
Abstract
Acute pain management in children and young people (CYP) attended by ambulance services is a significant challenge due to the complex nature of pain, the variation of approach needed across the age range, and the unpredictability of the environment. We aimed to understand how ambulance clinicians can provide improved prehospital acute pain management for CYP. A realist review was conducted and reported in accordance with the Realist And Meta-narrative Evidence Syntheses: Evolving Standards (RAMESES) guidance. We developed an initial programme theory (PT) using key stakeholder input, searched the major bibliographic databases MEDLINE, CINAHL Complete and PsycINFO, and other sources from January 2000 to February 2024, screened and assessed relevance and rigour in duplicate, and performed synthesis and programme theory refinement. We developed an initial PT that focussed on the preparedness of staff and the expectations of CYP and parents/carers, along with key outcomes such as pain score severity, fear and anxiety. The subsequent search strategy yielded 1503 documents, of which 95 were included, representing empirical research articles, reviews, theses, book chapters and clinical guidelines. The initial PT was tested and refined throughout the synthesis to produce a PT underpinned by 34 context-mechanism-outcome configurations. The PT portrayed positive (e.g. presence of parents, focussed education and training, building trust) and negative (e.g. misinformation, fear and anxiety, long-term consequences) effects on prehospital acute pain management for CYP. This PT was mapped to the Behaviour Change Wheel to provide a clinically relevant behaviour change model for improvement. This realist review has provided a clinically focussed model to guide the improvement of prehospital acute pain management in children and young people attended by ambulance. The programme theory lays a foundation on which future empirical testing can be conducted to effect behaviour change in practice. Registration: CRD42024505978.
Introduction
Every child and young person experiences pain at some point in their life. 1 Across England each year, 90,000 CYP under 18 years of age are transported by ambulance to emergency departments suffering acute pain,2,3 with an estimated 61% not achieving effective pain management (defined as the abolition or reduction of pain by 2 or more points on a 10-point scale). 3 While pain is inevitable, suffering is not. The potential consequences of poor acute pain management can include the development of post-traumatic stress disorder,4,5 altered pain perception,6,7 and the subsequent development of chronic pain.8,9
Pain is a complex sensory and emotional experience that is influenced by biopsychosocial factors. 10 Individuals also learn the concept of pain through their life experience. 10 Fear and anxiety are often experienced by CYP during painful emergencies, 11 which may lead to pain catastrophising – amplifying the perception of pain.12,13 Communication between the ambulance clinician and child has been identified as key to building trust, with limited scope of analgesics identified as a barrier to effective pain management. 14 A holistic, biopsychosocial approach, therefore, is key to managing acute pain and mitigating its consequences in CYP.
Environment is also a key consideration, as unlike paediatric emergency departments, ambulances typically do not have a broad suite of analgesics on board, nor do clinicians have extensive training on the management of pain in CYP. 15 In addition, the unpredictable nature of the prehospital environment, including weather, facilities and available resources, places further strain on ambulance clinicians. 16 These factors act as barriers to effective prehospital pain management.
Given the need for a biopsychosocial approach and the environmental challenges, this realist review aimed to understand how ambulance clinicians can provide improved prehospital acute pain management for CYP. Specifically, we aimed to:
Develop an initial programme theory (PT) to map the key processes of prehospital acute pain management in CYP. Focus on specific areas of the initial PT to explore potential behaviour change intervention components aimed at ambulance clinicians and determine: for whom, in what circumstances, how, and to what extent they work. Refine the initial PT into a realist PT supported by context, mechanism, outcome configurations (CMOCs).
The focus of the review was broad, aiming to capture the process of pain management in ambulance care holistically rather than focus on a specific intervention. A broad focus was adopted to facilitate intervention development – being able to target the most suitable parts of a broad programme theory should enable us to develop a strong evidence-based intervention.
Methods
Study design
This realist review represents stage one of the ‘improving Pain mAnagement for childreN and young people attendeD by Ambulance’ (PANDA) study, see Figure 1. The overall design of this programme of research is a realist informed17–21 complex intervention development and feasibility study, following the Medical Research Council (MRC) complex intervention development guidance. 22 A realist review was chosen to conform to these guidelines, 22 which acknowledges the importance of context and the need to develop and refine programme theory when developing complex interventions.
