
Abstract
Background
Health professional roles, organisations and workplace experiences are often studied in conjunction with professional identity (PI) and role theory. This study focused on paramedic PI and role perceptions within the United States context.
Methods
The exploratory qualitative case study data included 15 semi-structured interviews with practising paramedics in EMS contexts.
Results
The data is presented in five categories and 23 subthemes. Data categories included exploration of why paramedics were drawn to the profession, envisioning eventual exit from paramedicine, discussion of paramedic PI perceptions in relation to professional insiders, to first responders and to hospital-based healthcare professionals.
Findings
The study findings drew upon data categories to theorise four overall findings about participant PI and roles: (1) ‘I know that what I do is important!’ reflecting paramedic expressions of an inner reservoir of strength surrounding the importance of their work, even if the personal motivations for working in EMS are varied, (2) ‘My primary role is care of the patient’ indicating strong identification with a primary role as patient caregiver that serves as both an enduring positive foundation for identity and a constant role dissonance stressor, (3) ‘The respect I receive is variable and conditional’ suggesting a capacity to not only cope with, but to leverage a shared sense of being unevenly respected by other professionals into patient advocacy and a quest for excellence; and (4) ‘In my role, I have to function well with a fluctuating locus of control’ signalling that PI partially rests in an ability to shift identities in a fluid way because the locus of control and roles paramedics occupy throughout their environments vary constantly.
Conclusions
The findings contribute valuable information that may be used to address paramedic workplace stressors, enhance professional capacity building and to adapt paramedic environment structures and policies.
Introduction
In the United States (US) as well as globally, paramedic professional roles have undergone significant changes, encompassing complex clinical decision-making, interprofessional collaboration and community-based care services.1–4 The concepts of professional identity (PI) and professional identity formation (PIF) have been studied quite extensively in health professions and in the fields of teaching, social work, pastoral care, genetic counseling.5–7 The body of work underscores how deeply interconnected and meaningful work, workplace environments and individual experiences are within professions that serve others. Specific to paramedic PI, the majority of research connects to training and education requirements, licensure, pay structures, self-efficacy, job satisfaction, capacity for managing stress, cooperation and collaboration styles, and is internationally based.8–11 This empirical research contributes a qualitative case study focused on how paramedics in the United States describe and reflect upon their professional identities.
Literature review
Professional identity
PI is defined generally as the meaning and self-concept associated with a role or membership in a profession.8,12 We conceptualise PI analogous to Mancini et al.'s work 13 (p. 141) which defines PI as something which ‘describes both one's awareness of being a worker doing a specific job and one's identification with the groups and social categories to which one belongs by virtue of one's job’. In key foundational scholarship McCall et al. 14 argue that identities are not fixed, they are organised based on the salience or central importance of a particular role to the self. Identity is then created through navigating expectations via interaction. Research by Donnelly et al. 15 also finds that role identity theory, the multiplicity and salience of roles occur via repeated interaction with one's environment. The unavoidable blurring of PI and PIF add a measure of intangible benefit and challenge. PIF extends beyond the rhythms of transitions in a profession and serves as a mediator to a range of experiences, perceptions and shared knowledge. Sustaining a sense of stable identity as it evolves over time and circumstance is vital to the well-being of workers serving in high-demand, high-stress occupations with a sense of responsibility for others.3,7
Professional identity and role theory
One useful way to approach the study of PI is the exploration of role theory. Occupying a role carries internal elements as well as relational and performative elements. Roles can provide a sense of direction, comfort or discomfort, and often serve as unconscious scaffolding for our decision-making and senses of anxiety or peace.
More specifically, professional experiences may be analysed in relation to the presence of intra-role and inter-role conflict. Intra-role conflict is the presence of or perception of differing expectations for a person occupying a professional role. It is more likely to occur when professionals are accountable in some manner to more than one stakeholder or line of authority. Inter-role conflict is defined as the tension between multiple roles in different domains, for example work-life balance. 16 Exploring these two types of role conflict can be useful in management of work-related stress, or in providing strategies that can be utilised to address role conflict. 17
Relevant studies utilising role theory also include the concept of role ambiguity16,18,19 which guides analysis of what happens when individuals have a lack of clarity or insufficient information about their role expectations. Practically speaking, role dissonance occurs when who we believe ourselves to be isn’t aligned with what we do, creating inevitable changes as a result of those gaps.20–22
Role exit calls attention to individuals’ departure from roles that are meaningful or central to their identity 23 (p. 149). Ebaugh's (1988) study of role exit includes categories of enquiry surrounding individuals’ elements of doubts, seeking alternatives to their current roles, turning points of catalysts in leaving, and in subsequent new identity formation. This is specifically relevant considering the stressors within the paramedic profession. In a recent study, researchers identified several components to the process of law enforcement role exit – disengagement, symbolic decoupling and celebration 23 (p. 306). In a high stress occupation, understanding the process and experience of contemplating or exiting a professional role offers the possibility of informed change.
Finally, role-theoretical concepts also include analysis of cross-occupational collaboration competency (COCC), which frames self-awareness and the development of role knowledge and role skill dimensions as essential to successful or meaningful workplace collaboration. 24 Aspects of COCC are applied in research about aspects of health professional experience, including workplace culture, ethical decision making and paramedic education.25,26 Striković et al.'s 24 recent research expands on their previously proposed framework about occupational structures by focusing more deeply on the latent degree of distance in roles and the pluralistic or nuanced perspectives needed to work collaboratively in professional settings. This serves as a potential bridge to other aspects of role theory when applied to studies of PI and PIF in healthcare. It also aligns with the elements of symbolic interactionism that underlie PI and PIF research.
