
Abstract
The monotropism hypothesis posits that hyper-focus on interests is core to autistic cognition; moreover, hyper-focus is common in attention dysregulation hyperactivity development (ADHD). However, ADHD is partly defined by susceptibility to distraction, and research has found evidence of attention capture in autism. We investigated hyper-focus in autism and ADHD, its relationship to inattention, and whether it is related to quality of life, hypervigilance, negative repetitive thinking, and symptoms of anxiety and depression. 492 adults (122 ADHD-only, 130 autistic-only, 141 autistic + ADHD, and 99 comparison) completed questionnaires indexing hyper-focus in multiple domains, inattention, and the valence of their hyper-focus experiences. Hyper-focus and inattention were elevated in all neurodivergent groups, and were positively correlated, implying that atypical regulation of attention, sometimes manifesting in hyper-focus and sometimes in inattention, is a trans-diagnostic phenomenon. Hyper-focus predicted poorer global quality of life, more hypervigilance, more negative repetitive thinking, and more symptoms of anxiety and depression; however, positive experiences of hyper-focus mediated an indirect relationship between hyper-focus and greater quality of life, partially attenuating the overall negative association. Indeed, neurodivergent participants not only reported more negative experiences of hyper-focus than controls, but also more positive experiences. Further studies could explore contextual factors influencing whether hyper-focus has positive or negative impacts on daily life.
Community Abstract
What is already known about this topic?
Many autistic people support the monotropism theory, which says that hyper-focus on interests is central to autism. Prior research also shows that hyper-focus is common in ADHD. However, it is also the case that at other times autistic and ADHD people can be more likely to become distracted from things they are trying to focus on.
What does this paper add?
We asked autistic, ADHD, and control (i.e. neither autistic nor ADHD) adults to answer questions about their experiences of hyper-focus in different areas of life. We also asked participants about whether these experiences were good or bad, and we asked about inattention. Moreover, we asked about quality of life and mental health.
We found that both autistic and ADHD people had more experiences of both hyper-focus and inattention than control participants. Neurodivergent (autistic and/or ADHD) people said they had both more positive and more negative experiences of hyper-focus than controls, and there were ways that hyper-focus was related to both better and worse quality of life. Hyper-focus was related to experiencing more anxiety, depression, negative repetitive thoughts, and vigilance towards possible threats.
Implications
Our results emphasize the importance of understanding how attention is allocated in the world of autistic and ADHD individuals. These findings also imply that hyper-focus and inattention are not opposites but may have common roots. Finally, this study shows that hyper-focus can have either positive or negative impacts—but negative impacts were especially prominent. Future research could explore how we could change the world or provide specialized supports to maximize positive and minimize negative impacts.
Introduction
Attention, hyper-focus, and monotropism in autism and ADHD
Attentional processing has long been considered to lie at the core of ADHD, 1 and furthermore, there have been many suggestions that atypical attentional processing is closely intertwined with autism, and not just in social contexts (e.g. Ashinoff & Abu-Akel, 2021; Keehn et al., 2016; Landry & Bryson, 2004; Murray et al., 2005; Remington et al., 2009). ADHD and autism frequently co-occur in the same individuals (Lai et al., 2019; Lugo-Marín et al., 2019; Rong et al., 2021); in addition, these two neurodevelopmental differences frequently co-aggregate in the same families (Chen et al., 2019; Ghirardi et al., 2018). Given this overlap, it is plausible that the two might share at least some aspects of attentional processing. However, the complexity of attentional styles within each group complicates cross-group comparisons.
Indeed, discussing attentional styles can be difficult given the unclear boundaries between attentional constructs. For example, some evidence suggests that “hyper-focus,” an intense focus on something to the exclusion of other inputs, and “flow,” which includes an intense, intrinsically rewarding focus on resolving challenges, refer to the same phenomena (Ashinoff & Abu-Akel, 2021; Rapaport et al., 2023). However, hyper-focus and flow have also been empirically dissociated in some cases (Grotewiel et al., 2022). This only emphasizes the importance of further investigation of these attentional styles and constructs.
One key construct is monotropism (Murray, 1996; Murray et al., 2005; see also magazine article by Murray, 2018; preprint by Garau et al., 2023; Rapaport et al., 2023). According to the monotropism theory of autism, autistic attention is characterized by what appears to overlap with hyper-focus and flow states (Rapaport et al., 2023): specifically, a narrow attentional tunnel directed towards the interests held by an autistic person. These interests are “monotropic” in that they are postulated to be highly intense and relatively few in number (Murray et al., 2005). This theory was developed by autistic advocates and researchers, and anecdotal evidence suggests it is highly popular in communities of autistic adults (Warren, 2021), where it is often invoked in explanations of and practical strategies related to many aspects of autistic people's real-world experiences (see list of blogs, academic writings, presentations, etc., compiled by Murray, n.d.). Although the monotropism theory has received minimal direct attention in empirical, quantitative autism research studies (cf. Bonneh et al., 2008; Garau et al., 2023), a considerable volume of autism research either addresses probable aspects of monotropism or can be interpreted in line with the theory. Most obviously, many autistic people display intense interests in particular topics (Klin et al., 2007; Spackman et al., 2023; Uljarević et al., 2021; Wood, 2021). Autistic people can also be slow to disengage their attention from stimuli (Keehn et al., 2019a; Landry & Bryson, 2004; Sacrey et al., 2014). This slow disengagement, often called “sticky attention,” appears highly compatible with ideas of slow set-shifting and “autistic inertia” that are intertwined with monotropism (Buckle et al., 2021; Murray et al., 2005). The theory also harmonizes well with findings of enhanced local perception in autism (Mottron et al., 2006) and with difficulties integrating sensory information across modalities (Bonneh et al., 2008; Feldman et al., 2018). Furthermore, autistic people can attend to stimuli in idiosyncratic ways (Avni et al., 2020; Ramot et al., 2020; Tenenbaum et al., 2021), which might be compatible with the idea that autistic people could show an atypical focus on idiosyncratic targets.
However, autism is not only associated with narrow hyper-focusing of attention towards endogenous interests. Other studies suggest that autistic people may show greater awareness of peripheral or distracting stimuli, and when autistic people's task performance is not adversely affected by such distractions, these findings are sometimes postulated to reflect an autistic capacity to attend to and process a larger amount of information at once (Remington & Fairnie, 2017; Remington et al., 2009, 2019). This idea of an enhanced perceptual capacity seems to be essentially the exact opposite of the narrow attention tunnel posited by the monotropism theory. However, other studies suggest that autistic people's attention can be captured by stimuli in ways that do appear to interfere with task performance and learning (Allenmark et al., 2021; Amso et al., 2014; Keehn et al., 2019b; Poole et al., 2018; Venker et al., 2021). Thus, it is possible that autistic people might, in different contexts, display both increased endogenous hyper-focus and increased susceptibility to exogenous attention capture.
