
Abstract
Chronic stressors threaten child development with risk for poor mental health, disproportionately impacting those with pre-existing conditions such as attention-deficit/hyperactivity disorder (ADHD). However, associations between physical activity and mental health in children with ADHD during prolonged stressor experiences, such as the pandemic, are not well understood. Parents of youth (n = 412) with ADHD (n = 277) and without ADHD (n = 132) reported their youth's weekly physical activity levels, mental health symptom severity and subjective well-being during the pandemic. Bivariate correlation, independent t-tests and hierarchical multiple regression analyses assessed and compared relationships among factors between youth with and without ADHD during the onset of the pandemic. Children with ADHD had significantly higher mental health symptom severity scores and substantially lower subjective well-being scores than children without ADHD. Overall, there was no difference in physical activity levels between those with and without ADHD, and no association was identified between physical activity and subjective well-being in either group. However, counter to expectations and unique to the current study, for those with ADHD, there was a relationship between increased physical activity levels and worsened mental health symptom severity, warranting targeted attention to intervention and mitigation for future stressors and social disruptions.
Lay abstract
Experience of environmental stressors, such as the COVID-19 pandemic, affects those with pre-existing conditions like attention-deficit/hyperactivity disorder (ADHD), who may be at higher risk for mental health issues. Studies have shown that during the pandemic, there were increased rates of depression, anxiety and ADHD symptoms, as well as more screen time, less exercise and less sleep. However, we don't know much about how physical activity affects mental health in children with ADHD during this time. In this study, parents of children with and without ADHD reported their children's physical activity levels, mental health symptoms and well-being during the pandemic. They found that 16.3% of the children were not active enough, doing less than 30 min of physical activity per day, and 61.4% did not meet the recommended guidelines of more than 60 min of physical activity. Children with ADHD had higher scores for mental health symptoms and lower scores for well-being compared to children without ADHD. However, the children with ADHD who engaged in higher rates of physical activity paradoxically had worsened mental health symptoms, suggesting this association is more nuanced than first thought. Children with ADHD also had worse mental health symptoms when the pandemic started compared to those without ADHD. The study highlights the importance of population-specific research for children with ADHD and understanding the psychosocial factors that contribute to health and well-being, potentially informing future policy-making decisions, future research directions and tangible targeted interventions to preserve well-being for children with ADHD.
In March 2020, the World Health Organization declared the COVID-19 pandemic a threat to human health, which prompted the implementation of pandemic response protocols throughout the world in an attempt to mitigate infection spread (Cucinotta & Vanelli, 2020; World Health Organizations, n.d.; World Health Organization, 2020). In Canada, these protocols included strict physical distancing policies resulting in limited access to childcare, schooling, extracurricular activities and opportunities for physical activity (Emergency Management and Civil Protection Act, 2020a, 2020b; Hinshaw, 2020a, 2020b, 2020c; Public Health Agency of Canada, 2021; Reopening Ontario (A Flexible Response to COVID-19) Act, 2020; Shahab, 2020a, 2020b, 2020c, 2020d; Strang, 2021). Although these policies effectively slowed the rate of infection, they also prevented access to activities and facilities and, therefore, disrupted physical activity, which in and of itself could have adverse consequences on health and well-being (Galea et al., 2020; Gilbert et al., 2021; Santini et al., 2020; Soares et al., 2022).
Stress and health
The relationship between stress and adverse health effects is well-established in which a stressor is an experience external to the individual that exceeds or threatens to exceed the individual's coping resources, contributing to chronic health detriments, including inflammatory-related disease and mortality (Eisenberger, 2013). Stress also negatively impacts mental health, such as increases in anxiety and depression (Schneiderman et al., 2005; van Praag, 2004). For example, the experience of the COVID-19 pandemic encapsulated a double-sided chronic stressor through both the threat of infection and subsequent pandemic-response restrictions (Qi et al., 2021) that adversely impacted mental and physical health (Cowie & Myers, 2021; Dong et al., 2020; Lowe et al., 2023), with compounded effects on those with pre-existing mental health conditions (Fegert et al., 2020; García-Fernández et al., 2022; Gobbi et al., 2020). In terms of the lasting effects of stress on development, children are particularly susceptible (Condon, 2018). Moreover, those with neurodevelopmental conditions, such as attention-deficit/hyperactivity disorder (ADHD), may be disproportionately affected by chronic stressors, as these individuals are already more likely to experience comorbid mental health disorders such as depression and anxiety (Breaux et al., 2021). Indeed, as many as 80–90% of children with ADHD experience comorbid disorders such as anxiety, depression, behavioural and learning disorders (CADDRA, 2018).
ADHD is a neurodevelopmental disorder characterized by persistent inattention or hyperactive behaviour across environments (e.g. at home and in school), with current prevalence rates estimated around 8.6% in Canadian children (American Psychiatric Association [APA], 2022; Espinet et al., 2022). Given the rate of internalizing disorder comorbidities for children with ADHD, these children may be at a greater risk of detrimental mental health outcomes relative to their neurotypical peers exacerbated by chronic stressors, such as experienced in the COVID the pandemic and its subsequent responses. Future pandemics or environmental stressros pose a threat to this population alongside general populations, therefore, it is critical to understand the impact of the pandemic, to prepare and mitigate future stressor events.