Authenticity and professional identity
Studying authenticity and PI invites curiosity and analysis of how professionals cooperate, compete, generate trust, sustain loyalty and perform in tandem with one another. It can serve as a mechanism for explaining the implicit heaviness that is a part of many health professional roles. Authenticity, concordance and self-determination theory all offer insight into the ways we construct our professional selves and relate to those in our environments.27,28 Similarly, Mancini et al.'s 13 identity status research extends analysis of intra-individual and intergroup processes, creating a line of research that ties vocational identity to identity formation. They suggest practising PI while students (pre-professionals) are pivotal in PIF. It has implications of the extent to which professional preparation programmes shape and allow for individuals to explore and commit to both procedural knowledge and application 13 (p. 148).
Professional identity and paramedicine
In the context of paramedicine, identity formation is uniquely complex due to the field's hybrid origins.1,3,9,10,29,30 Within the United States, paramedics situated within Emergency Medical Services (EMS) systems fall under medical direction oversight whether serving in fire department-based systems, local government (county or city) or hospital-based. 31 This is expanded by discussions of academic formalisation, changes in credentialing, expanding parameters of professional autonomy and new professional pathways. There are emerging new ideas around what it means to ‘be’ a paramedic today.
While internationally paramedic professionalisation and opportunities are expanding, paramedics in the United States operate within a context that often marginalises prehospital care. This structural positioning and culture influences how paramedics see themselves relative to other health professionals, such as nurses or physicians, and affect their ability to advocate for their role within interdisciplinary teams. 32 It results in a complex dynamic and negotiation of status, legitimacy and professional boundaries, all of which are central to PIF.
The current US context raises concerns surrounding retention and burnout. Recent US 2022 survey data indicates that EMS personnel demonstrated high burnout across multiple domains, absenteeism and 15% of EMS clinicians reported an anticipated intent to leave the profession. 33 Yet another study indicates that ‘job satisfaction was the most significant predictor of leaving for EMTs and paramedics’ and agency type served as another predictor, with those working in hospitals, non-fire agencies and private agencies more likely to leave their roles 34 (p. 3). Studies indicate that paramedics are at unique risk for mental health and stress related issues, and this ties to other types of first responder and parallel occupations 15 (p. 213). In Donnelley et al.'s 15 research, they frame the study of paramedic professionals within role identity theory – and examine the salience and potential dissonance of paramedic roles. Through their quantitative research, they theorise four domains of paramedic or EMS role identity: caregiving, thrill seeking, capacity and duty as central to paramedic role identity. 15
Townsend et al. 35 and Reed et al.3,36 have steadily contributed to the study of paramedic professionalism, changes to the profession and PI particularly in the Australian context. Townsend et al. 35 argue that paramedics often face an identity tension between their technical, lifesaving image and the emergent expectations to be reflective, autonomous practitioners. This duality can lead to ambivalence in self-perception and a lack of coherent PI, especially when educational standards and regulatory bodies fail to align with evolving practise realities. Although Townsend's work is situated outside the United States, similar identity tensions are evident in the US context as well. 2 According to Reed et al., 36 scope of practise, employment and membership in a particular agency or ambulance service are crucial influences on identity formation. In their research, Reed et al. 37 advance data suggesting five aspects of paramedic identity – professional registration, qualifications, employment, membership of a community of practise and scope of practise were found to be key aspects of PIF. Hill et al. 1 reframe broadly by asking the question of what it is like to be a paramedic, and how might we probe more philosophically and deeply into paramedic experiences.
Methods
Research design: case study paradigm and research question
This study is epistemologically rooted in interpretivism, with acknowledgement that each participant may have their own perspectives in what may be seen as similar situations and contexts aligned with the paramedic world. Even in a close-knit professional environment with shared similarities, identity is a distinctively personal endeavour. It was our hope to carry out research that would elicit substantive, thoughtful responses to deeply meaningful paramedic PI topics.
Congruent with an interpretative and constructivist orientation, we aligned closely to case study method as theorised by Merriam. 38 Our case study design combined Stake's 39 characteristic of holistic exploration of the relationship between the topic and the context and Merriam's 38 heuristic emphasis on striving to engage the reader in understanding the nature of the experience from the perspective of the participants. 40 We further aligned the research design with the notion of ‘flexible’ design, anticipating intangibles and a need to reflect and tease out nuances in our approach. Drawing from an integration of PI and of role theory literature, the research question for this case study was: How do paramedics in an EMS context perceive their professional identity as individuals, and as members of their occupation?
Data collection design. Within the semi-structured interview (Appendix 1) design, questions were grouped as related to individual perceptions of PI (the self) or perceptions of PI in relation to others (group), loosely mapped onto supporting literature. By design our interview protocol emphasised the emergent prehospital context of practise. We aimed for 12 to 20 participants which is within a range posited by Hennink et al. 41 as an appropriate sample size for qualitative research. Regarding participant recruitment criteria, we arrived at a research protocol decision based on our belief that it takes time in the workplace to develop and evolve a PI and that perspectives from paramedics with a current EMS practise context were important for the credibility of the data as well as for participants’ capacity to articulate their experiences. This choice aligned with the research goal to discuss PI as it is unfolding, rather than retrospectively looking back. In this case, we relied upon Goyes et al. 42 work addressing the distinctions between recursive, repeat and retrospective interviewing distinctions. We recruited from two different states, with a goal of variation of experience levels and practise settings. Recruitment was done via occupational subscription to an electronic email list.
