
Abstract
Evaluate and compare the efficacy of pharmacological and psychosocial interventions on work-relevant outcomes, such as time management and productivity, for adults with attention deficit hyperactivity disorder. A meta-analysis that searched 12 databases. Included studies had a control group and an outcome measure related to workplace functioning or addressing time management/organization. Studies included intervention groups with 52% men and a mean age of 33.2 years. We evaluated studies using the random effects model and summarized standardized mean difference. We assessed sensitivity, publication bias, and risk of bias. We evaluated the efficacy of 23 studies, including 3835 participants. Overall, pharmacological (d = .19) and psychosocial (d = .56) interventions were more efficacious at improving work-relevant outcomes than control. Treatment with Methylphenidate was the only robust effect comparing the pharmacological interventions. For psychosocial interventions, cognitive behavioral therapy showed the most robust effect. There was evidence of heterogeneity; hence, findings need to be interpreted with caution. Findings suggest that combining pharmacological and psychosocial interventions may be useful for improving work-related outcomes. However, we contend that these need to be designed with transferability to the workplace in mind. For example, improving organization skills in workplace settings.
Lay abstract
What is already known about the topic?
It is well known that medication for adults with ADHD (ADHDers) works to improve attention and reduce hyperactivity or impulsivity. Research has also investigated what kinds of psychological interventions help ADHDers and has shown that cognitive behavioral therapy works to improve and reduce the same symptoms. Less is known about what kinds of interventions (medical or psychological or both) are helpful for challenges ADHDers experience in the workplace. Examples of these challenges are concentration, time management, and organization.
What this paper adds?
We wanted to compare the research already conducted to investigate whether medical or psychological interventions work better when assessing the impact on work-relevant outcomes like the challenges described above. We predicted that psychological interventions such as cognitive behavioral therapy and coaching may be better for targeting workplace challenges compared to medication because the skills you learn in these interventions are easily transferred to workplace settings.
Implications for practice, research, or policy
There needs to be more research looking at support for ADHDers in the workplace that is workplace relevant. A combination of medication and psychological support is recommended based on these findings.
Introduction
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental condition that is diagnosed through the assessment of core symptoms including inattention, hyperactivity, and impulsivity (American Psychiatric Association, 2013). Attention Deficit Hyperactivity Disorder impacts the lifespan and all domains of adult life (Epstein & Loren, 2013). To receive a diagnosis of ADHD, the symptoms must be present in two or more domains, one of which is likely to be the workplace for adult populations. Adults with ADHD (ADHDers)1 are more likely than those without ADHD to have poorer work-related well-being and performance that leads to burnout, longer absences, and an increased risk of being fired (Adamou et al., 2013; Brattberg, 2006; Gjervan et al., 2012; Lasky et al., 2016). Workplace challenges for ADHDers extend beyond the core symptoms, with the main challenges being time management, organization, and distractibility (Coetzer, 2015; LaLonde et al., 2013; Santuzzi et al., 2014). Therefore, interventions in this realm must address the breadth of challenges, beyond the core symptomatology, to enable ADHDers to succeed in the workplace and beyond.
Interventions or treatments documented in the literature that are aimed at adults with ADHD can be grouped into three categories: assessment of the efficacy of medical treatments (here referred to as pharmacological interventions), providing psychological treatments (or here referred to as psychosocial interventions), and evaluating a combination of the two. An important difference when examining these categories of interventions is that typically medical treatments are designed to reduce the core symptoms, whereas psychological treatments are aimed at improving mental health. When combined, a more holistic approach is adopted. Systematic reviews and meta-analyses comparing the effectiveness of pharmacological and psychosocial interventions largely focus on the reduction in the core symptoms. However, one exception suggested that psychosocial interventions may be more efficacious than pharmacological interventions for improving aspects beyond the core symptoms, such as quality of life and emotional regulation, due to the applicability of learned strategies and skills to other life domains (Moriyama et al., 2013). This can be explained through theories of training transfer where it is easier to transfer new skills learnt in similar contexts to other similar contexts, near transfer, and training designed to teach more generalized skills can be transferred to dissimilar contexts, far transfer (Sala et al., 2019). For example, the skills taught in psychosocial interventions, like managing anxiety, are easily transferred to other domains beyond the intervention such as everyday tasks. In contrast, pharmacological interventions lack an element of learning new skills that make understanding the effectiveness of medication and the transfer to contexts difficult to assess. Given that learning often involves near and far transfer, psychosocial interventions may be more relevant and effective than pharmacological interventions for ADHD-related workplace challenges. The former interventions may be superior because they are targeted and designed with workplace challenges in mind, which makes it easier to transfer what is taught in the intervention to the workplace. Yet, to the best of our knowledge, there are no meta-analyses that evaluate the efficacy of interventions on work-relevant outcomes and/ or contexts, and there is minimal research evaluating workplace interventions for ADHD more generally (Lauder et al., 2022). Therefore, our review aims to evaluate the relative efficacy of pharmacological and psychosocial interventions on work-relevant outcomes.