Children's mental health during COVID-19
The COVID-19 pandemic and its related pandemic responses disrupted the routines of millions of children worldwide. Although the particulars of the pandemic response varied by region, in Canada, they paralleled infection rates, in which increases and decreases were consistent across provinces with close timelines for public health restriction application and removals (Dong et al., 2020; Emergency Management and Civil Protection Act, 2020a; 2020b; Hinshaw, 2020a; 2020b; 2020c; Public Health Agency of Canada, 2021; Reopening Ontario (A Flexible Response to COVID-19) Act, 2020; Shahab, 2020a; 2020b; 2020c; 2020d; Strang, 2021). Throughout the country, children were forced to adapt to many simultaneous changes, such as school closures, online learning, extracurricular cancellations, parental job loss and isolation from friends and family, affecting access to social networks. Longitudinal research from the United Kingdom (UK) suggested that pandemic-related responses negatively impacted the mental health of UK children with the highest levels of behavioural, emotional and attentional problems at the time of the strictest measures in which children were significantly restricted from accessing social connections, schools and activities (Shum et al., 2021). Among those most affected were children with neurodevelopmental disorders who experienced increased stress, sadness, boredom, depressive symptoms, sleep disturbances and fear (Munir, 2021; Shum et al., 2021).
Children with ADHD in particular reported notably worse deterioration in their mental health in relation to pandemic-responses (Sciberras et al., 2022; Shum et al., 2021). Meta-analysis of longitudinal and cross-sectional studies found that children's ADHD symptoms increased around the globe during the pandemic (Rogers & MacLean, 2023), while worsened mental health symptoms such as irritability, hyperactivity, opposition, aggression and disruptive behaviours were prevalent for ADHD children during widespread public health restrictions (Bobo et al., 2020; Shah et al., 2021; Swansburg et al., 2021). For example, increases in child anxiety and depressive symptoms were reported by parents of children with ADHD (Swansburg et al., 2021), which was associated with an increasing negative mood state (Zhang et al., 2020), affecting focus and contributing to fatigue, irritability and loneliness (Sciberras et al., 2022).
Notably, it was the children with ADHD who previously had mild mood-behavioural problems who experienced the greatest change during the pandemic stressor and, subsequently, a significant worsening across all domains (Melegari et al., 2021). For these children, the public health restrictions may have disrupted their social networks by separating them from friends and enjoying activities that protected them against factors that worsen ADHD symptoms, such as access to social support. For example, restricted access to extra-curricular activities limited the availability of social connections and support. In sum, the severity of mood-behavioural problems before the pandemic was a mediating factor that determined how pandemic responses affected the mental health of children with ADHD (Melegari et al., 2021). Clearly, the pandemic as a chronic stressor had adverse outcomes on children generally but disproportionately on those with ADHD, indicating a critical need to identify potential mitigations to buffer detriments in this population.
On the other hand, COVID-19 also led to positive mental health outcomes for some children with ADHD, suggesting the chronic stress response experienced in the pandemic is nuanced in this population. Potentially, children with ADHD may also experience some protective factors that can buffer and mitigate adverse stress effects. For example, pandemic restrictions were also related to positive lifestyle changes that benefited the mental health of ADHD children, particularly those with severe behavioural and mood problems (Bobo et al., 2020; Melegari et al., 2021). Indeed, for some children and adolescents with ADHD in France, there was a reported stability or improvement in behavioural symptoms, which parents attributed to decreased pressure from schoolwork and increased flexibility in their daily schedule (Bobo et al., 2020). What is more, some parents reported increased family time and subsequent self-esteem benefits attributed to school closures, eliminating peer comparison and rejection (Bobo et al., 2020; Melegari et al., 2021). Clearly, how chronic stressors are experienced and its relationship with protective or risk factors that preserve or threaten child health outcomes varies and is not well understood, particularly in the ADHD population.
Physical activity as a health protective behaviour
In addition to experiences that threaten well-being such as prolonged stressors, some factors preserve health and well-being, such as physical activity. In addition to the well-known physiological health benefits, physical activity also preserves mental health outcomes and is associated with decreased depressive symptoms (Moore et al., 2021). For example, for children between 5 and 17 years, participating in 60 min per day of moderate to vigorous physical activity is related to better mental health generally (Canadian Society for Exercise Physiology, 2021) and, particularly in the event of chronic stressors (Li et al., 2020). For children with ADHD, physical activity has been robustly associated with improvement in relation to anxiety, depression and overall executive functioning (Gawrilow et al., 2016), in addition to the core ADHD symptoms, such that exercise is often used as a treatment adjunct (Mercurio et al., 2021). However, the experience of a stressor, such as the onset of the pandemic and subsequent public health restrictions, can affect access to and utilization of physical activity. For example, the onset of the COVID-19 pandemic resulted in decreased physical activity and worsening mental health of children (Gilbert et al., 2021; Xiang et al., 2020), with those with ADHD being 21% less likely than their non-ADHD peers to be physically active (Mercurio et al., 2021).
In the initial stages of the COVID-19 pandemic, public health restrictions were implemented, rescinded and re-implemented over time that encouraged the public to stay at home and restricted access to schools, sports clubs, gyms and recreation centres for extended periods (Emergency Management and Civil Protection Act, 2020a; 2020b; Hinshaw, 2020a, 2020b, 2020c; Public Health Agency of Canada, 2021; Reopening Ontario (A Flexible Response to COVID-19) Act, 2020; Shahab, 2020a, 2020b, 2020c, 2020d; Strang, 2021). As a result, children's physical activity levels suffered, especially for families without access to outdoor leisure space, who faced limitations to environments that facilitate movement; consequently, this may have had implications for overall mental well-being (Groot et al., 2020; Pouso et al., 2021). Globally, children demonstrated a dramatic decrease in physical activity during the COVID-19 pandemic (Xiang et al., 2020). Specific to Canadian children, only 23.8% of children (5 to 11 years) and 13.2% of youth (12–17 years) met the recommended physical activity guidelines during the initial stages of the pandemic (Moore et al., 2021), compared to 36% of all Canadian children pre-pandemic (Canadian Society for Exercise Physiology, 2021; Statistics Canada, 2017). In sum, these studies demonstrate that in the event of a prolonged stressor such as COVID-19, children may experience a decline in all areas of physical activity (Moore et al., 2021), with implications for their mental health, particularly those with ADHD.