Just as in autism, prior ADHD research also observes different attentional styles in different contexts. ADHD is clearly associated with distractibility, attention capture, and mind wandering (Friedman-Hill et al., 2010; Gumenyuk et al., 2005; Lanier et al., 2021), to the extent that inattention is considered one of the two main manifestations of ADHD in contemporary clinical conceptualizations (American Psychiatric Association, 2013; World Health Organization, 2019). Nevertheless, ADHD is also associated with enhanced attentional hyper-focus (Hupfeld et al., 2019; Ozel-Kizil et al., 2016; Sedgwick et al., 2019), and online writings have suggested that the monotropism theory has relevance to ADHD (Dwyer, 2021; Murray & Hallett, 2023). Further emphasizing the complexity of attentional processing, enhanced (self-reported) hyper-focus in ADHD may not be accompanied by enhanced flow (Grotewiel et al., 2022). Importantly, ADHD people's attentional experiences may be context-dependent; ADHD people appear to exhibit heightened hyper-focus when focusing on preferred “screen time” activities (e.g. video games, TV, and social media), but not necessarily in other domains such as school work (Grotewiel et al., 2022). Indeed, ADHD people generally appear to display greater inattention than typically developing people in classroom settings (Kofler et al., 2008). Hyper-focus primarily manifests when tasks are engaging and interesting (Ashinoff & Abu-Akel, 2021), and screen time may often be more inherently engaging than school work, suggesting that ADHD individuals might show greater hyper-focus than typically developing people when tasks are highly engaging, but heightened distractibility when tasks are less engaging.
Thus, based on prior research, it appears that both hyper-focus and distractibility/attention capture are evident in both autism and ADHD. This overlap is not necessarily surprising, given that the two neurotypes frequently co-occur with one another; meta-analyses suggest the prevalence of ADHD in autism is 26%–39% (Lai et al., 2019; Lugo-Marín et al., 2019; Rong et al., 2021), compared to a general-population prevalence of 7% (Thomas et al., 2015). Moreover, relatives of autistic people are at an elevated likelihood of being ADHD (Ghirardi et al., 2018; Jokiranta-Olkoniemi et al., 2016), and vice versa (Chen et al., 2019; Musser et al., 2014). However, there is evidence that the two neurominorities differ from one another in attentional styles. For example, prior laboratory-based research suggests that autistic people can on average show greater sustained attention than ADHD people (Johnson et al., 2007), but that ADHD people can on average perform better on a divided attention task (Boxhoorn et al., 2018). However, overall, context-independent attentional abilities can have an unclear relevance to engagement in specific tasks, where self-efficacy and other factors might have a large role in shaping a person's interests (Gillespie-Lynch et al., 2023). It is possible that trans-diagnostic comparisons of autistic and ADHD people's attentional experiences around their greatest interests in a variety of real-world contexts (e.g. school, hobbies and interests, and screen time) could provide further information about the complex attentional phenotypes in each neurodevelopmental difference.
Vigilance, rumination, and mental health
Another similarity between autism and ADHD is that both neurodevelopmental differences share a high prevalence of co-occurring mental health conditions, such as anxiety and depression (Accardo et al., 2022; Katzman et al., 2017; Lai et al., 2019; Pehlivanidis et al., 2020). It is possible that these mental health struggles are, in part, related to attention.
Anxious individuals often show heightened vigilance towards potential threats (Richards et al., 2014), and although studies exploring attention biases have yielded mixed results (Dennis-Tiwary et al., 2019), interventions aiming to diminish attention biases may be linked to small reductions in anxiety (Fodor et al., 2020), suggesting the existence of causal relationships. Longitudinal research in early development could help clarify relationships between attention biases and anxiety (Burris et al., 2019), but at present, it seems reasonable to suggest that attentional vigilance towards threat could exacerbate anxiety. It is possible that hyper-focusing of attention and susceptibility to attention capture in autism and ADHD might be linked to such vigilance.
Moreover, while prior research suggests that rumination is related to an enhanced ability to ignore distractors, it is also associated with difficulties disengaging attention at least from negative stimuli (Koster et al., 2011; Whitmer & Gotlib, 2013), and as noted above, slow disengagement has been observed in autism and is consistent with the monotropism account of autistic hyper-focus (Murray et al., 2005; Sacrey et al., 2014). A blog post by Hallett (2021) suggests that monotropic attention is linked to ruminative “loops of concern” experienced by many autistic people (see also Black et al., 2023). Given the links between rumination and depression, as well as anxiety (Olatunji et al., 2013), this may suggest a further attentional route towards mental health challenges in neurodivergent people.
Of course, this does not imply that atypical attention is solely responsible for the mental health crisis facing neurodivergent populations. Autistic and ADHD people are at risk for many negative life experiences, such as experiences of stigma and minority stress (Botha & Frost, 2018) and violence (Gibbs & Pellicano, 2023; Stickley et al., 2019), that can affect mental health.
Quality of life
Atypical attention need not have solely negative consequences. Indeed, there may be many aspects of atypical attention and hyper-focus that are beneficial in many contexts (Russell et al., 2019a). For example, autistic intense interests—if appropriately directed—could be a foundation for employment (Goldfarb et al., 2019) and academic success (Wood, 2021) and sources of motivation to engage in intense interests are positively associated with autistic people's well-being (Grove et al., 2018). Indeed, autistic accounts sometimes describe intensely positive emotional experiences (e.g. blog posts by Bascom, 2011; Grace, 2021), which could be related to hyper-focus. Thus, it does not seem unreasonable to suppose that even as some aspects of atypical attention could have negative impacts in many contexts, some aspects of neurodivergent hyper-focus might enhance quality of life (QOL).
Present study
The present study has several aims. Firstly, it aims to compare hyper-focus, intense interests, and inattention across groups of autistic-only and ADHD-only adults, a group of autistic and ADHD individuals (Autistic + ADHD), and a non-autistic, non-ADHD comparison group. Secondly, it aims to explore associations between attention measures and hypervigilance, rumination, anxiety, depression, and QOL. Finally, it aims to evaluate whether inattention and hyper-focus are associated, and if so, in what direction. We formulated these hypotheses:
Domain-general hyper-focus will be elevated in autistic-only and autistic + ADHD groups relative to ADHD-only, and elevated in ADHD-only relative to controls. Intense interests and hyper-focus on hobbies and schoolwork will be elevated in autistic-only and autistic + ADHD groups relative to ADHD-only, but hyper-focus on screen time will not differ between the autism groups and ADHD-only individuals. Greater hyper-focus will be associated with greater QOL in neurodivergent participants. There will be associations between greater hyper-focus and elevated anxiety, depression, hyper-vigilance, and negative repetitive thinking. Hyper-focus will be positively associated with inattention.
Methods
Before beginning recruitment, we distributed the survey to seven pilot participants (three autistic-only, two ADHD-only, and two autistic + ADHD), who each received $25 USD in exchange for suggestions and feedback. Based on pilot feedback, we shortened the survey considerably by adapting or removing several measures. Pilot participants’ data are not included in this report.
Participants
Participants from four groups were recruited: autistic participants who were not ADHD (autistic-only), ADHD participants who were not autistic (ADHD-only), participants who were both autistic and ADHD (autistic + ADHD), and participants who were neither autistic nor ADHD (comparison).
Participants were recruited from several online databases, each of which collected demographic information about participants in an effort to facilitate targeted recruitment; recruitment was targeted within the United States towards the four participant groups and in an effort to produce groups with comparable demographics. We planned to recruit ADHD and comparison group participants from CloudResearch (Litman et al., 2017), a general population database that allows for sampling based on ADHD status, and autistic participants from SPARK Research Match (Feliciano et al., 2018), a large cohort of diagnosed autistic participants. However, after the Prolific (Palan & Schitter, 2018) general population database introduced functionality for targeting recruitment based on autism status as well as ADHD status, we began recruiting from Prolific and SPARK instead.
Participants first filled out screening questionnaires to assess eligibility. A total of 1038 unique, complete screening responses were received (63 CloudResearch, 649 Prolific, and 325 SPARK), with a median response duration of 2.50 min. Self-identifications as autistic or ADHD were accepted, as long as ADHD identifications were consistent with ASRS-6 scores as described below. Participants with uncorrected hearing loss or who missed attention checks were excluded. Participants in the comparison group were required to not have first- or second-degree autistic and ADHD relatives. CloudResearch and Prolific participants received $0.55 USD for the screening survey.
