
Abstract
Emerging research suggests that menopause can be a difficult transition for some Autistic people. This international co-produced survey explored factors that might make menopause harder for Autistic people, such as lack of menopause and autism awareness; moreover, we aimed to explore what support Autistic people needed and what could help them cope and even flourish during this time. We employed a mixed-methods approach to analyze quantitative and qualitative responses from 508 Autistic participants. Both the quantitative and qualitative data supported relationships between lack of menopause and autism awareness and overall difficulties during menopause. Autistic participants wanted more appropriate and Autistic-specific information about menopause, and perceived lack of clinician awareness about both menopause and autism as barriers to care and support. Finally, participants reported discovery of ways to cope and even flourish during menopause through self-awareness and self-acceptance. Better awareness of autism and access to Autistic-specific menopause information is important in helping Autistic people transition through menopause.
Lay abstract
We believe that many Autistic people may struggle with menopause. However, we know very little about factors that might make menopause more difficult for Autistic people, and things that might help them through this transition. Our online survey, co-produced with Autistic people, explored whether a lack of awareness about menopause and autism might lead to a more difficult menopause experience. We also aimed to understand what kind of support and information Autistic people need in menopause, and what, if anything, helped Autistic people in menopause cope and even flourish through this life transition.
We received 508 usable responses from Autistic participants in 24 different countries. Overall, the study found a relationship between lack of menopause awareness and difficulty of menopause: i.e., that those who had less knowledge about menopause tended to have a harder time. The study also found that lack of awareness of one’s autism at the start of menopause was associated with a more difficult menopause experience. Participants reported that they wished they had had more appropriate and autistic-specific information about menopause before it started. They also indicated that a lack of information and training amongst clinicians about both menopause and autism were barriers to support. Finally, greater self-awareness and self-acceptance amongst other coping mechanisms helped participants.
Our findings highlight where there are gaps in knowledge and support for Autistic people during menopause. They highlight that knowledge about menopause, and about one’s autism, are extremely important. They also highlight coping strategies that some Autistic people have found helpful.
Menopause is a life stage which affects almost all people assigned female at birth (AFAB people). The transition from a reproductive to post-reproductive state (Harlow et al., 2012; Hoyt & Falconi, 2015) encompasses both perimenopause (a life stage marked by fluctuating hormones and accompanying symptoms, with menstrual periods becoming irregular and variable) and ‘reaching’ or ‘passing’ of menopause after 12 consecutive months without a period (post-menopause). The majority of AFAB people in higher-income countries enter menopause naturally in their mid to late 40s (Davis et al., 2015). Menopause involves physical and physiological changes, as well as cognitive and emotional symptoms. This transition typically lasts between 4 and 10 years (Davis et al., 2015; Harlow et al., 2012), and therefore can affect a significant portion of one's adult life.
Emerging research suggests that the menopausal transition can be a difficult time for some Autistic people (Brady et al., 2024; Charlton et al.; Groenman et al., 2022; Karavidas & de Visser, 2022; Matthews et al., 2024; Moseley et al., 2020, 2021). Autistic research participants report experiencing menopausal symptoms very intensely (Brady et al., 2024; Karavidas & de Visser, 2022; Moseley et al., 2020, 2021), and they report higher degrees of somatic symptoms, anxiety and depression than do non-Autistic people matched in age, IQ and education level (Groenman et al., 2022). Extreme distress, dysregulation, burnout and suicidality during menopause are cited in qualitative literature (Brady et al., 2024; Karavidas & de Visser, 2022; Moseley et al., 2020, 2021), and are consistent with broader literature on well-being of Autistic women at midlife (Grove et al., 2023; Leedham et al., 2019). Studies also suggest that some Autistic people start perimenopause with little awareness of the range of symptoms and impacts (Moseley et al., 2020, 2021), and have difficulty finding appropriate information, support, and healthcare during the transition (Brady et al., 2024; de Visser et al., 2024). Though not the focus of the present report, emerging research suggests that some of these challenges are shared by those with ADHD, who also appear to experience a heightening of cognitive, emotional and sensory difficulties and subsequent exhaustion (Dorani et al., 2021; Gottardello & Steffan, 2024; Kooij, 2023; Wasserstein et al., 2023). Broadly, the neurological nature of menopause (Brinton et al., 2015), and the role of (o)estrogen and other fluctuating hormones in cognition and emotion (Barth et al., 2015; Koebele & Bimonte-Nelson, 2017), may make people with existing neurological differences especially vulnerable during this life stage.