Taken together, the literature suggests an association between decreased physical activity and children's deteriorated mental health during this globally experienced stressor event. Aligning with global reports, Canadian Children with ADHD, also exhibited a relationship between decreased physical activity and both higher depressive symptoms and increased worry (Sciberras et al., 2022; Swansburg et al., 2021), which potentially exacerbated the stressor effects on well-being. All things considered, these results suggest an association between decreased physical activity and the deteriorated mental health of children with ADHD in the event of the pandemic stressor. However, whether these impacts were above and beyond those experienced by typically developing children is as of yet unknown. As such, the current study examined and compared the relationships between physical activity levels with mental health symptom severity and child subjective well-being between children with and without ADHD during a prolonged environmental stressor event, the COVID-19 pandemic. It was hypothesized that physical activity would be associated with improved mental health symptoms and child subjective well-being in both groups of children, but particularly for those identified with ADHD.
Methods
Participants
Participants (n = 473) were recruited via online advertisements shared on social media networks and the web pages of two national associations focused on ADHD. Parents of children diagnosed with ADHD and parents of typically developing children completed online questionnaires for all measures. Inclusion criteria were being the parent of a school-aged child (kindergarten to grade 12), residing in Canada, and being English-speaking. Only those who indicated whether or not their child had received an ADHD diagnosis and had two or fewer missing data points were included for analyses. A total of 473 participants consented to participate, of which 412 went on to complete study questionnaires hosted through Qualtrics (2005). Participants provided informed consent prior to completing any measures and received a gift card honorarium for participation. The Research Ethics Board of the University of Ottawa approved all procedures.
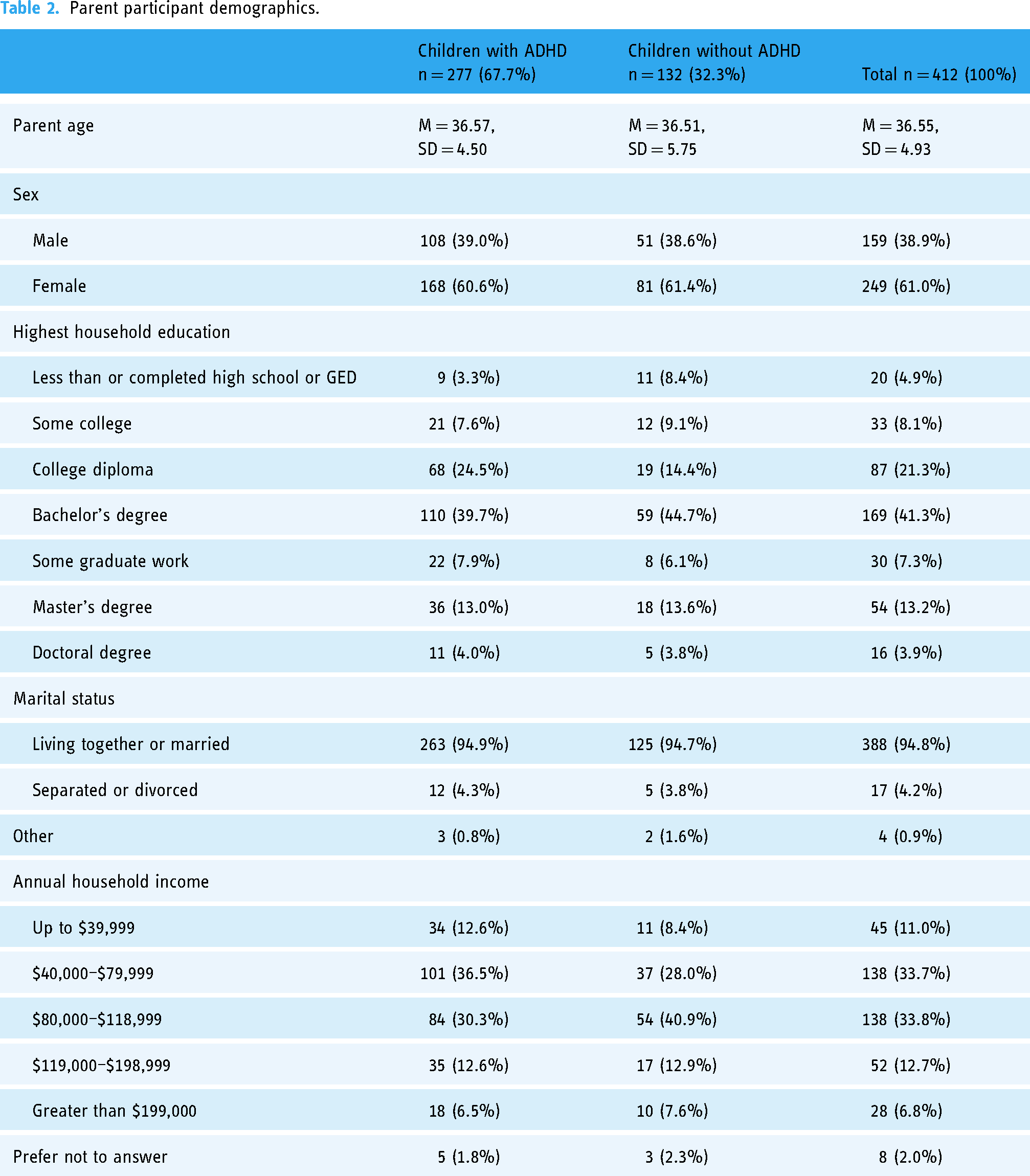
Participants provided demographic information on themselves and family in addition to their child's date of birth, sex, ethnicity and the presence or absence of an ADHD diagnosis. Sample characteristics are presented in Tables 1 and 2. The sampled children were 58% male and 42% female, and on average, males (n = 237; M = 10.02) were significantly older (t(407) = 2.01, p = .045) than female participants (n = 172; M = 9.43). Child participants were primarily White (61.9%) or Indigenous (18.6%) in the full sample, and there were significantly different proportions of reported child ethnicities between those diagnosed with ADHD compared to neurotypical children (X2 = 17.43, p < .001). In particular, Indigenous children represented 7.6% of the neurotypical sample and 23.8% of the ADHD-specific sample. However, there were no significant differences in average age (t(407) = − 1.14, p = .253) or distribution of sex (t(407) = − 1.18, p = .241), between the typically developing or ADHD-diagnosed groups. Children with an ADHD diagnosis made up 68% of the sample.