A total of 609 unique participants both screened as eligible and went on to provide full or partial responses to the full survey; however, some participants’ full survey responses were removed due to missed attention checks, self-reported random answering, or admitting to ignoring survey instructions (n = 17); discrepant answers between the screening survey and the full survey, including revised ASRS-6 responses outside eligibility criteria (n = 65); RAADS-14 scores above cut-off in comparison participants (n = 29); and RAADS-14 scores below cut-off in autistic participants (n = 6). This left a final sample of 492 participants (Table 1): 99 comparison (10 CloudResearch and 89 Prolific), 122 ADHD-only (seven CloudResearch and 115 Prolific), 130 autistic-only (38 Prolific and 92 SPARK), and 141 autistic + ADHD (one CloudResearch, 37 Prolific, and 103 SPARK). The median response duration was 44.82 min. All participants received $15 USD for completing the final survey.
Demographic characteristics of participants. Analyses of ordinal variables use omnibus Kruskal–Wallis tests and Wilcoxon–Mann–Whitney post-hocs; however, comparisons of the ages of ADHD and autism diagnoses use only Wilcoxon–Mann–Whitney tests, due to the availability of autism and ADHD diagnostic data only from autistic and ADHD participants. Analyses of categorical variables use Fisher's exact tests.

ADHD: attention dysregulation hyperactivity development; ASRS-18: 18-item version of the Adult ADHD Self-Report Scale; ASRS-6: six-item World Health Organization Adult ADHD Self-Report Scale.
Education was operationalized as an ordinal scale ranging from 1 (“Some high school or less”) to 10 (“Doctorate degree (e.g. PhD and EdD)”). Average responses were around 5 (“Associate degree (e.g. AA and AS)”) to 6 (“Bachelor's degree (e.g. BA and BS)”).
ASRS-18 Inattention and Hyperactivity-Impulsivity scores reported here are based on summing scores when considering all response options, that is, in line with “Method 3” as described by Kessler et al. (2005).
Including self-reports of both self-identified and formally diagnosed co-occurring conditions, if current.
Note that some participants with formal diagnoses could not recall which subtype they had been diagnosed with.
Questionnaires
Adult ADHD Self-Report Scale (ASRS)
The six-item World Health Organization ASRS (ASRS-6) (Kessler et al., 2005, 2007) was collected in the screening survey for the purpose of assessing eligibility. The ASRS-6 offers multiple cut-off scores (10, 14, and 18), allowing for varying levels of sensitivity and specificity (Kessler et al., 2007). These multiple cut-offs allowed us to take into account of phenotypic overlap between autism and ADHD (Krakowski et al., 2021; Vaidya & Klein, 2022), as well as whether participants had formal diagnoses or self-identifications only. As such, the following participants were considered eligible: (a) diagnosed or self-identified autistic participants who indicated that they were non-ADHD, and whose ASRS-6 scores fell under the least sensitive ADHD cut-off (18); (b) participants who indicated that they were non-ADHD and non-autistic, and whose ASRS-6 scores fell under the middle cut-off (14); (c) participants who self-identified as ADHD, but had no formal diagnosis, and whose ASRS-6 scores met or exceeded the middle cut-off (14); and (d) participants who had formal ADHD diagnoses and whose ASRS-6 scores met or exceeded the most sensitive cut-off (10).
In addition, we included non-autistic participants who reported formerly (but not currently) being ADHD, but whose ASRS-6 scores met or exceeded the middle cut-off (14). Only two such participants were included in the final full survey sample. Interestingly, one reported current ADHD at screening and historical ADHD in the full survey, while the other participant reported the opposite pattern. These participants were included in the ADHD-only group. Otherwise, participants with historical but not current ADHD were excluded.
In the full survey, we collected the longer 18-item version of the ASRS, the ASRS-18 (Kessler et al., 2005). As this included the six items used to calculate the ASRS-6, we re-examined ASRS-6 scores and excluded participants who no longer met the criteria for inclusion based on their second ASRS-6 score.
Ritvo Autism and Asperger Diagnostic Scale (RAADS-14)
The 14-item version of the RAADS (RAADS-14; Eriksson et al., 2013) was collected in the full survey, but not in the screening survey. Autistic participants were excluded if they did not have RAADS-14 scores at or exceeding the cut-off (14). Comparison participants were excluded if they scored at or above the cut-off. However, while the RAADS-14 has excellent sensitivity, its specificity is poorer, and the median RAADS-14 score of ADHD-only participants exceeded the autism cut-off in both the validation sample (Eriksson et al., 2013) and in the present study, which likely reflects the phenotypic overlap between autism and ADHD. As such, ADHD-only participants were included even if they scored at or above the RAADS-14 cut-off. As noted in Table 1, the average RAADS-14 score in the ADHD-only group remained much lower than in the autistic-only and autistic + ADHD groups.
Adult Hyperfocus Questionnaire (AHQ)
We presented an adapted version of the AHQ developed by Hupfeld et al. (2019). As in the original measure, participants were asked to answer items about the frequency of having certain experiences of hyper-focus in four domains: in general (dispositional hyper-focus), in their favorite school class, in their favorite hobby, and in their most frequent screen time activity. As the survey included six apparent doublet pairs of similar items (losing track of time, ignoring distractions, forgetting personal needs, difficulty shifting, captivation/fixation, and getting stuck on details), we, in consultation with Kathleen Hupfeld, removed one item from each doublet. This left six items for each of the four domains, or 24 items in total.
Furthermore, following a recommendation kindly provided by Kathleen Hupfeld, we added 5 Likert-scale items asking about feelings of enjoyment and productivity as consequences of hyper-focus in general (e.g. “I enjoy how captivated I become when doing an activity that is engaging to me”). We also included separate items asking about the valence of dispositional, school, hobby, and screen time hyper-focus, with the prompt, “I consider my experiences of focusing intensely on tasks or activities to be,” and a visual analogue scale (VAS) from “Completely Negative” (0) to “Completely Positive” (100); data on these items are presented in Supplemental Table 5. Participants also answered open-ended questions about activities causing them to be very focused, and a specific instance when they became very focused.
Evaluation of Autistic Special Interests-Adult (EASI-A)
The EASI-A (Williams, 2022) is a brief measure intended to assess autistic intense interests. The contents of the EASI-A are based on the structure of the Interests Scale, a parent-report developed for use in autism (Turner-Brown et al., 2011). In the version adapted for this study, participants were first asked, “Some people have very intense or focused interests in specific topics. Do you currently have any interests or hobbies that you believe are more intense or focused than most other people's interests?” If yes, participants were asked to list their primary interest. All participants were then asked to answer five items regarding the intensity and typicality of the interest (e.g. “Overall, how strong is your interest in this topic?”), with scales of 0–4 customized to each item.
Furthermore, participants were presented with VASs and asked to rate the positive and negative effects of their intense interest on their lives. The two scales were averaged, after reversing the negative scale, to yield a combined scale from 0 (negative) to 100 (positive). Effects on each scale separately are presented in Supplemental Table 6.
Finally, we included the customized Evaluation of Autistic Special Interests Social Addendum (EASI-Social), a brief bespoke measure asking participants to rate six items (e.g. “I have a hard time making conversation about things that are not my primary interest”), on a scale from Strongly Disagree (0) to Strongly Agree (5), assessing the degree to which participants’ social engagement depended on their intense interests.
