
Abstract
Mixed methods research, a methodology that integrates both qualitative and quantitative data in order to gain a more comprehensive understanding through drawing upon the strengths of each method, is increasingly used in the pre-hospital context. Despite its growing prevalence, little is known about how mixed methods research is conducted and reported in this unique setting. This methodological review builds on our prior systematic review and examines mixed methods studies in the pre-hospital context, mapping and describing how mixed methods research is conducted and reported. We searched MEDLINE, CINAHL Complete, Embase and Scopus bibliographic databases from 1 January 2012 to 3 June 2025, using an updated pre-hospital search strategy. Study screening was undertaken in duplicate. Articles reported in English, explicitly stating the use of ‘mixed methods’ in the pre-hospital ambulance setting were included, Data related to underpinning philosophical or theoretical framework, rationale for utilising mixed methods, background of the corresponding author, mode of data integration, model of publication and adherence to reporting standards, utilising the good reporting of a mixed methods study (GRAMMS) guidelines, was extracted and analysed. A range of pre-hospital mixed methods research was identified (n = 110). Reporting standards varied, with some studies demonstrating strong integration of qualitative and quantitative data, while others lacked clarity in methodological rationale. Diversity in subject and design reflects the need for flexibility in dynamic pre-hospital environments. This methodological review highlights opportunities for improvement in mixed methods research in pre-hospital care. While the approach supports comprehensive inquiry, it is largely not underpinned by philosophical frameworks which may support methodological rigour. In many cases, mixed methods research in the pre-hospital context is used for practical reasons, and the influence of the pre-hospital setting is observed in adaptable methodologies and a diverse range of subject matter. Our findings offer new insights and guidance for future research design and reporting in this field.
Introduction
Pre-hospital care is provided to patients by emergency medical services before arrival at a hospital. 1 Determination of need is made by trained personnel who receive the emergency call and dispatch resources such as ground and air ambulances and pre-hospital responders to the scene. Sick or injured patients are treated on scene and transported to definitive care at appropriate receiving healthcare facilities. 2 With rapid evolution in recent years, pre-hospital care plays a pivotal role in improving patient outcomes, 3 and is increasingly underpinned by clinical research that provides an evidence base for pre-hospital interventions such as 12-lead electrocardiography, rapid sequence induction, mechanical ventilation and finger thoracostomy. 4 As a result, the focus has been on clinical topics such as resuscitation, airway management and pharmacology 5 with strong representation of observational research approaches. The volume of pre-hospital research itself has seen accelerated growth, with rapid development of pre-hospital research agendas6–9 reflecting the desire for coordination and optimisation of pre-hospital research, even as the field continues to evolve and mature.
Our previous systematic review 10 noted the relatively recent utilisation of mixed methods in pre-hospital research, finding a range of approaches to its application. Our research found that few authors discussed the design and approach to pre-hospital mixed methods research, and studies covered diverse topics and answered often complex questions, contributing to the growing body of pre-hospital research. However, we also identified the need to exercise caution with pre-hospital mixed methods designs, highlighting that consideration should be given to ensuring that the methods are appropriate for addressing the research problem and that true mixing, or integration, of the data occurs.11,12
Given the significant growth in the utilisation of pre-hospital mixed methods research in recent years, this updated methodological review aimed to map and describe how mixed methods research is currently conducted and reported, including characteristics such as author background and use of theoretical frameworks. It also assesses adherence to reporting standards by describing the characteristics and adherence to relevant reporting guidelines and provides an outline of the utilisation of mixed methods research in paramedicine.
Methods
Study design
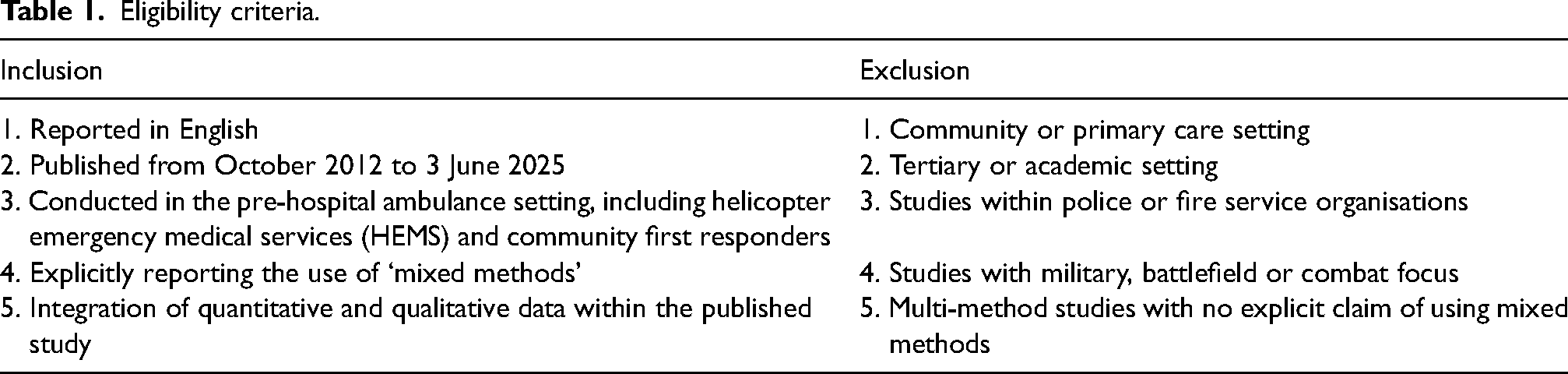
We used a systematic approach to conducting this methodological review, developing and publishing a protocol 13 to direct process and serve as a point of reference to each component. The design of this review was informed by Aguinis et al. 14 and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 15 The advice provided by Garner et al. (2016) with regard to when and how systematic reviews should be updated informed our decision making. All studies with a pre-hospital focus and in which a mixed methods research design was applied were sought. The eligibility criteria are shown in Table 1.