As menopause studies related to Autistic people have involved small samples to date, there is a need to replicate their findings on a larger scale, particularly to explore the extent and nature of unmet needs. Questions remain about the variability of menopausal symptoms in Autistic people. This variability occurs despite likely sampling bias, given the fact that research on this topic might appeal most to those who have struggled (Moseley et al., 2021). Two factors emerge as potential determinants of menopausal symptom severity: menopause awareness and age at autism realization and/or diagnosis. Research on the general population suggests that people's perceptions and attitudes about menopause, and thus their awareness and understanding of it, may influence symptom severity. Better understanding is typically associated with greater perceived self-efficacy and well-being (Harper et al., 2022; Huang et al., 2023; Richard-Davis et al., 2022; Süss & Ehlert, 2020). Lack of menopause awareness appeared to be a factor in the distress reported by Autistic people in the above qualitative studies, as participants sometimes mistakenly attributed menopausal symptoms to mental or physical illness. Relatedly, participants suggested a relationship between well-being at menopause and autism awareness (Brady et al., 2024; Moseley et al., 2021). Some suggested that the distress and confusion caused by menopausal symptoms were compounded by their inability to understand why their experiences differed from others; some suggested that knowing about their autism before menopause might have facilitated self-compassion, which has protective effects at menopause (Süss & Ehlert, 2020). There are additional reasons late autism realization could be associated with particular difficulty. Late-in-life or undiagnosed Autistic people often have a history of life adversity and poor mental health (Belcher et al., 2022; Dubreucq et al., 2022; Gellini & Marczak, 2023; Huang et al., 2020; Newell et al., 2023; Smith et al., 2024). Cumulative lifetime stress is associated with more severe difficulties during menopause (Kapoor et al., 2021; Metcalf et al., 2022), which can often exacerbate ongoing mental as well as physical illness (Behrman & Crockett, 2023; Hoyt & Falconi, 2015).
While there are reasons some Autistic people might struggle during the menopausal transition, another gap in the literature pertains to coping, adaptation, psychological growth and resilience of Autistic people during menopause. Perhaps in consequence of the biomedical model typically applied to autism and Autistic people, the vast majority of research pertaining to this group is problem-focussed, sometimes objectifying and/or dehumanizing, and non-participatory (Botha & Cage, 2022). Few studies report examples of Autistic flourishing (Pellicano & Heyworth, 2023), identity, and/or agency (Stenning, 2024). Similarly, previous qualitative studies on Autistic people at menopause hinted at growing self-awareness, self-acceptance and resilience through the turmoil of perimenopause (Brady et al., 2024; Karavidas & de Visser, 2022; Matthews et al., 2024; Moseley et al., 2021), but did not focus on these, or investigate factors associated with resilience and greater well-being during and after menopause. Coping strategies are essential to maintain well-being in relation to menopausal symptoms (Süss & Ehlert, 2020), and their importance has also been highlighted in relation to Autistic people (Ghanouni & Quirke, 2023; Muniandy et al., 2022). As such, coping during this life stage is an important omission from the current literature.
The current study
With existing knowledge on Autistic people at menopause based on relatively few individuals (Brady et al., 2024; Groenman et al., 2022; Karavidas & de Visser, 2022; Moseley et al., 2020, 2021), in the present mixed-methods and multi-national approach, we aimed to contribute information on a larger scale. Co-produced by Autistic community researchers and academics and led by feedback from Autistic people in a previous study (Brady et al., 2024), we aimed, firstly, to explore the symptoms experienced by Autistic people during the menopausal transition, their awareness of these symptoms, and relationships between overall menopause difficulty and menopause and autism awareness. Since earlier efforts indicated the importance of knowledge for Autistic people to prepare for menopause, and their difficulties accessing support (Brady et al., 2024; Moseley et al., 2020), we also aimed to explore what kinds of support and information participants felt they needed during menopause, and what specific barriers they faced in accessing care and support during the menopausal transition. Finally, given the predominantly problem-focussed approach of previous studies (Karavidas & de Visser, 2022; Moseley et al., 2021), we aimed to explore both struggles and examples of Autistic flourishing during and after the menopause transition, and to document the strategies that helped Autistic people cope and even thrive.
Methods
Participants
Team members, especially the two Autistic Community Research Associates (CAJ and RJM), recruited participants by sharing details through social media sites Twitter (X) and Facebook, our project website (‘Bridging the Silos: Autistic Menopause Study'), support groups, contacts, and conference presentations. Inclusion criteria required participants to be Autistic and have experience with the menopausal transition (from peri- to post menopause). Due to barriers to diagnosis that many Autistic people face (O'Nions et al., 2023), a formal diagnosis was not required. International participation was welcomed, with no exclusion criteria pertaining to country of residence or birth.
In total, 643 responses were received. One hundred and thirty-five were excluded. We excluded 119 datasets where participants had not completed up to the question whether they were aware of their autism when entering the menopause (a key variable in our analyses). This question occurred just over a third of the way through the whole survey, and those whose datasets were excluded had completed less than 35.7% of the survey. We also excluded 11 datasets where responses were likely fraudulent (through visual-checking and embedded data within Qualtrics), and five from participants who did not consent or decided to delete rather than submit their responses. As such, from 643 responses, 508 datasets were retained for analysis.
Measures and procedure
Following ethics approval from the last author's institution, the survey was available on the Qualtrics platform from March to June 2023. After initial demographic questions, the survey included:
which menopausal symptoms were experienced by participants (a selectable list with opportunity for text entry); which symptoms experienced were ‘a surprise’ (another selectable list with text entry); whether participants had known what to expect when menopause started (‘Yes’, ‘No’, with free-text option); whether participants felt they had sufficient information about menopause before or once it started (‘Yes’, ‘No’, ‘Not sure’); how difficult they would rate their menopause experience overall (between 0, ‘Not difficult at all’, and 100, ‘Extremely difficult’); whether participants accessed sufficient information for several topics (selecting between ‘I wish I had had more information’, ‘I had enough information’, ‘I did not need information about this’); where participants had found information about menopause (a selectable list with free-text); AND whether participants had accessed professional support at menopause, and if so, where from (a selectable list of private and public services with free-text).