Based on the above, volunteer participants for the study were: (a) licenced paramedics from two states, (b) working in a current EMS practise context, either part-time or full-time. Beyond these criteria, there was variation in paramedic professional setting and educational background among participants.
After conducting the first five interviews, we paused to analyse and assess the protocol and then resumed participant interviews. We stopped recruiting at 15 interviews based on researcher determination that saturation had occurred in three ways: (1) redundant participant data, (2) theoretical data not yielding new coding categories, and (3) researcher determination that participant interview engagement was authentic and comprehensive (Saunders, 43 Hennick et al. 41 ).
Data analysis strategies. The analytic strategy, based on Saldaňa 44 was collaborative with each researcher independently tagging, labelling and noting observations in an initial review of transcripts and video recordings and then jointly discussing and reconciling observations and interpretations. We repeated this inter-coding process iteratively through all phases, including manuscript preparation.
Initially we utilised an axial or category-based coding strategy based on an adapted list of professional role theory and PI characteristics and concepts and reliance upon Saldaňa. 44 Then we engaged in elaborative coding to refine the study categories and concepts in relation to existing research literature.
Research rigour. We focused on trustworthiness as a measure of quality and rigour. As a part of that, we followed an accepted intercoder process and aligned with investigator triangulation and theory triangulation practises to ensure that the study data was carefully collected, analysed and reported.45,46
Researcher positionality statement
This study is team-based research that rests within a shared larger research agenda focused upon investigating the human element of paramedic experience. We research the sociological, experiential and workplace aspects of being a paramedic. The goal is to increase visibility of paramedic work and contribute to paramedic working life, to education and to related policy deliberations. One member (first author) brings more than 30 years of combined professional experience as a credentialed paramedic in EMS and critical care settings, a paramedic educator in both the community college and university settings, and a researcher. The other team member (second author) contributes more than 30 years of relevant experience as an adult and lifelong learning specialist with a longstanding emphasis on health professions education in addition to adult education settings. As a team, we have established a flow which includes intentional independent and collaborative engagement at every phase from conception to disseminating research. In this specific study, we engaged in strategies at every step to ensure that we are critically examining our choice of literature and supporting theory, of research question formation, of appropriate conceptual framing and research design strategies and in the interpretation, coding and presentation of findings.
Ethical approval
Institutional Review Board approval #27388 was sought and obtained through North Carolina State University prior to initiating this study. Participants provided verbal informed consent prior to participation.
Results
Study participant overview
The semi-structured interview transcript data included interviews with 15 participants, 6 females and 9 males, for a total of 825 interview minutes, with an average interview length of 55 min. The participants average 13.6 years of paramedic experience. All participants have served as paramedics in EMS with 911 first response agencies and four participants have alternative practise experience such as Emergency Room, community paramedic or critical care transport. Table 1, Demographics and Participant List, presents an overview of the study participants (pseudonyms), years of paramedic experience and paramedic practise context.
Demographics and participant list.
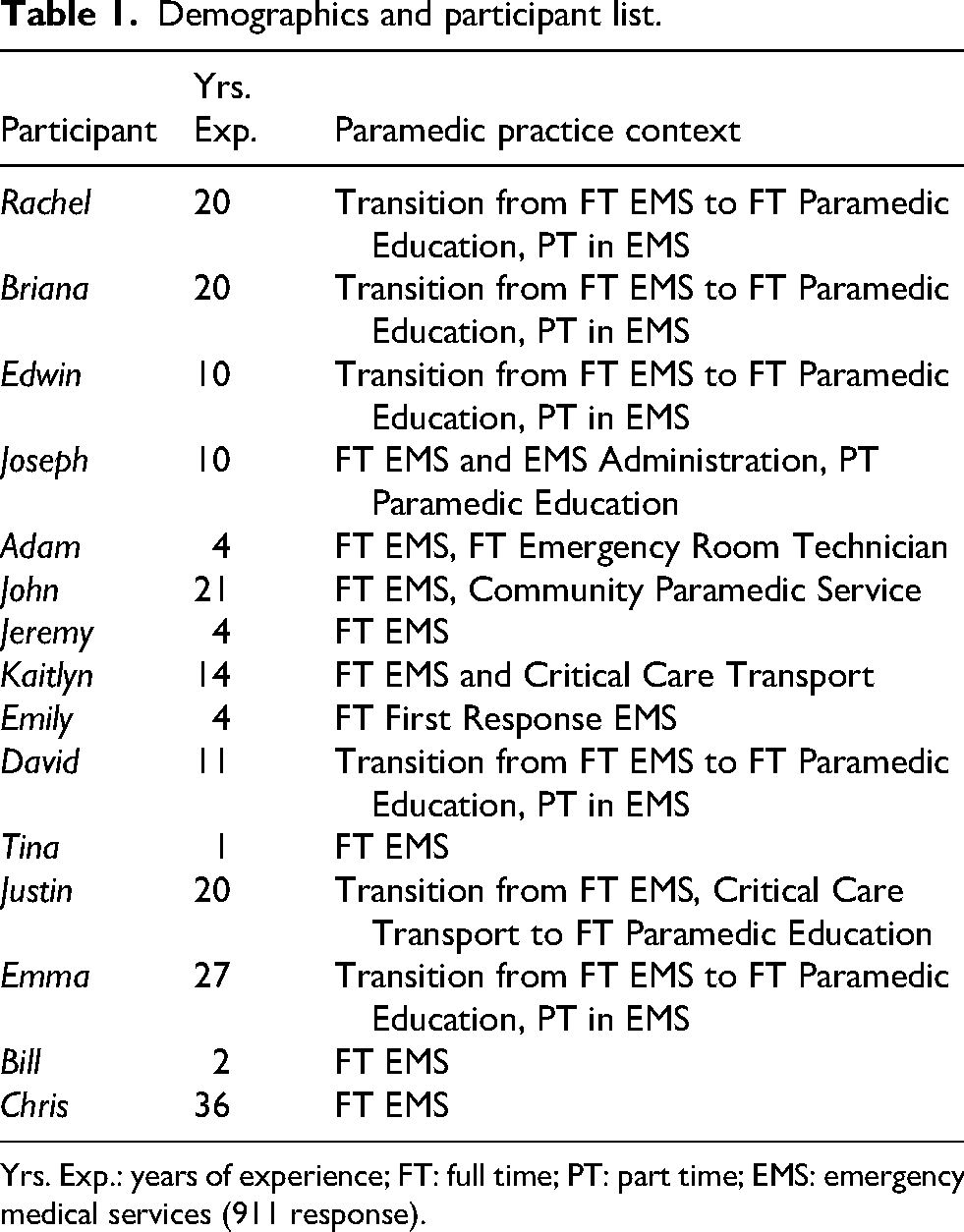
Yrs. Exp.: years of experience; FT: full time; PT: part time; EMS: emergency medical services (911 response).