Single Item Global QOL Scale (SIG-QOL)
The Single Item Global QOL Scale, Version 1.0 (SIG-QOL-1.0; Williams, 2021) invites participants to rate their global QOL on a VAS from 0 to 100, with the meaning of different ratings clearly described: for example, “21–35: Bad quality of life (Generally dissatisfied with life; Could still be worse).” Because SIG-QOL respondents are asked to base ratings on what is important to them, it circumvents the need to determine a priori what constructs and domains will be relevant to participants’ QOL, which—particularly for neurodivergent populations such as autistic adults—remains a subject of debate (Ayres et al., 2018; Erez & Gal, 2020; Evers et al., 2022; Higashida, 2022; Hong et al., 2016; McConachie et al., 2020; Tavernor et al., 2013), complicating cross-group comparisons and potentially biasing attempts to identify predictors of QOL.
Overall Anxiety Severity and Impairment Scale (OASIS)
The OASIS (Norman et al., 2006) is a brief, unidimensional measure with five items asking about the frequency and impacts of respondents’ experiences of anxiety. The measure's response options are accompanied by clear, often-vivid descriptions of what each option means, which may make it advantageous for research in neurodivergent populations where traditional scale options can be ambiguous. Prior studies support its reliability and convergent and discriminant validity (Campbell-Sills et al., 2009; Norman et al., 2006).
Overall Depression Severity and Impairment Scale (ODSIS)
The ODSIS mimics the structure and clarity of the OASIS, and is a unidimensional questionnaire with five items on the frequency and impacts of experiences of depression; it shows evidence of good convergent and discriminant validity (Bentley et al., 2014).
Brief Hypervigilance Scale (BHS)
The BHS (Bernstein et al., 2015) is a concise, 5-item, reliable, validated instrument measuring hyper-vigilance. Items (e.g. “As soon as I wake up and for the rest of the day, I am watching for signs of trouble.”) are rated on a 5-point Likert scale from “Not At All Like Me (never true)” to “Very Much Like Me (Always True).” The measure was constructed using items that converged with a hypervigilance item from a measure of post-traumatic stress symptoms (Bernstein et al., 2015).
Perseverative Thinking Questionnaire (PTQ)
The PTQ (Ehring et al., 2011) is a measure of negative repetitive thinking (rumination) with 15 items (e.g. “The same thoughts keep going through my mind again and again) asking participants to rate the frequency of their negative repetitive thinking experiences from “Never” to “Almost Always.” Items load onto one core factor, as well as three lower-order factors respectively reflecting characteristics of negative repetitive thinking, perceptions of (un)productiveness of negative repetitive thinking, and capture of mental capacity by negative repetitive thinking. The measure shows good reliability and convergent validity (Ehring et al., 2011), and has been used in prior autism research (Keenan et al., 2018).
Data analysis
All statistical analyses were conducted in R Studio. Where the factor structures of scales based on Likert items were unknown, exploratory graph analysis (Golino & Epskamp, 2017) was used to explore factor structures.
Group comparisons
To address hypotheses 1 and 2, we statistically compared participant groups based on ratings of their hyper-focus/intense interests (more specifically, frequency of dispositional and domain-specific hyper-focus per AHQ, interest intensity and relevance of intense interests to social connections per EASI-A and its social addendum, and ratings of the valence of hyper-focus and intense interests from the EASI-A and AHQ). We also compared groups’ mental health and well-being (SIG-QOL, OASIS anxiety, ODSIS depression, BHS hypervigilance, and PTQ negative repetitive thinking). These comparisons used two-way ordinal probit regression (Harrell, 2022; Ripley et al., 2022), with autism and ADHD as separate, dummy-coded independent variables. Significant interactions were probed using Wilcoxon–Mann–Whitney tests to compare all groups, with a Benjamini and Yekutieli (2001) false discovery rate correction for multiple comparisons. Cliff's delta (δ; Cliff, 1993; Torchiano, 2022) was reported as an effect size.
We also compared whether groups differed in the likelihood that participants reported having an intense interest using binary logistic regression, with comparisons of estimated marginal means for post-hoc comparisons (Lenth et al., 2021).
After we had defined the final sample included in statistical analyses in the main text, we later explored patterns of group differences while adjusting the RAADS-14 and ASRS score thresholds required for inclusion in the present study. These results are presented in Supplemental Tables 7 to 12.
Associations of measures
To address hypotheses 3–5, we examined associations between AHQ dispositional hyper-focus and well-being/mental health variables, as well as between AHQ dispositional and domain-specific hyper-focus and ASRS-18 inattention, using ordinary least squares regression with scaled, ranked continuous variables. Entering continuous variables into the regression models as ranks made them analogous to Spearman's correlation tests; standardization of ranks then enhanced ease of interpretation. Regression was employed so that both the continuous predictor and categorical autism and ADHD group status could be entered into the models, thereby allowing associations to be examined while controlling for group differences that might create illusory associations. Furthermore, interaction terms permitted the exploration of between-group differences in the magnitude of the correlations.
Where continuous predictor variables significantly interacted with autism and/or ADHD group status in predicting a continuous dependent variable, Spearman's correlations were calculated for all relevant groups. The Spearman's ρ correlation coefficients were then slightly transformed to make them analogous to Pearson's r (Myers & Sirois, 2006) before they were statistically compared across groups using the Fisher's z test (Diedenhofen & Musch, 2015). Confidence intervals for differences in the magnitudes of the correlation coefficients were calculated (Zou, 2007), and then transformed back to the metric of Spearman's ρ before reporting.
To further explore hypothesis three, we also examined associations between dispositional hyper-focus and QOL, as mediated in parallel by both positive and excessive engagement in hyper-focus, which were explored using PROCESS Model 4 (Hayes, 2022). Autism and ADHD group membership were entered as separate covariates. As with the regression analyses, continuous variables were scaled and ranked, making coefficients analogous to Spearman's correlations.
Finally, correlation matrices with all continuous variables employed in the present article are presented in Supplemental Tables 1 to 4.
Results
Psychometrics
Exploratory graph analysis grouped the AHQ dispositional Likert-scale valence/consequence items into two communities in all bootstrap iterations: Positive Engagement (three items; e.g. “I generate creative solutions or ideas when I am very engaged in an activity”) and Excessive Engagement (two items, e.g. “I do not like how fixated or obsessed I can become on an activity that I find engaging”). Item-level analyses are nevertheless presented in Supplemental Table 5.
Meanwhile, exploratory graph analysis suggested the Likert items from the EASI-A fell into two communities, 95% CI = [1.49, 2.51], in 92.6% of iterations. These were Interest Intensity (three items; e.g. “In the past week, on average, how much time did you spend on activities related to this topic?”) and Others’ Interest (two items; e.g. “How easy has it been for you to find other people who share this interest?”). Item-level analyses are nevertheless presented in Supplemental Table 6.
The EASI-Social was assessed as unidimensional in all instances; Cronbach's α was 0.82, 95% CI = [.79, .85].
Group comparisons
Hyper-focus and intense interests
There were main effects of autism and ADHD on summed Likert scores from all four hyper-focus domains from the AHQ (dispositional, Figure 1A; school, Figure 1B; hobbies, Figure 1C; and screen time, Figure 1D), reflecting greater hyper-focus in autistic and ADHD people than non-autistic and non-ADHD people. Interactions of autism and ADHD were also observed for all domains. As reported in Table 2, autistic + ADHD people reported more dispositional, school, and hobby hyper-focus than ADHD-only people, though they did not differ in screen time hyper-focus. ADHD-only people had significantly more dispositional, hobby, and screen time hyper-focus than autistic-only people, but they did not differ in school hyper-focus. All neurodivergent groups reported more hyper-focus in all domains than comparison participants.

