
Abstract
Advanced Practice Paramedics (APPs) are highly skilled paramedics who operate in diverse clinical settings both within and outside traditional ambulance services. International evidence demonstrates that APPs enhance patient outcomes in areas such as critical and primary care. In Australia, the expansion of APP roles and responsibilities has gained momentum; however, no nationally recognised framework exists to define their expected capabilities. This gap leads to inconsistencies in education, practice and role clarity. A standardised capability framework is therefore vital to guide the development, implementation and integration of APP roles within the Australian healthcare system. The primary aim of this study was to develop a comprehensive list of APP capabilities tailored to the Australian context through expert consensus. A modified Delphi approach was used across four iterative phases to establish consensus. An expert panel of clinical, academic, organisational and regulatory/governance leaders was identified via the Knowledge Resource Nomination Worksheet. Participants reviewed, rated and refined proposed APP capabilities derived from international frameworks and relevant literature. Consensus was defined as a minimum of 70% agreement among participants. Of the experts invited, 43 consented to participate in the Delphi process. A final set of 33 capabilities, achieving 96% overall consensus, was developed. These capabilities spanned four key domains: Clinical Practice (14), Leadership and Management (10), Education (7) and Research (2). Iterative feedback ensured each capability was clear, relevant and aligned with the Australian healthcare context. The resulting capability framework provides a robust foundation for standardising APP roles within Australia, promoting consistency in education, practice and professional expectations. This framework not only supports the national advancement of APPs but may also serve as a model for international adaptation, contributing to the global development and recognition of advanced practice roles in paramedicine.
Introduction
The increasing diversification of out-of-hospital care delivered by paramedics, covering the full clinical acuity spectrum, from primary care and social needs to critical care has highlighted the dependence of public health systems on paramedics adopting advanced practice roles.1–3 Globally, the evolution from standard paramedic roles towards advanced practice has led to the emergence of various roles often described as specialised or extended practice positions.4,5 Examples of these extended practice roles include intensive and critical care paramedics, 6 community or extended care paramedics 7 and paramedic practitioners.8,9 These roles leverage existing paramedic strengths to focus on addressing more specific and complex healthcare challenges, ranging from providing care to the most acutely unwell, to focusing on reducing unnecessary transportation to emergency departments by addressing healthcare needs within community settings. In the Australian context, existing titles such as extended care paramedic and intensive or critical care paramedic typically denote role-specific competencies within clearly defined clinical scopes, rather than indicating broader, higher-level clinical autonomy. In this paper, we introduce the umbrella term Advanced Practice Paramedic (APP) to distinguish paramedics practising autonomously at an advanced clinical level, irrespective of clinical focus area, from these existing extended-scope roles. Here, we suggest autonomy refers to the capacity to independently initiate, manage and evaluate care episodes within an agreed scope of practice and clinical governance framework, without the requirement for direct oversight. Adopting the term APP specifically avoids the legally protected title ‘specialist’, as defined under Australia's National Law, 10 and clearly differentiates broader advanced practice roles from more narrowly scoped extended roles previously described. Our approach to defining APP in this broad way aligns closely with international approaches to advanced practice, such as the UK's Advanced Clinical Practitioner role, 11 and mirrors other Australian advanced practice roles, such as Nurse Practitioners, where a single advanced practice definition and title encompass practitioners across multiple specialty areas. 12
While it's important to recognise some paramedics in existing extended roles may already be practising at a level approaching advanced practice, formal recognition of advanced practice as a distinct level of autonomous paramedic practice has yet to be clearly established in Australia. Internationally, APP like roles have diversified to adapt to changing community needs and have been integrated into both traditional ambulance service models of care as well as broader healthcare system roles worldwide.9,13–18 Alongside the development of advanced practice roles, a robust capability framework is essential to guide the education, regulation and practice of paramedics stepping into these roles.19,20 A capability framework is a structured outline of capabilities that define the essential responsibilities, behaviours and attributes required for individuals within a specific profession or role.21,22 It serves as a comprehensive roadmap outlining the knowledge, skills, behaviours and qualities necessary to practice.20,23,24 In identifying capabilities it's important to delineate the difference between capabilities, competencies and skills – terms that are frequently applied with different meanings. For the purposes of this study, capabilities are defined to encompass responsibilities, attributes, behaviours and knowledge. In contrast, competencies are more focused, detailing the specific knowledge and abilities necessary to perform or execute a particular skill or task.25–27 Finally, skills are defined as the precise, individual actions or techniques required within a competency. A well-defined capability framework lays a foundation for developing competencies and guides education, training and professional development initiatives.20,24 This ensures that individuals possess the diverse skills needed to succeed in their given roles across varying contexts. 20
The absence of a dedicated capability framework for APPs in Australia represents a critical gap, not only in standardising expectations for advanced practice within the profession but also in safeguarding public safety. Without a structured framework, there is limited guidance on essential capabilities, leading to potential inconsistencies in education, practice and understanding of APP roles. This lack of clarity can result in disharmony within the profession and confusion among stakeholders.20,28 To address this issue, it is critical to develop a broadly accepted and harmonised capability framework that aligns APP roles with their current responsibilities and expectations. Using a Delphi methodology is an ideal approach, as it seeks expert consensus to identify and prioritise the key capabilities required for APP roles. Establishing a national capability framework will promote consistency in role expectations, education and regulatory standards, supporting the delivery of high-quality, consistent care.15,29 Therefore, this study aimed to achieve consensus on the essential capabilities that can underpin the development of a national APP capability framework in Australia.
Methods
Delphi methodology overview
This study utilised a modified Delphi methodology to reach a consensus on the capabilities that are deemed most appropriate in the creation of an APP capability framework tailored to the Australian context. 30 To facilitate this, experts were identified and recruited through a systematic process, based on their knowledge and expertise surrounding APP. Participants were invited to partake in a four-phase online Delphi process. Consistent with a modified Delphi design, Phase 1 began with a literature-derived list of candidate capabilities (instead of an open item-generation step as seen in traditional Delphi designs) 31 and the study concluded with a final binary accept/reject vote after three Likert rounds, rather than continuing Likert scoring until statistical stability. A modified Delphi technique was also selected because it (i) enables structured, anonymous feedback from geographically dispersed experts; (ii) allows iteration with controlled feedback so that panellists can reconsider their views without the pressures of face-to-face group dynamics; and (iii) is well-established for developing professional capability frameworks where empirical evidence is limited and expert judgement must be aggregated systematically.32,33 Alternative consensus methods such as nominal group technique were considered but rejected because they either require in-person meetings or lack the iterative refinement necessary for refining complex capability statements. The methods and results are reported using the standard for Conducting and REporting of DElphi Studies (CREDES). 32
Research paradigm
Although the Delphi process is often described as a method of inquiry, all research is underpinned by a broader theoretical framework or research paradigm. In this study, the Delphi process was anchored in an interpretivist ontology and guided by the paradigm of realism. Realism holds that a single external reality exists, yet individual interpretations of that reality can vary based on each person's experiences and context. 34 Where realism diverges from purely interpretivist approaches is in its acknowledgment that, through iterative and systematic inquiry, researchers can progressively approximate an understanding of this singular reality by accumulating experiential evidence and perspectives. 35 Within the Delphi context, realism is manifested in the integration of diverse expert opinions and experiences, converging towards an agreed central understanding of essential APP capabilities.