Child participant demographics.

Parent participant demographics.
Procedure
The current study data is a subset of a larger ongoing longitudinal study. Only measures included in the current study are reported. Participants reported sociodemographic information and completed online surveys assessing child mental health, subjective well-being and physical activity described below via Qualtrics (2005). All participants received a gift card honorarium for survey completion.
Measures
The child and adolescent symptom inventory-progress monitor-parent form (CASI-Pm-P)
The CASI-PM-P is a 29-item rating scale (Lavigne et al., 2009) consisting of eight disorder subscales linked to diagnostic categories in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5-TR; APA, 2022): ADHD – inattentive presentation (ADHD-I), ADHD – hyperactive-impulsive presentation (ADHD-HI), oppositional defiant disorder (ODD), conduct disorder (CD), generalized anxiety disorder (GAD), separation anxiety disorder (SAD), social phobia (SP) and major depressive disorder (MDD), with one item assessing functional impairment. The CASI-PM-P is a psychometrically valid and reliable scale, with high internal consistency, high test re-test reliability and moderate to high correlations between subscales (Lavigne et al., 2009).
The CASI-PM-P was used to assess the severity of child mental health problems. Parents indicated the severity of the problem by rating behaviour observed in the previous month using a Likert scale from never (0), sometimes (1), often (2) or very often (3). A symptom of one of the eight disorders is considered present if the caregiver responds with ‘often’ or ‘very often’. Scores across all mental health problems were summed, with total higher scores indicating increased severity of overall mental health problems (Lavigne et al., 2009). Total scores exceeding the clinical cutoff of 22 suggest clinical mental health concerns for all ages and sexes.
Child subjective well-being
The Child Subjective Well-being (CSW) is a single-item question adapted based on the Statistics Canada General Social Survey (2017) that measures the parent's perception of their child's satisfaction with their life. The parent responded on a scale of zero to 10 to the question: ‘How do you think your child feels about their life as a whole right now?’ with zero meaning ‘very dissatisfied’ and ten indicating ‘very satisfied’.
The physical activity scale
The Physical Activity Scale is a three-item questionnaire adapted from Millstein et al. (2011) that measures the number of minutes of physical activity that children accumulate weekly. To gain an understanding on weekly child physical activity, parents were asked to estimate the amount of daily physical activity their child had completed (excluding physical education class in school) within the previous seven days and to indicate how many days per week their child was physically active (at least 15 min, 30 min and 60 min). Then, the total number of minutes of physical activity per week was calculated for each child, ranging from a possible minimum of zero minutes to a maximum of 735 min. Physical inactivity in children was defined as less than 30 min of physical activity per day (Xiang et al., 2020); therefore, participants in the current study were classified as physically inactive if they acquired less than 210 min of physical activity per week.
Co-variates
Child demographic information was collected and incorporated within analyses as covariate variables. The current age and sex of the child were reported and controlled for in all regression modelling. Due to the disproportionate distribution of reported child ethnicities resulting in an extreme skew, child ethnicity was re-coded as (1) White, (2) Indigenous and (3) Not White or Indigenous. Additionally, parents reported the presence of absence of an ADHD diagnosis for all child participants.
Analyses
Independent unpaired t-tests evaluated significant differences between those with and without ADHD for each mental health symptom severity, physical activity and subjective well-being, and covariate information. Hierarchical regression modelling was used to assess relationships between physical activity and child mental health symptom severity and subjective well-being within the total sample and between groups of those with and without ADHD diagnosis. Modelling incorporated all covariates and physical activity at each level, with ADHD status and a moderating variable that looked at the interaction of physical activity and ADHD status at subsequent levels. Power analysis for a medium effect size (α = 0.3) using G*Power 3.1 (Faul et al., 2007) for a two-tailed multiple regression model with six and five predictors for the full sample and secondary within-group analyses, respectively, and an alpha level of .05 suggests a sample size of 68 and 64 to be sufficiently powered. Each regression model exceeded this suggested sample size, ensuring all models were adequately powered regardless of missing data (n = 350, 231 and 83, respectively, for mental health symptom severity, and n = 350, 250 and 99 for subjective well-being, respectively). Finally, Pearson correlation coefficients were computed to assess independent associations with physical activity and specific sub-scales for mental health diagnoses in those with ADHD. Missing items (three or fewer) were imputed by averaging the participant's previous responses. Participants with four or more missing items were excluded from the analysis (n = 61), for a total of 412 participants included in all analyses. All models were run using IBM SPSS Statistics (Version 26).