The survey design prioritized accessibility (see Supplementary Materials, item 1), influenced by feedback from Autistic participants in an earlier focus group phase of the project (Brady et al., 2024), and was reviewed by four Autistic and one non-Autistic beta testers. The survey was estimated to take 45–60 min to complete, and participants did so anonymously.
Data analysis
We employed a mixed-method approach focused on qualitative analysis. Initially, we computed descriptive statistics for participant age when self identifying or being diagnosed as Autistic, and age at menopause onset; menopausal symptoms experienced by participants, and those which were unexpected; and participant responses to whether they felt they had enough information about menopause generally, and how difficult their menopause had been overall.
We used the rating of general menopause difficulty as the dependent variable in three statistical analyses aimed at exploring relationships between menopause awareness, autism awareness and menopausal difficulty; for each, we used SPSS (Statistical Package for the Social Sciences) version 28. Firstly, to test whether menopause awareness was associated with the severity of menopausal difficulties, we examined correlations between overall menopause difficulty and, as a proxy measure of menopause awareness, the number of symptoms that were unexpected for each participant (while controlling for the overall number of symptoms they experienced). We corroborated this by comparing menopause difficulty ratings in those who said they did know what to expect when entering menopause (n = 102), and those who said they did not (n = 356). Next, in order to test whether menopausal experiences differed in relation to an individual's autism awareness, we compared menopause difficulty ratings between participants who did and did not know they were Autistic at menopause. We collated participants who had already been diagnosed with those who had already self identified as Autistic at the time (n = 228), and used a between-subjects ANOVA to compare these with those who did not know they were Autistic at perimenopause onset (n = 270; datasets of participants who expressed uncertainty or preferred not to answer, n = 10, were not analyzed so n = 498).
To examine the information and support that participants had, and felt they needed, we computed descriptive statistics for information types that participants wanted at menopause, as well as their sources. We also produced descriptive information about where participants had tried to access support and analyzed parts of the qualitative data using a codebook thematic analysis (Braun & Clarke, 2022). The team identified 19 open-ended data fields which were good candidates for qualitative analysis (see Supplementary Materials, item 2); they included longer text entries rather than short responses. Following Braun and Clarke (2022), two team members familiarized themselves with the data and worked together to inductively create an initial codebook, with a table of codes and short descriptions. Both team members independently coded qualitative fields with initial codes and added new ones. They then shared their coded data and created one combined codebook; a third team member worked with the coders to create candidate and final themes and subthemes, through data interpretation and continuous review and consensus.
Reflexivity was a key practice in our research, and we assumed a model of co-production between two Autistic community researchers and four academics. As Braun and Clarke (2022) discuss, reflexivity involves reflection on behalf of researchers on their role and subject position in the design and execution of the research throughout the entire process.
The respective subject positions of the research team members inherently shaped our relationship to all aspects of this research. Our team included two Autistic Community Research Associates (CRAs) based in Canada and the UK, who are deeply rooted and active in Autistic communities (CAJ, RJM). Their involvement and lived experiences fundamentally formed and shaped the project. The team also included academics based in Canada involved in research in Communication and Media Studies and Social Work, one of whom is the parent of an Autistic child (MJB), the other with experience working with Autistic people (MJVR). Academics from the UK are experts in Psychology with an established track record in relevant areas (JGT, RLM); one also has lived experience as an Autistic academic (RLM). Though we each have different connections to Autistic communities, we understand that as full-time professionals within academic institutions (JGT, MJB, MJVR, RLM), some of us have unequal class and social power relative to some (but not all) participants. We recognize that all team members benefit from white privilege, and would like to acknowledge the unceded Algonquin territories on which three of the researchers live and work (CAJ, MJB, MJVR).
Results
Our 508 Autistic respondents took part from 24 different countries, but were concentrated in the UK, USA, Canada and European countries. A much smaller percentage (1.6%) of participants hailed from countries in the global south, such as South Africa, Costa Rica, the Philippines, Singapore, and South Korea. Their demographic information is displayed in Table 1. Our analysis includes both descriptive statistics and qualitative analysis explained further below. Descriptive statistics tested whether menopause awareness and autism awareness were associated with overall difficulty of menopause, and this relationship was supported in both cases. The majority of participants also indicated they had not found sufficient information about menopause before perimenopause onset.
Participant demographic characteristics.

Note: N = 508.
Multiple response options allowed, percentages may not add up to 100%.
Includes hypermobile Ehlers Danlos (hEDS), Ehlers Danlos, Postural Orthostatic Tachycardia Syndrome (POTS), and Mast Cell Activation Syndrome (MCAS).
Participants who did not respond to the question about menopause status were included in the analysis because they had indicated that they met the inclusion criteria of having at least started perimenopause in the consent language before beginning the survey.