Violin plots, with overlaid horizontally jittered data points, depict scores on measures of hyper-focus (HF), intense interests, and the valence of those experiences. Panels (A) to (D) depict AHQ HF scores. Panels (E) and (F) depict subscales from the Likert portion of the EASI-A, while Panel (G) depicts EASI-Social scores. Panel (H) depicts EASI-A VAS ratings of the effects of intense interests. Panel (I) depicts scores for positive engagement in dispositional HF on the AHQ, while Panel (J) depicts scores for self-reported excessive HF engagement.
Results of ordinal probit regression analyses, as well as Benjamini–Yekutieli FDR-corrected Wilcoxon post-hoc tests, comparing groups on AHQ, EASI-A, and EASI-Social subscales and VAS scales. Coefficients and their 95% confidence intervals are reported. For post-hoc tests, Cliff's δ and its 95% confidence interval are reported as effect sizes; post-hocs are shaded in grey when the interaction is not significant. Autism and ADHD group status were entered into the regression models as separate, dummy-coded variables (that is, in the omnibus model, we collapse across the autistic-only/control and autistic + ADHD/ADHD-only distinction, to examine a single overall effect of being autistic, and same for the overall effect of being ADHD). An interaction would indicate these overall effects are not independent, but depend upon each other (e.g. the difference between autistic-only and control participants might be larger than that between autistic + ADHD and ADHD-only participants). For the effects of autism, the reference group is non-autistic participants (i.e. positive coefficients mean higher scores among autistic people, and negative coefficients mean lower scores among autistic people). For the effects of ADHD, the reference group is non-ADHD participants.

AHQ: Adult Hyperfocus Questionnaire; ADHD: attention dysregulation hyperactivity development; EASI-A: Evaluation of Autistic Special Interests-Adult; VAS: visual analogue scale.
.
There were main effects of autism and ADHD on EASI-A Interest Intensity, p = .0004 (Table 2), reflecting greater intensity of interests in autistic than non-autistic participants, and in ADHD than non-ADHD participants (Figure 1E). We also used binary logistic regression to examine the effects of autism and ADHD on whether participants endorsed having an intense interest. We observed the main effects of autism, OR = 7.24, 95% CI = [4.02, 13.39], p < .0001, and ADHD, OR = 4.36, 95% CI = [2.47, 7.87], p < .0001, and an interaction between them, p = .01. Per post-hoc comparisons of estimated marginal means, autistic + ADHD participants were more likely to report an intense interest than ADHD-only participants, corrected p = .01. Participants in all neurodivergent groups were more likely to report an intense interest than controls, corrected p's < .0001.
Meanwhile, there were main effects of autism and ADHD on EASI-A Others’ Interest scores, reflecting how easily participants could find others sharing their interests; there was also an interaction between autism and ADHD (Table 2). Post-hocs suggested all neurodivergent groups struggled more than comparison participants to find others sharing their interests (Figure 1F). There were also main effects of autism and ADHD on EASI-Social scores, and an interaction between them. As depicted in Figure 1G, this indicated that autistic and ADHD participants appeared to depend more than non-autistic and non-ADHD participants on social connections with others who shared their interests—despite, as previously shown by EASI-A Others’ Interest scores, struggling more to find those connections. Autistic + ADHD people depended more than ADHD-only people on these interest-based social connections.
There were main effects of autism and ADHD on averaged VAS scores from the EASI-A (Table 2), reflecting more negative experiences of intense interests in autistic and ADHD people than non-autistic and ADHD people (Figure 1H); there was no interaction.
There were main effects of autism and ADHD, and interactions between them, on AHQ positive engagement and excessive engagement scores (Table 2, Figure 1I and J). Post-hocs found more positive engagement and more excessive engagement in almost all neurodivergent people, relative to comparison participants (although the positive engagement effect fell slightly below the corrected significance threshold in ADHD-only participants). The three neurodivergent groups did not significantly differ from one another in positive engagement, but ADHD-only and autistic + ADHD participants experienced more excessive engagement than autistic-only participants, who in turn experienced more excessive engagement than comparison participants.
Interestingly, even though neurodivergent people experienced more positive hyper-focus than non-autistic and non-ADHD controls, they did not report more positive effects of intense interests (Supplemental Table 6).
Well-being
There were main effects of ADHD on QOL (SIG-QOL), anxiety (OASIS), depression (ODSIS), hypervigilance (BHS), and negative repetitive thinking (PTQ) scores, reflecting poorer QOL and more anxiety, depression, hypervigilance, and negative repetitive thinking in ADHD than non-ADHD participants (Figure 2 and Table 3). Furthermore, there were significant main effects of autism on all of those variables, and in the same directions. However, there were also interactions of autism and ADHD on anxiety, depression, hypervigilance, and negative repetitive thinking. According to post-hoc tests (Table 3), ADHD-only participants reported more negative repetitive thinking than autistic-only participants. Autistic + ADHD participants had higher scores on all four measures with interactions than autistic-only participants, and people in all three neurodivergent groups had higher scores on those four measures than comparison participants.

Violin plots, with overlaid horizontally jittered data points, depicting quality of life (SIG-QOL, panel A), anxiety (OASIS, panel B), depression (ODSIS, panel C), hypervigilance (BHS, panel D), and negative repetitive thinking (PTQ, panel E) scores. Significance bars reflect Benjamini-Yekutieli-corrected Wilcoxon-Mann-Whitney post-hoc tests, equivalent to those in Table 3.
Results of ordinal probit regression analyses, as well as Benjamini–Yekutieli FDR-corrected Wilcoxon post-hoc tests, comparing groups on quality of life (SIG-QOL), anxiety (OASIS), depression (ODSIS), hypervigilance (BHS), and negative repetitive thinking (PTQ) scores. Coefficients and their 95% confidence intervals are reported. For post-hoc tests, Cliff's δ and its 95% confidence interval are reported as effect sizes; post-hocs are shaded in grey when the interaction is not significant. For the effects of autism, the reference group is non-autistic participants. For the effects of ADHD, the reference group is non-ADHD participants.