Consequently, our research questions are:
How many intervention studies have been published regarding (i) pharmacological, (ii) psychosocial, and (iii) combined for ADHD in a work context? Where has any such evidence been published and what is the relative strength of evidence? Are psychosocial interventions more effective than pharmacological interventions for ADHDers given the inherent capacity to equip individuals with transferrable skills?
Method
Eligibility criteria
Included studies primarily evaluated either a pharmacological intervention or a psychosocial intervention for adults (above 18 years old) with a formal diagnosis of ADHD, as diagnosed by the Diagnostic and Statistical Manual of Mental Disorders 3, 4, or 5. Studies had to include a control or comparison group in their evaluation and be written or translated in English. We placed no limits on the date of publication and completed our search in 2022.
Outcome measures
To meet our aim, we included outcome measures that were work relevant and we defined this as any measure of organization or time management, the most common challenge for ADHDers at work, or a measure relevant to work functioning and quality such as work productivity, satisfaction, or performance. We included measures that had subscales that met our criteria so long as the study provided data on these subscales rather than an overall score. There were 13 measures in total, those that assessed organization or task-related outcomes included: Adapted Child Organizational Skills Measure, Behavior Rating Inventory for Executive Function – Adult version, On Time Management, Organization, and Planning Scale, Organization and Activation for Work, Strategies for Success, and the Wender–Reimherr Interview. Those that measured work functioning were: Adult ADHD Quality of Life, Canadian Occupational Performance Measure, Endicott Work Productivity Scale, The Quality-of-Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q/Q-LES-Q-SF), Sheehan Disability Scale, Work and Social Adjustment Scale, and the Work Limitation Questionnaire. Examples of organization items include questions about completing to-do lists and using planners whereas items that measured workplace functioning asked about the person's ability to perform work tasks and satisfaction with work life. Details of these measures and example items are displayed in Table 1.
Work-related outcomes: Details of the measure, purpose, variations, items, and responses.

Search strategy and study selection
We used the following search terms to select studies that met our inclusion criteria: Adult ADHD, Adult ADD, Adult Attention Deficit Disorder, adults with ADHD, adults with ADHD, adults with ADD, adults with attention deficit disorder, and, intervention, treatment, management, program, counseling, coaching, therapy, trial, and training. We entered these search terms, with their variations, into 12 databases that included management, ADHD-specific, and medical journals. These databases included Academic search complete, ADHD Attention Deficit and Hyperactivity Disorders, Business source premier, Criminal justice abstracts, Journal of Attention Disorders, Library, information science and technology abstracts, PsycARTICLES, PsycINFO, MEDLINE, ProQuest Business collection, Scopus, and Web of Science. We additionally consulted an expert panel of practitioners who work with ADHDers to identify any recently published studies.
Studies were first screened by their title and abstract using EPPI reviewer software to manage the references (see Figure 1 for PRISMA diagram) (Page et al., 2021; Thomas et al., 2020). We then retrieved and screened the full texts against the inclusion criteria. A second reviewer independently screened 5% of the titles and abstracts from the search. The second reviewer then screened and checked 5% of the full texts for accuracy. Cohen's kappa was κ = 0.86 representing strong agreement between the two reviewers (McHugh, 2012). A third reviewer independently reviewed the full texts for inclusion and assessed the included studies for risk of bias with κ = .90 showing high agreement. The meta-analysis was not preregistered.

PRISMA diagram displaying identification of studies.