Identification of participants
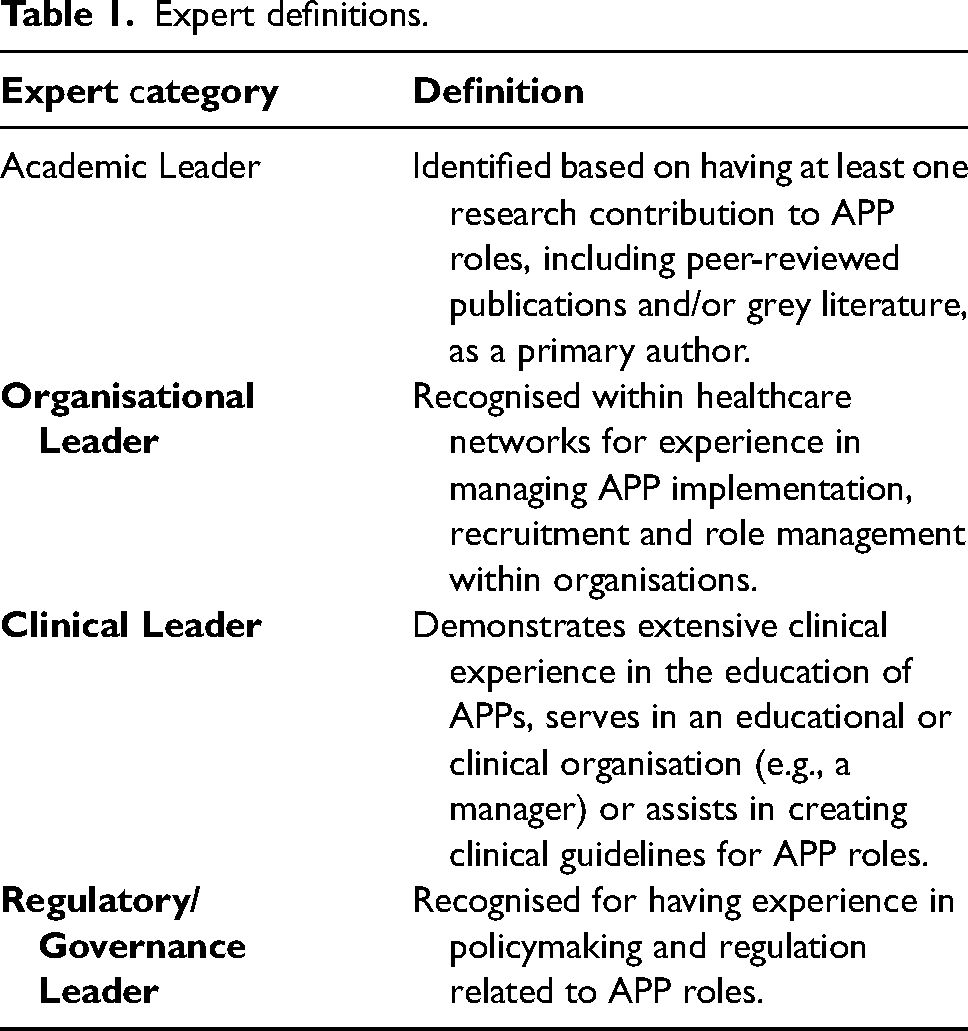
Delphi studies fundamentally rely on the rigorous identification and selection of expert participants. To structure this process, the research team followed Delbecq et al.'s guidance, 36 aiming to ensure a comprehensive overview of APP. Experts were recruited from four domains deemed critical to APP: (1) Clinical Leaders, (2) Governance/Regulatory Leaders, (3) Organisational Leaders and (4) Academic Leaders. Each domain had specific inclusion criteria (Table 1). In cases where individuals met multiple sets of criteria, they were assigned according to their preferred domain. To systematically recruit experts with varied perspectives, the Knowledge Resource Nomination Worksheet (KRNW), a structured tool frequently used in Delphi studies, was employed. 33 The research team began by compiling an initial participant list through their professional networks, categorising potential contributors under the most appropriate domain. Once these networks were fully utilised, further participants were identified by searching authors in the APP literature 37 to locate additional Academic Leaders, and second, by reviewing the publicly available membership of the Paramedicine Board of Australia, the National Board that, in partnership with the Australian Health Practitioner Regulation Agency, sets professional standards and makes registration decisions for paramedics in Australia, to identify individuals with governance or regulatory leadership expertise. After populating the KRNW, potential experts were invited to join the Delphi study via an electronic survey link. At that point, a snowball recruitment strategy was implemented: invited participants were asked to nominate other individuals who they believed met the expert definitions, thereby expanding the overall pool of potential contributors.
Expert definitions.
Delphi questionnaire
The Delphi questionnaire was conducted online via the use of Qualtrics software. Each phase survey and accompanying instructions were pilot tested by three members of the research team (AR, LM and BS); feedback on clarity, completeness and potential wording bias was incorporated before distribution. The four-phase Delphi process is described in Figure 1.