Results
A total of 16.3% of all children in the sample were classified as physically inactive and obtained less than 30 min of physical activity per day. Furthermore, more than half (61.4%) of the total sample did not meet the Canadian Society for Exercise Physiology Guidelines (2021) of at least 60 min of physical activity daily. Of the children with ADHD, 17.3% were reported to be physically inactive, compared to 14.4% of those without a diagnosis of ADHD. In addition to children classified as physically inactive, 65% of children with ADHD and 55.3% of typically developing children who were reported to be physically active still failed to meet the minimum recommended guidelines (Table 3); however, there was no significant difference in the rates of physical inactivity (t(377) = .34, p = .736), or physical activity per week overall (t(377) = .99, p = .321) between groups, with those with ADHD (M = 344.38 min per week of physical activity, SD = 150.29) and those without diagnosis (M = 362.37 min per week of physical activity, SD = 185.28) reporting similar rates. Additionally, there were no significant differences between the consistency of physical activity at either 15 min (t(388) = − .67, p = .506), 30 min (t(382) = − .44, p = .664), or 60 min per day (t(378) = 1.68, p = .094) between those with or without ADHD diagnosis.
Physical activity, mental health symptom severity and subjective well-being.


Significant associations with child mental health symptom severity in total sample.
Regression analyses for mental health symptom severity ratings (CASI-PM-P).
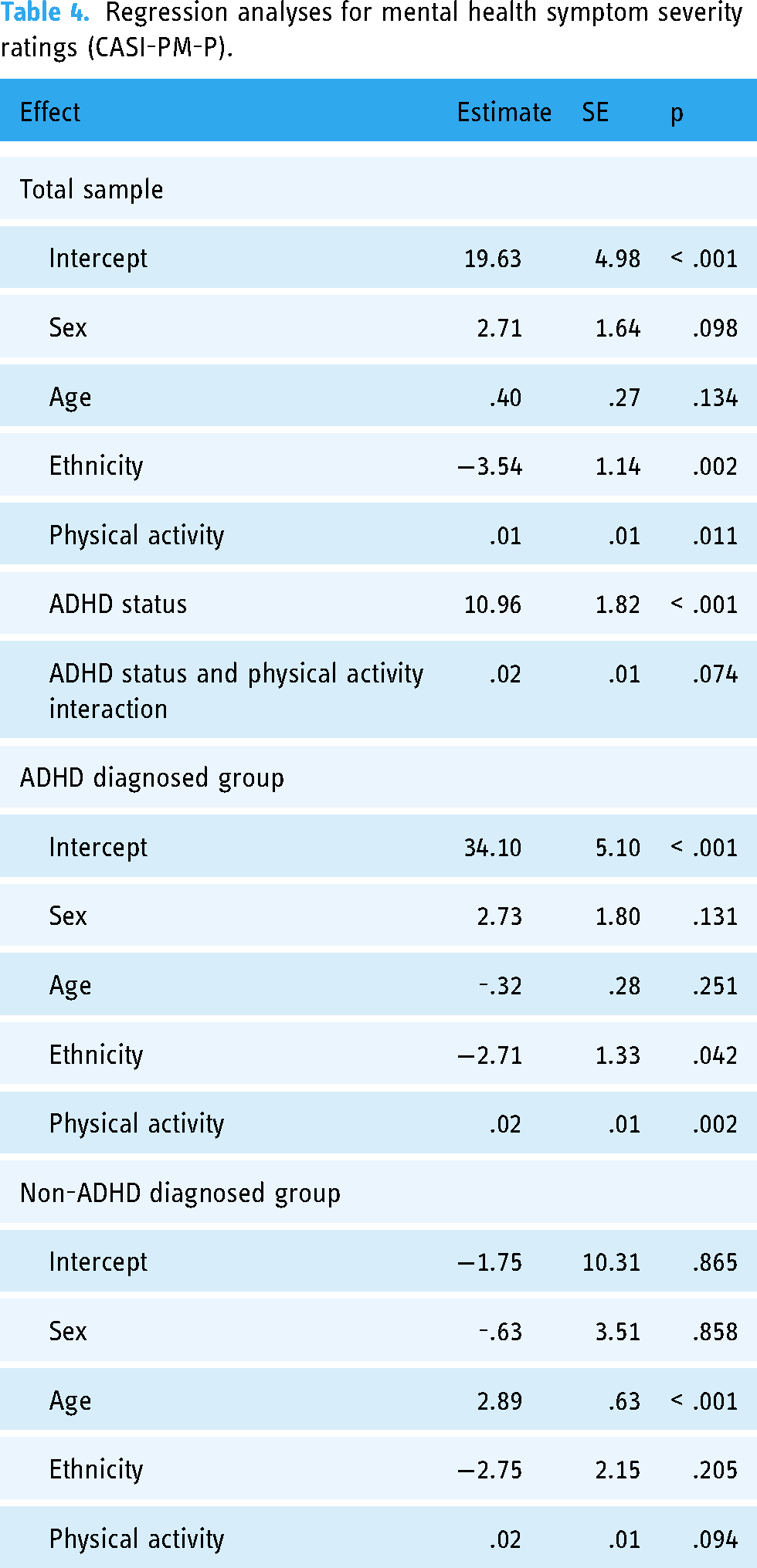
Mental health severity differed based on ADHD status (t(348) = − 6.13, p = <.001), in which children with ADHD had significantly higher CASI-PM-P scores (M = 39.10, SD = 13.65) than those without ADHD diagnosis (M = 28.40, SD = 16.68), indicating worsened mental health relative to their peers. Secondary regression models assessed these relationships within each of the ADHD-diagnosed and non-diagnosed groups. Within the ADHD group, child ethnicity continued to be related to mental health symptom severity (β = − 2.71, SE = 1.33, p = .042), whereas children with White ethnic backgrounds reported decreased mental health symptoms. For children with ADHD, increased time spent in physical activity was related to worsened mental health symptom severity ratings (β = 0.02, SE = 0.006, p = .002) (Figure 2). Specifically, bivariate correlations suggested that symptom severity for oppositional defiance disorder (r = .23, p < .001), conduct disorder (r = .25, p < .001), generalized anxiety disorder (r = .18, p = .003), separation anxiety (r = .18, p = .004), social phobia (r = .18, p = .005), global anxiety (r = .21, p < .001) and global depression (r = .26, p < .001) saw small positive associations with increased physical activity in the ADHD diagnosed group.