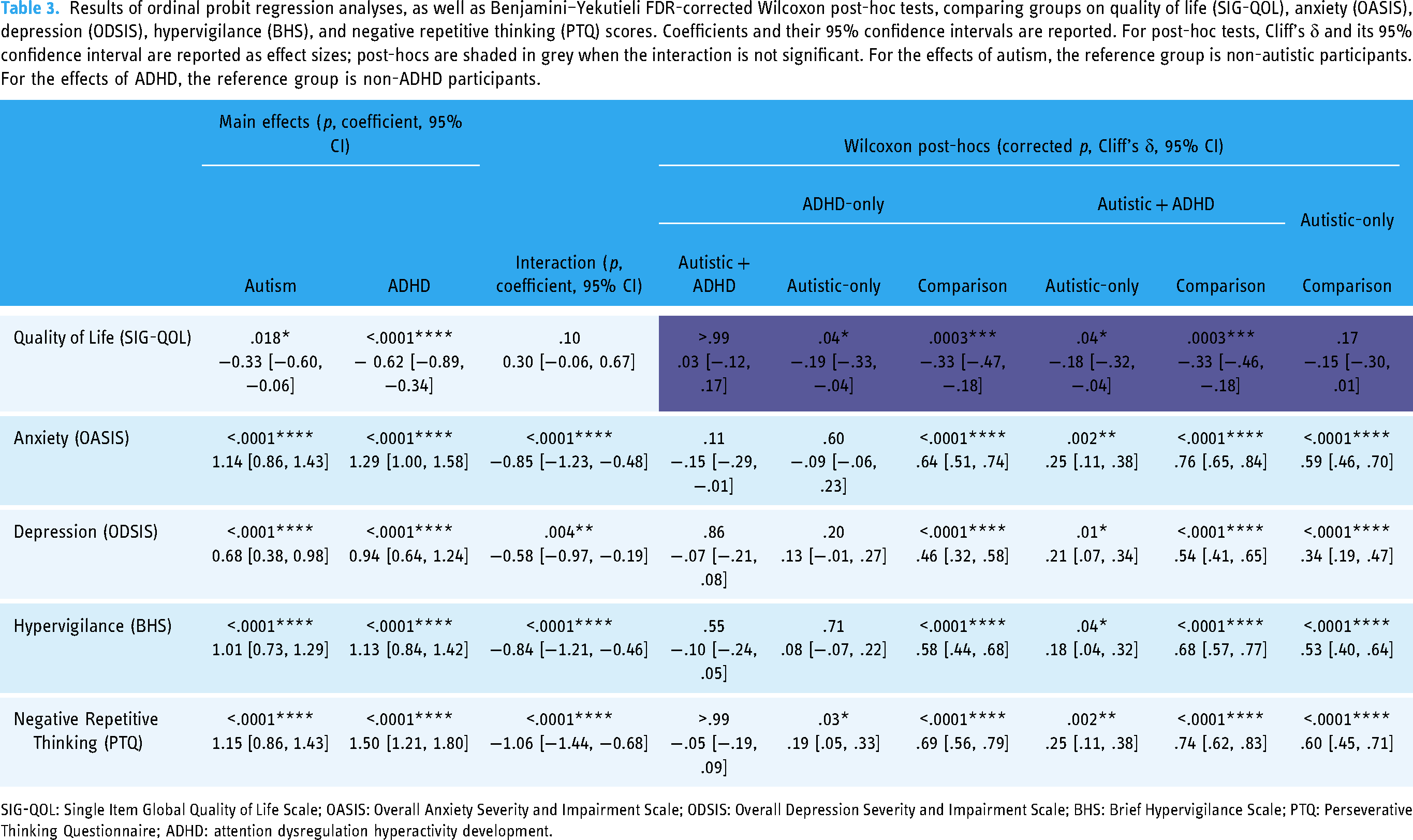
SIG-QOL: Single Item Global Quality of Life Scale; OASIS: Overall Anxiety Severity and Impairment Scale; ODSIS: Overall Depression Severity and Impairment Scale; BHS: Brief Hypervigilance Scale; PTQ: Perseverative Thinking Questionnaire; ADHD: attention dysregulation hyperactivity development.
Associations of measures
Associations of attention and well-being
Unexpectedly, there was no overall effect of AHQ dispositional hyper-focus on QOL, nor did hyper-focus significantly interact with autism or ADHD group membership to predict QOL (Table 4 and Figure 3A). However, as expected, dispositional hyper-focus was significantly associated with greater anxiety, greater depression, greater hypervigilance, and greater negative repetitive thinking (Table 4 and Figure 3B to E).

Linear slopes representing associations between well-being variables (SIG-QOL quality of life, panel A; OASIS anxiety, panel B; ODSIS depression, panel C; BHS hypervigilance, panel D; and PTQ negative repetitive thinking/rumination, panel E) and AHQ dispositional hyper-focus scores. Note that the statistical analyses use ordinal ranked regression and Spearman's ordinal correlation, not the linear slopes depicted here. Data points are slightly jittered for display purposes.
Results of standardized, ranked regression analyses examining associations between AHQ Dispositional Hyper-Focus (AHQ-DHF) scores and quality of life (SIG-QOL), anxiety (OASIS), depression (ODSIS), hypervigilance (BHS), and negative repetitive thinking (PTQ) scores. Autism and ADHD group status are included in the regressions, in order to control for group differences and explore whether associations vary by group. Autism and ADHD were entered into the regression models as separate, dummy-coded factors. For the effects of autism, the reference group is non-autistic participants. For the effects of ADHD, the reference group is non-ADHD participants.

SIG-QOL: Single Item Global Quality of Life Scale; OASIS: Overall Anxiety Severity and Impairment Scale; ODSIS: Overall Depression Severity and Impairment Scale; BHS: Brief Hypervigilance Scale; PTQ: Perseverative Thinking Questionnaire; ADHD: attention dysregulation hyperactivity development.
Moreover, there was an interaction between autism status and hyper-focus in predicting ODSIS depression scores, p = .04 (Table 4 and Figure 3C). Hyper-focus was associated with greater depression in autistic participants, ρ = .18, p = .003, 95% CI = [.06, .30], and in non-autistic participants, ρ = .46, p < .0001, 95% CI = [.34, .56]. However, the association was stronger in non-autistic participants, Fisher's z = 3.45, p = .0006, Zou's 95% CI = [.12, .42].
Similarly, there was an interaction between autism status and hyper-focus in predicting PTQ negative repetitive thinking scores, p = .009 (Table 4 and Figure 3E). Hyper-focus was associated with more negative repetitive thinking in both the autistic, ρ = .30, p < .0001, 95% CI = [.18, .40], and non-autistic, ρ = .64, p < .0001, 95% CI = [.55, .71], groups. Again, the association was stronger in non-autistic participants, Fisher's z = 4.95, p < .0001, Zou's 95% CI = [.20, .46]. However, this statistical effect appeared to be driven primarily by the comparison group, not the ADHD-only group (Figure 3E and Supplemental Table 3); the variability of scores due to the presence of both typical and neurodivergent participants among non-autistic people may also have provided more range for the association to reveal itself among non-autistic participants.
Because AHQ dispositional hyper-focus unexpectedly failed to predict better QOL, we conducted a parallel mediation analysis to explore whether a more complex relationship might become apparent when differently valenced experiences of engagement in hyper-focus were allowed to mediate the association (Figure 4). AHQ dispositional hyper-focus directly predicted reduced global QOL, β = −0.23 [95% CI: −.35, −.11], p = .0002. However, dispositional hyper-focus indirectly, as mediated by its association with more positive engagement in hyper-focus, predicted greater QOL, β = 0.06 [95% CI: .02, .11], p = .004. Excessive engagement in hyper-focus did not mediate an indirect relationship between hyper-focus and QOL, β = 0.01 [95% CI: −.03, .04], p = .72.

Path diagram depicting results of parallel mediation analysis examining how positive and excessive experiences of hyper-focus mediate links between overall, dispositional hyper-focus and global quality of life. Hyper-focus directly predicted a lower quality of life, but as mediated by positive hyper-focus, it indirectly predicted a greater quality of life.
Associations of inattention and hyper-focus
As expected, ranked regression analyses indicated that AHQ scores measuring the frequency of hyper-focus experiences in different domains (dispositional, school, hobby, and screen time hyper-focus) were positively associated with ASRS-18 Inattention scores (Table 5 and Figure 5A to D). No interactions between autism/ADHD group status and ASRS Inattention scores were observed, suggesting the associations did not meaningfully differ across groups.

Linear slopes representing associations between ASRS-18 Inattention scores (x-axis) and AHQ hyper-focus scores, indexing the frequency of experiences of hyper-focus in different domains (panels A–D), and EASI-A interest intensity scores, measuring the degree to which participants have intense, time-consuming interests (panel E). Note that the statistical analyses use ordinal ranked regression and Spearman's ordinal correlation, not the linear slopes depicted here. Data points are slightly jittered for display purposes.