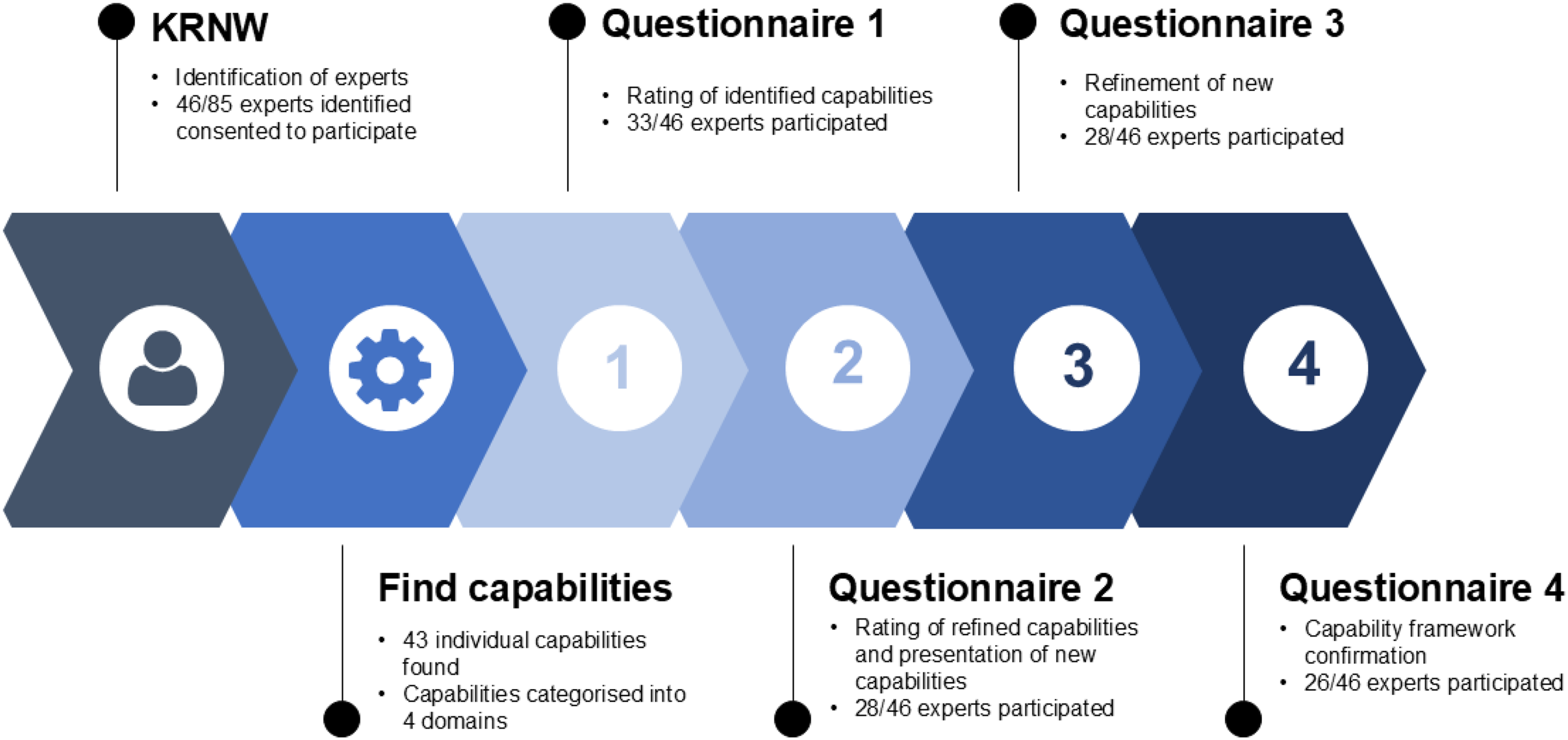
Overview of Delphi process.
Phase 1 – Rating of initial capabilities
To establish a national consensus on the capabilities that should underpin an Australian APP capability framework, we first provided participants with a consolidated list of all existing APP capabilities. These capabilities were identified via a scoping review of the APP literature. 37 Capabilities were grouped across four different known domains that were identified in the literature being (1) Clinical Practice, (2) Leadership and Management, (3) Education and (4) Research. At this stage participants were asked to rate each capability on a Likert-type agreement scale (1 = ‘inappropriate’, 5 = ‘extremely appropriate’), to indicate its suitability for inclusion in an Australian APP capability framework. Capabilities with a total of 80% or greater of participants scoring each capability a 4 (somewhat appropriate) or 5 (extremely appropriate) were then considered to be suitable for inclusion in a final presentation of APP capabilities. Participants were also invited to input any amendments or suggestions surrounding each capability which could inform possible revisions via free text. Additionally, in the free-text response area participants could leave suggestions for new capabilities that they believed were integral to APP though not already presented.
Phase 2 – Rating of refined capabilities and presentation of new capabilities
Following the initial rating, any capability that attracted substantive free-text feedback about clarity or conceptual overlap was revised or, where appropriate, merged with a related item and re-presented. Participants were shown both the original and the revised versions of these capabilities and asked to rate the revised versions using the same 5-point Likert scale and 80% threshold employed in Phase 1. Additionally, new capabilities proposed via Phase 1 free-text feedback were introduced for the first time. These new capabilities were also evaluated using the same Likert scale and scoring mechanism as in Phase 1.
Phase 3 – Refinement of new capabilities
In Phase 3, capabilities that were further revised based on Phase 2 feedback were presented again. Participants continued to use the same 5-point Likert scale and the 80% threshold for evaluating these updated capabilities, with both the original and newly revised versions displayed for clarity. Free-text responses remained available for participants to offer further feedback or recommendations.
Phase 4 – Acceptance or rejection of capability framework
In the final phase, participants were presented with a compilation of capabilities that had been accepted during Phases 1–3. These were organised according to their respective domains for clarity. Participants were then asked whether they accepted or rejected the capabilities within each domain in a binary accept or reject approach. An optional free-text response box was provided to allow participants to explain or clarify their choices if desired.
Consensus and convergence of opinion
To achieve consensus on the requisite capabilities for APPs in Australia, this study was designed with a minimum of four Delphi rounds. In the iterative rating rounds (Phases 1–3) each capability was scored on a 5-point Likert scale; items endorsed by ≥80% of panellists at the ‘4–5’ level were carried forward. An 80% threshold was used for Likert-based refinement rounds to ensure that only strongly supported items proceeded to the final vote.
38
The confirmatory round (Phase 4) then employed a binary accept/reject vote with a 70% consensus threshold, consistent with Delphi recommendations for dichotomous closure rounds.
39
In Phase 4, if agreement on capabilities were below 70% the survey would be recirculated, providing participants with their previous responses, the overall mean scores and relevant qualitative feedback to facilitate reconsideration and refinement. To streamline the process and reduce fatigue, two stopping criteria were established as outlined by Okoli and Pawlowski:
33
Halting after reaching 70% consensus. Ending iteration if successive rounds showed no statistically significant changes in mean rankings, assessed by McNemar's test.
This structured approach allowed for a balanced convergence of participants insights while respecting participant time, ultimately solidifying a consensus-driven framework for APP capabilities.