Data extraction
We extracted the following data from the included studies: the type of treatment, number of participants in both the experimental and control group, and the outcome measure used. For pharmacological interventions, we extracted the name of the drug and the dosage in administered in each group. In studies where outcome measures were taken at multiple time points, we extracted the data from the final time point measure and recorded time in weeks.
Risk of bias
We assessed risk of bias in line with the Cochrane Collaboration recommendations using the RoB 2 tool for randomized control studies and the ROBINS-I tool for nonrandomized control studies (k = 2) (Bueno et al., 2015; Edel et al., 2017). Each of the domains (selection, reporting, performance, and detection bias) was rated low, some concerns, or high risk of bias. For the nonrandomized control trials, selection and classification bias were evaluated instead of the randomization process. Any study that was rated as having some concerns in one domain was evaluated to have an unclear risk of bias overall (Higgins et al., 2011). An independent rater evaluated the risk of bias as well as the principal researcher; any disagreements were discussed until there was an agreement.
Data synthesis
Studies reported either the mean and standard deviation for both the control and the intervention group at preintervention and postintervention or they reported the mean change and standard deviation in each group computed as the postintervention mean minus the preintervention mean. For studies in which there were different doses of stimulants administered or different interventions, data were extracted at the dose/intervention level and analyzed this way. Effect sizes were calculated from the data extracted. Although some of the sample sizes were considered small, total sample sizes were all above 20 so we deemed Cohens d the most appropriate (Cooper, 2017; Ellis, 2010). When interpreting effect sizes, we considered the standard below 0.2 a small effect size, medium effect size for values above 0.5, and above 0.8 a large effect size (Cohen, 1988). The d values for each study are presented in Table 2. We used Comprehensive Meta-Analysis Version 3 (CMA) software to manage and analyze the data (Borenstein et al., 2009). Effect sizes were computed using the random effects model (Borenstein et al., 2009).
Included studies and their characteristics.

Pharma: pharmacological; Psycho: psychosocial; CBT: cognitive behavioral therapy; AAQoL: Adult ADHD Quality of Life questionnaire; AOSM: Adapted Child Organizational Skills Measure; BRIEF-A: Behavior Rating Inventory of Executive Function (Adult version); COPM: Canadian Occupational Performance Measure; EWPS: Endicott Work Productivity Scale; Q-LES-Q: The Quality of life enjoyment and satisfaction questionnaire; ON-TOP: On Time Management, Organization, and Planning Scale; OAW: Organization and Activation for Work; SDS: Sheehan Disability Scale; SFS: Strategies for Success; WSAS: Work and Social Adjustment Scale; WLQ: Work Limitation Questionnaire; WRI: Wender–Reimherr Interview.
We contacted authors of any studies that did not provide the necessary information to calculate the effect size was listed to request further details. In total, we contacted authors of four studies, none of whom responded with data. We, therefore, excluded these studies from our analysis.
Results
Description of studies
A total of 23 studies, published from 2002 to 2021, met the criteria for the meta-analysis (Table 2). We classified studies according to intervention type as assessing either the efficacy of a pharmacological intervention (k = 12) or a psychosocial intervention (k = 11). We excluded data that assessed the combination of pharmacological and psychosocial interventions due to there being too few studies (k = 2). The psychosocial interventions typically involved cognitive behavioral therapy (CBT) or mindfulness compared to the pharmacological interventions that administered a range of drugs classified as stimulants (Methylphenidate, k = 5), selective norepinephrine reuptake inhibitors (Atomoxetine, k = 4), antidepressants (Vortioxetine, k = 1), nonstimulants (Guanfacine, k = 1), and eugeroic (Modafinil, k = 1). We further categorized the psychosocial studies based on the type of intervention. The most common type of psychosocial intervention was CBT (k = 4) which included group CBT and online CBT, the other types were mindfulness (k = 3), cognitive training (k = 3), and group psychotherapy (k = 1).