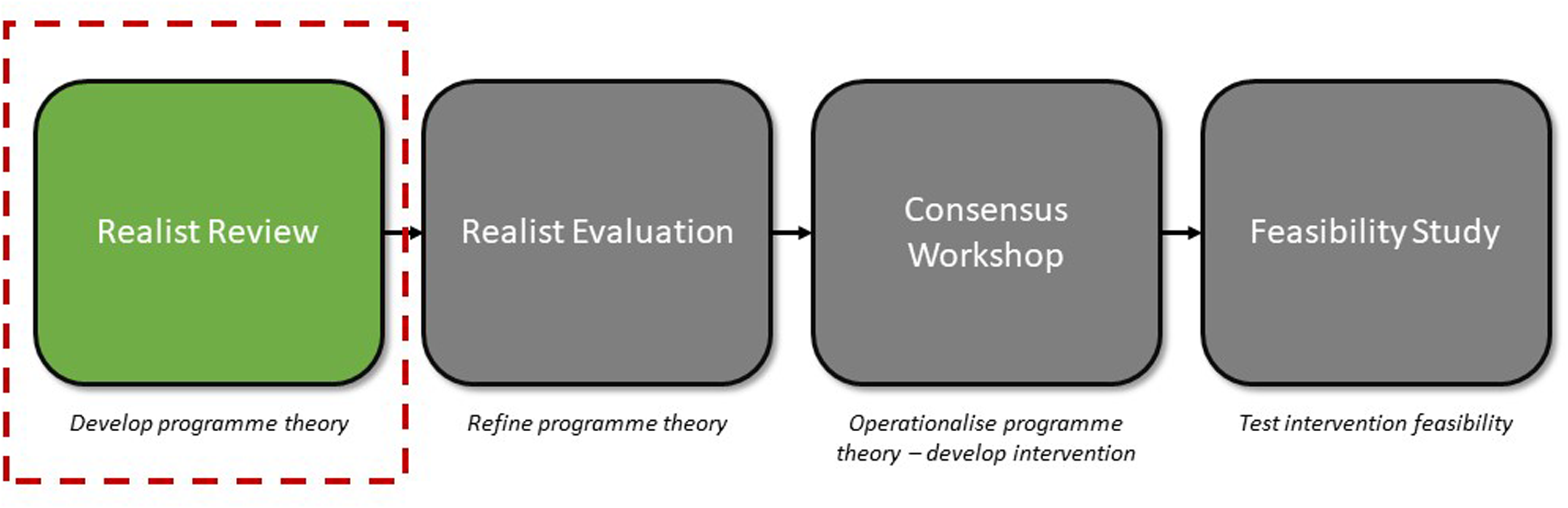
PANDA study overview.
This realist review has been conducted and reported according to the Realist And Meta-narrative Evidence Syntheses: Evolving Standards (RAMESES) guidance,23,24 registered on PROSPERO (CRD42024505978) and the protocol has previously been reported. 25 No changes were made from the published protocol.
