
Abstract
Ambulance clinicians may have to apply coercion while delivering healthcare. However, coercion is a source of stress for all involved. Challenges include unclear legislation, lack of training, equipment, support, not least ethical dilemmas. This paper explores factors influencing ambulance clinicians’ experiences of exercising coercion. An anonymous online survey was conducted between Oct 2021 and Nov 2022. During a six months period, 488 ambulance clinicians reported using coercion, and 431 answered a free-text response question about their experience. Using Graneheim & Lundman's analysis of qualitative content, 376 answers were analyzed. Three overarching themes were identified. First, ambulance clinicians reflected on what constitutes healthcare and how they perceive their professional role, including the idea that coercion can, in some cases, be a legitimate form of healthcare; at the same time, clinicians expressed concern about patients’ experiences, and described feelings of powerlessness. Second, participants highlighted encounters and situations that they found especially distressing, often due to ethical ambiguity. Third, the experience of exercising coercion was shaped by various contextual and structural conditions concerning equipment, legislation, insufficient training and expertise, as well as the complex impact of police involvement during critical incidents and lack of support. Social identity theory was used to understand how the described challenges influenced the use of coercion and shaped ambulance clinicians’ professional identity at the individual, service, and societal levels. This identity was challenged across all levels. Clinicians often found themselves in situations where they felt morally conflicted, underprepared, and isolated from the wider healthcare system. These findings underline the need for integrated strategies that address coercion through a multi-level lens. Clinical implications include the implementation of structured ethical reflection, improved training, adequate equipment, and clear, context-specific guidelines. Such efforts can strengthen ethical competence, reduce moral distress, and align prehospital practice with broader health-led efforts to minimize coercion.
Introduction
In prehospital emergency care, coercion refers to actions undertaken against a patient's expressed will—overcoming either verbal or physical resistance—to provide necessary treatment or ensure transport. 1 Such situations present ethical and emotional challenges for ambulance clinicians, who may need to apply coercive measures in response to patients with impaired decision-making capacity, often due to intoxication or mental health issues. 2
Ambulance clinicians is used as a generic label for skilled and qualified clinical healthcare workers employed by ambulance services, like paramedics and qualified emergency medical technicians.
Definitions of coercion
Coercion can manifest in various forms primarily categorized into physical and psychological methods. Physical coercion includes techniques such as holding, lifting or restraining patients while psychological coercion, also termedpragmatic coercion employes verbal pressure, persuasion, or threats of invoking external authority. 1 Since chemical restraints are not permitted outside hospitals in Norway, they fall outside the scope of this study.
Reasons for coercion
Many individuals refuse healthcare despite its necessity due to various factors, notably mental health disorders and substance-related conditions, which constitute a significant portion of such cases. 2 Alarmingly, mental health conditions affect one in six people annually, 3 demonstrating the increasing prevalence of crises requiring ambulance intervention. Studies, including one from New Zealand, show that ambulance clinicians frequently confront mental health emergencies yet often feel unprepared, 4 reflecting similar experiences in Norway.
Coercion is sanctioned under Norwegian law when vital medical care is required; the Penal Code allows the use of coercion in emergencies.5,6 However, coercive actions are not systematically documented in the prehospital context in Norway, with an exception for the Psychiatric Ambulance, which tracks the use of physical force.7,8 Psychiatric ambulances are modified vehicles staffed by paramedics and mental health professionals, responding to mental health emergencies. 9
Challenges faced by ambulance clinicians
Ambulance clinicians experience significant emotional stress related to the use of coercion. 10 This moral stress occurs when clinicians recognize the ethically appropriate course of action but feel constrained, leading to frustration and feelings of helplessness. 11 The interplay of ethical discomfort and repeated exposure to coercive situations can result in long-term emotional burdens and contribute to professional burnout, sometimes termed moral injury. 12
Despite the challenging nature of coercive interventions, emergency departments often become the default destination for unwilling patients, due to a lack of alternatives. 4 Studies from Switzerland and Germany emphasize the need for debriefing following coercive events,13,14 and a scoping review highlights frequent conflicts between clinical guidelines and personal beliefs, particularly in cases involving intoxicated or non-compliant patients.15,16 Such factors exacerbate the strain placed on ambulance clinicians, contributing to prevalent mental health concerns within the field.17,18
Paternalism and ethical dilemmas
Paternalism—acting on behalf of others without their consent—raises complex ethical questions,19,20 especially in prehospital contexts where rapid decisions are essential. The balance between patient autonomy and the duty to protect individuals from harm complicates ethical deliberations, requiring paramedics to quickly assess a patient's decision-making capacity.
While reducing coercion remains an objective in healthcare, it is still a prevalent issue.21-25 Studies show the stress experienced by ambulance personnel during coercive incidents and highlight the necessity for supportive mechanisms.16,26-28 Clinicians often encounter conflicting roles and ambiguity in their interactions with other authorities,10,29 further complicating their ability to provide optimal care.
Aim
This article explores factors that influence ambulance clinicians’ emotional responses to coercion, including the challenges they face and the justifications for its use.
The quantitative results from the same survey are published elsewhere. 30
Methods
An anonymous, voluntary, retrospective, cross-sectional online survey was conducted among all ambulance personnel in Norway from October 2021 to November 2022. The survey tool “Nettskjema” 31 was used, with questions developed by the authors based on a pilot survey.10,29 The survey had a quantitative approach, but included one free-text question, which is reported in this article.