Significant associations with child mental health symptom severity in ADHD children.
However, for those without ADHD diagnosis, only age was associated with mental health severity ratings (β = 2.89, SE = 0.63, p < .001), with older children exhibiting worsened mental health symptoms, while physical activity was unrelated to mental health severity ratings (β = 0.02, SE = 0.01, p = .094) (Figure 3).

Significant association with child mental health symptom severity in non-ADHD group.

Significant associations with child subjective well-being in total sample.
Regression table for child subjective well-being.

Subjective well-being differed based on ADHD status (t(392) = 4.84, p < .001), with parents of children with ADHD reporting significantly decreased well-being scores on the CSW (M = 6.96, SD = 1.27) compared to children without ADHD diagnosis (M = 7.70, SD = 1.65). Additional linear modelling assessed relationships between physical activity and subjective well-being within each ADHD-diagnosed and non-diagnosed groups. For those without ADHD diagnosis, neither physical activity (β = 0.00, SE = 0.00, p = .851), nor any other covariates were significantly associated with subjective well-being ratings. In the case of those with an ADHD diagnosis, although those of an Indigenous and Non-White background indicated better subjective well-being (β = 0.25, SE = 0.12, p = .043), physical activity continued to be unrelated to well-being ratings (β = − 3.83, SE = 0.001, p = .945).
Discussion
The purpose of the current study was to examine the mental health and physical activity levels of children with ADHD compared to typically developing children during a prolonged environmental stressor experience. The findings show that most of the sample fell short of the movement guidelines, and 11.7% were classified as physically inactive. Further, children with ADHD experienced more mental health challenges during the study stressor, the pandemic, compared to their peers without ADHD.
Interestingly, children with ADHD experienced significantly poorer mental health symptom severity and subjective well-being relative to those without ADHD during prolonged stressor experiences, such as the COVID-19 pandemic, contrasting earlier pandemic research which suggested improved mental health for those with ADHD (Bobo et al., 2020; Fegert et al., 2020). Although pre-pandemic research indicated that 50%–90% of children with ADHD experience comorbidities such as anxiety, depression, behavioural and learning disorders (CADDRA, 2018), it is plausible that these large-scale pandemic responses, such as public health restrictions to public classrooms or structured activities, caused disruptions to daily routines and access to social connections which disproportionately exacerbated mental health challenges for those with preexisting conditions, aligning with earlier pandemic research (Fancourt et al., 2021; Lowe et al., 2023).
Further, that child ethnicity was significantly disparate for mental health symptom severity and subjective well-being was intriguing. Here, parents of children of a White ethnicity indicated reduced mental health concerns while concurrently reporting worsened subjective child well-being. Unique to the current study in the Canadian research landscape at this time was the ethnic diversity in our child sample. Indeed, although children of a White ethnicity represented 61.9% of the total sample and 60.3% of the ADHD group, representation from 7 ethnicities was present, collapsed into 5 to minimize identification for small groups, with an 18.6% Indigenous person representation. Although child ethnicities were not representative of the Canadian general population, sampling was improved over other pandemic research that relied on the increasingly disparate overrepresentation of White participants (Lowe et al., 2023). Potentially, parent and child expectations, behaviours and perceptions may have been mismatched and varied based on cultural heritage and identity, contributing to these disparate results. On the other hand, parents may have conceptualized well-being as distinct from mental health symptoms severity, rating overt behaviours of their children as more severe but non-disruptive to their child's perceived well-being in general, highlighting the resilience of their children in light of the prolonged environmental pandemic stressor event.
Indeed, the current study echoed findings of pandemic-related stressors exacerbating symptoms and increasing the risk of depression and anxiety in those with ADHD (Shah et al., 2021; Shum et al., 2021; Swansburg et al., 2021), which proved to be robust in longitudinal research also (Summerton et al., 2023). Ultimately, this worsened ADHD symptom and mental health response support the tenet that children with ADHD are more vulnerable to the effects of prolonged environmental stressors. Significantly, however, the current results extended the already identified stress–response phenomenon in children with ADHD and evaluated potential protective or moderator factors, such as physical activity. Interestingly, and counter to hypothesized associations given the extensive literature on health benefits (Gawrilow et al., 2016; Mercurio et al., 2021; Moore et al., 2021; Li et al., 2020), physical activity failed to be protective for this population, rather, it showed no marked improvements overall and was instead related to worsened mental health symptom severity for children with ADHD, a peculiar outcome indeed.