Eligibility criteria.
This review was not registered on the international prospective register of systematic reviews (PROSPERO), as it does not involve an outcome of clear relevance to the health of humans, and is instead a methodological review that assesses the quality of reporting. This review received no financial or nonfinancial support, and there were no funders or sponsors involved in the design, conduct, analysis or reporting of this review.
Search strategy
The search strategy (Table 2), developed in collaboration with an academic librarian (MO) was developed for Medline and translated to CINAHL Complete via EBSCOhost, Embase via Ovid and Scopus. For our initial search, databases were searched from October 2012 (the last period searched in our previous systematic review) to 15 March 2023, with a search update performed to 3 June 2025. We utilised an optimised search strategy 16 and added two new 2023 Medical Subject Heading (MeSH) terms previously unavailable (‘Paramedics’ and ‘Paramedicine’).
Search terms.
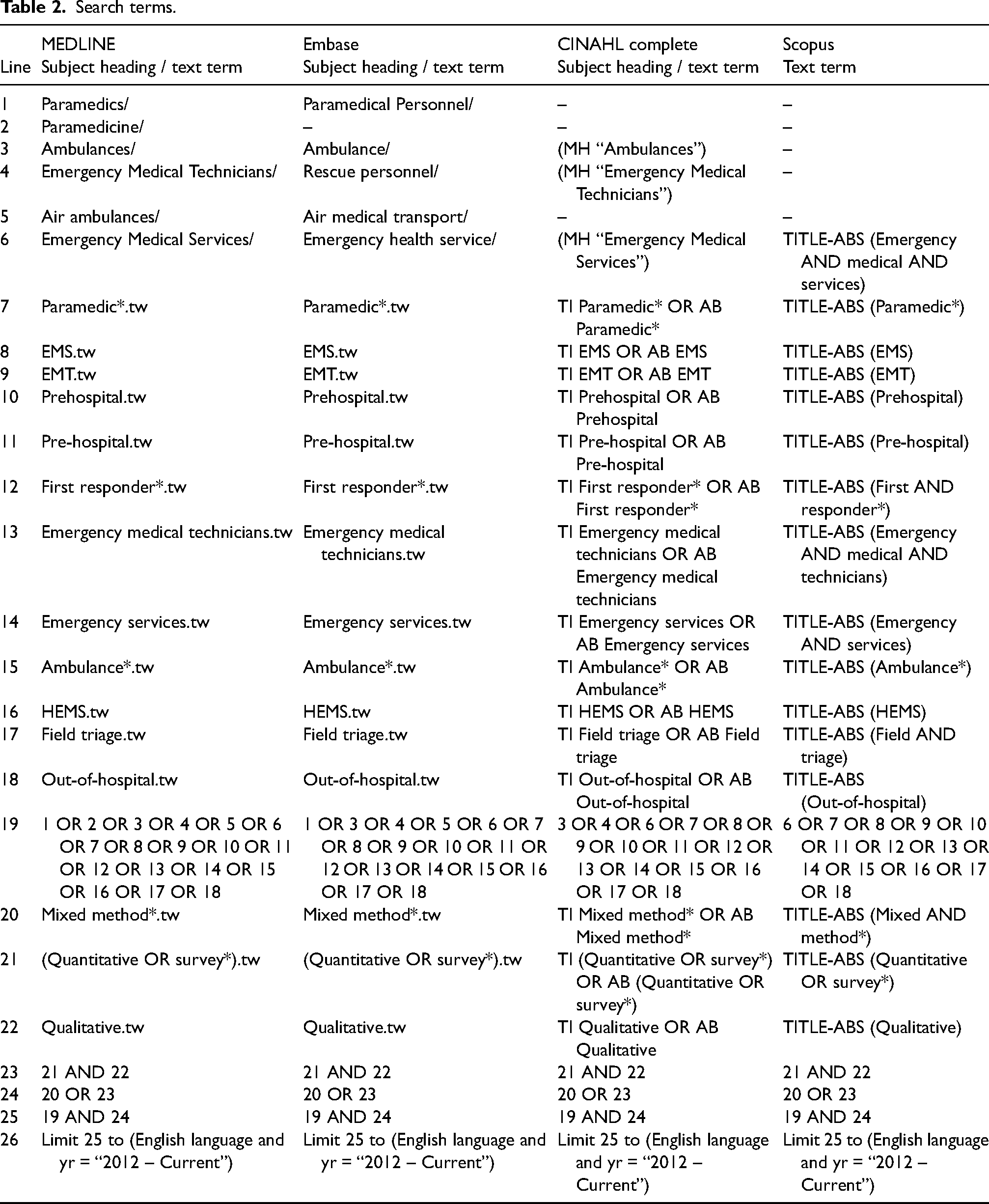
In addition to the database search, key journals were hand searched to identify relevant studies, including paramedic journals not indexed in large databases. Google Scholar was searched using key search terms and the top 200 results were screened.
Study selection
Titles and abstracts were screened in duplicate by two or more authors using the systematic review management software Covidence (Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia). The full texts of potentially eligible studies were retrieved and assessed for eligibility by two or more authors. Presence of integration (Table 1) was assessed using author judgement rather than relying solely on explicit reporting of integration. Integration may have been achieved at the design, methods and/or reporting and interpretation level. 17 Virtual study selection meetings were held, with inclusion decisions being made as a team. Reasons for study exclusion were recorded and any differences of opinion between authors were resolved through group discussion with three or more authors. There were three disagreements across all studies retrieved, resulting in minor adjustments only.