The study followed relevant ethical guidelines, including the Declaration of Helsinki, the Norwegian National Research Ethics Committee for medical and health research (NEM) guidelines, and the Vancouver Protocol. Participation was voluntary, with informed consent obtained from all participants, including parents/legal guardians for minors. One participant was under 19 but over 16. The study was deemed outside the scope of the Norwegian Health Research Act, and the Regional Committees for Medical and Health Research Ethics Sør-Øst C granted an exemption from ethics approval (ref. no. 270172). The Privacy Ombudsman at OsloMet—Oslo Metropolitan University considered the data anonymous (ref. no. 599674), and data were stored in accordance with regulations at OsloMet.
The context
The ambulance services in Norway operate as departments within 18 out of the country's 20 hospital trusts. Both hospitals and ambulance services are publicly funded. According to Statistics Norway, as of 2023, there were 5025 individuals employed as ambulance personnel in Norway. 32 In this paper, the term “ambulance clinicians” 33 is used as a generic label for skilled and qualified clinical healthcare workers employed by ambulance services, like paramedics and qualified emergency medical technicians, medical doctors excluded.
In the Norwegian healthcare system, there are many groups of personnel who, in accordance with the law, are authorized to exercise power and coercion when deemed necessary to save lives and protect health. In mental health care, individuals may be admitted and detained against their will if they meet the criteria for involuntary psychiatric treatment, and they may also be subjected to intrusive measures such as forced medication, seclusion, and the use of coercive measures in accordance with The Mental Health Care Act. 34 Coercion is the use of force to persuade someone to do something that they are unwilling to do. 35 Coercion may involve physical force, psychological manipulation, or other forms of duress to influence a person's actions.
Recruitment strategy
An information letter about the study and a link to the survey was emailed to the managers of ambulance departments in the 18 hospital trusts. No incentives were offered for participation. Reminders were sent to encourage participation, and managers were asked to share the survey information with their employees. The survey was also advertised on relevant Facebook groups and the professional journal Ambulanseforum's website. Due to low response, one author contacted health trust managers by phone in February 2022, and they agreed to distribute the survey via email or local information platforms. The survey was also shared on the NAKOS (National competence service for prehospital emergency medicine) website. 36 There was no direct personal or professional contact between any member of the research team and the respondents at any point during the process.
The analytical process
Of the 488 respondents who reported using coercion in the last six months, 431 (88%) provided a free-text response to the question: “Can you say something about how you experience transporting patients where force had to be used to secure the patient during transport?”
From a pilot study, we already had numerous responses to the same question, and there was no doubt that the use of coercion was experienced as distressing. 10 Rather than repeating the same analysis on a new and expanded dataset, we instead chose to examine more closely the emotional experiences or reflections the respondents described beyond the account of the coercive act itself. To identify factors influencing emotional reactions to coercion, responses without emotional content, that is, statements that included only practical descriptions were excluded, leaving 376 responses that expressed emotions or described emotional reactions. The selection process is illustrated in Figure 1.
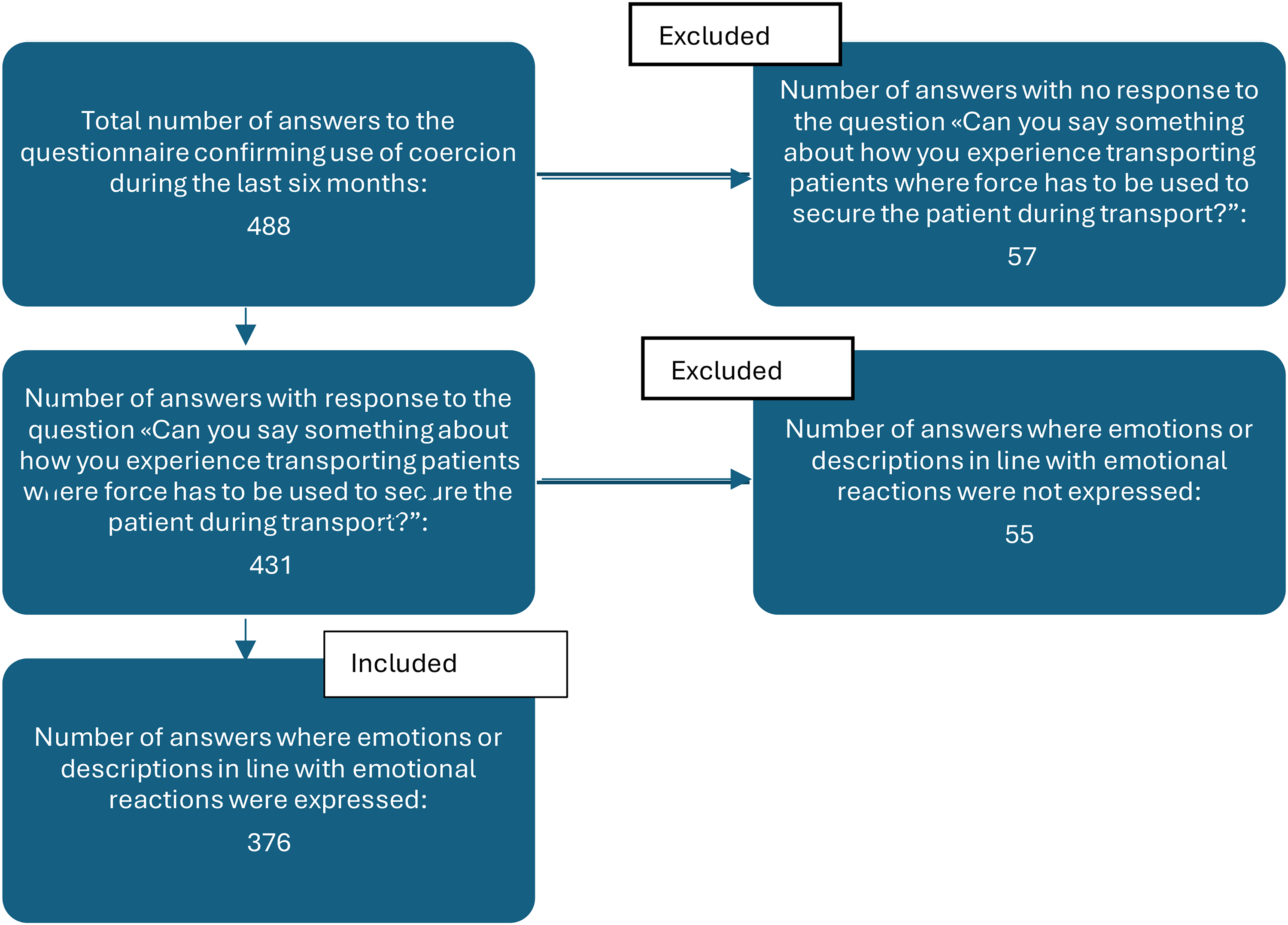
Flowchart: selection of answers.