Analysis
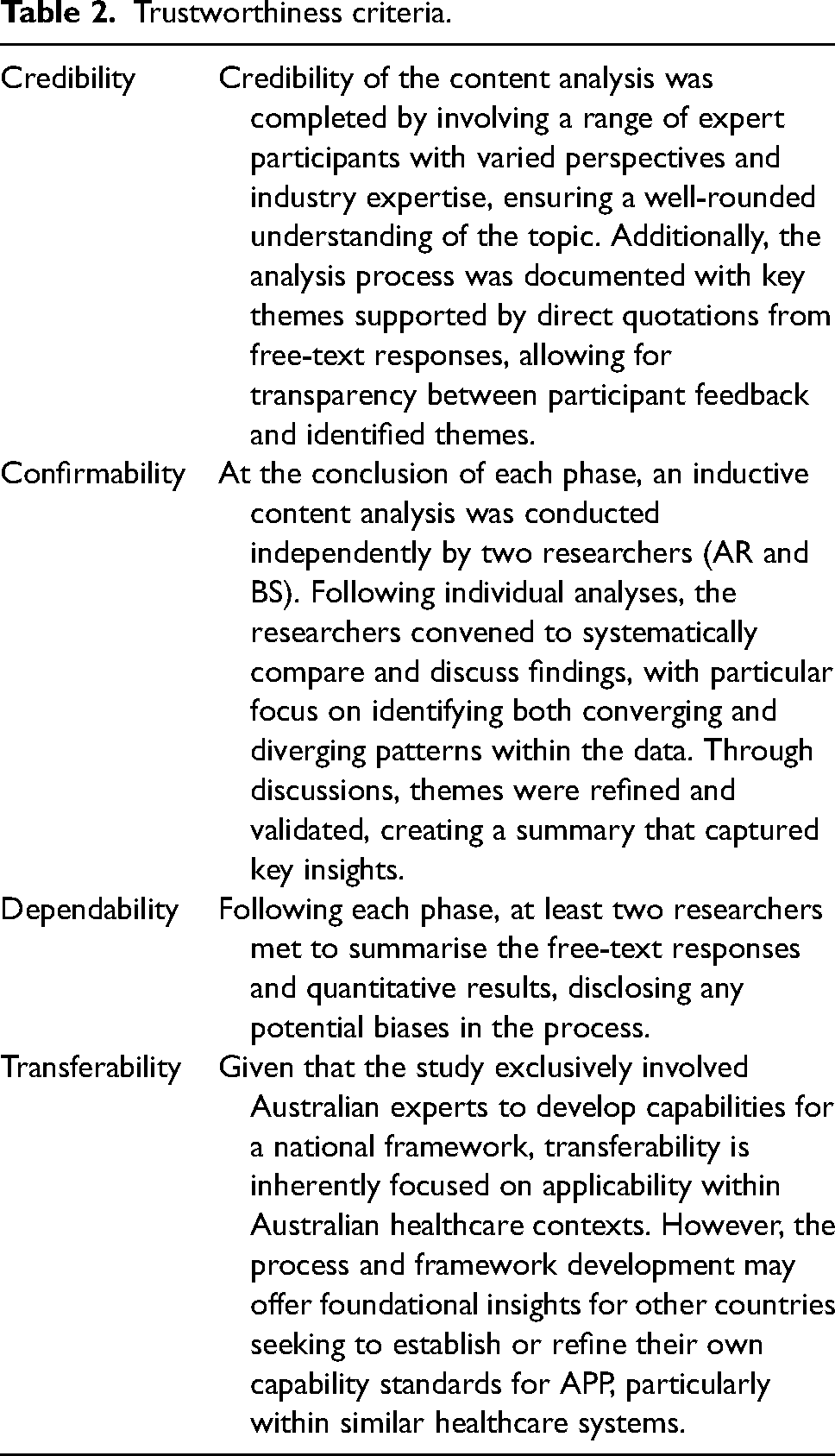
Descriptive statistics were used for quantitative variables and the research team analysed free-text responses via a descriptive content analysis at each phase and created themes to summarise participant qualitative data.40,41 Researchers AR and BS reviewed each free-text response critically and proposed revisions to individual capabilities based on participant responses which were then presented to the entire research team for further analysis and review. Table 2 outlines the application of Graneheim and Ludman's trustworthiness criteria in the content analysis approach drawn from Lincoln and Guba's work.40,42
Trustworthiness criteria.
Ethics
This research received ethics approval through Monash University, Human Research Ethics Committee, project ID 43558.
Results
Phase 0 – Populating the KRNW
Included participants
A total of 85 participants were identified as experts and invited to participate. The author team populated 71 expert names and invited them to Phase 0 of the Delphi. Through the snowballing technique, an additional 14 participants who met the established criteria were invited to participate by being nominated by other participants. Of the 85 participants invited to participate, 46 consented to involvement. Participants identified their area of expertise based on the provided expert criteria descriptions. Eleven identified as academic experts, 7 as organisational experts, 20 as clinical experts and 8 as regulatory/governance experts giving a representative sample across all four targeted areas. Participation rate at each phase of the Delphi by expert category can be found in Supplementary Table 1.
Phase 1 – Rating of initial capabilities
Phase 1 questionnaire was sent to 46 participants with a response rate of 71.7% (n = 33). Through searching relevant literature 43 individual capabilities were identified, presented and scored (see Table 3 for results organised by domain). Of the 43 capabilities presented, 30 (70%) were accepted in Phase 1 having received greater than or equal to 80% of participants scoring the capability a score of 4 or 5.
Phase 1 results.
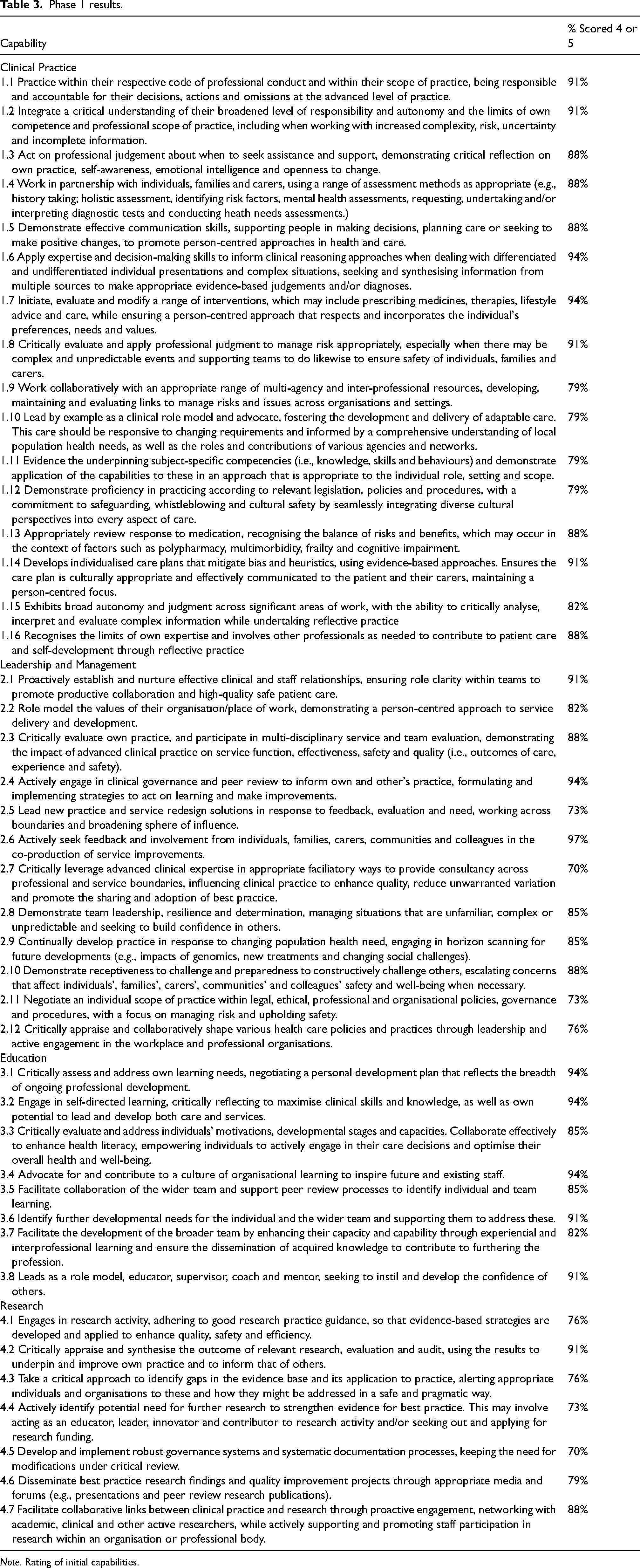
Note. Rating of initial capabilities.