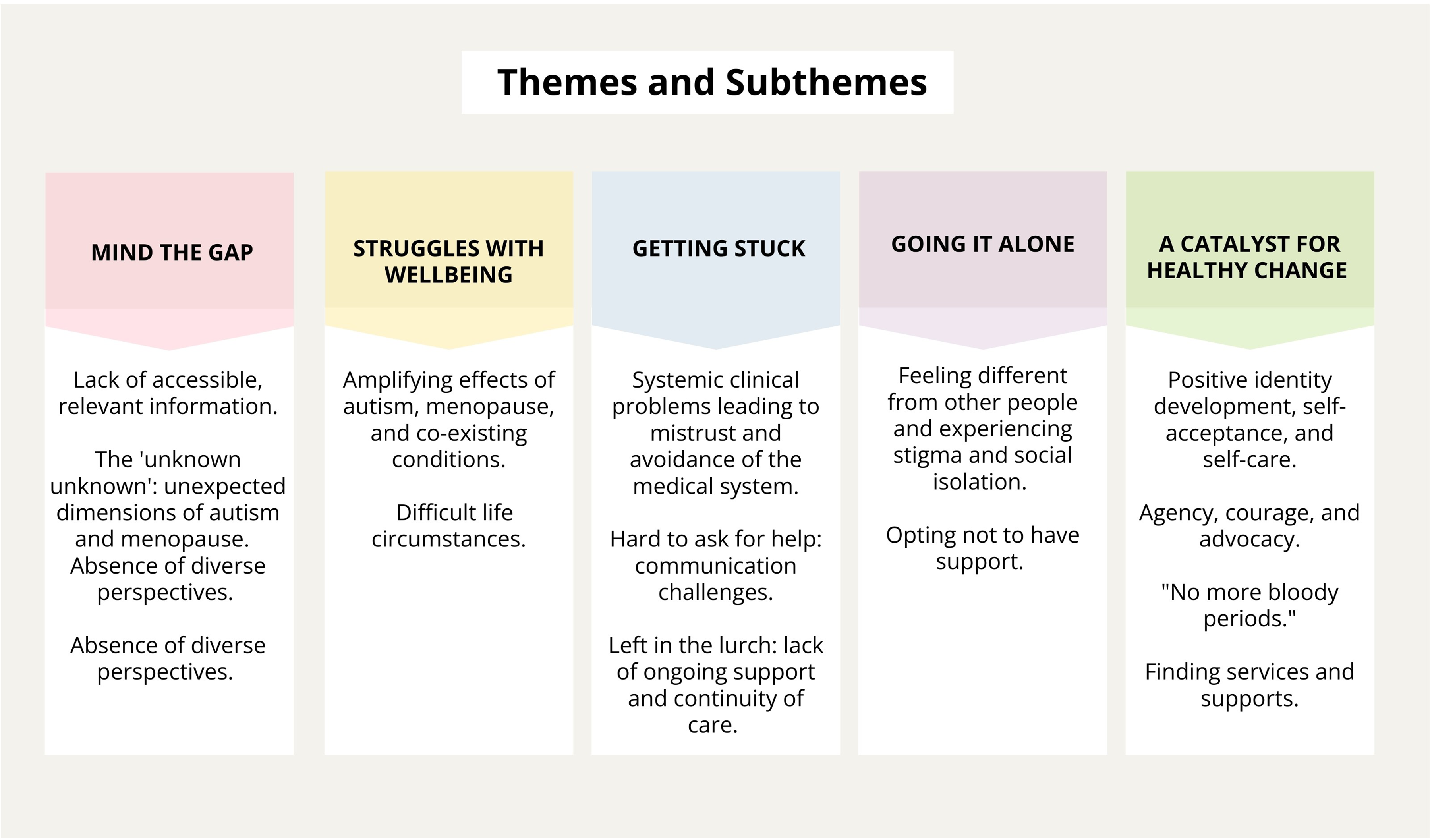
Our qualitative analysis provided further insights; we arrived at five themes and 14 subthemes outlined further below and illustrated in Figure 1: Theme 1: Mind the Gaps: Knowledge, Information, and Representation (3 Subthemes: Lack of accessible, relevant information; The unknown unknown: unexpected dimensions of autism and menopause; Absence of diverse perspectives); Theme 2: Struggles with Well-Being (2 Subthemes: The amplifying effects of autism, menopause, and co-existing conditions; Difficult life circumstances including late discovery of autism); Theme 3: Getting Stuck: Barriers to Accessing Health Care and Support (3 Subthemes: Systemic clinical problems leading to mistrust and avoidance of the medical system; Hard to ask for help: communication challenges; and Left in the lurch: lack of ongoing support and continuity of care). Theme 4: Going it Alone (2 Subthemes: Feeling different from other people and experiencing stigma and social isolation; Opting not to have support). Theme 5: A Catalyst for Healthy Change (4 Subthemes: Positive identity development, self-acceptance, and self-care; Agency, courage, and advocacy; Finding services and supports; “No more bloody periods”).

Themes and subthemes from qualitative analysis.