Data categories
Self in relation to career…how did it start? And, how will it end? Early in the interviews we asked participants about what led them to choose a career in EMS and how they imagined they might end up leaving their career in the future. The responses varied considerably; we clustered them into subthemes. Edwin shares,
Part of the struggle I have with our profession is we forget why we do what we do. Why we were called and why we want to serve. I live with mine every day – relates storey of his son. I don’t know if my storey is unique as to why I came into EMS, if you can’t honestly say that you’re here to help people, then you’re in the wrong business.
For Edwin, his son's emergency care led him to his career choice as a paramedic, and to his strong sense of duty or service as the driving force behind what it means to be a paramedic. In contrast, David witnessed an emergency and response and was drawn to what he perceived as the importance of the role being ‘something different’ and not just ordinary service. David shares,
I was in [high school] and on the way to a scout camping trip, and the vehicle in front of us struck a female pedestrian going about 55 miles per hour. There's actually a private ambulance on the other side… our troop leader is like, ‘Don’t look. Don’t look.’ I’m sitting there looking, because that's what I want to do [law enforcement]. Law enforcement showed up pretty quick, and all 30 of them sat there, and one group talked to the driver, a couple did traffic, and the rest of them just sat there talking…I saw fire and EMS roll up and started watching things… I want to do that! Not law enforcement– paramedic.
Other participants described their entry into the profession as a career decision – either because someone they knew was already a paramedic, or they happened to receive career advice, fell into it and thought it seemed like a good idea at the time. John said,
I totally derailed on my radiology dreams and career path and signed up for paramedic school. Started out, you know, just as an EMT in the Summer after I graduated high school, kind of sealed that deal and I really loved it, and the rest was history.
For Briana, it was simple, ‘I grew up around EMS because of my Uncle {xx} and just really always wanted to do what he did’. Bill recounted, ‘When I joined the EMT programme, started working. With that, I began developing a passion for it. I just love the adventure of being in the back of the ambulances and being able to practise medicine’.
A cluster of responses focused upon the need for challenge, uniqueness or excitement in their work. Jeremy shares,
…realised very quickly that I liked this high adrenaline getting to actually care for people and making a difference when there wasn’t another unique resource to do so. Doctors are super. Nurses are super in their field, but when you’re dying on your living room floor…there's not a nurse in that hospital that is going to be willing to come and work in filth on somebody's floor while they have a heroin needle in their arm.
John saw it as an adventure, one where you ride the energy,
If you like adventure, and not really knowing what's going to happen next…that's what still draws me to it. I still love that level of suspense. If you’re an adrenaline junkie and just like to go into the unknown. This is for you.
Edwin, Rachel and Emily shared the belief that being a paramedic is a calling, and to some degree all other participants conveyed in various ways how important the deep sense of commitment and duty is as a part of their professional identities.
John expressed it as:
…it just kind of has to be who you are as a person. You can’t learn that if something that has to be in your heart, it kind of has to flow… kind of felt called into this career field.
Kaitlyn states,
I would definitely say, it has been the hardest, but most rewarding thing I've ever done in my life.
Participants also described what it meant to them, how they imagined exiting their role as paramedics – distinguishing and explaining that being ‘on the truck’ as their core paramedic identity. We grouped responses into four categories: It's physically, mentally and emotionally intense – so I’ll know when it's time to go; it's a [career] steppingstone; I don’t ever want to leave it completely; and, I want to sustain a sense of purpose, for what I do is [that] meaningful.
Adam explains, ‘I don’t know that I will retire as a field medic. I believe that this is definitely a steppingstone into possibly the administration side’.
For John, his vision for his future was a little different, with a desire to serve as a community care paramedic.
I hope it ends in the role that I’m in right now as a community care paramedic…you really get to know them as a person and you can see you’re impacting their health by making sure they’re taking their medication, making sure they can afford their medication, making sure they have food in their house… It makes you feel good, that's what I like…just look back over the years and just hopefully see that you’ve made a difference in people's lives, and not dwell on what you could have done, but dwell on what you did do. So it doesn’t destroy you inside.
Emma describes the sense of loss she imagines when she no longer identifies as a paramedic.