In addition to the Good Reporting of A Mixed Methods Study (GRAMMS) criteria ascertaining adherence to reporting standards, studies were evaluated for key elements with the intent of highlighting disparity or areas of interest within the pre-hospital mixed methods literature. These included the background of the corresponding author, the declaration of an underpinning philosophy or theoretical framework (studies were allocated ‘yes’ or ‘no’ if there was clear inclusion or absence of such an underpinning, and ‘somewhat’ if a framework was vaguely included), and the model of publication (single study or multi-study).
Data extraction
Data regarding study characteristics, including the background of the corresponding author, declaration of an underpinning philosophy or theoretical framework, model of publication and adherence to reporting guidelines were extracted. Authors of studies were contacted to request missing information where required, and the Google internet search engine was utilised to source author background information if unable to be determined within the published work.
Reporting quality
While recognising the clear distinction between methodological quality and reporting quality in mixed methods research studies, we focused here on assessing the reporting quality of the included studies. Reporting quality refers to how well the study’s methods, results and interpretations are communicated or reported, and therefore we assessed adherence to the GRAMMS reporting guidelines 18 tool to ascertain whether individual studies followed the reporting criteria for mixed methods research. Cross-checking of study alignment with GRAMMS criteria was performed by two authors independently for n = 56 (50.9%) of the retrieved studies, with only two minor adjustments made.
Data synthesis
Findings are presented in tabular form, with key words ‘yes’, ‘no’, ‘somewhat’ and ‘inadequate information’ indicating the level of alignment with GRAMMS reporting guidelines. 18 Key findings are reported narratively.
Differences between protocol and review
There is one major difference between our previously published protocol and this review. Initially, we set out to produce a contemporary version of our 2015 systematic review 10 however during our research realised that our focus was on methodological process, rather than the specific outcomes of the studies under review. The goal became therefore not to produce any meta-findings, or synthesise evidence to answer a specific research question, but to describe how mixed methods research is conducted and reported in the pre-hospital setting. While we used a systematic approach to accomplish this, our research design was adjusted to that of a methodological review14,19 which provided an opportunity to understand current practices, and to identify potential gaps in methodological or reporting quality. 19
There were in addition some minor differences between our previously published protocol and this review. We had not accounted for studies that discuss decision making of patients prior to pre-hospital care, including decision making around when to make an emergency call. As these studies involve a timeframe before the scope under examination in this methodological review, they were not included. In addition, research undertaken in a quasi-academic setting (e.g. university-initiated drone simulation studies) was assumed to relate largely to academic investiture and was not included.
Results
Of the initial 3821 articles screened, 185 were selected for full text review, with 83 studies meeting eligibility criteria. Following the update to 3 June 2025, an additional 422 articles were screened, with 36 selected for full text review, adding 27 studies to those meeting eligibility criteria. The results of the search and study inclusion process are presented in Figure 1.
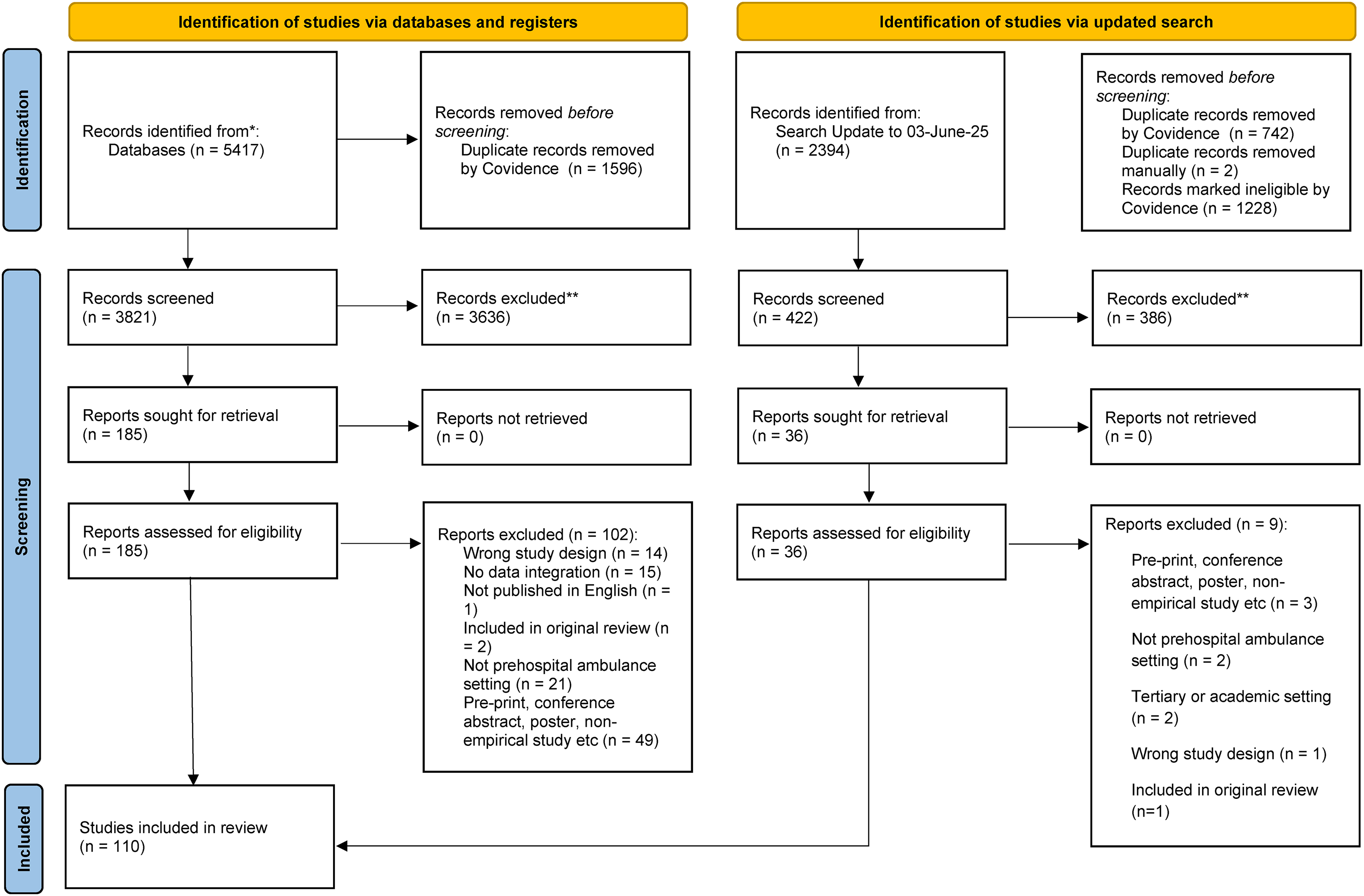
PRISMA diagram.