All responses in the open text fields were analyzed using Graneheim & Lundman's qualitative content analysis method, 37 based on a phenomenological approach. Graneheim and Lundman's qualitative content analysis integrates phenomenological descriptions of manifest content with hermeneutic interpretations of latent content, highlighting its foundation in both phenomenological and hermeneutic traditions. 38 Phenomenology in content analysis focuses on understanding human experiences as they are perceived by individuals. It involves identifying patterns in how participants describe experiences, emotions, or thoughts, aiming to capture the essence of a shared experience. Researchers prioritize participants’ own words and expressions to uncover the universal core of the phenomenon, while respecting individual differences. 39 The first and second authors, with the first author having prior experience with qualitative analysis, conducted a thorough examination of both the manifest and latent content within the texts. Manifest content refers to the explicit and observable statements, while latent content involves interpreting underlying meanings through thematic analysis.
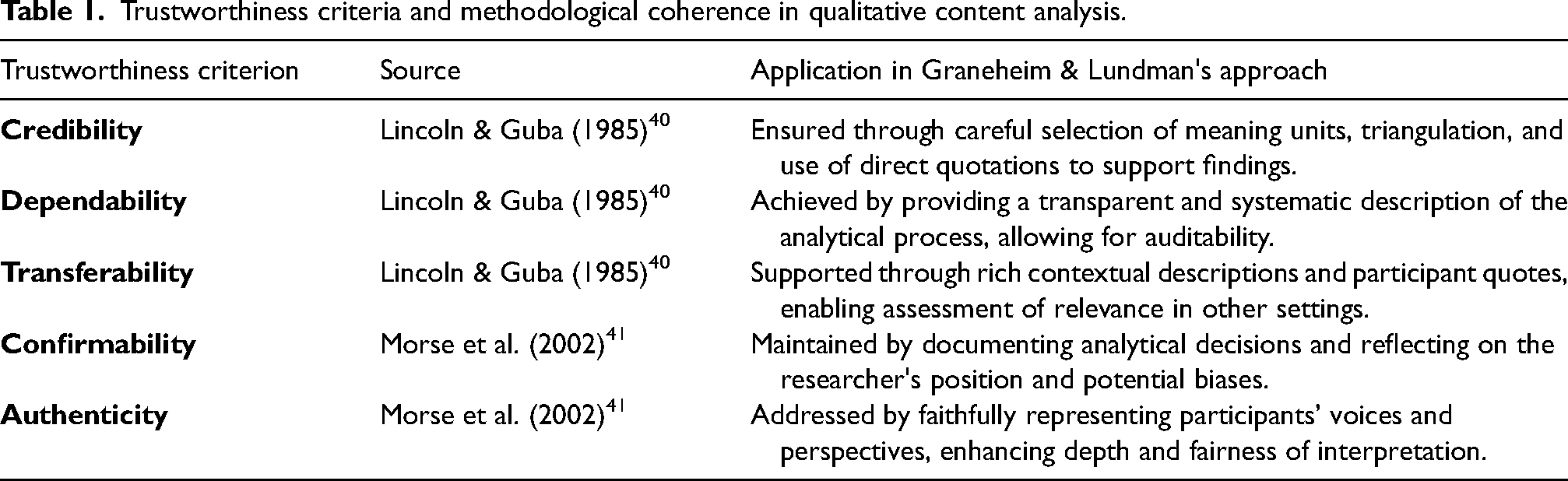
To demonstrate methodological coherence and trustworthiness, we have included Table 1 that maps key criteria from Lincoln & Guba 40 and Morse et al. 41 to the steps taken in the qualitative content analysis by Graneheim & Lundman. 37
Trustworthiness criteria and methodological coherence in qualitative content analysis.
The first and second authors reviewed each response multiple times, initially independently, and then collaboratively to ensure a thorough understanding. Any discrepancies were resolved through discussion with the other authors.
For most respondents, the use of force and coercion triggered negative emotional reactions. Words such as “abuse,” “degrading,” and “deprives patients of autonomy and violates human rights” were commonly used. These negative emotional reactions align with findings from a previous study, 10 so the analysis focused on the responses that described factors that intensified or alleviated the emotional experience.
In the analysis, we focused on understanding the subjective experiences of ambulance clinicians when they are required to use coercion, and what factors make the act distressing for them. The approach emphasizes the importance of personal perspectives and the meanings that individuals attach to these experiences. By exploring how these professionals interpret their actions, the aim is to uncover the emotional and psychological complexities involved. This approach values the contextual understanding of these experiences, allowing for a deeper understanding of the factors that influence the way force is perceived and the impact it has on those who must employ it.
An interpretive approach was well-suited for this study as it focuses on understanding the subjective experiences, meanings, and perspectives of those involved in the situation. The goal is to explore how ambulance personnel perceive and make sense of the use of coercion, allowing for a deeper insight into these individual experiences. By emphasizing contextual understanding, interpretive research aims to understand these experiences in the setting in which they occur.