Sample sizes ranged from n = 25 to n = 542 with 3835 participants included in total (M = 167, SD = 149). The mean age for intervention groups was 33.2 years with 1280 men and 1107 women. Ten studies reported ethnicity data with white people being overrepresented (ranging from 70% to 94% in nine of the studies and 47% in one study). Studies were published from 2002 to 2021; control group designs varied from placebo control groups in all pharmacological studies (k = 11) compared to control groups that involved an alternative therapy or medication (k = 4), treatment-as-usual (k = 4), or those that involved no treatment such as a waiting list (k = 5). In the pharmacological intervention studies, all but one study involved a control group that was either a placebo or waiting list compared to the psychosocial studies that included alternative therapies and treatments as usual. Hence, control participants in the psychosocial interventions were receiving some form of intervention. Such difference in control group designs is worth bearing mind for the interpretation of the meta-analysis findings.
We defined work-relevant outcomes as any measure of time management and organization or workplace functioning including work productivity, satisfaction, or performance.
Risk of bias
The risk of bias across the studies is displayed in Figure 2. A total of six studies met the criteria for low risk of bias with the remaining studies (k = 17) having some concerns in at least one of the five domains assessed. One study met the criteria for high risk of bias in the randomization domain because participants were randomized by the principal investigator hence indicating bias so in line with guidance the study was given an overall high-risk rating (Cherkasova et al., 2016). Comparing risk of bias for both pharmacological and psychosocial interventions, pharmacological studies all received low risk of bias for their randomization of participants with the majority including details of how the participants were randomized and whether the investigators were blinded to the conditions. Contrary to this, they were judged as having some concerns due to the missing data for participants, notably indicating large dropout rates. For psychosocial intervention studies, half were scored as having some concerns due to the outcome data being collected from unblinded assessors or through self-report. Therefore, it is uncertain whether participants realized the study intentions or which group they were in. A total of seven psychosocial studies were rated as some concerns in the deviation category due to limited detail or information about missing data and analysis (see Figure 3). It must be noted, however, that it was difficult to assess study quality for psychosocial studies because of the lack of description in methods sections and explanations of data analysis that may be a result of the variety in journal guidance and rules. For example, the Cochrane collaboration is primarily a health network that evaluates risk of bias based on medical science which is not always comparable to the quality standards of psychosocial studies.