A summary of included studies can be seen in Supplemental Appendix 1.
Background of the corresponding author
Serving as the correspondent between the research team and the publishing journal, the corresponding author brings research to the public eye. Where publicly available, we reviewed the gender, geographical location and professional background of the corresponding author of all publications, to ascertain who is driving pre-hospital research.
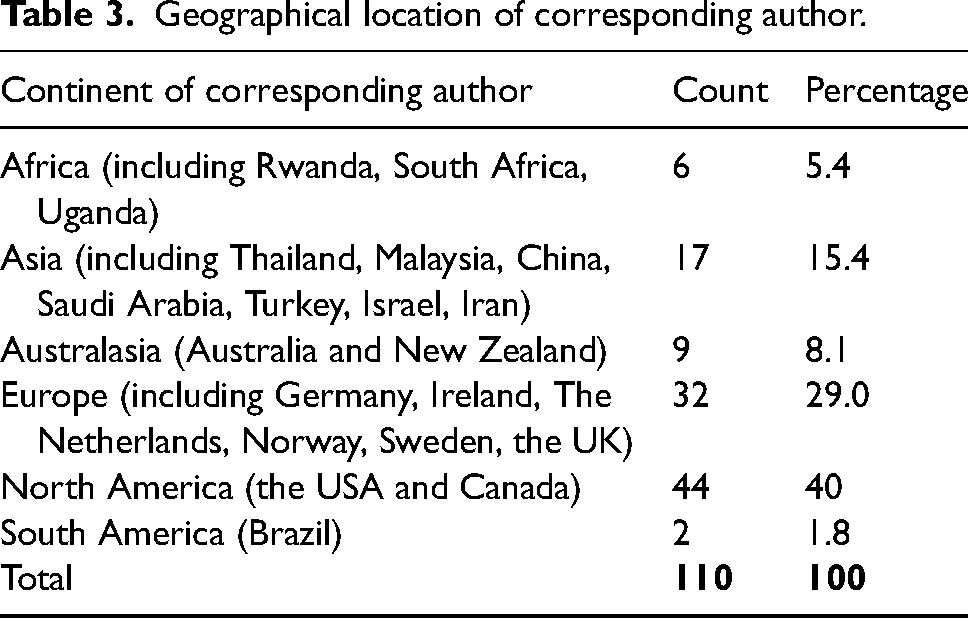
Of the eligible studies, 37.2% (n = 41) of corresponding authors were female, 60% (n = 66) were male, and in 3 studies the apparent gender of the corresponding author remained unknown. The majority of mixed methods research with a pre-hospital focus was from authors in North America (44%, n = 40) followed by Europe (32%, n = 29) (see Table 3).
Geographical location of corresponding author.
Pre-hospital research is undertaken by researchers with professional backgrounds in medicine, allied health and health services research. In addition, the growing interest and rapid increase in pre-hospital research agendas has spurred the increasing involvement of paramedics in research teams. 20 We reviewed the background, where publicly available, of the corresponding author of eligible studies (see Table 4).
Professional practice/domain of corresponding author.