So I when I am no longer a paramedic, when I no longer have that professional identity that is internally strong in our profession. Who, then, am I? Who is Emma outside of being a paramedic? If someone says to me, ‘Tell me about yourself.’ The 1st thing out of my mouth is ‘I'm a paramedic’. (refers to wearing EMS t-shirts) It's pride. I want everyone to know that I'm a part of this. This profession is pride.
Being a paramedic is like… Participants discussed at length what it is like to be a paramedic as perceived from different vantage points. One vantage point we sought was asking participants to share how they might imagine explaining their roles to someone outside of the EMS world, for instance a patient or a neighbour. Another perspective was what they felt their roles and identity were as seen as by others in the first responder world (fire and law enforcement). Another looked at ‘what it was like’ from the vantage point of health professionals in receiving hospitals or other professional contexts. Overwhelmingly, there was a sense from participants that being a paramedic was inexplicable – something so unique that others would either not understand or perhaps have limited understanding of what it is like and what it means to be a paramedic.
The variability across the responses was considerable. Some participants saw paramedicine akin to other health occupations. Joseph compared EMS to nursing:
EMS is very similar to nursing. In some cases the environment is, I would say, a little bit more unpredictable than that of what would be in facility. I would also argue that the policies and the governmental oversight of EMS from a national perspective is very different from nursing as well.
Jeremy explains it slightly differently,
My other favourite comparison is feral nurses on a truck. Hours of boredom, followed by moments of sheer adrenaline, which kind of fits if I had to describe it.
In the alternative, others focused upon the uniqueness of EMS. Adam states,
I would ask them if they know what a pharmacist is, if they know what a general surgeon is, if they know what an ER doc is…a respiratory therapist…a pediatrician…a neurologist is? I would say, put all of those little pieces into one person and throw them into the community. You’ve got it …put an ER on wheels. That's what I do.
For David and Briana, it's about service and their focus was upon patients and their communities. They talked of it with a feeling of compassion with some chaos thrown in.
David discussed it ‘…they call us, complete strangers, to come in. So to me it was an honour to be a paramedic, you know. It's a privilege where someone needs you the most, and you can just enter whatever situation they’re in provide aid and get the higher level of care….’
Paramedics Briana and Tina focus on the concept of being a part of a larger team. For Tina,
It feels like everyone is on the same page, and you're all trying to work towards a common goal, even though there's a lot of chaos around. You're trying to manage the chaos, and everyone has their role that they fulfil. It's really cool when everything works and everyone does what they're supposed to. You can kind of like be very efficient and manage everything and help people.
For Briana, ‘I don’t think you can do it alone, like I think anybody who thinks that you can is crazy…it takes a team of people, especially on those critical calls’.
Joseph saw a clear delineation of roles, ‘each different responder that comes to the scene has their own specific value to provide to the scene and overall care of whatever's going on’.
Justin and Chris see the paramedic as a leader,
Chris: In the moment you got to call the shots and just do it, and then you can worry about your fears and did we do it right? Did we do it wrong?
Justin: I'm the orchestra conductor. Yeah, we've got multiple vehicles, multiple patients. Hopefully, I can trust that law enforcement is doing their traffic control and safety thing. I can trust that fire is in charge of heavy rescue and extrication. I'm also assuming I'm 1st on scene as a paramedic. I'm the conductor going, ‘Okay, what's the what's the big view?’.
When it came to receiving hospitals, the sense of PI in relation to others shifted considerably. Nearly all participants described a concern about receiving less or at times no respect as well as a concern about the complexity of communication and being ‘heard’. Participants spoke intensely about the priority that credibility be established due to the crucial importance and inherent difficulties of the hand-off. When asked about assertiveness and/or patient advocacy, participants’ language and tone was noteworthy. All participants spoke intensely about ‘advocating for’ or ‘fighting for’ their patients to explain their identity as a professional and the relationship between asserting oneself with others and being an excellent paramedic. Rachel explains,
Being a patient advocate, you have to dive into that and be like, if this were my mom, my dad, or myself, what would I want done? If they want you to go send a patient to Triage that you know's got chest pain and you’re looking at their 12 lead, and you’re going…there's something here. My gut instinct is, I will hold that wall until they get me a bed, because my gut instinct is never wrong.
Joseph's explanation regarding the identity shift is clear, regarding respect for being a paramedic,
I feel… EMS itself is valued lower on the totem pole within the hospital. Traditionally we would hand off our care over to a nurse or a doctor. In the hospital, we’re viewed more of first responders than medical personnel.
Briana echoes this, ‘I have been made to feel inferior to a nurse, because you’re a paramedic’. John expresses frustration,
You just cannot get them to see the big picture. I mean, I think they just think we throw band-aids on and rush to the hospital, and then they have to do everything else, no matter how much we do. I don’t think we will ever be that respected partner in healthcare.
Kaitlyn and Edwin's experiences were more positive, stating that everyone knows their role and offers to help in the spirit of teamwork. To Kaitlyn, it comes down to communication and finding a way to cross that divide. And to Edwin, relationship building and building a reputation can make all the difference. Across the spectrum, participants believed that their ability to communicate, project a professional appearance and gain education earned respect. They felt most respected and understood by their patients and by their crew and partner, in their reception on the scene, and less understood and respected within receiving hospitals. Participants didn’t discuss this as a simple process – pointing to the fact that during the trajectory of one call, they were shifting identities and their behaviours and attitudes in response to others’ perceptions of paramedic identity as they navigated calls. Emily explained it like this:
In healthcare, in general {it} tends to view paramedics as more of first responders, and they don’t understand the extent of interventions that we can do in the field…with a great deal of autonomy, a strong emergency component to it. I mean, that's the backbone of what paramedicine is that we’re going to respond to any emergency and we’re going to get those people to definitive care.