Overall risk of bias for all included studies.
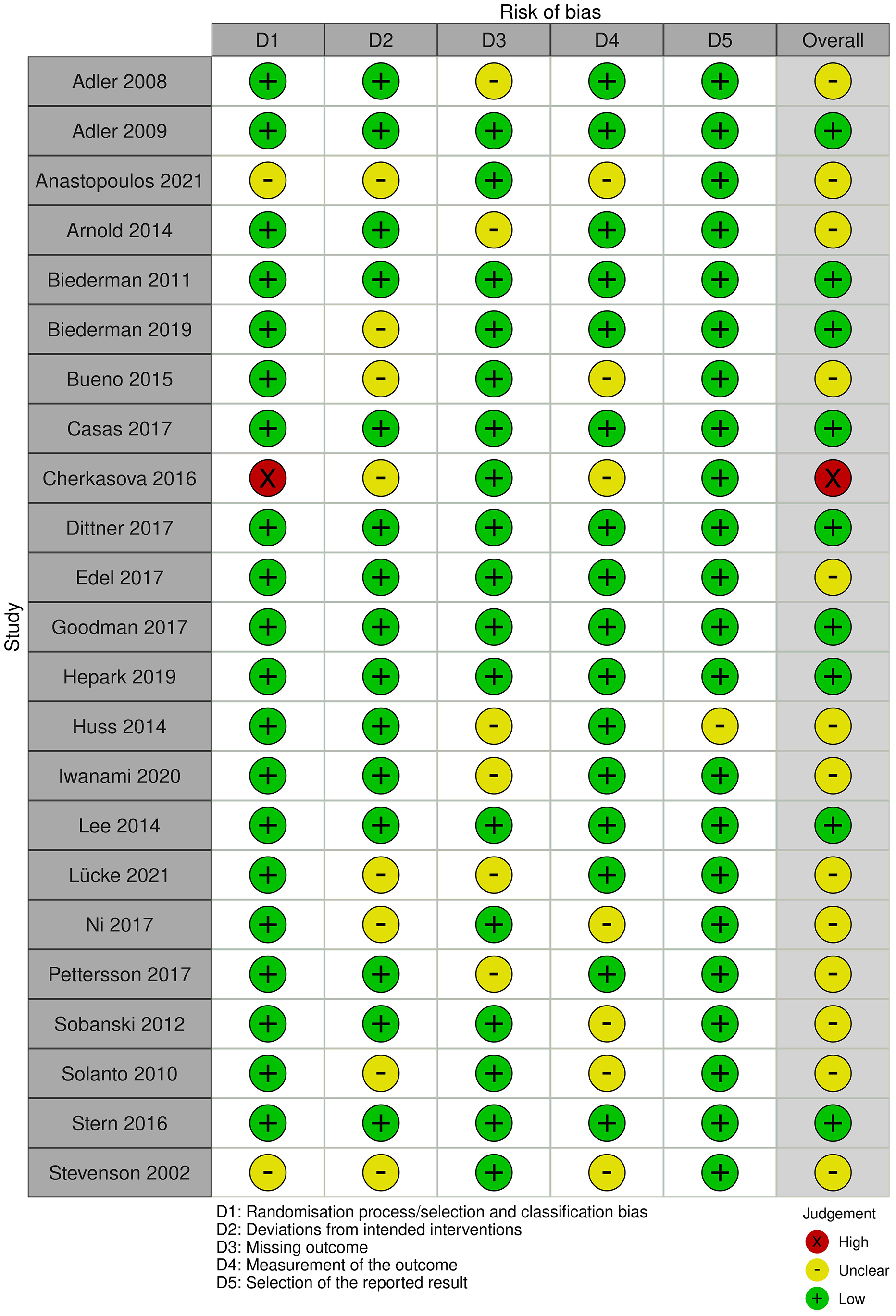
Risk of bias for individual included studies.
Overall intervention effect
The 23 studies had an overall weighted mean effect size of d = .30 (p < .001) with a 95% confidence interval from .20 to .40. The sample was heterogeneous, Q w (30) = 70.98, p < .001 with an I2 of 57.73%, indicating substantial variance (Higgins et al., 2003). Therefore, a moderator analysis was employed to examine any variance beyond sampling error (Lipsey, 2003).
Effects of pharmacological interventions
There was a significant overall effect size for pharmacological interventions, d = .19 (95% CI [.10–.29], p < .001). Heterogeneity was substantial I2 = 49.71%, Qw(18) = 35.79, p < .01. Therefore, we compared the medications separately, see Figure 4. Methylphenidate was the only pharmacological intervention to show robust effects d = .31 (95% CI [.21–.42], p < .001), with no observed heterogeneity, although this should be interpreted with caution due to the small sample of studies Qw(7) = 5.41, p = .61, I2 = 0% (Von Hippel, 2015). The following medications had small nonsignificant effect sizes with small to substantial heterogeneity: Atomoxetine d = .13, (95% CI [−.06, .31], p = .18, I2 = 26.03%), Vortioxetine d = .01, (95% CI [−.24, .25], p = .96, I2 = 1.71%), Modafinil d = .07, (95% CI [−.31, .44], p = .73, I2 = 79.08%). Guanfacine was examined in a single study so heterogeneity could not be determined there was a small nonsignificant effect size d = .23, (95% CI [−.05, .51], p = .10.

Forest plot of pharmacological studies.
Effects of psychosocial interventions
The weighted mean effect size for psychosocial interventions was medium d = .56 (95% CI [.40–.73], p < .001) and significantly different from the weighted mean effect size for pharmacological interventions Qw(1) = 14.43, p < .001. There was small nonsignificant heterogeneity Qw(11) = 14.39, p = .21, I2 = 23.55%. Studies involving CBT had the largest significant effect with no observed heterogeneity d = .65 (95% CI [.46–.83], p < .001, Qw(5) = 0.99, p = .96, I2 = 0%) compared to mindfulness where there was a large nonsignificant effect with substantial heterogeneity d = .79, (95% CI [−.05, 1.63], p = .07, I2 = 78.66%). The remaining effects were assessed on individual study effect sizes and only cognitive remediation had a large significant effect size d = 1.02 (95% CI [.36–1.68], p < .01). Meta-cognitive therapy (d = .42, 95% CI [−.02, .86], p = .06), group psychotherapy (d = .14, 95% CI [−.24, .52], p = .47), and cognitive training (d = .34, 95% CI [−.18, .85], p = .20) had small to medium nonsignificant effect sizes (see Figure 5).