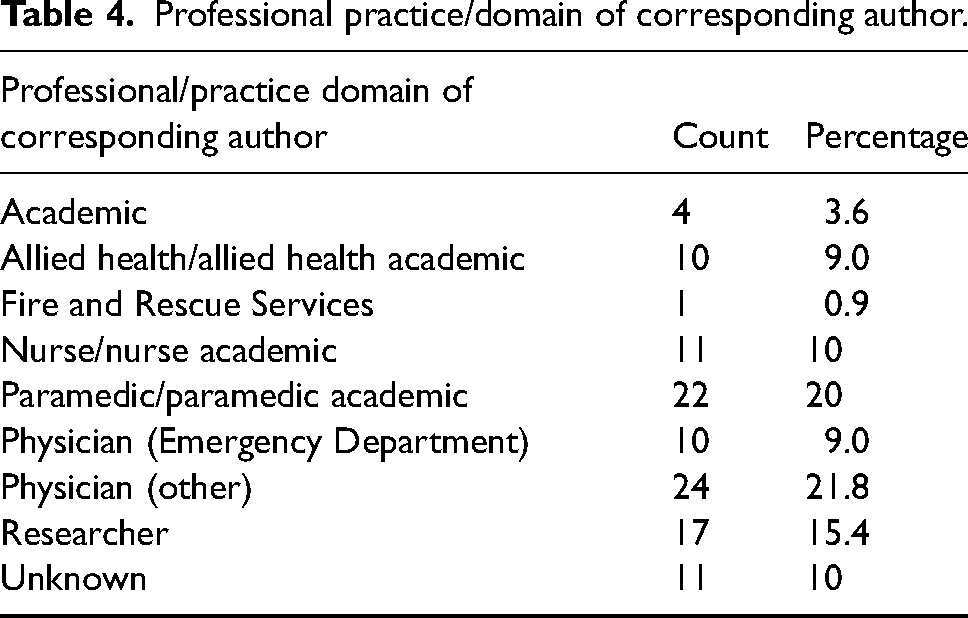
Of the 34 studies listing a physician as the corresponding author, most were physicians from the United States, several of whom were employed as the medical director of municipal or private emergency medical services (EMS). There were 10 studies authored by researchers with a professional background as an emergency department physician.
Declaration of an underpinning philosophy or theoretical framework
We reviewed all studies to determine whether they included a clearly defined philosophical or theoretical framework. Overwhelmingly, pre-hospital mixed methods research did not include a declaration of an underpinning philosophical or theoretical framework (88.1%, n = 97). Ten studies (9.0%) were underpinned by a theoretical framework. These included one design underpinned by a critical realist worldview and informed by a Naturalistic Decision Making theoretical framework, 21 use of a constructivist grounded theory approach 22 and pragmatism.23,24 Three studies (2.7%) referred to such an approach but stopped short of utilising them to assist with design or methodological decisions.
Model of publication
Of eligible research, the majority (96.3%, n = 106) were published as stand-alone studies. Four (3.6%) were published as separate items of an overall study, including one mixed methods study within a mixed method study. 25
Whilst most included papers described the mixed methods design (84.5%) and described each method in terms of its sampling, data collection and analysis (85.4%), the remaining elements of the GRAMMS criteria were mostly overlooked. Of included papers, 60% did not justify the use of mixed methods to answer the research question, while 83.6% did not describe any limitation of one method associated with the presence of the other method and 64.5% did not describe any insights gained from mixing or integrating methods (see Table 5).
Summary of GRAMMS assessment.
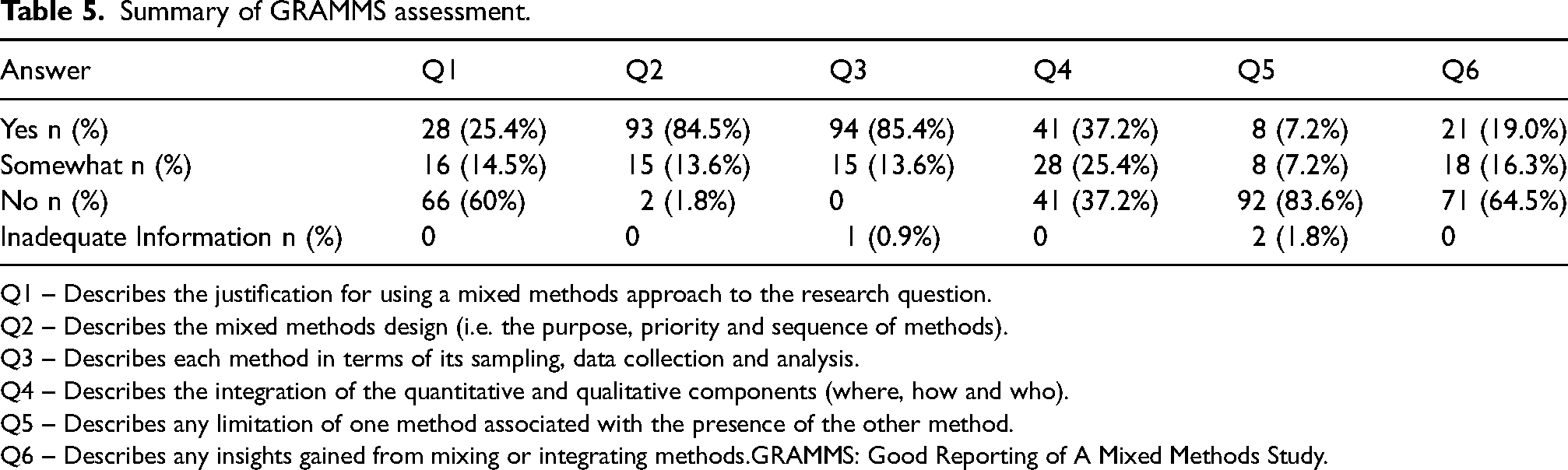
Q1 – Describes the justification for using a mixed methods approach to the research question.
Q2 – Describes the mixed methods design (i.e. the purpose, priority and sequence of methods).
Q3 – Describes each method in terms of its sampling, data collection and analysis.
Q4 – Describes the integration of the quantitative and qualitative components (where, how and who).
Q5 – Describes any limitation of one method associated with the presence of the other method.
Q6 – Describes any insights gained from mixing or integrating methods.GRAMMS: Good Reporting of A Mixed Methods Study.
GRAMMS criteria 1: Justification for using a mixed methods approach to the research question
The GRAMMS framework was used to assess the quality of retrieved studies. Only 28 studies (25.4%) clearly justified why a mixed methods approach was necessary and offered full transparency in design and design components. 18 The majority (60%, n = 66) did not specify a rationale for the use of the research methodology and 16 (14.5%) provided partial consideration for the use of mixed methods research. A summary of results is provided in Supplemental Appendix 2.