Descriptive statistics
Symptoms experienced and expected and awareness of autism and menopause
Most participants were diagnosed or self identified as Autistic in adulthood: in those who could recall their age (n = 473), the average age was 45.9 years (SD: 8.37, range: 3–67). Not all participants knew or could recall their age at first menopausal symptoms (n = 100); in those who did respond to this question (n = 408), the mean age when participants reported first menopausal symptoms was 43.81 years (SD: 4.90, range 36). Of participants who completed these questions (n = 497), the most commonly-reported symptoms were changes in memory and/or concentration (brain fog), changes to mental health, sleep disturbance and hot flushes/hot flashes (Figure 2, Part A). Changes in memory and/or concentration (brain fog), changes to mental health and sleep disturbance, and joint pain were the symptoms most commonly reported as unexpected (Figure 2, Part A). The majority of participants (52.3%) reported that their symptoms, overall, had been much more intense than expected (Figure 2, Part B).

Menopause symptoms experienced by participants. Part A shows the number of participants who reported each symptom and number of participants who experienced this symptom as a surprise. Frequencies are out of the 497 participants who completed the question, with values expressed as percentages in brackets. Part B shows whether overall menopausal symptoms were more or less intense than expected (answered by all 508 participants).
On a scale from 0 (not difficult at all) to 100 (extremely difficult), participants who responded to this question (n = 485) rated their symptoms at 66.8 on average (SD: 25.03, median 71, range 0–100). Correlation analysis revealed that individuals who reported more numerous unexpected symptoms rated their menopause as more severe (r = .18, p < .001). Similarly, those who said they knew what to expect when their menopause symptoms started tended to rate their symptoms as significantly less severe on average (55.5, SD: 27) than those who said they did not know what to expect (71.4, SD: 22.5; F (1, 457) = 35.44, p < .001). Similarly, individuals who did not know they were Autistic at menopause (54%) tended to rate their menopause symptoms as more severe on average (70.49, SD: 24.31) than did those who knew they were Autistic at menopause (62.28, SD: 24.96; F (1, 474) = 13.12, p < .001).
Many struggle to access appropriate information and menopause support
When asked about whether they had sufficient information about menopause before and during the menopausal transition, the majority said no (211); 151 felt they did have sufficient information overall, while 105 were unsure and 41 did not respond. The most common source of information about menopause was the internet (indicated by 357 participants); other sources included healthcare professionals (143 participants), family or friends (121 participants), online autism (70 participants) or menopause (58 participants) support groups (13 participants reported accessing information through in-person forms of each). Participants also indicated they did not have enough information about specific topics during menopause, which is ranked in Figure 3. The impact of menopause on Autistic traits was the most common topic about which participants indicated they did not have enough information (n = 430), followed by autism-related aspects of menopause (n = 424), and mental health effects of menopause (n = 370).
Information desired by Autistic people at menopause. Types of information are ranked by the number of participants who indicated that they would have liked more information of that type. Displayed for comparative purposes are the number of participants who indicated that they had enough or did not need information on that topic. Frequencies are out of the 508 participants who completed this question, with values expressed as percentages in brackets.
When asked about whether they had accessed any professional support at menopause, of those who responded (n = 508), some participants accessed support from public (141) or private (98) healthcare services. Some sought help from mental health professionals like counsellors, psychologists or therapists (97). A smaller number accessed support from organizations associated with menopause (36), mental health (22), or autism (26). Some participants (n = 173) reported not having received professional support, although this response did not differentiate between those who had wanted help and tried to access it, and those who had not.
Qualitative analysis
The team arrived at five themes and 14 subthemes as outlined below and depicted in Figure 1.
Theme 1: mind the gaps: knowledge, information, and representation
I was overwhelmed by my symptoms because I was not prepared or properly informed about the symptoms of menopause and the side effects of the medications in HRT. I also realized that I had to do extra research to fully understand my situation because most of the health care providers I have encountered were also limited in their knowledge and resources in providing the optimal solution to my problems. (42-year-old East/Southeast Asian woman from Germany in post-menopause who did not know she was Autistic at menopause onset, age 34).
Participants explained how identity factors like gender impacted menopause; one participant who identified as non-binary commented, “the gendered nature of pretty much all existing information is jarring and disappointing” (47-year-old white, gender-non-binary participant from Australia in perimenopause who did not know they were Autistic at age of menopause onset, 45). Others noted additional intersectional factors that affected experiences and accessibility of support, including culture, ethnicity, language, and socioeconomic status:
“The NHS case studies were always annoyingly chirpy, well-off people I couldn’t relate to.” (63-year-old white woman from the UK in post-menopause who did not know she was Autistic at the age of menopause onset, 46).
Theme 2: struggles with well-being
Some participants experienced challenging physical symptoms like weight gain and irregular bleeding; others struggled with interoceptive awareness, executive functioning, cognition, sleeplessness, and communication, which in some cases, “…contributed to a stricter adherence to routine due to ‘brain fog'/confusion” (39 year-old white woman from the UK in post-menopause who did not know with certainty she was Autistic at menopause onset, age 35).
Adding to confusion over symptoms, many participants described co-existing mental and physical health conditions, and other forms of neurodivergence. Some noted rage, anger, stress, anxiety, emotional volatility, and difficulty with emotional and physical regulation, burnout, and suicidality.
While some mentioned that they had to rely more on family or friends, others experienced breakups and family bereavement: “…during this period, my marriage broke up, COVID hit, and both my parents died. That makes it difficult to attribute issues like mental health problems to menopause, but it definitely didn't help” (52-year-old white woman from Ireland in post-menopause who knew she was Autistic at menopause onset, age 49). Others described the loss of a sense of identity, fertility, libido, and social status, and felt the impacts of being seen differently by other people, due to ageing and a perceived decline in physical attractiveness. Some participants expressed feeling a sense of grief and loss.