This unexpected association between physical activity and poorer mental health symptom severity was nuanced in this population. Although 54% of participants in the present study failed to meet the Canadian daily movement guidelines, this seems to be an improvement compared to 64% pre-pandemic (Statistics Canada, 2017) and 81% reported in early-pandemic research (Moore et al., 2021) for the general population. However, this difference may be related to sample-specific characteristics and highlights the need for population-specific research to reflect the unique experience of those with attention challenges. A possible reason for this increase in physical activity is that data was collected in the spring of 2020, after the initial onset of the pandemic amidst changing restrictions, as children and families acclimated to the ‘new normal’ (Emergency Management and Civil Protection Act, 2020a; 2020b; Hinshaw, 2020a, 2020b, 2020c; Public Health Agency of Canada, 2021; Reopening Ontario (A Flexible Response to COVID-19) Act, 2020; Shahab, 2020a, 2020b, 2020c, 2020d; Strang, 2021). This acclimation may be related to the posited phases of pandemic reactions described by Fegert et al. (2020): preparation, punctum maximum and the return to normality. At the start of the pandemic, in the preparation phase, many parents may have been afraid and uncertain about the length of public health restrictions and sheltered their children at home as much as possible. As a result, many parents worked from home, and children remained home from school. However, as time passed and public health restrictions progressed into the punctum maximum phase, parents may have acclimated to the new routine and sought expansion of their child's social networks and participation in activities outside the home. Possibly, the combined effect may have increased children's leisure time, resulting in increased play opportunities that naturally incorporate physical activity.
In addition to cross-sectional comparisons to pre-pandemic activity rates, nearly 12% of the total sample was classified as physically inactive. Still, this is a considerably smaller percentage relative to previous pandemic-related studies. For example, physical inactivity in children and adolescents increased from a pre-pandemic low of 21% to 65% after introducing public health restrictions (Xiang et al., 2020). The comparatively low level of physical inactivity in the current sample may have been protective for mental well-being generally. There are several explanations as to why the present study found physical inactivity levels relatively low. First, reported differences may be related to provincial and regional variances in public health restrictions affecting access to physical activity facilities and organizations (Emergency Management and Civil Protection Act, 2020a; 2020b; Hinshaw, 2020a, 2020b, 2020c; Public Health Agency of Canada, 2021; Reopening Ontario (A Flexible Response to COVID-19) Act, 2020; Shahab, 2020a, 2020b, 2020c, 2020d; Strang, 2021). Next, regional differences such as those between rural and urban centers may also be related to housing itself, household density and access to outdoor spaces in which to be active (Amerio et al., 2020; Groot et al., 2020; Canet-Juric et al., 2020; Amerio et al., 2020; Pouso et al., 2021; Ravens-Sieberer et al., 2021).
Still, the relationship between weekly physical activity and mental health was mixed, demonstrating the nuanced relationship between physical activity and psychological health for children with ADHD. Given that ADHD diagnosis was such a powerful predictor of outcomes, secondary analyses were conducted within each diagnostic group to better understand the effects of physical activity on child mental health. In this case, it was clear that the associations between physical activity and worsened mental health symptoms were restricted to those with diagnosed ADHD, likely driving the effect observed in the full sample. However, the association with child subjective well-being was diminished when assessed by group, suggesting that it was the presence of the ADHD diagnosis that was solely related to worsened child well-being outcomes. Although expected and paralleling mental health research in ADHD at all ages, this association with worsened well-being emphasizes the need to identify population-specific factors that can moderate and mitigate health outcomes to preserve ADHD well-being.
Specifically, the present study found that children without a diagnosis had no relationship between weekly physical activity and mental health; however, it is notable that the standard deviation for those without ADHD diagnosis (SD = 299) was considerably larger than for those with ADHD (SD = 163), suggesting an increased variability in physical activity levels, which may have dampened the signal of this relationship. Over and above this unexpected finding relative to the expansive exercise research conducted during the pandemic showing mental health benefits related to physical activity (Marconcin et al., 2022), these associations were further counterintuitive for children with ADHD. In ADHD children, increased physical activity was associated with worsened mental health symptom severity but not overall subjective well-being, countering expectations. The current findings contrast earlier pandemic research in which children and youth with higher physical activity had significantly lower mood disturbance during the pandemic than those with low physical activity (Zhang et al., 2020). It was expected that those who met the movement recommendations during the pandemic would experience fewer emotional and behavioural difficulties and fewer externalizing symptoms, with protective effects on emotional and behavioural challenges and overall mental health as seen in earlier stressor-related pandemic research (Tandon et al., 2021). Possibly, this finding highlights that although some children with ADHD engaged in increased physical activity relative to their peers, many were still well below the suggested threshold from the Canadian Society for Exercise Physiology Guidelines (2021), and that this association is more nuanced, potentially representing a curvilinear relationship between mental health symptom severity and physical activity for this population. Indeed, this relationship may be less dose-dependent, and, instead, the potential health benefits may be contingent on exceeding a specific physical activity threshold or consistency. In this case, those with increased physical activity efforts may have engaged in novel activities as a response to pandemic-related disruptions. This shift to alternative activity options may have had downstream impacts on their well-being by demanding increased physical efforts or attention to learn and engage in a new activity. In conjunction with adjustment to other environmental stressors, such as the ongoing pandemic, this increased attention demand may have proven to be a challenge for this particular population, with downstream impacts on mental health symptom severity overall.
It is also possible that those with more mental health symptoms were more physically active as a means of coping with difficulties. Moreover, recent research suggests that ADHD symptoms, including motor hyperactivity, increased during the time period of data collection (Rogers & MacLean, 2023). Thus, the present findings could also represent an overall increase in the physical or externalizing symptoms of ADHD. For the children with ADHD, higher rates of physical activity were associated with poorer mental health symptoms overall, both internalizing and externalizing. Specifically, these children reported increased occurrences of oppositional defiance disorder, conduct disorder, anxiety and depressive symptoms, aligning with findings that suggest those diagnosed with ADHD experience heightened and comorbid symptoms with mental health disorders (CADDRA, 2018). In this case, it may be the case that those exhibiting increased physical activity also represent those with the most adverse mental health symptom severity ratings. Not only does this association highlight the differentiated experience of mental health overall, but also how ADHD interacts with other environmental or psychosocial interventions in ADHD populations relative to those without ADHD, demonstrating the demand for ADHD-specific understanding of prolonged stressor experiences and associations with potential mitigating responses.