The analysis was informed by a phenomenological aim to describe and interpret the lived experience of ambulance clinicians in situations involving coercion. This involved moving from codes and categories to a deeper synthesis that captured the existential meaning of their moral and professional struggles. The analysis process followed five steps: (1) Extraction: Meaningful elements were extracted from the responses, grouping words with similar meanings, (2) Condensation: These elements were condensed into a shorter text while preserving the core message, (3) Abstraction: Interpretations of the condensed elements were formulated, (4) Code formulation: Each condensed element was examined to identify the underlying essence, resulting in several codes—succinct descriptions capturing the content of similar meaningful elements and (5) Category organization: Codes were grouped into categories based on thematic relevance, leading to a structured and comprehensive analysis of the data. An example of the five steps in the content analysis is shown in Table 2.
Example of content analysis.

The analytical process moved beyond categorization of manifest content to explore the latent meanings embedded in participants’ narratives. Guided by a phenomenological orientation, the aim was to understand how ambulance clinicians experience the act of enforcing coercion—not only as a procedural obligation, but as an emotionally and ethically charged encounter. Through iterative interpretation and abstraction, a core experiential tension emerged: the conflict between their professional and regulatory obligation to control situations, and their internal sense of inadequate training, agency, and emotional support. This moral tension contributes to distress and potential psychological injury. The findings illustrate how clinicians are caught between justice-led expectations (such as collaboration with police) and their own inclination toward health-led, therapeutic care approaches. This synthesis underscores the need for service models that reconcile these conflicting demands and better support clinicians in ethically complex care situations.
Social identity theory (SIT) 42 was a suitable theoretical framework for interpreting the findings, as it offers a robust lens through which to understand how group membership influences identity, group identity, and intergroup dynamics. By applying SIT, the findings could be contextualized within broader social processes of identity formation, belonging, and exclusion, thereby enhancing the explanatory depth and theoretical coherence of the analysis.
The quotes presented in Results are illustrative examples extracted from the 376 open text answers from different ambulance clinicians and translated into English by the first author. F stands for female and M for male. The respondents were for descriptive purposes categorized into five-year age groups.
Results
Description of the sample
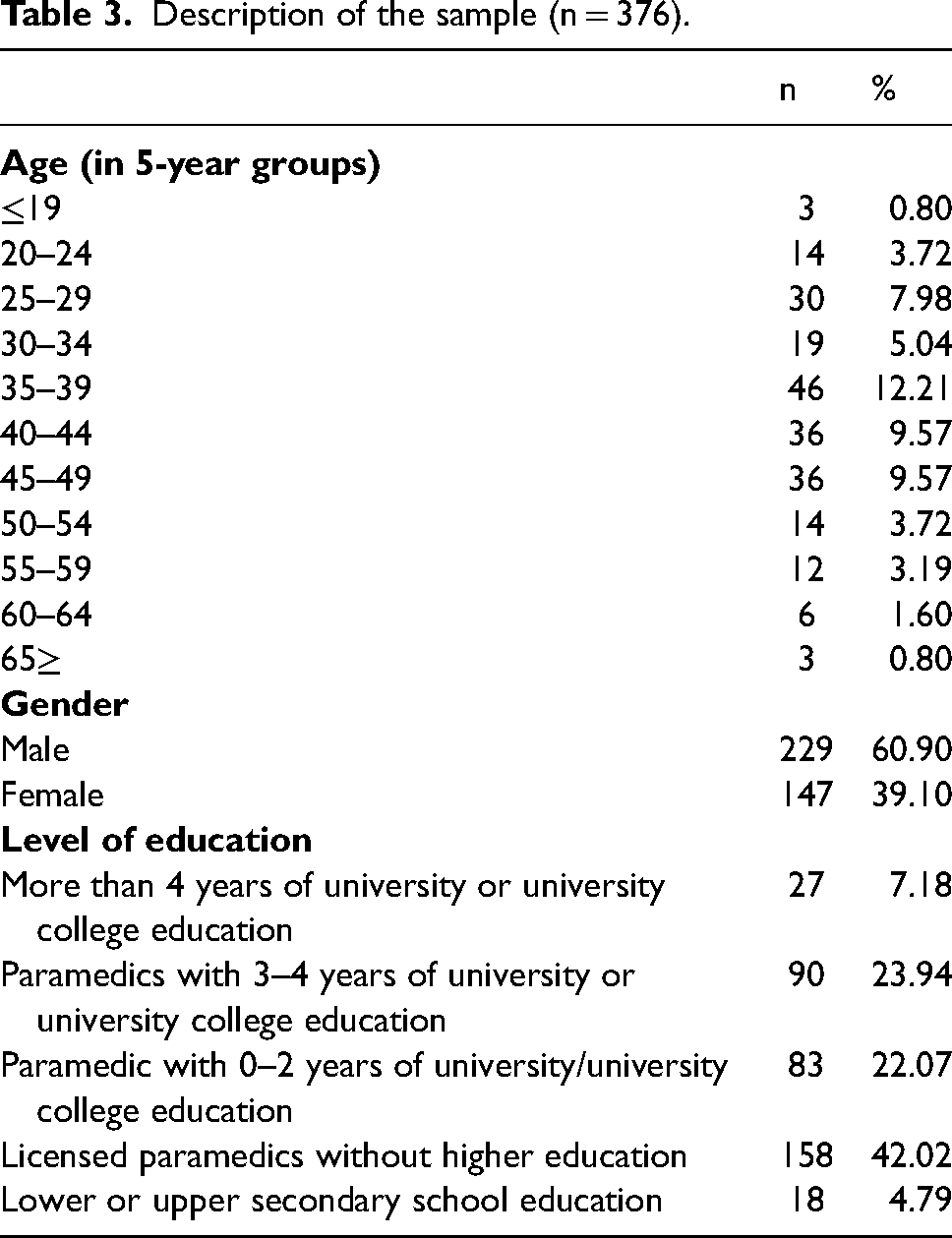
In the last 6 months prior to completing the survey, 488 (72.4%) out of the 674 (N = 681, 7 missing) ambulance clinicians stated that they had employed coercion. Among these, 349 (71.5%) respondents had used coercion one to three times, while 186 (27.6%) respondents reported no use of coercion during the last six months. The open text question was answered by 431 respondents, and 376 of the answers were included in the analysis. Some characteristics of the sample are presented in Table 3.