Theme 3: getting stuck: barriers to accessing health care and support
My GP [General Practitioner] refused to believe my perimenopausal symptoms and also refused to believe me about the Autism as well. If I had known more, I could have been more assertive about this and provided information, instead of the long drawn-out process I had to endure (47-year-old white woman from the UK in perimenopause who did not know she was Autistic at menopause onset, age 42).
Some participants reported that they had been ignored, misdiagnosed, denied services, or offered inappropriate or restricted treatments. They noted the dire effects of their mistreatment by healthcare professionals and the extension of neuronormativity and misogyny into the medical context: “Most of the negative treatment I got was down to the normal attitudes in our society towards menopausal women. We are seen and treated as less than. The autism tipped this ‘less than’ attitude into something far more dangerous…” (55-year-old woman of mixed, white non-European heritage in post-menopause who knew she was Autistic at menopause onset, age 52).
Some doctors refused to believe that perimenopause had started: Was told I was too young (i.e., under 45) so perimenopause was not considered despite multiple symptoms. I was only taken seriously when I demanded to be listened to. This made me feel uncomfortable, and frustrated that I had to put myself in such an unpleasant situation before I was listened to (44-year-old white woman from the UK in perimenopause who knew she was Autistic before menopause onset, age not specified).
Participants found that physical, structural, economic, attitudinal, and environmental barriers restricted access to healthcare services and diagnosis. As a result, some participants described avoidance of medical support and treatment.
Similarly, not understanding what was happening with confusing or unknown symptoms, lack of interoceptive awareness, and not knowing about available services or treatments made it harder for participants to ask for help. The requirement to contact a medical centre by telephone was also noted as a barrier.
Theme 4: going it alone
Theme 5: a catalyst for healthy change
Some also made adjustments to make their lives less stressful and tiring, such as changing jobs, working more from home, spending time alone, ending unhealthy relationships or setting boundaries. Some made positive changes by finding Autistic community through social media; exercise; creative work; support from family and friends; yoga, Pilates, Tai Chi, and meditation; spending time in nature; gardening; medication, hormone replacement, or supplements; and learning more about menopause.
“
Discussion
In this international survey, we explored the menopausal experiences of Autistic people on a larger scale than earlier research. While aiming to corroborate previous descriptions of symptoms experienced at menopause and their impact, we also explored the relationship between menopause difficulty ratings and participants’ awareness of menopause and of their autism. We built on previous work by exploring unmet support and information needs and barriers to access them, as well as participants’ coping strategies.
Information gaps
As in previous qualitative work related to Autistic people (Brady et al., 2024; Karavidas & de Visser, 2022; Moseley et al., 2020, 2021) and those with other or additional forms of neurodivergence (Dorani et al., 2021; Gottardello & Steffan, 2024; Kooij, 2023; Wasserstein et al., 2023), many of our Autistic participants found menopause to be an extremely difficult transition with the overlap of neurodivergence, mental and physical health challenges. The symptoms most commonly reported by participants were those associated with the aforementioned neurological nature of menopause (Brinton et al., 2015): changes in memory and concentration span (brain fog), changes in mental health, and disturbed sleep; symptoms that were described as unexpected (‘a surprise’) by 62.2%, 59.8% and 47.2% respectively of participants who experienced them. This fits with other reports, where for neurodivergent people broadly, these neurological symptoms loom larger than physical ones (Gottardello & Steffan, 2024). While hot flushes were the fourth most common symptom experienced by our participants, they were unexpected for only 2.8% of participants who experienced them. While corroborating that Autistic people are typically aware of this stereotypical symptom (Moseley et al., 2021), our analysis demonstrated knowledge gaps around certain symptoms which are less commonly experienced but which, due to their neurological nature, might cause considerable impairment for those with neurological differences. Similarly, the qualitative theme “Mind the Gaps” indicated that information about menopause would be more accessible if it reflected more diverse accounts, namely neurodivergent and non-gender binary perspectives and less commonly- known symptoms.
Previous research in the general population indicates a correlation between poorer menopausal awareness and symptom severity (Harper et al., 2022; Huang et al., 2023; Richard-Davis et al., 2022; Süss & Ehlert, 2020), and previous studies in Autistic people suggested that poorer awareness might make the transition more difficult (Brady et al., 2024; Moseley et al., 2021). Our Autistic participants who reported more numerous unexpected symptoms tended to rate their menopause as more difficult overall, as did those who indicated a general lack of awareness of what to expect when perimenopause started. Detrimental impacts of lack of menopause awareness also emerged in the qualitative data. Beyond knowledge of menopause symptoms, many participants indicated that they had entered menopause unaware of how it might affect them as Autistic people. In the quantitative data, “impacts of menopause on autistic traits” and “autism related aspects of menopause” were the two topics about which most participants reported not having enough information. Critically, 54 percent of participants entered menopause unaware of their autism, and these individuals tended to rate their menopause as more difficult overall.