Other participants spoke more directly of the ways that their identities were not fixed, stating it depended upon the evolving context and whether they were within their ‘own’ environment with each other or patients, or with first responders and hospital settings. David states, ‘You've got healthcare on one side, and you've got public safety on the other, and we really do fit either category’.
Briana explains this, discussing how it is more about being able to navigate a flexible role and identity:
Sometimes you’re the mental health counsellor. Sometimes you are providing life-saving care. I think it's broader than it was when I started in 2005.
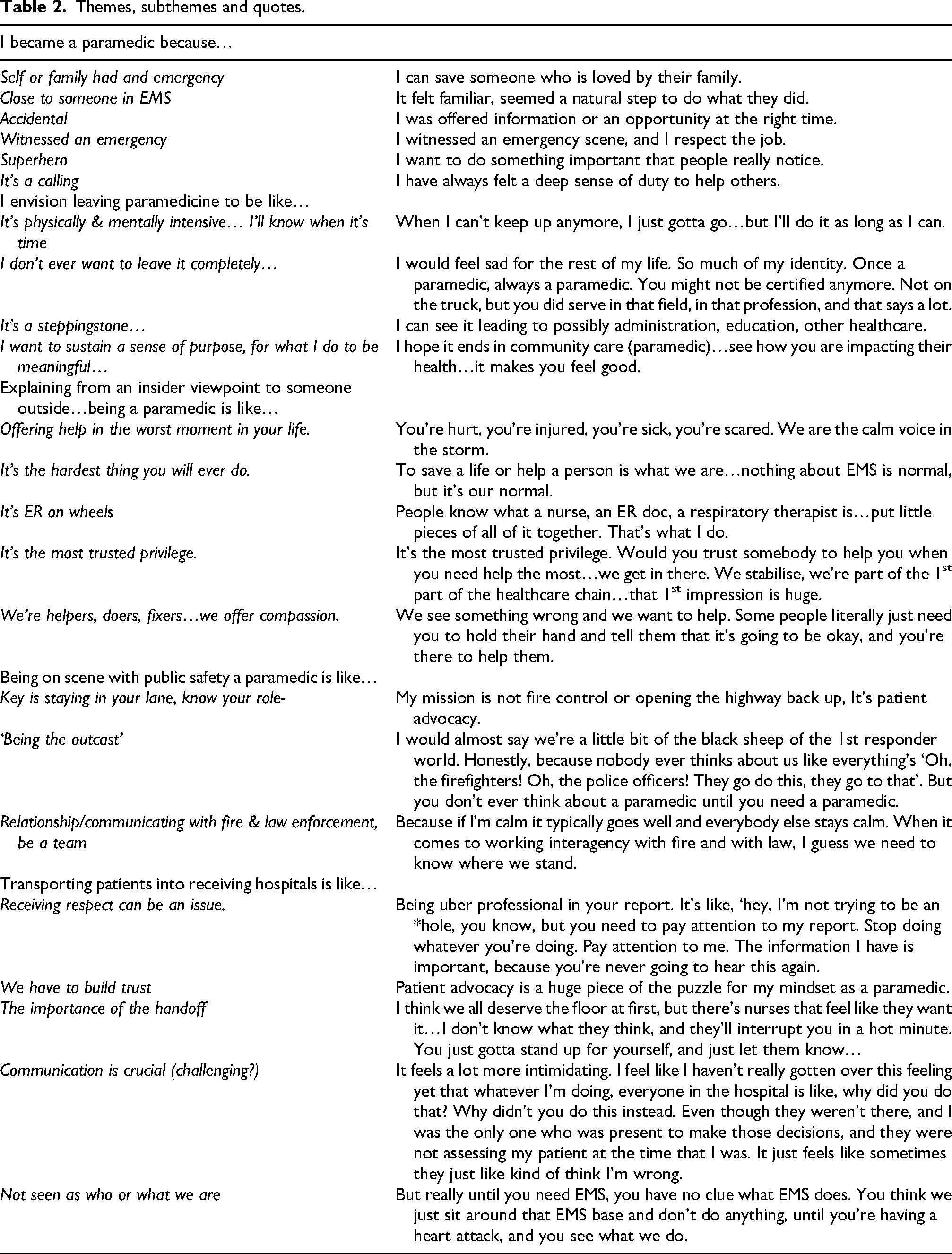
Table 2 presents a synopsis of the data categories, subthemes and illustrative quotes.
Themes, subthemes and quotes.
Discussion
Data categories presented above included exploration of why paramedics were drawn to the profession, envisioning eventual exit from paramedicine, discussion of paramedic PI perceptions in relation to professional insiders, to first responders and to hospital-based healthcare professionals. Analysis of the categories then led to four findings, which are an expression of the paramedic participants’ concepts of PI. The four findings are:
‘I know that what I do is important!’ reflecting paramedic expressions of an inner reservoir of strength surrounding the importance of their work, even if the personal motivations for working in EMS are varied, ‘My primary role is care of the patient’ indicating strong identification with a primary role as patient caregiver that serves as both an enduring positive foundation for identity and a constant role dissonance stressor, ‘The respect I receive is variable and conditional’ suggesting a capacity to not only cope with, but to leverage a shared sense of being unevenly respected by other professionals into patient advocacy and a quest for excellence; and, ‘In my role, I have to function well with a fluctuating locus of control’ signalling that PI partially rests in their ability to shift identities in a fluid way because the locus of control and roles paramedics occupy throughout their situational environments vary constantly.