Description of the sample (n = 376).
Following the methodology outlined by Graneheim and Lundman, we chose three overarching themes with subthemes. The themes, that is, the varieties of factors influencing emotional reactions in ambulance personnel are shown in Table 4.
Themes and subthemes.
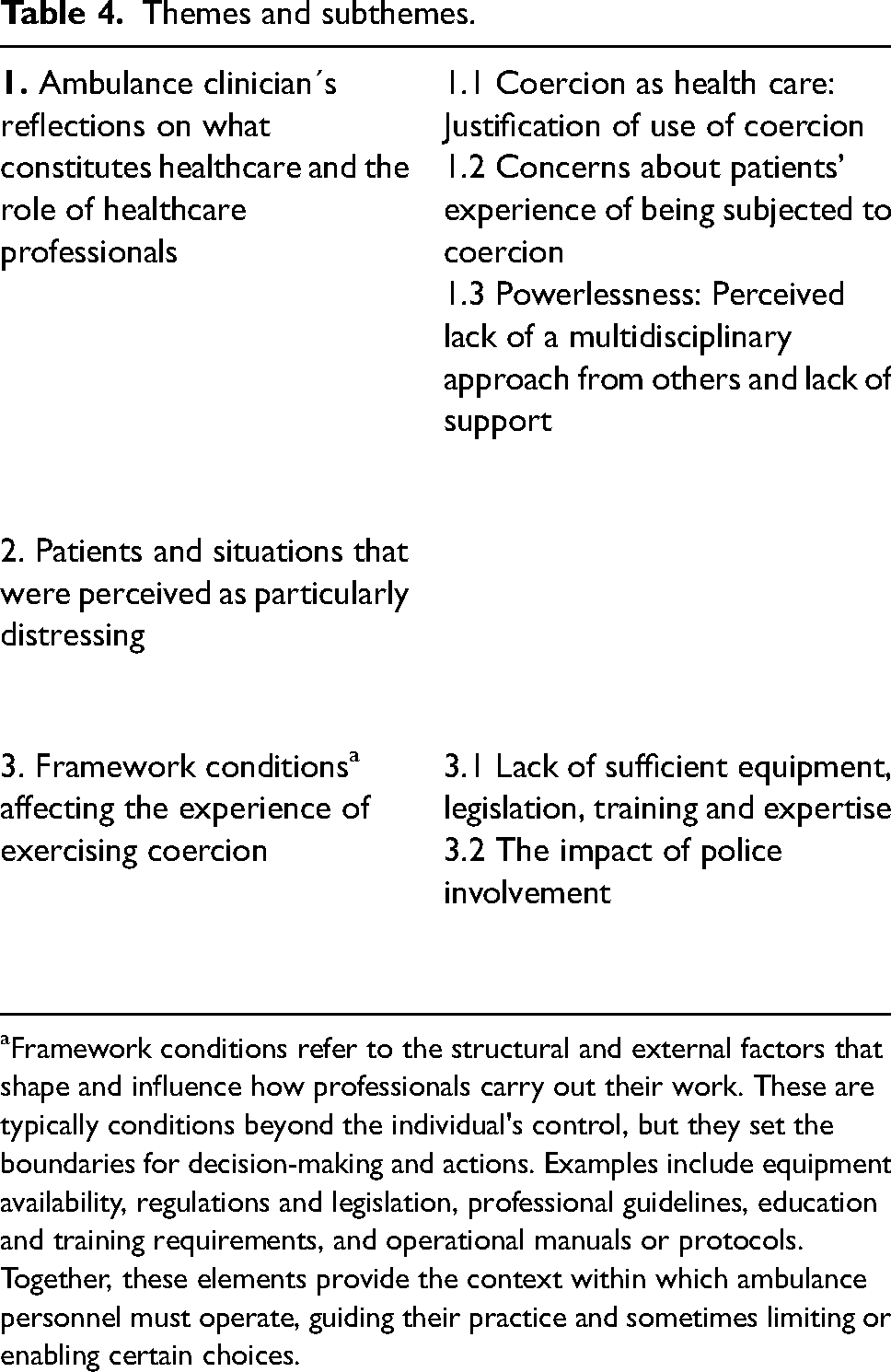
Framework conditions refer to the structural and external factors that shape and influence how professionals carry out their work. These are typically conditions beyond the individual's control, but they set the boundaries for decision-making and actions. Examples include equipment availability, regulations and legislation, professional guidelines, education and training requirements, and operational manuals or protocols. Together, these elements provide the context within which ambulance personnel must operate, guiding their practice and sometimes limiting or enabling certain choices.
Ambulance clinicians’ reflections on what constitutes healthcare and the role of healthcare professionals
The first main theme described how the ambulance clinicians described their role as health personnel and the healthcare professional-patient relationship in situations where coercion was exercised.