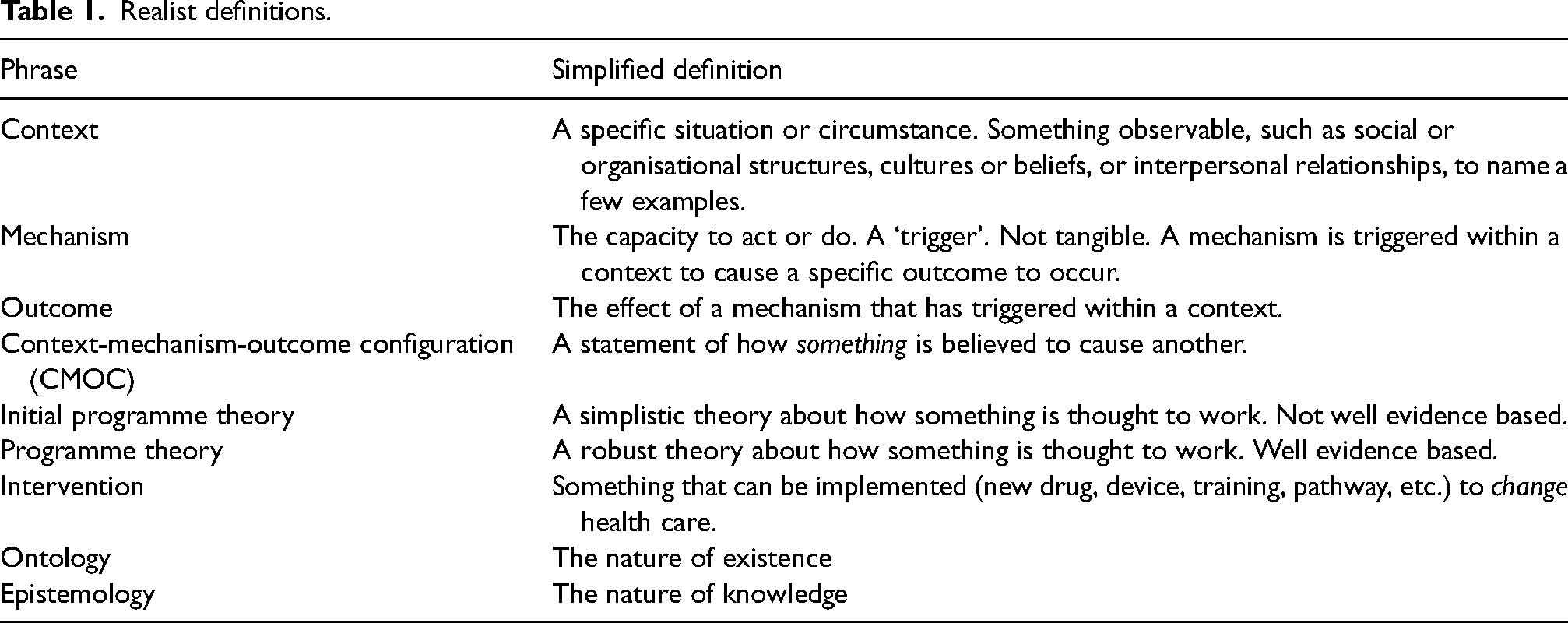
The language used within realist research can be confusing; therefore, we provide a simple lay translation for many of the key terms and phrases used within this paper to make this work more accessible (see Table 1).
Realist definitions.
Theory
Realist reviews are situated within a realist philosophy of science,21,26 which is founded on the principles of Bhaskar's critical realism. 27 This theoretical stance acknowledges that we can never fully know the truth about the scientific world due to flawed human ability to perceive and comprehend it, but we can build our knowledge on a foundation dug deep enough to support itself, for now. 28
According to Pawson and Tilley, there are hidden areas of reality containing causal structures, including mechanisms, and observable areas that contain events, including contexts and outcomes. 19 In the pursuit of causal explanation, realist researchers combine these to create context-mechanism-outcome configurations, illustrated as C + M = O. These statements simply explain how one thing is thought to cause another, for example: ‘The parent of a small child will offer a cuddle when they fall over and graze their knee (C) because the sense of safety (M) will make the child feel better (O)’. Such statements need evidence to support them. When adopting a realist approach, the realist epistemological position accepts and encourages the use of multiple types of data, including both quantitative (numerical data) and qualitative (non-numerical data, including audio, written text and images).
Stakeholder involvement
Several stakeholder groups were involved in this realist review to help develop the Initial Programme Theory (IPT) and discuss possible CMOCs, ensuring that different perspectives were considered when developing and adjudicating between them. The groups met separately, as required throughout the review, and any difference of opinion between groups was discussed and managed iteratively by the PANDA study realist review working group.