Viewed in this manner, there was an unpredictable dynamic flow to paramedic PI. Participants may have had unique individual approaches to sustaining these elements of PI, but the four conceptual findings appeared to be the ‘glue’ that held the elements of their identities together. Figure 1 illustrates the paramedic professional identity.
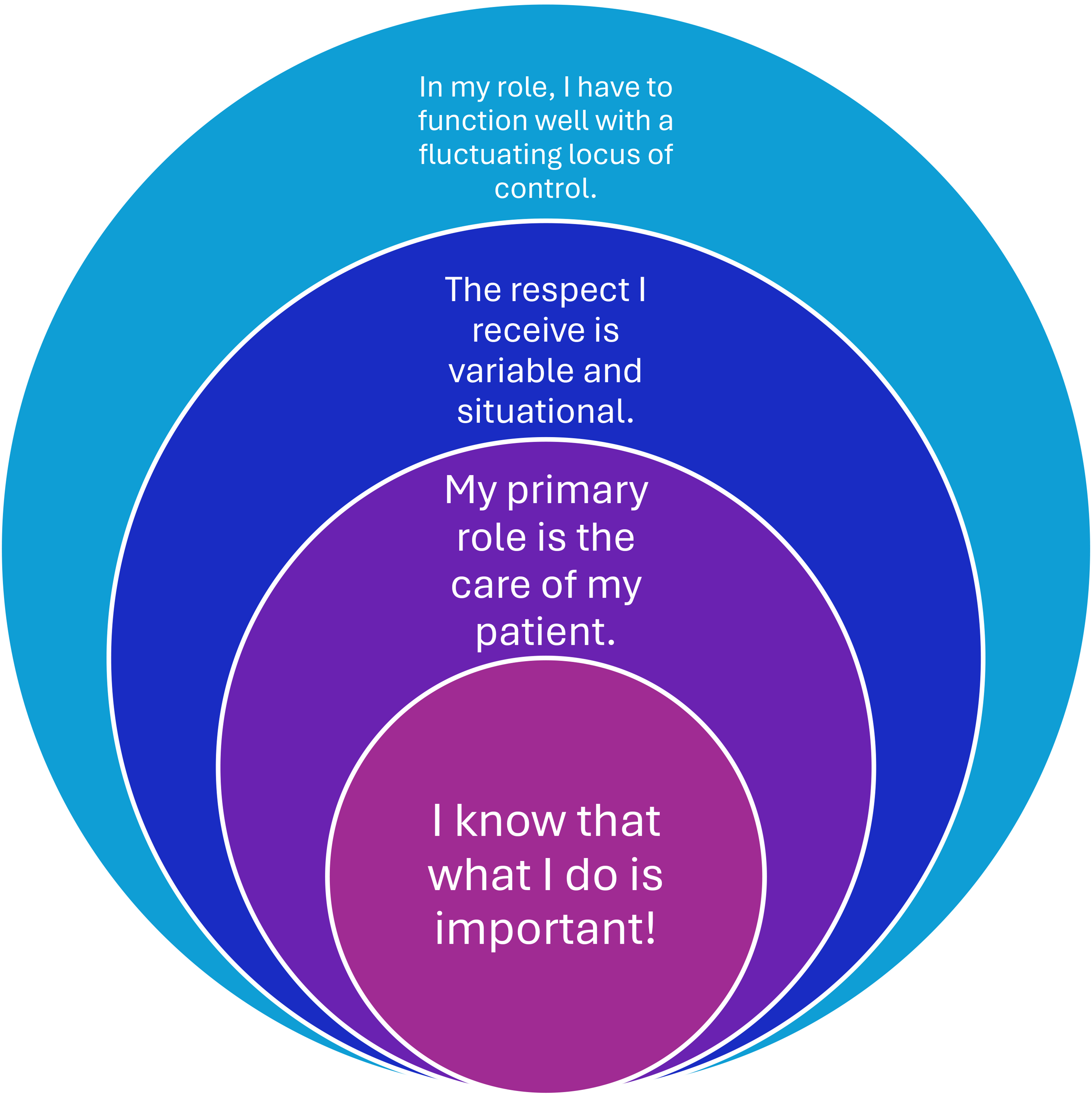
Paramedic professional identity – findings organised into four concepts.
It is generally understood in the United States that there is a ‘revolving’ door of sorts for paramedics. This has led to studies aimed at addressing burnout, moral injury, or structural practises and policies that may lead to the loss of paramedics from the workforce. Mausz et al. 21 investigated role dissonance as a cyclical process in forming and sustaining paramedic PI. Our findings generally echo their discussion of role dissonance's influence on mental health issues, absenteeism, disillusionment, stressors or exit from the profession. While our participants clearly showed evidence of what could be categorised as role dissonance, the data also led our analysis into a new direction.
The juxtaposition of participants’ discussions of vantage points of the self and self in relation to others lent insight into the experience of being a paramedic. The data suggests that entry and belonging to the profession is perceived by paramedics as unique and meaningful in some way, even if arrived at serendipitously. PI was envisioned and described as privileged, challenged, offering help, rescue and compassion. There was an air of mystery/being misunderstood. An imagined exit corresponds to PI as well. For example, by leaving the profession when it becomes too much or ‘is time’ or holding onto a sense of purpose by shifting roles within the EMS arena. In either case ‘once a paramedic, always a paramedic’ asserts an authentic, powerful, lasting PI that has become inseparable from the individual. Role exit theory logically focuses upon the exit process, and our interpretation of the data leads us to making the suggestion that there is prolonged role limbo. We defined role limbo as being tied to an unfulfilled desire for role exit or the ongoing influence of imagined role exit as an important influence in paramedic PI.