Content analysis of free-text responses – Phase 1
The content analysis of free-text responses in Phase 1 generated three themes: (1) the need for improved clarity in the phrasing of capabilities, (2) the limited emphasis on research as a core component of APP and (3) clarifying the scope of practice, competence and autonomy.
Clarity in phrasing
Participants frequently expressed concerns about the phrasing of the existing capabilities, with several comments indicating that the language was overly complex. “This is a word salad. More clarity required” “A little wordy and repetitive in places, again I suggest they need robust editing for clarity.”
Comments such as these highlighted the need for more concise and direct language. These comments suggest the simplification and clearer expression of the capabilities would enhance understanding and translatability.
The role of research in APP
A second theme generated from expert feedback regarded the role of research within APP capabilities. While research was acknowledged as important, several participants noted that it should not be a core requirement for advanced practitioners. Some caution in assuming that an advanced practitioner will also be interested and able to undertake their own research. Acting as a researcher shouldn’t be a requirement for an advanced practitioner, however, the abilities to appraise and synthesise the research is important.
Overall, the research domain received less engagement in the free-text responses compared to the other three domains. There were few suggestions for improvement or explanations regarding why these research capabilities were considered inappropriate.
Scope, competence and autonomy
A further theme of the feedback emphasised the need to clarify the scope of practice for advanced paramedics, ensuring it is distinct from other paramedic roles. The feedback highlighted that the current capability statements were not sufficiently clear in defining the competence required at the advanced practice level. Competence is not just a function of knowledge, but the ability to apply it in diverse situations.
Additionally, participants emphasised that advanced practice should be defined by autonomy in decision-making, based on competence. Autonomy comes with the responsibility to know when to seek guidance, maintaining accountability at all time.
Phase 2 – Rating of refined capabilities and presentation of new capabilities
Phase 2 had a response rate of 61% (n = 28) of participants respond to the rating of revised and new capabilities generated from Phase 1. Table 4 presents Phase 2 results that show that 16 of 17 capabilities were accepted. See Supplementary Table 1 for the revised capabilities along with a comparison of the original and updated versions.
Phase 2 results.
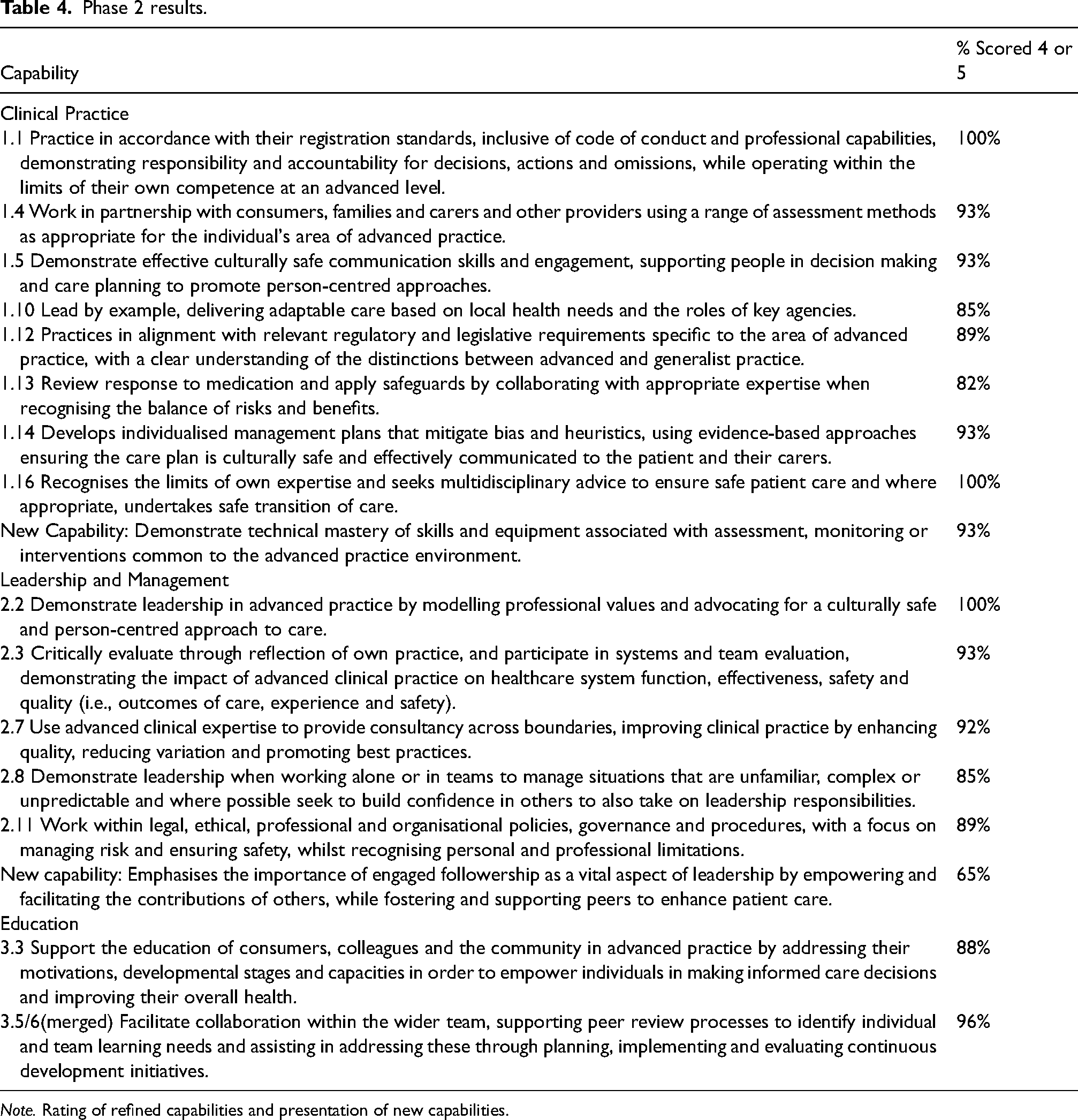
Note. Rating of refined capabilities and presentation of new capabilities.