These findings corroborate and extend previous suggestions (Brady et al., 2024; Moseley et al., 2021) that, for Autistic people, and possibly neurodivergent individuals more broadly, prior knowledge about menopause and about neurodivergent-specific aspects of menopause is crucially important; the latter, of course, is contingent on awareness of your own neurodivergence. While the qualitative data indicate lack of general menopause awareness and lack of Autistic menopause awareness as barriers to coping with menopause and seeking help, the importance of menopause and autism knowledge is clearly evidenced by the ways that Autistic people coped with menopause. Participants indicated the crucial importance of preparedness and advance planning, and how awareness of their autism had helped them find social support, develop appropriate coping strategies and self-compassion—in other words, to cultivate factors linked with resilience during menopause (Süss & Ehlert, 2020; Zhao et al., 2019). Just as a later-in-life autism realization can facilitate self-compassion and a more positive social identity (Gellini & Marczak, 2023), it appears to have important implications for health and well-being at menopause.
Implications for support and coping
Our quantitative and qualitative data were informative with regards to where participants tried to access information and support, and the barriers they faced. While proportionately few participants had sought help from private and public healthcare sectors (19.3% and 27.8% respectively), qualitative data corroborate the many healthcare barriers Autistic people face, including lack of physician training, infrastructural issues, and time constraints (Corden et al., 2022; Doherty et al., 2022; Zerbo et al., 2019). They also corroborate difficulties for Autistic women and AFAB people in accessing healthcare during menopause (Brady et al., 2024; de Visser et al., 2024; Moseley et al., 2021), as well as, perhaps, broader inconsistencies in the menopause awareness and attitudes of healthcare practitioners (Armeni et al., 2022; DePree et al., 2023; Martin-Key et al., 2023). As in previous studies (Brady et al., 2024; Moseley et al., 2021), some participants in our study indicated that their healthcare providers had neither recognized nor believed them about their perimenopausal symptoms; some related this to a broader disregard for women's healthcare and lack of medical training around autism. The inaccessibility of healthcare reported by our participants may have been exacerbated by what Shaw et al. (2024) describe as the “triple empathy” problem. Some participants felt that they were not believed in clinical settings and found it difficult to communicate there.
The feeling of not being believed in menopause appeared to add to feelings of being misunderstood by non-Autistic people in general. A substantial number of participants received no support at all during menopause: some participants had no friends or family to turn to, while others felt more socially isolated and different during perimenopause. Our findings reinforce the importance of validating Autistic identity and experiences in making information accessible for Autistic people (Stenning, 2024), while recognizing crucial intersections such as gender identity (Glyde, 2022) race (Richard-Davis et al., 2022), and additional forms of neurodivergence (Craddock, 2023).
Despite the many difficulties reported by participants, several also described resilience and coping mechanisms. Some reported Autistic flourishing (Pellicano & Heyworth, 2023), or a sense of self determination and self compassion that came with understanding of their autism. Feelings of liberation – from periods, from caring what others thought – were described by some participants. Some of our participants found lifestyle changes (e.g., diet, exercise, at work and in relationships) helpful as a means of coping with menopausal symptoms and stress. Other strategies identified as helpful included creative expression; time spent in nature or in activities like gardening, meditation or yoga; connection with family, friends, and other Autistic people; and researching menopause. Notably, these are strategies corroborated by other samples of non-menopausal Autistic people (Ghanouni & Quirke, 2023), who highlight the importance of recreation and leisure time in their daily routines; seeking and receiving emotional support; and learning about their needs and triggers as a means of being better able to self-advocate (Chen et al., 2024).
Despite this reported resilience, we wish to highlight the following implications. Representation of different neurotypes and gender identity is essential in making information about menopause more accessible. Moreover, while many Autistic and non-Autistic individuals feel unprepared for menopause (Brady et al., 2024; Harper et al., 2022; Moseley et al., 2021; O'Reilly et al., 2022), better information about common and less-common symptoms and possible treatments may promote a sense of control for Autistic people, which is linked to general well-being in menopause (Süss & Ehlert, 2020). In addition to improving clinical recognition of autism in individuals of all ages, clinicians should be trained to appreciate differences in Autistic communication style, in order to avoid the “triple empathy” problem (Shaw et al., 2024) and even the “quadruple empathy” problem related to other intersections (Brady et al., 2024) in healthcare settings.
Strengths and limitations
This study was the first of its kind to include a broad international Autistic population, and adds to growing knowledge about unique Autistic challenges during menopause. It also assumed an inclusive model (Chown et al., 2017; Fletcher-Watson et al., 2019) where Autistic people fundamentally shaped and conducted the research. Nevertheless, there were several limitations.