Young Persons Advisory Group
A Young Persons Advisory Group (YPAG) consisting of 25 members, aged 12 to 18 years, recruited from a local secondary school, were involved in the initial design of the PANDA study. The group was mixed in sex (60% female) and ethnicity (64% White British, 24% Asian or Asian British, and 13% other of mixed ethnicity). Six members attended a 50-min face-to-face session in February 2024 to discuss the initial PT, and propose important contexts and outcomes relevant to CYP, such as their expectations when an ambulance is called. The YPAG lead (TB) was then involved in interpreting this input and translating it into the initial PT. A final face-to-face session was held in January 2025 to discuss the review findings.
Ambulance Clinician Advisory Group
An Ambulance Clinician Advisory Group (ACAG) consisting of four members from the fields of clinical practice, education and leadership were recruited across England and Scotland. An initial online 1-hour meeting was held to discuss the initial PT, and several refinements were made based on feedback. Subsequent discussions were held via email, with pre-recorded presentations of the CMOCs and programme theory development shared with the group. This allowed a sense check of the CMOCs and final programme theory, with changes made based on feedback.
Healthier ageing patient and public involvement (HAPPI) group
An established patient and public involvement group based at the University of Lincoln (the HAPPI group) supported and advised on the overall PANDA study and has met twice to support design and delivery activities. The group met a third time in February 2025 to review the findings of this review and provide insights from a public perspective.
PANDA study realist review working group
The PANDA study realist review working group contained expertise in paramedicine, nursing, general practice, psychology, library services, realist methods and lived experience, with multiple members holding clinical academic roles. Online and face-to-face meetings were held monthly as a minimum, with meetings occurring every two weeks during Step 5, with iterative email discussions supplementing the meeting schedule as needed.
Realist review stages
A five-stage approach for this realist review was adopted, supported by the RAMESES guidance 23 and a previous realist review. 29
Step 1: Locating existing theories and developing initial programme theory
Existing theories and documents were initially sourced from a PhD thesis on the topic of prehospital pain management in children. 30 The author (GAW) also had a large collection of resources relevant to the topic. These were combined with informal searching of PubMed and Google Scholar to identify recently published documents.
The initial PT was developed using the sourced documents and iterative discussion with key stakeholder groups, as outlined above. All members contributed to the iterative development of the initial PT via multiple face-to-face, online and email discussions.
Step 2: Searching and screening
Using the initial PT as a framework, we developed a comprehensive search strategy. The following databases were searched between the dates January 2000 to February 2024 MEDLINE, Cumulative Index to Nursing & Allied Health (CINAHL) Complete, PsycINFO, Web of Science Core Collection, Education Source, and Education Resources Information Centre (ERIC) from within the EBSCOHost platform. The search string used for each database, developed with the support of an academic librarian (MO), can be found in the Supplementary File.
Other resources were searched, including the Cochrane Library, the clinical trials registry ISRCTN, ProQuest, ProQuest Dissertations and Theses, and Google. Expert knowledge was included at this stage to identity relevant documents not found in formal searches. This included emailing the ACAG and discussing with the PANDA study realist review working group to request relevant resources. Once the initial searches had been completed, forward and backward citation tracking was then conducted on all included documents.
Only documents reported in English, and involving or aimed at the following populations were included:
Ambulance clinicians (including but not limited to paramedics, emergency medical technicians, prehospital emergency nurses) who attend children and young people (CYP) suffering acute pain. Children and young people suffering acute pain in the prehospital setting. Parents/carers of CYP suffering acute pain in the prehospital setting.
Documents were excluded if they were:
Based in the battlefield, in-hospital, primary care or helicopter emergency medical service (HEMS) setting. Documents from these settings would not be representative of standard ambulance service practice. Focussed on chronic pain.
Identified documents from the database search were imported into Covidence software and then independently screened in duplicate (GN and GAW), first by title and abstract, then by full text review against the inclusion and exclusion criteria. Documents that were identified from the additional resources search were added to and managed using Microsoft Excel software and were also independently screened in duplicate by the same authors. All grey literature documents were subject to an initial screen – similar to a title and abstract screen – followed by a full-text screen, where the full document was reviewed against inclusion and exclusion criteria. Any disagreements were resolved through discussion between GN and GAW initially, and if unresolved, via group discussion with the PANDA study realist review working group.