Results of standardized, ranked regression analyses examining associations between ASRS-18 Inattention scores and AHQ subscales measuring the frequency of experiences of hyper-focus in multiple domains, as well as between ASRS-18 Inattention and EASI-A Interest Intensity. Autism and ADHD group status are included in the regressions, in order to control for group differences and explore whether associations vary by group. Specifically, autism and ADHD status were entered as separate, dummy-coded factors. For the effects of autism, the reference group is non-autistic participants. For the effects of ADHD, the reference group is non-ADHD participants.

ADHD: attention dysregulation hyperactivity development; AHQ: Adult Hyperfocus Questionnaire; EASI-A: Evaluation of Autistic Special Interests-Adult; ASRS-18: 18-item version of the Adult ADHD Self-Report Scale.
There was no statistical evidence suggesting that EASI-A Interest Intensity was associated with ASRS-18 Inattention (Table 5 and Figure 5E).
Discussion
The present study explores, in a large online sample, experiences of attention and hyper-focus in autism, ADHD, and a comparison group. As might be expected under a monotropism account, neurodivergent participants reported experiencing more hyper-focus than comparison participants. Neurodivergent people were also more likely to report having intense interests. However, in all participant groups (autistic-only, ADHD-only, autistic + ADHD, and comparison), people reporting elevated hyper-focus were also more likely to report seemingly opposite experiences of inattention and susceptibility to distraction. Hyper-focus in the present study was robustly associated with increased anxiety, depression, hyper-vigilance, and negative repetitive thinking. Hyper-focus was also directly associated with poorer QOL, but having more positive engagement in hyper-focus mediated an indirect relationship between hyper-focus and greater QOL.
Hyper-focus group differences
Our finding that neurodivergent participants experienced more AHQ hyper-focus than comparison participants was expected, and consistent with the monotropism account. However, we were surprised to observe that ADHD-only people reported more general/dispositional hyper-focus, more hyper-focus on hobbies, and more hyper-focus on favorite screen time activities than autistic-only people, contrary to Hypotheses 1 and 2. We also found no differences between autistic-only and ADHD-only people in hyper-focus on favorite school classes, while autistic + ADHD people had the greatest hyper-focus in all domains except screen time, in which they did not statistically differ from ADHD-only people. We had expected autistic-only and autistic + ADHD people to display more general/dispositional, hobby, and school hyper-focus than ADHD-only people, and not to differ from them in screen time hyper-focus.
One possible contributor to these patterns of group differences might be the history of the AHQ. The instrument was developed in the context of ADHD research, and it, therefore, may be that some items—particularly those that ask about intense focus experiences that interfere with daily life and other tasks—might capture aspects of hyper-focus that are particularly prominent in ADHD. Difficulties measuring and conceptualizing these constructs are discussed further below, in the “Understanding neurodivergent attention and hyper-focus” section.
However, differences between neurodivergent and comparison participants were very robust and consistent, and it seems clear that autistic, ADHD, and autistic + ADHD people all experienced elevated hyper-focus relative to the comparison group.
Moreover, patterns of hyper-focus across domains did appear to show some differences across the neurodivergent groups. For example, ADHD-only people showing more hyper-focus than autistic-only people in all domains except school suggests that factors in the school domain differentially affect the expression of hyper-focus in ADHD versus autism. Similarly, the pattern whereby autistic + ADHD participants showed more of all forms of hyper-focus except screen time hyper-focus, relative to ADHD-only participants, may suggest that ADHD tends to have a particularly strong influence on screen time hyper-focus: an influence to which autism makes little or no further additive contribution.
We also explored how participants’ intense interests shaped their social lives. Autistic and ADHD people reported struggling more to find others to share in their interests; non-autistic and non-ADHD people more easily connected with others with common interests. Nevertheless, autistic people's social connectedness depended more on social relationships based on common interests than non-autistic people's connectedness; similar effects for ADHD were also observed. Thus, it seems interest-based social connections are crucial for many neurodivergent people, but that these connections are very difficult for them to make. This emphasizes the importance of efforts to promote interest-based social connections (Jones et al., 2021; Koegel et al., 2013), particularly in nuanced, respectful, non-deficit-oriented ways (Tansley et al., 2022), and of ameliorating stigma towards intense interests (Stockwell et al., 2020).
Furthermore, we explored the valence and consequences of hyper-focus and intense interests. Autistic and ADHD people reported more positive (i.e. productive, creative, and enjoyable) experiences of hyper-focus than non-autistic and non-ADHD people. However, autistic and ADHD people also reported more negative (i.e. time-wasting and non-enjoyable) experiences of hyper-focus. This suggests that the elevated hyper-focus reported by neurodivergent people was sometimes beneficial and sometimes bothersome, depending on context; this nuanced conclusion is very consistent with prior qualitative research (Rapaport et al., 2023; Russell et al., 2019a), as well as quantitative (Grove et al., 2018) and qualitative (Wood, 2021; see also conference presentation by Boucher et al., 2023) studies on intense interests. However, in another as-yet-unpublished qualitative study, autistic adolescents described predominantly positive experiences of intense interests (Batkin et al., 2023). This appears to contrast with the findings of the present study, in which neurodivergent participants did not report more positive effects of intense interests than comparison participants, and the reported overall effects of intense interests appeared to be more negative in neurodivergent people.
Relations with QOL
Just as neurodivergent participants reported both more positive and negative engagement in hyper-focus, we observed evidence that hyper-focus could be associated with greater or reduced QOL. There was a robust direct relationship between dispositional hyper-focus and poorer global QOL, but we also found an indirect relationship between dispositional hyper-focus and greater QOL; this indirect relationship was mediated by positive (i.e. creative, productive, and enjoyable) engagement in hyper-focus.
In this sense, Hypothesis 3 was not wholly supported; hyper-focus was not solely related to reports of better QOL. Indeed, the direct relationship between hyper-focus and poorer QOL appeared to be somewhat stronger than its indirect relationship to greater QOL. This is in line with suggestions that hyper-focus and intense interests should not be seen as wholly positive, and that their beneficial effects may depend upon a variety of other factors (Goldfarb et al., 2019).
Relations with mental health
We observed clear and robust relationships between hyper-focus and anxiety, depression, hyper-vigilance, and negative repetitive thinking, as predicted by Hypothesis 4. Although mental health struggles in neurodivergent populations can in large part be understood as a reaction to negative experiences (Wood & Gadow, 2010), such as peer rejection and victimization (Becker et al., 2017; Cappadocia et al., 2012; Mrug et al., 2012), being repeatedly criticized (Beaton et al., 2022), not feeling accepted by others (Cage et al., 2018), and indeed the everyday stress of being part of a minority group and facing discrimination and stigma (Botha & Frost, 2018), a hyper-focused attentional style might exacerbate the situation further. Negative repetitive thinking and rumination upon perceived failures and challenges could amplify their mental health impacts. Meanwhile, hyper-focus combined with a history of negative experiences could naturally lead many neurodivergent people to become hyper-vigilant towards potential threats. Hyper-vigilance and rumination might then exacerbate anxiety and depression (Burris et al., 2019; Olatunji et al., 2013). However, this cross-sectional study does not provide causal evidence of this.
Understanding neurodivergent attention and hyper-focus
Finally, as we predicted in Hypothesis 5, hyper-focus scores were correlated with ASRS Inattention scores, suggesting that inattention and susceptibility to distraction tend to be accompanied by greater levels of hyper-focus. This may suggest that both patterns can reflect an underlying shared atypical regulation of attention, which might manifest differently in different contexts.