Content analysis of free-text responses – Phase 2
The free-text responses from Phase 2 highlighted key areas for refining the capability statements for APP. Three themes were generated to summarise the feedback: (1) the distinction between advanced practice and standard roles, (2) the relevance of certain capabilities and (3) the importance of cultural sensitivity and patient-centred care.
Scope of advanced practice vs standard practice
A significant amount of feedback suggested that many of the capability statements appeared more applicable to standard practice (expressed in capability statements as generalist practice) rather than advanced practice. This overlap raised questions about whether certain capabilities should be categorised as advanced practice or whether they were more appropriate for healthcare practitioners at all levels. This could be as applicable to general practice as advanced practice – there is nothing unique to advanced practice for this statement
Relevance and applicability of capabilities
There were concerns about the relevance and necessity of some of the capability statements, with feedback suggesting that certain capabilities seemed redundant or unnecessary for advanced practitioners. Some respondents felt that these capabilities were inherently part of any healthcare provider's role, such as ensuring patient safety or engaging in person-centred care. This feels a little redundant to me as any advanced practitioner is doing this is as an intrinsic part of their role. I’m not sure that it needs to be explicitly stated this way.
Cultural sensitivity and patient-centred care
Another prominent theme was the need to better incorporate cultural sensitivity and patient-centred care into the capability statements. Participants recommended specific terminology such as ‘culturally sensitive care’, ‘health literacy’ and ‘advocacy’ to reflect the importance of these concepts. Recommended terms … culturally sensitive care, diverse needs, advocacy, supporting health literacy, culturally informed care. Respecting core values and spiritual beliefs.
Furthermore, feedback highlighted the need to ensure that patient involvement is central to the care process. Ensuring the co-constructed care plan is culturally safe
Phase 3 – Refinement of new capabilities
Phase 3 had a response rate of 61% (n = 28) to refine new and refined capabilities generated from Phase 2. See Supplementary Table 2 for revised capabilities and comparison of ratings between Phases 2 and 3. All six revised capabilities were accepted. See Table 5 for Phase 3 results.
Phase 3 results.
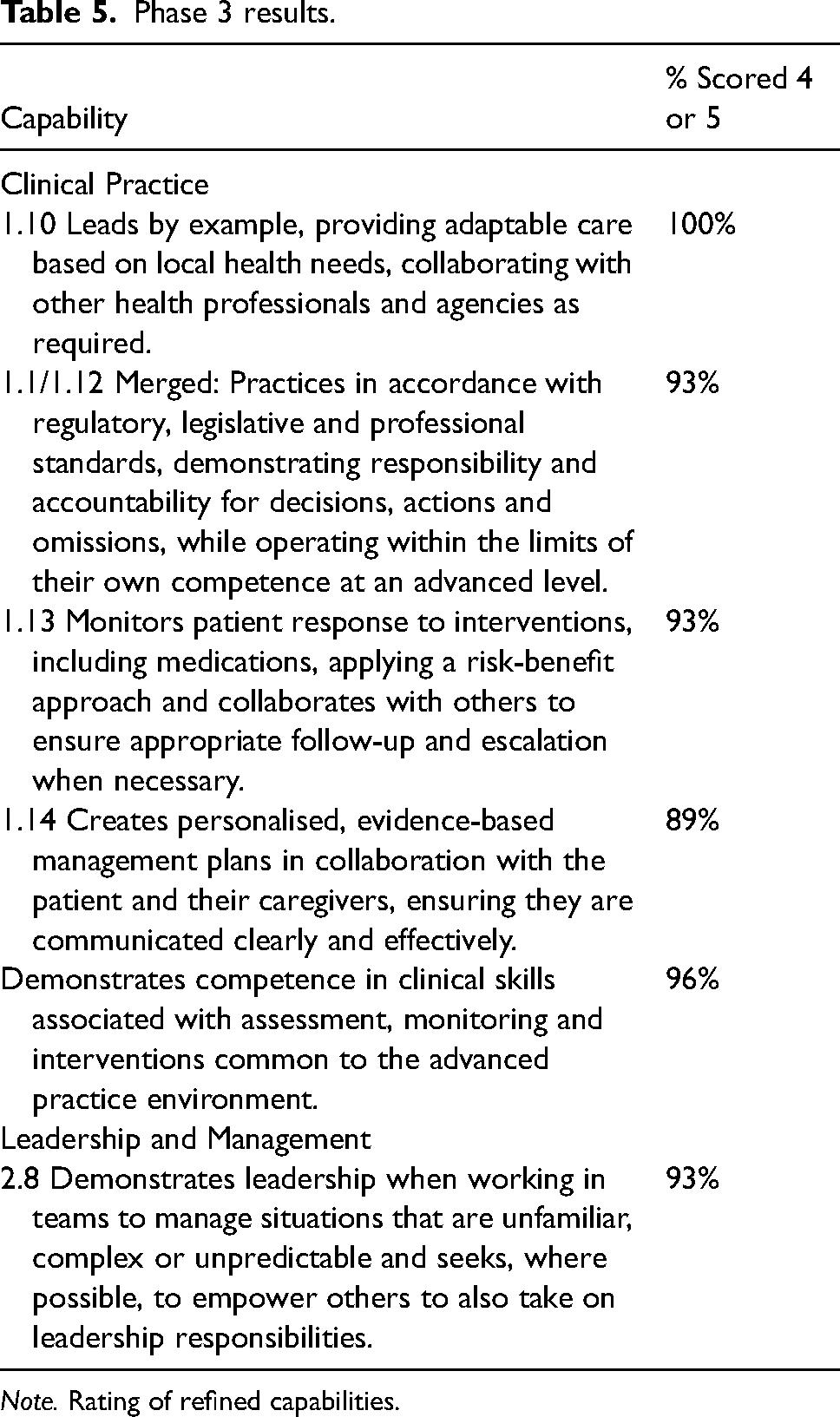
Note. Rating of refined capabilities.