Coercion as healthcare: justification of use of coercion
The responses from the ambulance clinicians gave the impression that the prevailing opinion among them was that coercion is necessary in some cases. The justifications were that coercion is necessary to provide healthcare and that the use of coercion was in the patient's best interest in the bigger picture, like in the quote from F35–39: “If one can justify the use of coercion in the ambulance with medical treatment or necessary monitoring, it is perceived as acceptable” and “It [exercising coercion] can be mentally exhausting in the moment, but I feel that after the task is completed, it is in the patient's best interest,” by M35–39. Yet another example is by F25–29: “It [exercising coercion] ensures that the patient receives adequate healthcare.”
Others mentioned that coercion is incompatible with good healthcare and is not something ambulance clinicians should practice, like expressed by F25–29: “An ambulance shouldn't be associated with coercion” or by M55–59: “Not my job.”
The ambulance clinicians were concerned with their own safety. Use of coercion to ensure their own safety was a justification for the use of force, like expressed by F50–54:
“It's uncomfortable, but for my own safety, this must be done, and we aim for the gentlest transport possible” and by M40–44: “Unpleasant, but necessary for one's own safety.”
Concerns about patients’ experience of being subjected to coercion
In the responses, participants’ reflections regarding the patient's perspective were sometimes highlighted. The ambulance personnel reflected on the patient's past experiences and vulnerability and expressed concern about the additional burden being subjected to coercion could impose on them, exemplified by the quote from F35–39: “Many patients have had or currently have traumas that we are not aware of” and from M40–44: “Uncomfortable [with submitting patients to coercion] because it feels like we're infringing on the patient's autonomy.”
Concerns were also raised about how the trust in the healthcare system might be undermined among patients who are subjected to coercion, as exemplified in the quotes from M50–54:
“How much of the experience does the patient carry forward in life? What effect does it have on them regarding potential future re-contact, or lack thereof, as they may have lost trust in being heard, seen, or respected” and F20–24: “I feel that we, as healthcare personnel, [we]do not act professionally [when using coercion], and that the patient loses trust in us.”
Powerlessness: perceived lack of a multidisciplinary approach from others and lack of support
Ambulance clinicians expressed their frustration with other staff in several ways. They felt that they were left to handle assignments because mental health services were not doing their job. An example of such a feeling is described in the quote from M45–49: “As of today, we have no good tools. The psychologists ‘hide’ in their offices and believe this is our job.”
They experienced that no one cared about the difficult situations ambulance clinicians faced as is described in the quote from F30–34: “…there is often little understanding from other healthcare personnel about what it entails to have uncooperative patients in the car over long transport distances.”
And they felt they had little or no autonomy in their collaboration with the emergency medical communication center (AMK), as described by M45–49: “I am feeling conflicted about AMK (Emergency Medical Communication Center) – they want assignments to proceed, but some assignments shouldn't.”
The concern about lack of support from the management also emerged in the responses. Examples are found in the quotes from M30–34: “We are accused of this and that and suddenly find ourselves with an explanation problem as to why we have chosen to use force” and M30–34: “Support is limited if things go wrong.”
Patients and situations perceived as particularly distressing
The experience of exercising coercion was influenced by who the ambulance clinician perceived the patient to be, considering their age, diagnoses, and behavior. This theme stood out clearly from the other main themes and was therefore considered deserving of its own heading. However, due to the way the question was formulated and the nature of the responses it generated, it was not deemed appropriate to further divide it into sub-themes. Subjecting children and adolescents to coercion was described as very challenging by all the respondents mentioning subjecting minors to coercion. An example is the one from M25–29, who states: “When children are involved, it [exercising coercion] becomes highly problematic” and another one from M60–64: “It [exercising coercion] is almost cruel when it comes to teenagers who have acted out in desperation.”
Dealing with patients suffering from confusion, dementia, and mental disorders evoked similar feelings, like stated by F35–39: “Never pleasant, unwillingness [to cooperate] is mostly due to dementia or psychological issues.”
However, when encountering people under the influence of drugs, responses were divided as some described it was easier to use coercion on individuals under the influence of drugs like described by F30–34: “It is easier to use coercion on unruly intoxicated individuals than on patients with severe mental disorders or on mentally healthy patients requiring medical involuntary admissions,” while others described exercising coercion on people under the influence of substances as emotionally taxing as on people with mental disorders.
If the patient was physically aggressive or made sexual advances, it was reported as a factor that made the use of coercion less difficult. Examples illustrating this subtheme are F35–39: “…but also recognizing that it [exercising coercion] was necessary due to significant, disruptive agitation in the patient” and “Often, I/we have had to use varying degrees of force/restraint due to inappropriate sexual advances from male patients during transport,” by F30–34.
Encountering aggression was described as challenging, both when the patient was aggressive before the coercion, illustrated in the response by M45–49: “It depends on how aggressive the patient is. If they are very aggressive, it is unpleasant” and when the coercion triggered the aggression, as the quote from F20–24 is an example of: “Transports where coercion is necessary are challenging. Patients often become angry, and the situation can be somewhat uncomfortable.”
Framework conditions affecting the experience of using coercion
The third main theme we decided on during the analysis was encompassing all the factors outside the actual relationship between the patient and the ambulance clinician. The ambulance clinician’s lack of equipment, practical and legal competence, as well as the experience of not being recognized by managers or healthcare professionals in other agencies, were highlighted as factors contributing to increased emotional stress in situations involving the use of coercion.
Lack of sufficient equipment, legislation, training and expertise
Both the practical aspects of enforcing coercion, such as equipment and training, and the uncertainty related to legislation and their own competence were highlighted as factors that made exercising coercion more challenging as illustrated in the examples by M40–44: “We wish there were more adequate means available to secure the patient instead of having to improvise with bandages, tape, etc.,” M40–44: “That I have very few resources in my ‘toolbox’ to handle such tasks. That I have little knowledge about the use of coercion,” F30–34: “I feel that my competence in this area is too low” and M55–59: “Unclear and messy legislation, with ambiguous room for interpretation.” The response from M25–29 sums it up: “I find it difficult to have responsibility for the patient while also having to manage a physically aggressive patient, as I believe the laws, equipment, and training are not adequate.”