Step 3: Relevance and rigour assessment
Documents that met the inclusion criteria were assessed for relevance and rigour. A document was deemed relevant if the data within could contribute to the testing and refinement of the initial PT, and rigour was conceptualised as whether or not the methods used to generate the relevant data were credible and trustworthy. 23
Two reviewers (GN and GAW) assessed relevance separately using a binary ‘yes/no’ system, which was conducted within MS Excel software, with disagreements settled through discussion. As a benchmarking exercise, three documents were assessed in duplicate and then reviewed by the PANDA study realist review working group – full agreement was achieved. Once the relevance assessment was complete, a third reviewer (MB) then examined 10% of the reviewed documents to ensure consistency. Any documents that were deemed not to be relevant were excluded from the review.
Rigour was assessed according to the work of Dada et al. 31 at two different levels. First, at the data level, and then at the level of the programme theory. Each document was assessed for rigour in duplicate by two reviewers (GN and GAW) and was based on the reviewer judgement as to how trustworthy the document was. A three-tiered rating scale was used – low, moderate, or high. Clarity of methods used and supporting evidence within the document was assessed during this process. Any disagreements were settled through discussion. A third reviewer assessed a random sample of 10% [MB]. Rigour was not used as a reason for exclusion for any document, however any CMOCs that were considered conceptually weak (supported by few and/or low rigour documents) were removed from the final programme theory.
Step 4: Extracting and organising data
The first part of this step included collating details of all relevant documents to form a summary of the included documents table. This included: author and year, title, document type, country, population group, sample size, and aim.
The second part of this step was to upload the included documents to NVivo version 14 software for data extraction. Both qualitative and quantitative data were coded. Coding was considered deductive (based on the initial PT) and inductive. Initial coding into ‘conceptual buckets’ was completed by a single reviewer (GN), with 10% of all coded documents being checked by a second (GAW). Text was coded into multiple ‘conceptual buckets’ where appropriate. Example ‘conceptual buckets’ included: ‘Education and Training’, ‘Fear and Anxiety’ and ‘Limited Exposure’.
Step 5: Synthesis and programme theory refinement
As each ‘conceptual bucket’ grew with more coded data, the review team met to assess the ‘bucket’ and determine as far as possible what was functioning as context, mechanism, and outcome. Using a realist logic of analysis, 21 we developed context-mechanism-outcome configurations (CMOCs). This was an iterative process supported by input from various key stakeholders to sense check the statements. Data from more than one conceptual bucket were used to create multiple CMOCs. We juxtaposed, reconciled, adjudicated, consolidated or situated data throughout the analytic process, as necessary. 21
Each new CMOC was contained within its own ‘parent node’ within NVivo, and a ‘linked memo’ attached, describing all the changes made to the CMOC during iterative discussion with key stakeholders. All supporting excerpts from included documents that contributed to the development of each CMOC were captured within the ‘parent node’. CMOCs that were not fully substantiated were excluded from the final programme theory and retained (rather than deleted) as primary data from the subsequent realist evaluation may substantiate them.
All developed CMOCs were printed and organised into groups based on outcome. These ranged from proximal outcomes (focussed on the ambulance clinician) to distal outcomes (longer-term consequences). Similar clusters of CMOCs were grouped and labelled according to their common context or mechanism. These were illustrated and discussed iteratively among key stakeholder groups. Once agreement was in place for the final CMOCs and CMOC clusters, we began to search for substantive theories that could support the final programme theory. Again, this was an iterative process, drawing on the expertise of the research team and iterative searching for theories in the fields of education, sociology, psychology, and health.
Results
An initial PT was developed, which focussed on the contexts of preparedness and expectations, with key outcomes identified as pain score severity, confidence, and fear and anxiety. Potential mechanisms were identified as trust and empowerment, and two if-then statements were produced to support the theory, see Figure 2.