However, many unanswered questions remain about the nature, conceptualization, and measurement of hyper-focus and atypical attention regulation. Although hyper-focus is sometimes regarded as identical to flow (Ashinoff & Abu-Akel, 2021), and scores on the AHQ hyper-focus measure used in this study have been shown to inversely correlate with flow (Grotewiel et al., 2022). As noted above, AHQ items often ask about intense focus interfering with tasks; it thus seems important to ask whether experiences of positive, creative, productive flow might differ from these more disruptive hyper-focus experiences. However, in this study's mediation analysis, a greater frequency of AHQ hyper-focus experiences was not only associated with having more negative experiences, but also with having more positive ones.
These semantic and measurement questions also extend to the meaning of monotropism itself. Although the developers of the monotropism account endeavoured to connect some of its tenets to findings from the developmental and cognitive science literatures (Murray et al., 2005), to date, monotropism theory has not been well-linked with constructs from those literatures. However, there have been recent efforts to develop a measure of monotropic tendencies (preprint by Garau et al., 2023). Future trans-diagnostic studies utilizing multiple questionnaire- or interview-based measures of hyper-focus, intense interests, flow, and monotropism, in conjunction with cognitive science attention and executive function tasks, and/or investigations of attention allocation in naturalistic contexts, may be able to clarify the nature of these phenomena and their precise relationships with one another. Future research should also endeavor to develop measures of these attention constructs suitable for children and minimally-verbal neurodivergent people and those with intellectual disabilities.
Limitations
Although the present study has a number of strengths—notably, a large sample size, autistic leadership, good gender representation, the inclusion of a broad battery of measures, and participant groups that are statistically equivalent in key demographic characteristics—we recognize that it also has limitations.
Most notably, in this online study, we had a limited ability to verify participants’ diagnostic group assignments. Diagnostic overshadowing of autism and ADHD can delay or prevent accurate, comprehensive diagnosis (Davidovitch et al., 2022; Kentrou et al., 2018; Rødgaard et al., 2021). Moreover, many neurodivergent people experience barriers to diagnosis (Lewis, 2017), which could also prevent one or both diagnoses in an autistic + ADHD person. To address the issue of poor access to diagnosis, we accepted self-identifications. Furthermore, because participants might be misdiagnosed or unaware that they could meet the criteria for an additional diagnosis, we used ASRS-6 and RAADS-14 scores to exclude participants whose questionnaire responses appeared inconsistent with their identities. However, we encountered challenges in defining inclusion and exclusion criteria; for example, because ADHD people often obtain high scores on the RAADS-14 autism screening questionnaire (Eriksson et al., 2013), we did not exclude ADHD-only participants with high levels of autistic traits. We conducted supplementary analyses using different inclusion and exclusion criteria, which altered some patterns of differences among the three neurodivergent groups. In a sense, given the socially constructed nature of these diagnoses (Chapman, 2020; Ellis, 2023; Grinker et al., 2011; te Meerman et al., 2022), it is not surprising that changing category boundaries led some participants to have more or less obviously neurodivergent phenotypes. Nevertheless, it is unclear how well the definitions used in the main text of the present study match current clinical conceptualizations in the United States. Readers are therefore advised to treat patterns of group differences with caution, especially when they are inconsistent across the main text and the supplementary analyses using different inclusion criteria.
Another limitation is that the present study sample is not representative of all autistic or ADHD people, or even of those in the United States. While our use of curated databases for participant recruitment may have avoided some of the issues that can arise in social media recruitment (see Pellicano et al., 2023; Rubenstein & Furnier, 2021), the present study sample contains a disproportionately large number of non-Hispanic White participants, thereby contributing to the exclusion of racialized minorities from research. Very few people with intellectual disabilities, a highly under-researched population (Russell et al., 2019b), participated in this study. Moreover, our sample also appeared unusually well-educated (although similarly above-average levels of education appear typical of autistic samples recruited online; Rødgaard et al., 2021). Furthermore, a substantial number of participants—particularly in the autistic + ADHD group—reportedly had learning disabilities, and it is unclear whether the written modality of the study might have altered their response patterns, or prevented other participants with learning disabilities from participating. Thus, it is unclear how well our findings apply to many multiply marginalized neurodivergent communities.
One final caveat to consider is that some experiences of hyper-focus may be considered more socially desirable than others (e.g. school vs. screen time). We did not assess whether social desirability affected our results.
Conclusions and future directions
We found elevated levels of hyper-focus in autistic, ADHD, and autistic + ADHD people relative to comparison participants, consistent with the monotropism account. Furthermore, somewhat counter-intuitively, hyper-focus appeared to be positively associated with susceptibility to inattention and distraction. Together, these findings imply that hyper-focus and inattention might at least in part be different manifestations of an underlying atypical regulation of attention involved in both autism and ADHD, though also presenting differently in each. However, further trans-diagnostic research is required to better understand constructs such as hyper-focus and monotropic tendencies, and their relation to executive functions and performance in cognitive and developmental science tasks.
We also explored some of the practical correlates and consequences of hyper-focus. Neurodivergent participants sometimes found their hyper-focus to be productive and enjoyable, but participants also reported many negative effects of hyper-focus, as well as negative effects of intense interests. Similarly, while hyper-focus directly predicted poorer QOL, more positive engagement in hyper-focus mediated an indirect relationship between hyper-focus and greater QOL, partially mitigating the association between overall hyper-focus and worse QOL. Neurodivergent participants reported that their intense interests offered important opportunities for social connections with like-minded others, yet they also had more difficulty finding these social connections, suggesting that efforts to help neurodivergent adults find like-minded peers could be highly valuable. Lastly, we found robust associations between hyper-focus and anxiety, depression, hyper-vigilance, and negative repetitive thinking/rumination, suggesting that hyper-focus may amplify the mental health impacts of the negative experiences neurodivergent people often face. Future research could investigate additional potential correlates of attention and monotropism, such as sensory experiences, interoception, and personality traits; moreover, future studies could explore the social-ecological and contextual factors that might shape whether hyper-focus has positive or negative impacts on particular individuals at particular times.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330241237883 - Supplemental material for A trans-diagnostic investigation of attention, hyper-focus, and monotropism in autism, attention dysregulation hyperactivity development, and the general population
Supplemental material, sj-docx-1-ndy-10.1177_27546330241237883 for A trans-diagnostic investigation of attention, hyper-focus, and monotropism in autism, attention dysregulation hyperactivity development, and the general population by Patrick Dwyer, Zachary J Williams, Wenn B. Lawson and Susan M Rivera in Neurodiversity
Footnotes
Acknowledgements
The authors thank other researchers who contributed to this project, particularly Kathleen Hupfeld, who unhesitatingly shared the latest unpublished versions of the Adult Hyperfocus Questionnaire (AHQ), as well as advice regarding further modifications of the measure. In addition, we thank Tiffany Woynaroski for a suggestion that improved this paper. Most importantly, we thank participants in the present study for their time and for making this study possible, and we particularly thank pilot participants for their valuable feedback. We also thank the Simons Foundation and SPARK Research Match for supporting recruitment in the present study, as they provided this service to us free of any charge.
Author contributions
All authors helped to design the study. PD conducted the statistical analysis with advice and support from ZJW. PD collected study data and drafted the present study manuscript, which was read, edited, and approved by all authors.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ZJW has received consulting fees from F. Hoffman Laroche Ltd. ZJW and PD have received consulting fees or honoraria from Autism Speaks. No other authors have any conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the Autism Intervention Research Network for Physical Health (AIR-P) and by the Tsakopoulos Foundation. Furthermore, the first author's time was supported by an Autism Speaks Royal Arch Masons Fellowship.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.