There is a duality to the idea that participants’ belief in the unique aspects of EMS was so strong regarding others’ weak grasp of the nature of their work may also be a factor in paramedics’ interpersonal struggle with profoundly difficult and rewarding experiences. There were varied indications that participants accepted role dissonance without fully addressing it due to a belief that it naturally intertwines with EMS roles. When discussing the circular nature of PI, paramedics run the risk of trying to sound as if they are ‘all things to all people’ as generalists due to their fluid roles and responsibilities. This echoes Tavares et al. 4 research finding that paramedics can be seen to occupy six different roles to include clinician, team member, health and social advocate, educator, reflective practitioner, and professional. 4 Recent research publications by Bolster et al. 47 and Nudell et al. 48 focus upon the multifaceted value of enhanced professionalisation in paramedicine. Of importance, the recent establishment of an American College of Paramedics is an initiative that allows growth in professionalism and career pathways by building upon examples such as Career Frameworks in Canada or the UK and Australasian Colleges. Many of the PI challenges identified in this study could be further studied and potentially addressed in alignment with concepts of professionalisation, education, career pathways, unique stressors, and roles in policy and decision-making.47,48
Paramedic participants described the jarring unpredictability involved in their work. Their identities were intertwined with reconciling how others perceived paramedics’ identities and roles. These differences influenced their communication, trust, leadership, and professional boundaries. The data was compelling and vivid – the receiving of respect was indeed variable and situational. It had to be reconciled in numerous ways as a part of participants’ PI. The struggle also potentially served as internal motivation for excellence. This aspect warrants further investigation and could be better understood in the future if studies connect to concepts of professional socialisation and related analyses of how prior or anticipatory socialisation, idealism and mission play a role in paramedic PI 49 (p. 371–372).
As paramedic descriptions of their work unfolded, our analysis established that paramedics understood and cultivated their own capacity for giving, relinquishing and reclaiming control of their autonomy and authority. The participant perspectives focused less upon control associated with agency or hospital policies and practises and more as a demanding situational reality that required developing deep professional capacity. This was evidenced in language positioning, descriptions of assertiveness, desire for teamwork and collaboration. Advocacy was strongly salient in data surrounding ‘the handoff’ at hospitals. Juhrmann et al. 50 research findings contribute five categories of paramedic identity, with two of them especially relevant to our research: the tension or dichotomy between a life saver and community responder identity, and ‘the harsh reality’ of navigating their role in a limited or siloed environment. Another potential framing for future research in this area might align with delving more substantively into concepts of authenticity and concordance.
We initially consulted interprofessional healthcare literature to guide interpretation of paramedic PI in relation to adjacent professionals such as first responders and hospital healthcare workers. We identified a paper that detailed research on cross-occupational collaboration that contributed to our finding development in two ways. 24 One, paramedics are often the only person other than the patient that is present and engaged in both the field and the hospital and this limits the knowledge and role-taking abilities for other professionals to observe and reflect upon the totality of the paramedic role/s and experiences. Two, the determining factors in coordinating care is at its most difficult for the person with the role that assumes responsibility for coordinating care and navigates the highest number of collaborative partners, as well as navigates lateral and vertical roles all within emergent circumstances. The more latent distance a healthcare worker has from prehospital setting conditions the more difficult it is to relate to and explain role differences. This lends explanatory power to the ‘role making’ tendencies for paramedics assumed identities not just as caregivers, but as care advocates. We then combined these cross-occupational perspectives with empirical arguments by Rai 18 positing that role conflict and ambiguity are potentially reduced in organisations and structures that practise ‘organisational virtue’ (p. 511). In Rai's 18 (p. 511) framework organisational virtue is a metatheory and can be thought of in two ways – amplifying and affirming positive and prosocial behaviours and by buffering or deflecting and protecting organisational members from negative dimensions of their work. The second way of considering organisational virtue and the role of organisations, suggests agencies and hospitals may bear enhanced responsibilities in creating conditions that nurture healthy and productive roles and relationships among those who share caregiving and lifesaving responsibilities.
Strengths and limitations
This qualitative study has limitations that should be considered. Expansion of geographically diverse participant profiles beyond two states may have yielded additional data depth or breadth. Next, while the focus of interviews related to experiences in paramedic EMS practise, perceptions of PI that relate to alternative practise setting, education acquired, or experience as a paramedic educator cannot be separated and may influence responses. Finally, while helpful, the use of role theory and integrated PI concepts as selective coding may potentially preclude alternative explanations of the data from additional theoretical lens.
Conclusion
This paper invites others to learn about and consider paramedic experiences as they relate to PI, and we aimed to share a paramedic-centric perspective. Conceptually, this study expands interpretations of role dissonance in connection to self and self in relation to others, and in cross-occupational collaboration and organizational virtue. It suggests further consideration of PI in relation to role exit theory. Finally, this study points to the vital importance of further aligning current daily practice, expanding notions of professionalism and policy evolutions inspired by international exemplars.
Footnotes
Acknowledgements
The authors would like to acknowledge the paramedics who shared their experiences in this study. The authors would also like to thank the reviewers and editors for their meaningful feedback during the review process, which strengthened this article.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.