GRAMMS criteria 2: Design purpose, priority and sequence of methods
Robust mixed methods studies offer transparency of the mixed methods design 18 and are clear about the selection and construction of methodologies. All studies were read in full for an outline of design purpose, priority and sequence of methods, with the majority (n = 93, 84.5%) including a discussion of these components. This item, and GRAMMS criteria 3 (‘description of methods in terms of sampling, data collection and analysis’) were the most commonly fulfilled components of the GRAMMS framework in the studies retrieved.
GRAMMS criteria 3: Describe each method in terms of sampling, data collection and analysis
All studies included a description of sampling, data collection and analysis of individual components relating to the mixed methods design. A number of studies (n = 15, 13.6%) did not explicitly articulate the methodological steps involved with these components, or lacked information, leaving some gaps relating to feasibility and validity.
GRAMMS criteria 4: Data integration
A fundamental component of mixed methods research lies in the integration of data or findings from the different methods utilised (O’Cathain et al., 2008). It is a pivotal component of designing and conducting a mixed methods study, requiring researchers to consider at the outset why and how integration of components will occur. 26 We employed the view that mixed methods research can be integrated at the levels of method, methodology and paradigm, 27 and extended this to mixing occurring at any research stage including purpose, research question, theoretical drive, method, methodology, paradigm, data, analysis and results. 28
Whilst all included studies were deemed to have some level of data integration as per the review study selection and eligibility criteria (Table 1), not all studies described the integration of the qualitative and quantitative components for the purpose of the GRAMMS criteria. Of the included studies, only 37.2% (n = 41) described the integration of data, with 25.4% (n = 28) somewhat describing the integration of data, and the remaining studies (37.2%, n = 41) not describing any integration of quantitative and qualitative data. Largely, researchers maintained separation of qualitative and quantitative components throughout the studies, including in the reporting.
GRAMMS criteria 5 and 6: Limitations and insights
Limitations arising from the use of one method associated with the presence of the other method were reported in 7.2% of studies (n = 8). The reporting of insights gained from mixing or integrating methods was observed in 19.0% (n = 21) of studies. Ten of these had provided a justification for using a mixed methods approach to the research question, highlighting the positive implications of integration, including ‘overcoming limitations’ 29 ‘obtain[ing] a deeper understanding and description of a very complex situation using a scientific approach’ 30 and ‘enrich[ing] our understanding of risk factors and opportunities’. 31
The research topics of the studies retrieved are diverse. Pre-hospital mixed methods research reflects an expanded scope, with authors exploring pre-hospital decision making, 21 palliative care,32,33 child abuse34,35 and patient safety,36,37 topics which have previously not been explored in the pre-hospital field using mixed methods.
Discussion
This methodological review provides a contemporary update around how pre-hospital mixed methods research is undertaken and what standards of reporting are achieved. Importantly, it offers the observation that while the quantity of mixed methods studies focused on the pre-hospital environment is increasing, many studies lack methodological rigour. Design challenges are infrequently reported, particularly those relating to data integration, insights gained from mixing methods, and acknowledgement of the limitations of one method associated with the presence of another. This may limit transparency of the research process in general, reducing the potential for contribution to the ongoing development of this methodology. Conversely, it could also be indicative of the direction mixed methods research is taking in a specific community of practice, where the priority of reporting quality is perhaps secondary to the discovery and reporting of pragmatic answers to complex pre-hospital research questions.
This updated methodological review found that that the use of mixed methods in pre-hospital research has continued to grow in the years since the publication of our initial study. Our initial systematic review identified 23 studies published within a nearly 12-year period, while this updated review has identified 110 research studies published within the past 10 years. Notably, there has been significant expansion in the scope of pre-hospital research using mixed methods, 38 even when considering the international trend of increased pre-hospital research publication, which has seen an 800% growth in 20 years. 39
We analysed the backgrounds of corresponding authors in the studies retrieved for this methodological review, with some key findings. While backgrounds were varied, authors with physician training outnumbered other disciplines, particularly in studies published in the United States. In the United States, paramedics operate under the medical supervision and authority of board-certified physicians, following highly regulated protocols developed by physician medical directors. 40 Education and credentialling of EMS staff from the United States is often via certification rather than a tertiary degree. There were only two studies from the United States in which the corresponding author was a paramedic.41,42 This is in contrast to the remainder of the paramedic or academic paramedic authored studies, published in countries such as Australia, the United Kingdom and Canada. In both Australia and the United Kingdom, paramedics are regulated, with pre-registration education via a 3-year university degree and the emergency medical system has less of a physician-led focus. What is represented in the backgrounds of corresponding authors is the growing engagement of researchers in mixed methodologies across the globe and throughout practice domains.