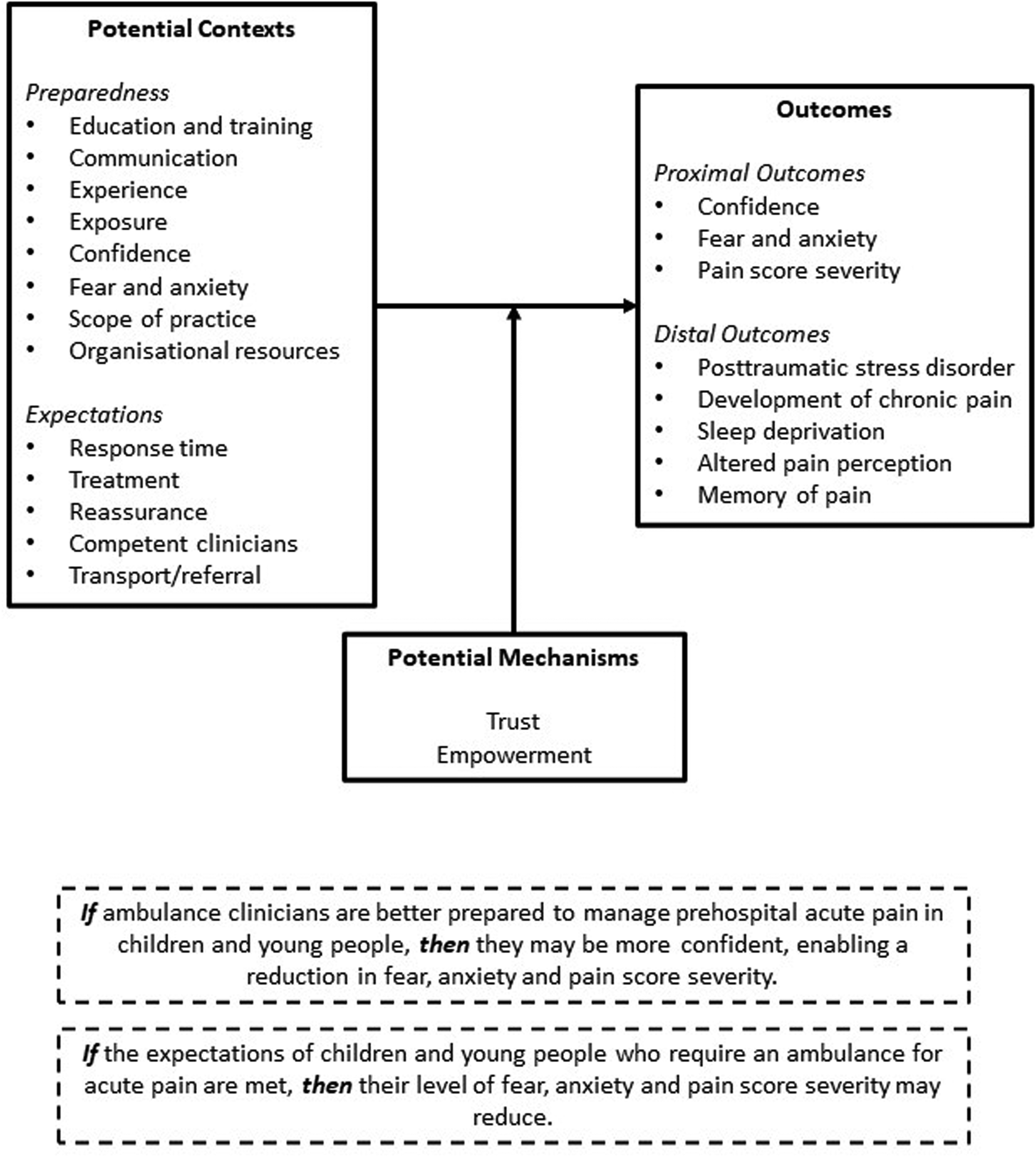
Initial programme theory.