The impact of police involvement
Assistance from the police was described as positive among most of the participants mentioning cooperation with the police, and something that provided a great sense of security, although both critical comments about excessive use of force, and the low availability were mentioned, as illustrated by the quotes from M25–29:
“Good to have the police involved in such incidents” and from F40–44: If the coercion is carried out by the police, I feel it is as comfortable as it can be to execute coercion.”
On the other hand, F25–29 wrote “Difficult as the police are often far away or unable to participate due to a lack of resources” and M40–44: “The police use more physical force than necessary.”
Discussion
Previous research indicates that ambulance clinicians experience significant emotional strain when exercising coercion. 10 Our study highlights several key factors that affect the emotional impact on these practitioners. Although our findings stem from a single free-text response within a larger quantitative survey, the substantial number of respondents adds weight to the results.
The experiences of clinicians are complex and multifaceted. To fully understand the experiences, it is crucial to consider the three interconnected levels at which ambulance clinicians operate: individually, within the ambulance service, and within the broader healthcare and societal frameworks. We employed SIT to explore the tensions and alignments between personal values, professional obligations, and societal mandates influencing how ambulance clinicians navigate coercive interventions.
According to SIT, developed by Tajfel and Turner, 42 individuals derive identity and self-worth from both personal attributes and social group memberships. These dynamic identities shape attitudes and behaviors. This framework enables a deeper understanding of how personal and professional values intersect when ambulance clinicians face coercive situations.
Level 1: the individual ambulance clinician
While ambulance clinicians often view coercion necessary to provide healthcare, it remains a source of emotional burden. 10 They justify coercion as a paternalistic ethical principle aimed at acting for the greater good.19,20 However, these interventions lead to moral dilemmas and an inherent fear of making wrong decisions. 20 Even when coercion is deemed necessary, it can cause significant moral distress, 43 as our respondents noted. Actions consistent with standard practice still provoke internal conflict and a sense of disrespect for patient autonomy. This emotional dissonance may manifest as guilt or frustration, risking burnout and decreased job satisfaction among clinicians. 44
SIT explains that when ambulance personnel act against their own ethical norms, it creates ruptures in their social identity. This misalignment can erode their commitment to the profession 45 and hinder the development of a coherent professional identity. 46 Studies from Sweden, the UK, and Canada33,47-49 suggest that fostering ethical competence and promoting discussions can alleviate stress for ambulance personnel, enhancing patient safety and care quality. 48 The most effective strategies for reducing moral distress may involve structured ethical reflection, providing support to address intense emotions and integrating fractured belief systems.16,50-52 Group-based reflection with colleagues can reinforce social identity by fostering consensus around core professional values.48,49 Such reflections serve as stress-buffering mechanisms, transforming moral distress into shared insight and professional cohesion.53,54
Level 2: the ambulance service
The organizational context within the ambulance service significantly influences emotional burdens. Our study identified lack of adequate resources, ambiguous clinical guidelines, and limited managerial support as key factors amplifying the challenges faced by clinicians. Concerns for personal and colleague safety further complicate their roles. The two-person crew model, essential for distributing responsibility decision-making, is critical in these contexts.
Respondents expressed distress when coercive actions were necessary, especially with individuals experiencing confusion or mental disorders, echoing previous findings.10,33 Some believed their training inadequately equipped them to handle mental health crises, leading to increased psychological distress and burnout. 55
SIT posits that the norms and perceived status of ambulance personnel shape their professional identity. When clinicians must use coercion in the absence of adequate support or training, their core values may feel undermined, creating identity threats. 56 Moreover, a lack of proper equipment and leadership support weakens team trust and collective efficacy54,55 crucial for a positive social identity. Research indicates that repeated value conflicts without structural support may lead to disengagement from professional identity and diminished job satisfaction.16,57,58
On the other hand, enhanced training in mental health care can bolster professional identity and buffer against moral distress.56,59-62 Embedding ethical standards into organizational culture can reinforce professional integrity.63-65 Predictable leadership and interprofessional collaboration are vital in promoting collective efficacy, enabling clinicians to align their actions with established ethical standards.
Ambulance services have evolved to treat a wider range of medical conditions, including mental health crises. However, specialized mental health support is often lacking, with psychiatric ambulances limited to specific urban areas.66-69 This absence signifies a systemic deficiency, especially in Norway, where ambulance personnel frequently respond first in such emergencies. The introduction of psychiatric ambulances is a pressing issue in Norway, where they have shown promise in improving mental health crisis management.8,66,69 Nevertheless, their limited availability reflects a disconnect between international best practices and the realities faced by ambulance staff. Discussions surrounding these services in a geographically expansive country like Norway must consider practical implementation alternatives.
From an SIT perspective, this gap can create identity threats for ambulance clinicians, particularly when navigating ethically complex situations without adequate support. Establishing psychiatric ambulances should not only be a patient-centered initiative but also an effort to enhance clinicians’ sense of belonging and ethical agency.
Level 3: the healthcare system and societal context
Professionals derive identity and self-worth from the broader systems in which they operate.53,54 When ambulance personnel feel marginalized by the healthcare system, it can lead to feelings of abandonment and an overwhelming sense of responsibility. Our findings corroborate previous studies showing that disrespect from other healthcare providers is common among ambulance staff, mirroring our respondents’ experiences. 16
Ambulance clinicians often feel unsupported by the mental health system, particularly after-hours when psychiatric professionals are unavailable. This structural arrangement places the burden of handling complex situations—and the associated coercive decisions—entirely on ambulance staff.