Content analysis of free-text responses – Phase 3
Phase 3 yielded limited free-text responses from participants. Much of the feedback echoed themes from earlier phases, emphasising the need for clarity and specificity in language, as well as clear distinctions between advanced and standard practice. However, Phase 3 also saw an increase in positive responses, highlighting significant improvements in the language and specificity of the revised capabilities. This is much better stated and is more inclusive. This is a significant improvement
Phase 4 – Acceptance or rejection of capability framework
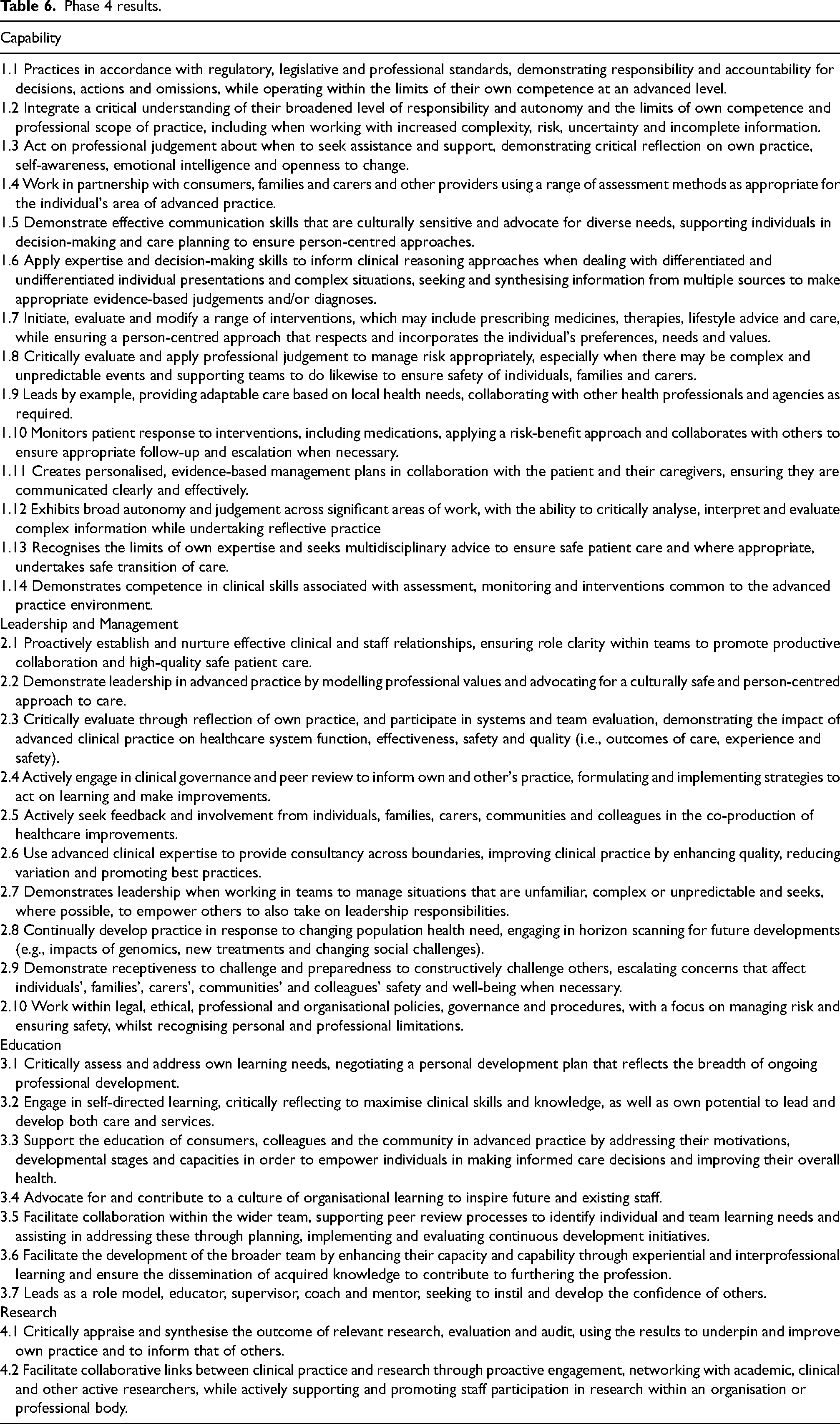
Phase 4 had a response rate of 54% (n = 26) achieving 96% consensus across all four separate domains of capabilities presented. This resulted in a finalised list of 33 capabilities distributed across the domains as follows: Clinical Practice with 14 capabilities, Leadership and Management with 10, Education with 7 and Research with 2 capabilities. Table 6 presents the complete list of the 33 accepted capabilities by domain.
Phase 4 results.
Content analysis of free-text responses – Phase 4
Free-text responses in Phase 4 were minimal, with only a few participants providing comments within each domain. Among the feedback, a recurring concern was that the capabilities appeared too generic and not sufficiently tailored to advanced practice. One participant specifically highlighted a significant gap in the approved capabilities within the research domain, expressing disappointment with the limited emphasis on research: I'm disappointed in the minimal research capabilities and the lack of those in advanced practice to take a lead role in enhancing the evidence base for the profession. We have shown a lack of maturity compared to other nations who see research as a key component of advance practice, and I feel we have missed the opportunity to embed research as a key domain in future practice.
Discussion
The purpose of this Delphi process was to gain expert consensus on capabilities which could inform a national capability framework for APPs in Australia. Through four phases a list of 33 capabilities reached consensus across the domains of clinical practice, education, leadership and research. The findings of this Delphi process align with broader debates in the literature about the challenges of developing clear and consistent capability frameworks, particularly in the health sector, where ambiguity in language can be problematic. 28 Capability frameworks often conflate functional and behavioural approaches, blending task-specific capabilities with broader professional behaviours in ways that create conceptual ambiguity. 43 For instance, some capability frameworks categorise specific knowledge areas as capabilities, deviating from the notion of capabilities as attributes demonstrated through behaviour. 28 These inconsistencies lead to a misalignment between a framework's definitions, conceptual underpinnings and intended applications and undermining their effectiveness. Additionally, educators often critique capability frameworks that reduce the concept of capabilities to discrete tasks and their associated standards, arguing this approach oversimplifies professional practice and overlooks the broad range of attributes required for effective performance.24,28,44–46 Literature emphasises that defining roles through isolated tasks is insufficient without considering the real-world context in which these tasks occur. 47 Conversely, industry perspectives highlight the challenges of assessing abstract attributes such as empathy and resilience, suggesting that their inclusion may undermine a framework's validity as a tool for evaluating professional competencies.23,28,48,49
The challenges in defining and categorising capabilities are highlighted when attempting to distinguish between standard and advanced practice roles. This difficulty in clearly delineating the capabilities of standard and advanced practice within paramedicine mirrors a broader issue faced across many healthcare professions in establishing clear definitions of advanced practice.5,50 In this study, participants noted at times overlap in the responsibilities attributed to standard paramedics and those proposed for APPs, making it challenging to delineate or attribute APP exclusive capabilities. This issue is not unique to paramedicine; similar challenges have been identified in professions such as nursing, where role boundaries between registered nurses and nurse practitioners can blur, given the advanced knowledge and specialised scope of the nurse practitioners.26,51 Literature on nursing capability frameworks has pointed out that capabilities attributed to nurse practitioners can also be relevant to registered nurses, who often perform foundational tasks in preparation for escalated or advanced care, highlighting an inherent overlap in practice.26,51,52 A core reason for this overlap lies in the reality that advanced practitioners operate as extensions of non-advanced roles, maintaining a strong basis in standard practice while applying additional advanced skills.