Forest plot of psychosocial studies.
Publication bias and sensitivity analysis
To assess for publication bias, a visual examination of the funnel plot was carried out followed by the application of the Trim-and-Fill technique (Duval & Tweedie, 2009; see Figure 6). The visual analysis of the funnel plot found asymmetry of the studies toward the mean. An application of the Trim-and-Fill technique allows for the removal of the extreme studies from either the negative or positive side of the mean. In the current meta-analysis, the trim-and-fill method suggested seven theoretical missing studies and adjusted the effect size from d = .30 to d = .21 (95% CI [.11–.32]). Further analysis of Orwin's (1983) Fail-safe N calculated that a total of 55 studies would need to exist for the observed effect to be no longer statistically significant. There was a nonsignificant negative correlation between sample size and effect size, rs (23) = −.36, p = .09. A sensitivity analysis was further conducted to examine the effect size if each study was removed (Borenstein et al., 2009). The standardized mean effect sizes ranged from Cohen's d = .28 (95% CI [.18–.37], p < .001) to d = .32 (95% CI [.22–.41], p < .001) after Anastopoulos et al. (2021) and Arnold et al. (2014) were removed, respectively. Thus, the effects remained statistically significant during the sensitivity analysis.

Publication funnel plot.
Discussion
The search of the literature for included studies in the meta-analysis revealed a lack of intervention studies targeted at adults with ADHD assessing outcomes relevant to a workplace context or designed specifically for work. We identified 23 studies that assessed the efficacy of pharmacological and psychosocial interventions on work-relevant outcomes such as time management, organization, and workplace functioning. Nearly all studies (k = 20) were conducted in outpatient clinics or other clinical sites and published in psychiatry or medical journals demonstrating the dominance of the medical research into supporting adult ADHD. Due to rigorous medical research guidelines for high study quality, many of the studies scored low on risk of bias, those that indicated some concerns tended to be because of the lack of detailed methodology or explanations around missing data rather than clear evidence of bias.
Overall, the meta-analysis identified a small overall effect for interventions improving work-relevant outcomes compared to control. Our comparison of the effect sizes between pharmacological and psychosocial interventions indicated that the effect size for psychosocial interventions, particularly CBT, was significantly larger than the effect size for pharmacological interventions when both were compared to control conditions. The transferability and applicability of the skills developed during psychosocial interventions to the workplace is a possible explanation. For example, nearly all psychosocial interventions provided ADHDers with tasks in their training that focussed on improving time management. The strategies taught during these trainings are directly associated with coping with the key challenges ADHDers experience in the workplace (Coetzer & Gibbison, 2016). Therefore, supporting the existing literature on near and far transfer whereby learning is best transferred between similar contexts (Kim & Lee, 2001). We then looked at psychosocial interventions more closely to attempt to identify key mechanisms that may be most effective (Lukens & Mcfarlane, 2004). We define mechanisms like “active ingredients” that explain how and why the intervention can lead to the desired outcome (Dalkin et al., 2015). One mechanism that was evident in six of the studies was psychoeducation, learning about ADHD and how it impacts cognition and behavior (D’Amelio et al., 2015). Psychoeducation can then shape interventions to be more personal, developing specific skills related to specific challenges, and even involving people from the ADHDers network in the knowledge sharing (Seery et al., 2022). Gaining a deeper understanding of ADHD that is personal to a person's lived experience can utilize far-transfer learning and be applied to a variety of contexts. Hence, why it may be an effective mechanism in psychosocial interventions and improve work-relevant outcomes. However, more research is required that evaluates the role of psychoeducation in interventions to establish an evidence base to support these findings.
Our findings additionally indicate that Methylphenidate has a small but significant effect on work-relevant outcomes. The effectiveness of Methylphenidate in reducing the core symptoms of hyperactivity and inattention is well established in the medical literature. Therefore, the impact on general life domains, including aspects like workplace productivity, is unsurprising due to the improved concentration and reduced distractibility.
However, our conclusions need to be interpreted with caution due to the small number of studies included in the analysis, variety of intervention types, evidence of publication bias, some risk of bias, and heterogeneity in the results.