Declaration of an underpinning philosophical or theoretical framework
With more than 90% of studies retrieved for this review eschewing the utilisation of an underpinning philosophical or theoretical framework, it is evident that reporting of theoretical and philosophical underpinning hasn’t improved since our 2015 pre-hospital mixed methods review. Creamer et al. note that there is a general absence of reflexivity about philosophical orientation during reporting of mixed method research, which presents a challenge when gauging prevalence 43 and this observation applies to our findings. Most pre-hospital mixed methods researchers appear to focus more on the selection of methods for investigations and the consequences of the research without consideration of the basic assumptions fundamental to the research approach itself. 44 Mertens 45 notes that ‘working without an awareness of our underlying philosophical assumptions does not mean that we do not have such assumptions, only that we are conducting research that rests on unexamined and unrecognised assumptions’ – a practice that may diminish the benefits that come with utilising mixed methods in the first place, and one that could affect the validity of research findings and conclusions. 46 Consideration of philosophical assumptions can motivate and justify mixed methods research in practice, rationalising the integration of qualitative and quantitative data and designs 46 and its absence may reduce transparency surrounding design decisions. The ability of mixed methods research to answer complex clinical problems in the pre-hospital setting 47 has undoubtedly contributed to the rapid proliferation of pre-hospital mixed methods research. It is possible that some pre-hospital authors choose to use mixed methods research as a pragmatic or ‘what works’ approach, perhaps perceiving it as not necessitating engagement with the methodological rigour or distinctive design features that characterise mixed methods research.48,49 Given that half the studies retrieved for this review lacked integration of the qualitative and quantitative data utilised, it is possible that confusion exists around the distinction between ‘mixed methods’ and ‘multi-methods’ researches. A lack of clarity between the terms and their individual methodological techniques could contribute to misunderstandings around the conceptualisation of mixed methods and its application in pre-hospital research. These gaps may undermine the coherence and depth of pre-hospital mixed methods research, limiting its ability to generate comprehensive insights or contribute meaningfully to theory development, and impacting research quality.
Standards of reporting
We utilised key tools to assess the quality of included studies by describing their key characteristics and adherence to reporting guidelines, using the GRAMMS framework which places emphasis on the design, purpose and sequence of methods used in mixed methods research. 50 Interestingly, all studies that used an underpinning theoretical or philosophical framework to underpin the research also included a clear outline of the mixed methods design purpose, priority and sequence of methods. This suggests that the utilisation of a theoretical or philosophical framework assists authors with the implementation of key components of mixed methods research that increases their methodological rigour and quality. The standards of reporting observed in our study indicate that while there has been a significant increase in the use of mixed methods research, it is largely in isolation to the adherence to any mixed methods guidelines or theoretical underpinnings. In the retrieved studies, the focus appears to be on the practical applications of research approaches, or ‘what works’ 51 and the consequences of the research, rather than on the methods themselves. We found that objectives of the studies retrieved for this review were generally successfully answered through the use of two or more forms of data, even if there were gaps in the reporting of integration and inconsistences in design. With some retrieved studies fulfilling only one of the GRAMMS criteria in full, it is clear that standards of reporting in pre-hospital mixed methods research are not particularly high, likely providing opportunities for improvement in overall quality. Failing to account for key methodological concepts such as data integration may reduce the full potential of mixed methods research and limit the breadth and depth of possible outcomes.
It is, however, important to note that while adherence to guidelines such as GRAMMS provides a useful benchmark for quality, prescriptive adherence is not always necessary. As seen in qualitative research, overly rigid application of guidelines can sometimes risk reducing research to a formulaic process, neglecting the broader understanding of research design. 52 In mixed methods research, flexibility in applying these guidelines can allow researchers to adapt to the practical complexities of real-world problems, ensuring that methodological rigour is achieved without stifling creativity and relevance.
Mixed methods research in paramedicine
Research associated with paramedicine (e.g. research about the paramedic profession itself) was evident amidst the studies retrieved. Of included studies, 20% listed a corresponding author with a professional background as a paramedic or a paramedic with a position in an academic institution, the majority recording the United Kingdom or Australia as their home nation. The desire for a stronger evidence base in paramedicine has helped to drive an increase in paramedic research agendas 20 with paramedics taking an active role in leading and participating in research. There is no doubt that utilisation of mixed methods research in paramedicine is shaped by the pre-hospital setting itself. Mixed methods research may help pre-hospital researchers navigate complex clinical problems requiring the insight of both generalisable quantitative methodologies, and of person-centred, contextual qualitative methodologies. The pre-hospital environment poses some inherent challenges to paramedicine research 53 which mixed methods is suited to overcome through its integration of quantitative and qualitative data, providing a deeper understanding of complex problems than either approach utilised alone. However, mixed methods research is not a panacea to the challenges facing pre-hospital research, and the methodological limitations of both quantitative and qualitative research must be considered and addressed if high quality pre-hospital research is to be forthcoming. The substantial growth of paramedicine research has led to a vast array of pre-hospital research activities largely driven by smaller localised collaborations which may lack the impact of larger partnerships that benefit from pooled skills and resources. 54 Much of the focus on research priorities and development of research agendas has focused on improved patient care and enhanced system performance, 7 with research driving changes in clinical practice in a range of areas. However, other authors have considered the shifting academic focus around research topics as evidence of a lack of strategic direction in paramedicine, 5 calling for realignment of research focus with paramedic direction-setting and ongoing development. Here, the topic shifts to the relative juniority of paramedicine amongst the health professions, with confirmation of key research needs internationally55–57 evidencing a young profession experiencing rapid growth. There are opportunities for improvement in pre-hospital research, with limited funding and research capacity, and methodological limitations 6 challenging the rigour of the evidence-base. This provides additional complexity when considering mixed methods research in paramedicine and our findings: of the 22 studies published by paramedics/paramedic academics, half described data integration, while 6.36% (n = 7) partially described data integration and four did not. If the quality of mixed methods research is inferred by adherence to design quality and rigour, then there are likely opportunities for improvement in paramedicine.