As this study aimed to follow lines of enquiry posed by Autistic people (Brady et al., 2024), most notably around gaps in information and support and experiences of coping and resilience, our approach focused on the qualitative questions which would best address these questions. Our quantitative approach was subsequently less detailed, and interpretation was limited by question phrasing. For instance, while Autistic people who reported fewer unexpected symptoms typically rated their menopause as less difficult overall, we are unable to interpret this finding in relation to factors underpinning both menopause awareness and symptom severity (e.g., access to healthcare and social support). Similarly, while our data suggested that the 46 percent of participants who knew about their autism prior to entering menopause had a slightly easier time, this finding may be compounded by factors such as age (with participants who were older at the point of this study less likely to have been identified before menopause) (O’Nions et al., 2023); relatedly, older individuals might be more likely to be post-menopausal, and retrospective reporting affects attitudes about menopause (Brown et al., 2018). Broadly speaking, relationships between knowledge and attitudes about menopause and experience of menopause would benefit from more detailed approaches than those allowed by our proxy measure of menopause awareness. This might be especially important in Autistic people, given previous indications that some Autistic people are clearly aware of the symptoms that menopause entails, but are nevertheless surprised by the intensity and severity of their impact, and sometimes struggle to recognize these symptoms when they occur (Moseley et al., 2021). There is a clear gap between factual awareness of symptoms vs. recognition and understanding of symptoms which our proxy measure could not capture, and which might be related to interoceptive awareness, a known difficulty for Autistic people (Trevisan et al., 2021). As a possible moderator of how Autistic people experience their symptoms, this is a worthy target for further research.
Indeed, we have no way of knowing whether menopausal difficulties experienced by our participants could be related to other factors than being Autistic. Other factors of possible importance in moderating menopause experience are menopause stage, gender identity and country of residence (both of which might affect access to support), the presence of co-occurring health conditions and other forms of neurodivergence, particularly given the additional challenges associated with being Autistic with co-occurring ADHD (Craddock, 2023). While we did not statistically compare or explore thematic differences between participants in relation to these factors, we highlight them for future research. Differences in menopausal experience between early- and late-diagnosed individuals are also important to explore in greater depth than the preliminary statistical approach adopted here. We suggest that, alongside more rigorous statistical designs, interdisciplinary approaches may also contribute greater depth of understanding to the experiences of Autistic people at menopause (Matthews et al., 2024).
Our online approach precluded independent validation of autism diagnoses or menopausal stage, and prevented participation of Autistic people with intellectual disabilities or who may not be able to type or dictate responses in English. Minority ethnic groups, transgender and non-binary people were under represented. Finally, people who had negative experiences of menopause may have been more likely to participate, and the design of our survey, informed by earlier phases of our research, may have evoked a bias towards negative responses.
Conclusion
In the largest study on menopause in Autistic people to date, we aimed to understand the relationship between menopause difficulty and participant awareness of their menopause and autism; the kinds of information needed by Autistic people at menopause; barriers to help and support; and Autistic resilience and coping tactics. Findings support the importance of menopause and autism awareness, and the need for accessible and inclusive Autistic-specific information about menopause. Access to more appropriate and earlier awareness, and better help and information could increase Autistic flourishing during the menopausal transition.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330241299366 - Supplemental material for “Struggling for Years”: An international survey on Autistic experiences of menopause
Supplemental material, sj-docx-1-ndy-10.1177_27546330241299366 for “Struggling for Years”: An international survey on Autistic experiences of menopause by Christine A. Jenkins, Rachel L. Moseley, Rose J. Matthews, Margaret Janse van Rensburg, Julie M. Gamble-Turner and Miranda J. Brady in Neurodiversity
Footnotes
Acknowledgements
The authors wish to thank their Autistic participants for their generosity with their time and insights, as well as five beta testers who helped us refine our survey. We would also like to thank the Social Sciences and Humanities Research Council of Canada for funding which made this research possible.
Author contributions
Joint First author CAJ: conceptualisation (lead); funding acquisition (equal); investigation (equal); methodology (support); writing original draft (equal); writing—review and editing (equal); resources (lead). Joint First author RLM: conceptualisation (equal); funding acquisition (equal); data curation (lead) formal analysis (lead); investigation (equal); visualisation (lead); writing original draft (lead); writing—review and editing (lead); Author 3 (RJM): conceptualisation (equal); investigation (equal); formal analysis (lead); methodology (lead); writing—review and editing (support); visualisation (equal); resources (lead); Author 4 (MJVR): conceptualisation (equal); data curation (lead); investigation (equal); methodology (equal); formal analysis (support); writing—review and editing (support); Author 5 (JGT): conceptualisation (equal); funding acquisition (equal); formal analysis (equal); writing—review and editing (equal); Author 6 (MJB): conceptualisation (lead); funding acquisition (lead); investigation (equal); methodology (equal); formal analysis (equal); writing original draft (equal); writing—review and editing (equal); supervision (lead); project administration (lead); resources (lead); software (lead). CAJ = Christine A. Jenkins; JGT = Julie Gamble-Turner; MJB = Miranda J. Brady; MJVR = Margaret Janse van Rensburg; RJM = Rose J. Matthews; RLM = Rachel L. Moseley.
Availability of data and materials
Unfortunately, data cannot be made publicly available. However, further information about the overall project, of which this is one part, can be found on the project website, ‘Bridging the Silos: Autistic Menopause Study'.
Consent to participant and consent to publish
Participants were fully informed about the nature and content of the study, and all gave consent to participant. Participants also consented to publication of the anonymous data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The study was reviewed and approved by the Ethics Panel at Carleton University. It was performed in accordance with the ethical standards set out in the 1964 Helsinki Declaration.
Funding
The study was funded by an Insight Development Grant from the Social Sciences and Humanities Research Council of Canada (# 430–2021-00664).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.