Limitations
The main limitation of the meta-analysis is the small sample of primary studies included. Despite an extensive search of the literature, studies that assess the efficacy of interventions for adult ADHD tend not to assess primary or secondary outcomes related to the workplace which limits the generalizability of the findings. Indicators of publication bias showed there was a high likelihood of publication bias in the sample, which is reflected in the findings of no studies from grey literature as mentioned. Publication bias is particularly difficult to reduce but needs to be addressed especially when involving studies that are used as part of evidence-based recommendations for practice. Furthermore, there was high risk of bias for one study and unclear risk of bias overall for 13 of the studies indicating that future research should aim to be clearer in their methodology around randomizing participants and selecting outcome measures.
When examining the types of interventions and outcome measures, there was variation in psychosocial interventions, such as the differences in mechanisms for cognitive training and online CBT, leads to challenges with generalizing the findings. Another is that a combination of both pharmacological and psychosocial interventions is likely to be effective, but there is a lack of research examining the effectiveness of these. Similarly, there was a wide variety of measures employed to assess workplace functioning. Therefore, there is a clear need for more robust research that assesses the efficacy of interventions for adult ADHD, including workplace outcomes with clear methodology and research design. It is important that interventions are designed with transferability to the workplace in mind, so that domain-specific transferrable skills are developed and scaffolded.
Another limitation is that ADHDers in pharmacological interventions may have differed from those in psychological interventions. For example, they may have been prescribed medication because they displayed visible signs of ADHD during any diagnostic or healthcare process whereas others may go unnoticed. One limitation of meta-analysis is that when comparing across studies, we cannot make causal arguments because participants cannot be randomly assigned to the study (Bornstein et al., 2009).
A final limitation of the studies is the outcome measures themselves. These significantly varied and we were unable to access example items for six of the measures to confirm our categorizations of either workplace functioning or time management/organization. Hence, the constructs themselves vary. Of the information we did collect about the outcome measures, they often demonstrated poor psychometric properties for example, we were unable to locate reliability coefficients for three of the studies and others had poor internal consistency. Furthermore, nine were self-reported measures which give rise to potential discrepancies or recall bias in reporting challenges and uncertainty to confirm or compare scores with other informants such as clinicians or educators (Garnier-Dykstra et al., 2010; Johnson & Suhr, 2021). These findings indicate a need for reliable and valid workplace measures that can be used to evaluate interventions and use a combination of sources beyond self-report.
Future research
The small number of studies in the meta-analysis highlights the need for more research on workplace interventions for ADHDers that combine medication like Methylphenidate with psychosocial intervention. With estimates of around 3.5% of the workforce screening positive for ADHD, it is vital that there is an evidence base of effective support and strategies that target work-related challenges associated with ADHD. Our meta-analysis additionally emphasizes the need for valid and reliable measures of workplace outcomes such as time management and organization to support with the evaluation of workplace interventions. Future work could also explore psychoeducation as a potential effective mechanism in ADHD-related interventions whereby an ADHDer learns about their ADHD, includes members of their social network, and has the autonomy to focus on developing strategies related to their specific challenges and experience. Building on this, coaching is an example of an intervention that was not evaluated in the meta-analysis but has been shown to include personalized strategies, psychoeducation, and be effective for other neurodivergent conditions such as dyslexia (Doyle & McDowall, 2019). More research is needed to investigate coaching as a potential avenue for support for ADHDers in the workplace.
Conclusion
Our findings highlight the gap in research and literature on workplace interventions for adults with ADHD. We conclude that while there is evidence that Methylphenidate is effective at improving work-relevant challenges, it should be combined with psychosocial interventions such as CBT, to include mechanisms like psychoeducation, to be most effective for outcomes such as organization/time management and functioning at work. Our findings highlight the need for future research to focus on evaluating interventions designed for workplace challenges, implemented in workplace settings, and assessed for effectiveness using valid and reliable work-relevant measures.
Footnotes
Acknowledgments
The authors wish to thank the members of the expert panel for their knowledge and advice and Sherilyn Dawson for assisting in reviewing articles for risk of bias.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge funding through the Birkbeck Wellcome Trust Institutional Strategic Support Fund, award 204770/Z/16/Z, which supported a 3 months period for the writing up and refinement of the current meta-analysis.