Still, although those without a diagnosis did not exhibit the same worsened mental health symptoms as those with a diagnosis, physical activity failed to demonstrate protective capacities, instead showing no significant impact. Potentially, for the same reasons children with a diagnosis also did not benefit from increased physical activity generally, those without a diagnosis may have been limited from access to preferred physical activities due to pandemic-related restrictions, confounding the beneficial effects of exercise. Within these analyses, only older child age was related to worsening mental health symptoms in non-ADHD children, which echoes existing literature that showed increased mental health challenges in adolescents at this time (Cost et al., 2022; Krokstad et al., 2022). Although this relationship is not unexpected, it is worth highlighting that this did not come through for those with ADHD, suggesting that this group potentially experiences consistently worsened mental health symptoms throughout child and adolescent development. This suggests that those with ADHD are disproportionately impacted relative to the fluctuations in mental health experienced in the general population, compounding the already elevated adverse mental health challenges often experienced by those with ADHD and underscores the need for ADHD-specific intervention and response, particularly during prolonged stressors, such as a pandemic.
Limitations
The current study noted several limitations in which the findings should be generalized with caution. First, the study design was cross-sectional. Because children with ADHD experienced more mental health comorbidities than typically developing children prior to the pandemic (CADDRA, 2018), it is difficult to determine the degree to which pandemic-related restrictions or physical inactivity were responsible for the mental health disparity between the two groups. Therefore, a longitudinal design which examines the mental health and physical activity of children with and without ADHD could provide further insight into this relationship. Second, recruitment utilized a snowball strategy, which may result in a homogenous sample due to participant selection bias (Parker et al., 2019). Third, there were more males than females in the total sample, and additionally, the ratio of sex differences in the ADHD group did not align with the proportion of males to females expected in the general population. In the case that physical activity and mental health vary as a function of sex, future research should evaluate these relationships when interpreting clinical population differences. Finally, the physical activity measure employed in this study was stratified with only three response options per day, limiting reported physical activity below and above the provided options. Additionally, parental reports of child mental health symptom severity, subjective well-being and physical activity levels may have been subject to social desirability bias and, therefore, provided incorrect estimations. Future research may consider using an accelerometer to measure children's physical activity to account for this limitation. Finally, although asked to disclose confirmed or disconfirmed ADHD diagnosis, the current study did not validate diagnosis, possibly missing ADHD status in the non-diagnosed group as well as overidentifying ADHD in the diagnosed group.
Conclusion & future directions
Overall, the present study examined the mental health and physical activity levels of Canadian children with and without a parent-reported ADHD diagnosis during the COVID-19 pandemic. Although research to date has identified associations between environmental stressor events and health outcomes (Schneiderman et al., 2005; van Praag, 2004), the current study uniquely bolstered these findings by incorporating a cross-sectional and typical developing control analyses.
Disparate results between the ADHD and non-ADHD groups highlight critical disparities that demand future research direction. For example, that child ethnicity was consistently associated with child outcomes but only within the ADHD group suggests a potential absence of understanding of cultural impacts on perceptions and interpretations of child behaviours and behaviours. A significant strength of the current study is the incorporation of a diverse sample that over-sampled minority ethnicities relative to the distribution in the Canadian context, giving rise to more diverse ethnic representation and identifying disparaging patterns in child wellbeing within the ADHD group. It is as of yet unclear why child ethnicity was consistently related to outcomes in children with ADHD. However, that variance in child ethnicities and potential cultural expectations and perceptions is significant and underscores the urgent need to incorporate more representative research in ADHD research.
Importantly, the findings of this study suggest that children with ADHD faced greater mental health challenges during the pandemic than typically developing children. In addition, most children reported sub-optimal physical activity levels. The reported relationships in the present study potentially suggest that although physical activity levels did not moderate outcomes, they could mediate the mental health of children with ADHD specifically, with inconsequential results for typically developing children; however, future research is required to understand better the direction and nature of this relationship over and beyond a linear association. Moreover, it is important to take an ADHD population-specific approach to exercise research, particularly when recommending it as an adjunct treatment. Clearly, the downstream associations with health and well-being differ between groups and may be contingent on the existing physical and social environment, the presence of environmental stressors and accessibility to activities.
Finally, and most importantly, the findings from the current study have important implications for mitigating risk in the event of future prolonged environmental stressors for children with ADHD. This is particularly important in the context of future global events, such as pandemic-related public health restrictions that disrupt access to physical activity. Notably, this research may inform public health policies and inform targeted intervention programs support to mitigate disproportionate adverse mental health outcomes for ADHD children affected by prolonged stressors, such as pandemic responses.
ADHD is a prevalent neurodevelopmental condition that encompasses one of the largest groups of neurodevelopmental disorders in children. Understanding the unique experiences of this population in the event of a global environmental stressor is critical to preserving health and well-being in future stressor events. Although COVID-19-specific threats are currently reduced, future pandemics and global environmental stressor events will also affect children with ADHD. Learnings, such as the discrepant ADHD-specific mental health symptom severity and subjective well-being outcomes and associations with physical activity, are critical to understanding to drive health-protective policies, population-specific research and implementation of evidence-based interventions to preserve and protect the health of children with ADHD.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research.