Limited access to medical records and expert input further complicates their decision-making, positioning ambulance services as logistics providers rather than integrated partners in mental health care. This systemic shortfall underlines the importance of establishing regulated care standards, analogous to those in Australia or the UK, to improve collaboration across the healthcare system.64,65,70
SIT helps clarify the implications of disconnects between ambulance clinicians and the mental health system. When practitioners perceive their role as disrespected within the system, it leads to moral distress and professional burnout. Societal narratives framing coercion as a moral failure exacerbate identity conflicts, complicating their ability to provide necessary care in crisis situations. Without robust institutional backing, the burden of invoking coercion becomes increasingly isolating for clinicians.
Addressing these systemic issues requires redefining roles and responsibilities within the healthcare framework. A more integrated structure, one that includes ambulance clinicians in clinical and ethical decision-making, could improve coherence between their identity and practice. By reinforcing shared values and norms within a supportive environment, the healthcare system can help reduce the burdens associated with coercive interventions.
Considering recent reforms promoting health-led responses,64,65,70 ambulance clinicians are increasingly recognized as key players in patient care, empowered to act with moral clarity and professional integrity. This inclusion fosters intergroup trust vital for effective crisis intervention. Thus, structural integration serves not only logistical purposes but is essential for enhancing social identity among prehospital professionals.
The involvement of police during mental health crises emerged as a significant and ambiguous theme.69,71 While their presence is sometimes seen as necessary for safety, it can also lead to stigmatization and trauma for patients.69,71 This duality highlights the tensions inherent in crisis responses, where collaboration with law enforcement can create dissonance for ambulance clinicians.
SIT elucidates these dynamics; involvement of the police may challenge ambulance personnel's self-concept, particularly when their role shifts from health care providers to enforcers. Clarity in role expectations and adequate support is crucial for enabling effective health-led interventions.
As the international discourse on ambulance roles evolves, Norway currently lacks clear policies regarding coercion in mental health situations. Ambiguities within existing regulations contribute to widespread coercion, necessitating clear guidelines and acknowledgment of ambulance staff as integral ethical actors.
In conclusion, systemic reform must address both resource allocation and the social construction of clinical roles within healthcare. Collaborative crisis planning and decision-making structures that include ambulance personnel can help mitigate moral distress while promoting their professional identities. Current disparities must be addressed through recognition, support, and inclusion, affirming ambulance clinicians as essential contributors to person-centered mental health care.
Strengths and limitations
Our study involved 376 respondents, providing a broad range of perspectives. The analysis focused on short, concise answers, which helped minimize irrelevant information and ensured consistency. However, the use of short responses may have limited the depth of insight, as it lacked the opportunity for follow-up questions or elaboration, potentially leading to incomplete understanding or misinterpretation of respondents’ true intentions.
This research aligns with “Small q” qualitative research, which uses a less interpretative approach and focuses on predefined hypotheses and categories for replicability. Unlike “Big Q” qualitative research, which values context, “Small q” research employs methods like content analysis, allowing for systematic scoring and structured comparisons, reflecting our aim for reliable and replicable results within a qualitative framework. 72
The research team, consisting of a member with ambulance experience, a psychiatrist, and two without experience in ambulance work or coercion, brought a diverse range of perspectives. The insider provided practical understanding and credibility, the psychiatrist contributed expertise on coercion and ethical considerations, while the outsiders offered an objective perspective that challenged preconceived notions. This combination allowed for a comprehensive and nuanced analysis. However, challenges arose, such as potential bias from the insider, limited contextual understanding from the outsiders, and occasional disagreements in interpretations. Success depended on ensuring thorough reflection and transparency throughout the process.
Conclusion
The findings from our study highlight that ambulance clinicians often resort to coercion when they perceive it as necessary for patient care, despite viewing it as degrading. The experience of using coercive measures is exacerbated by feelings of incompetence, inadequate resources, legal ambiguities, and a lack of support from the broader healthcare system. Clinicians frequently feel burdened by responsibilities that challenge their professional identity and efficacy, leading to feelings of isolation and doubt.
To effectively address coercion in ambulance services, a multi-layered approach is essential. This involves enhancing individual ethical competence, establishing systematic support, and fostering coordination within the healthcare framework. Implementing structured ethical discussions, ongoing training, and setting clear legal guidelines can bolster professional identity and mitigate emotional strain. While further research is undoubtedly needed, efforts to implement ethical reflection and decision-making tools should commence immediately, capitalizing on the existing evidence that underscores their benefits. Ultimately, integrating ambulance services more effectively within the healthcare system is crucial to minimize coercion while promoting patient autonomy. Future research should align with education, training, and policy development to support these objectives.
Footnotes
Acknowledgements
ChatGPT has been used for the translation of words and sentences, as well as for improving sentence structure in English.
Author contribution(s)
Data availability
Data cannot be shared publicly because of the risk of recognition of participants in qualitative data. Data are available from the OsloMet Privacy Ombudsman (contact via personvernombud@oslomet.no) for researchers who meet the criteria for access to confidential data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to publish
All procedures were carried out in line with relevant guidelines and regulations, including the Declaration of Helsinki, the guidelines by the Norwegian National Research Ethics Committee for medical and health research (NEM), and the Vancouver Protocol. Participation in this study was entirely voluntary, with written informed consent obtained from all participants, who remained anonymous throughout. The study was determined to fall outside the jurisdiction of the Norwegian Health Research Act. Accordingly, the Regional Committees for Medical and Health Research Ethics sør-øst C granted an exemption from the need for ethics approval (ref. no. 270172). The Privacy Ombudsman classified the data as anonymous (ref. no. 599674), and the data were stored following current regulations and OsloMet University's local procedures.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.