress. Examination of the impact previous parent program participation and stimulant versus non-stimulant medication has on intervention efficacy should also be considered.
Conclusion
The results of this study, including participant feedback on the acceptability of the program and the positive effect of its neuro-affirming parenting approach on the parent-child attachment relationship, provide evidence that the program is worthy of further development. Supporting children with ADHD in the manner outlined in the program could potentially help parents raise independent, well-adjusted and empowered adults with ADHD.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330251340443 - Supplemental material for A Novel ADHD Parenting Program to Improve Parent-Child Attachment: A Mixed Methods Feasibility Study
Supplemental material, sj-docx-1-ndy-10.1177_27546330251340443 for A Novel ADHD Parenting Program to Improve Parent-Child Attachment: A Mixed Methods Feasibility Study by Louise E Brown, Mary Tallon, Garth Kendall, Mark Boyes and Bronwyn Myers in Neurodiversity
Supplemental Material
sj-docx-2-ndy-10.1177_27546330251340443 - Supplemental material for A Novel ADHD Parenting Program to Improve Parent-Child Attachment: A Mixed Methods Feasibility Study
Supplemental material, sj-docx-2-ndy-10.1177_27546330251340443 for A Novel ADHD Parenting Program to Improve Parent-Child Attachment: A Mixed Methods Feasibility Study by Louise E Brown, Mary Tallon, Garth Kendall, Mark Boyes and Bronwyn Myers in Neurodiversity
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LEB was funded by a Curtin University RTP Scholarship. MB is supported by the National Health and Medical Research Council, Australia (Investigator Grant 1173043).
National Health and Medical Research Council, Australian Government, (grant number Investigator Grant 1173043, RTP Scholarship).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.