This overlap in role delineation highlights that advanced practitioners must not only extend foundational competencies but also strengthen less mature domains, most notably research. 43 Although consensus was strongest in the clinical, education and leadership domains consistent with other nursing literature,53,54 the research domain provides valuable insight into areas of opportunity for future development in APP. In our Delphi, full consensus emerged only for research capabilities focused on critically appraising evidence and facilitating research engagement, not for leading original research itself. The ability to critically evaluate and integrate research findings into clinical practice is essential for driving innovation, identifying knowledge gaps and contributing to the broader evidence base that supports healthcare advancements.55,56 Advanced practice clinicians often report that research responsibilities are more challenging to navigate compared to clinical, educational and leadership duties.57,58 These challenges are frequently attributed to limited confidence, insufficient time to engage meaningfully with research activities and a lack of formal expectations or pathways which is a phenomenon observed across various sectors and internationally.55,59–61 Some programmes, such as the US National Institute of Nursing Research doctoral tracks, show what targeted support can achieve,62,63 yet these remain the exception. Introducing similar supports in Australia could turn this leading research gap into a clear, expected capability for future APPs.
While the research domain generated further insights, it is important to note that the highest levels of consensus across the Delphi rounds were achieved within the clinical practice domain, where 14 capabilities were ultimately retained. These capabilities reflected strong support for key elements of advanced paramedic autonomy, including clinical reasoning, complex decision-making, interprofessional collaboration and person-centred care, consistent with global literature on advanced practice roles. 64 Translating this into practice means educators teaching postgraduate APP courses should feel confidence mapping curricula to these agreed capabilities. Similarly, the education and leadership domains demonstrated robust consensus, with panellists endorsing the importance of mentoring, team development and system-level thinking as integral to the APP role, capabilities also recognised in nursing literature as essential for advanced clinical roles.53,54 Embedding formal mentorship training and quality-improvement projects into APP programs would operationalise these expectations and create measurable leadership outputs during training. These findings reflect a maturing view of advanced practice in paramedicine, one that balances clinical excellence with leadership and education responsibilities. The convergence of expert opinion around capabilities in clinical leadership, team collaboration and person-centred care mirrors broader healthcare shifts towards integrated, systems-aware models of practice. These attributes position APPs to contribute meaningfully not only to direct care, but also to service redesign, quality improvement and interprofessional models of care delivery.65,66
While many countries face common challenges in paramedicine, including growing demand for out-of-hospital care and an ageing population, which necessitate greater professional autonomy in advanced practice roles. 67 Literature suggests that establishing clear, evidence-based capability frameworks can help ensure consistent and safe standards of care in out-of-hospital settings. 19 Professional autonomy is dependent on enhanced education and robust regulatory frameworks. By focusing on core capabilities that emphasise adaptability, autonomy and transferability, the framework developed in this study could inform national standards for APPs.8,68
Limitations
Whilst a Delphi methodology is viewed as a robust research strategy and methodology was reported utilising the CREDES guideline there were still limitations to the study. Of the 85 participants invited to participate only 46 consented. There was also a noticeable attrition rate across the phases of the Delphi, however every phase had a representative sample greater than 20 with previous research indicating that consensus stability in Delphi studies is typically reached with a minimum of 20 participants. 39 We also acknowledge our decision to limit the expert panel to professionals practicing within the Australian healthcare system rather than including international participants. While international input might have expanded the generalisability of APP capabilities, often each country has unique general registration capabilities and regulatory requirements.69–71 By focusing on Australian participants, we ensured that the resulting capability framework was directly relevant and tailored to Australia's specific healthcare landscape. The relative paucity of new research capabilities may reflect the nascent state of clinical-academic pathways in Australian paramedicine 72 ; future iterations of the framework should revisit this domain as research capacity matures. Finally, Delphi-derived agreement should be interpreted as expert convergence rather than definitive validation; the proposed capabilities require prospective validation by educational, regulatory and clinical authorities to confirm their utility.
Implications
The outcomes of this project have the potential to influence paramedic education and advance the profession. By establishing a capability framework informed by a diverse expert consensus on core capabilities, we can ensure that paramedics are equipped with the right balance of capabilities across the domains of clinical practice, leadership and management, education and research. Developing an Australian national framework based on these identified capabilities will enable APPs to meet the demands of an evolving healthcare environment and set clear expectations for their roles. Furthermore, it will provide regulatory authorities, education providers, healthcare organisations and policymakers with a robust framework to assess the readiness of paramedics for advanced practice roles, thereby enhancing the overall professionalism and credibility of APP roles.
Conclusion
A final compilation of 33 requisite capabilities to inform APP roles in Australia met expert consensus using a four-phase Delphi methodology. The iterative refinement process ensured that these capabilities, organised under the domains of clinical practice, leadership and management, education and research, accurately reflect the unique and evolving demands of APP roles. The final compilation provides clear, relevant and actionable capabilities that can guide the education, training and practice of APPs. Future work should encompass broad stakeholder consultation and iterative evaluation across Australia while also providing a flexible reference point for international adaptation. The adoption of these capabilities by relevant bodies holds potential to standardise APP roles nationally and contribute to the overall advancement and recognition of the paramedic profession within the healthcare system.
Supplemental Material
sj-docx-1-pam-10.1177_27536386251360833 - Supplemental material for National consensus on the capabilities that inform the role of advanced practice paramedics: A Delphi study
Supplemental material, sj-docx-1-pam-10.1177_27536386251360833 for National consensus on the capabilities that inform the role of advanced practice paramedics: A Delphi study by Alessia Restiglian, Lorna Martin, David Long, Louise Reynolds, Tony Walker, Ben Meadley, Ashleigh Finn, Alan Batt, Alecka Miles and Tania Johnston, Brendan Shannon in Paramedicine
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Alan Batt is a Deputy Editor for Paramedicine, Dr David Long and Dr Louise Reynolds are Associate Editors for Paramedicine, all played no role in editorial decision making, which was conducted in adherence to the journal's blind review policy. All other authors declare no actual or perceived conflict of interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.