Strengths and limitations
This is the first update of a previous systematic review focusing on pre-hospital mixed methods research, providing a contemporary view of how mixed methods research is currently undertaken in this domain. The overall quality of included research studies varies widely, largely due to gaps in methodological rigour which may be partially explained by design decisions relating to the pragmatic use of mixed methods research over philosophical or epistemological viewpoints. Adhering strictly to the GRAMMS criteria provided a level of trustworthiness and rigour – to support reliability, > 50% of studies were independently verified by two authors, with only three minor changes on verification indicating a high level of confidence. Despite this robust process, some limitations remain. Our judgement of data integration during study selection was subjective. We offset this by conducting this process as a team, rather than individually. The precise level of integration of qualitative and quantitative data was challenging to define for the purpose of the GRAMMS criteria, resulting in additional time being taken with data extraction when considering whether a study displayed ‘full’ or ‘partial’ data integration. Other methodological limitations included that while some studies did not include the phrase ‘mixed methods’ in their title or abstract, some may have integrated qualitative and quantitative data in the body of the paper, but not have been retrieved by the search strategy. This review did not include studies published in languages other than English, though this is unlikely to significantly affect outcomes. Finally, despite creating and implementing a search strategy with the assistance of a specialist academic librarian, it is possible that some relevant studies were missed.
While we made efforts to capture studies that used a publishing model in which mixed methods components were reported and published separately, it is possible that our review still missed some. Stringent word count limits set by many journals 26 may lead authors to choose to publish qualitative and quantitative components of a mixed methods study in separate papers without explicitly stating that they are part of a larger mixed methods project. 49 This fragmented model of reporting can make it difficult to identify and include such studies in methodological reviews like ours. However, this approach does offer some benefits, as publishing each component separately can provide authors greater scope to explore each method in more detail, offering a deeper exploration of either the qualitative or quantitative aspects. This can enhance the richness of the findings from each part of the study, as long as integration occurs to satisfy the purpose and rigour of the mixed methods approach.
Despite these benefits, the separate publication model also has potential drawbacks. It can obscure the visibility of the mixed methods design as a whole and reduce the opportunity to clearly describe how the qualitative and quantitative data are integrated: a critical element of mixed methods research. Additionally, in some cases, one part of the study may be accepted while the other is not, 26 or authors may move on without completing the publication of all components. Stringent word counts may also be another cause of the low adherence to reporting guidelines found in our review. While we support journals allowing greater flexibility in word counts to facilitate the full and transparent reporting of mixed methods studies, ensuring that both components and their integration are adequately described, opportunity also exists for authors to be as concise as possible when constructing their manuscripts, to allow for adequate representation of the complexity of the mixed methods process and their findings within word count limits. 26
Research contribution
This methodological review provides an important methodological contribution. Not only does it provide new information about the utilisation of mixed methods research in the pre-hospital setting, but it maps eligible studies according to the GRAMMS criteria, providing novel information about the standards of reporting achieved in this area. It also suggests that pre-hospital mixed methods research in paramedicine is largely not underpinned by philosophical frameworks which may support methodological rigour, but is used for practical reasons, with design decisions being ‘practical, contextually responsive, and consequential’. 58 Philosophy does not appear to be valued as a criterion of research quality 59 with decisions around design based less on epistemological features and more on practical viewpoints and desired outcomes.
Recommendations for future mixed methods inquiry based on this review's unique contribution include the development of pre-hospital mixed methods conceptual frameworks. Such a framework should take into account the particular challenges of the pre-hospital environment and in undertaking pre-hospital research and seek to support researchers with the conduct of high-quality mixed methods research.
Conclusion
This methodological review has examined different aspects of pre-hospital mixed methods research including the presence of any underpinning philosophy or theoretical framework, the rationale for utilising mixed methods, the background of the corresponding author, mode of data integration, model of publication and adherence to reporting standards, utilising the good reporting of a mixed methods study (GRAMMS) guidelines. Pre-hospital mixed methods research continues to evolve, with a rapid increase in published studies showing diverse approaches to the application of mixed methods. The majority of studies do not wholly address key methodological criteria such as design, purpose, sequence and integration of methods, however the stated objectives of pre-hospital research are largely met. The ongoing challenge to pre-hospital researchers, therefore, is to ensure a balance is achieved between high level methodological rigour and the pragmatic development and reporting of answers to complex research questions.
Supplemental Material
sj-docx-1-pam-10.1177_27536386251366694 - Supplemental material for Pre-hospital mixed methods research: An updated methodological review
Supplemental material, sj-docx-1-pam-10.1177_27536386251366694 for Pre-hospital mixed methods research: An updated methodological review by Tegwyn McManamny, Scott Munro, Paul A. Jennings, Georgette Eaton, Marishona Ortega and Gregory Adam Whitley in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386251366694 - Supplemental material for Pre-hospital mixed methods research: An updated methodological review
Supplemental material, sj-docx-2-pam-10.1177_27536386251366694 for Pre-hospital mixed methods research: An updated methodological review by Tegwyn McManamny, Scott Munro, Paul A. Jennings, Georgette Eaton, Marishona Ortega and Gregory Adam Whitley in Paramedicine
Supplemental Material
sj-docx-3-pam-10.1177_27536386251366694 - Supplemental material for Pre-hospital mixed methods research: An updated methodological review
Supplemental material, sj-docx-3-pam-10.1177_27536386251366694 for Pre-hospital mixed methods research: An updated methodological review by Tegwyn McManamny, Scott Munro, Paul A. Jennings, Georgette Eaton, Marishona Ortega and Gregory Adam Whitley in Paramedicine
Footnotes
Author contribution(s)
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tegwyn McManamny is an associate editor at Paramedicine. Georgette Eaton is a Deputy Editor at Paramedicine. Neither played an role in the editorial process, which was conducted in adherence to Paramedicine's editorial policy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.