Based on this initial PT, the subsequent search strategy identified 1503 documents for screening. After screening and assessment of relevance, 95 documents were included, see Figure 3. for the PRISMA flow diagram. 32
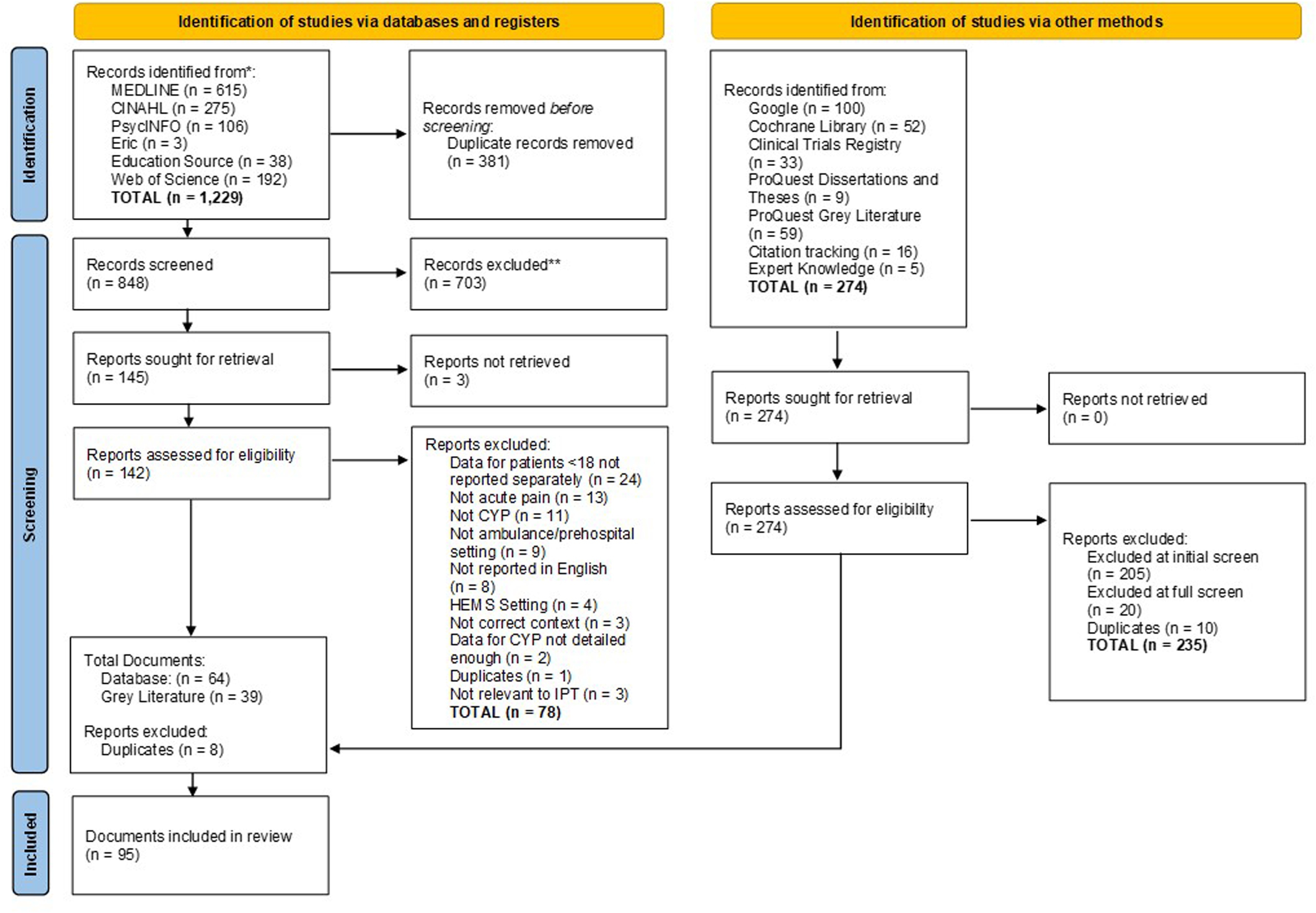
PRISMA flow diagram.
We did not perform any additional iterative searches to further refine the final programme theory due to time and resource constraints. Instead, we will conduct further refinement and testing through our planned realist evaluation (see Figure 1).
These 95 included documents represented a range of empirical research articles, reviews, theses, book chapters and clinical practice guidelines, see Figure 4.
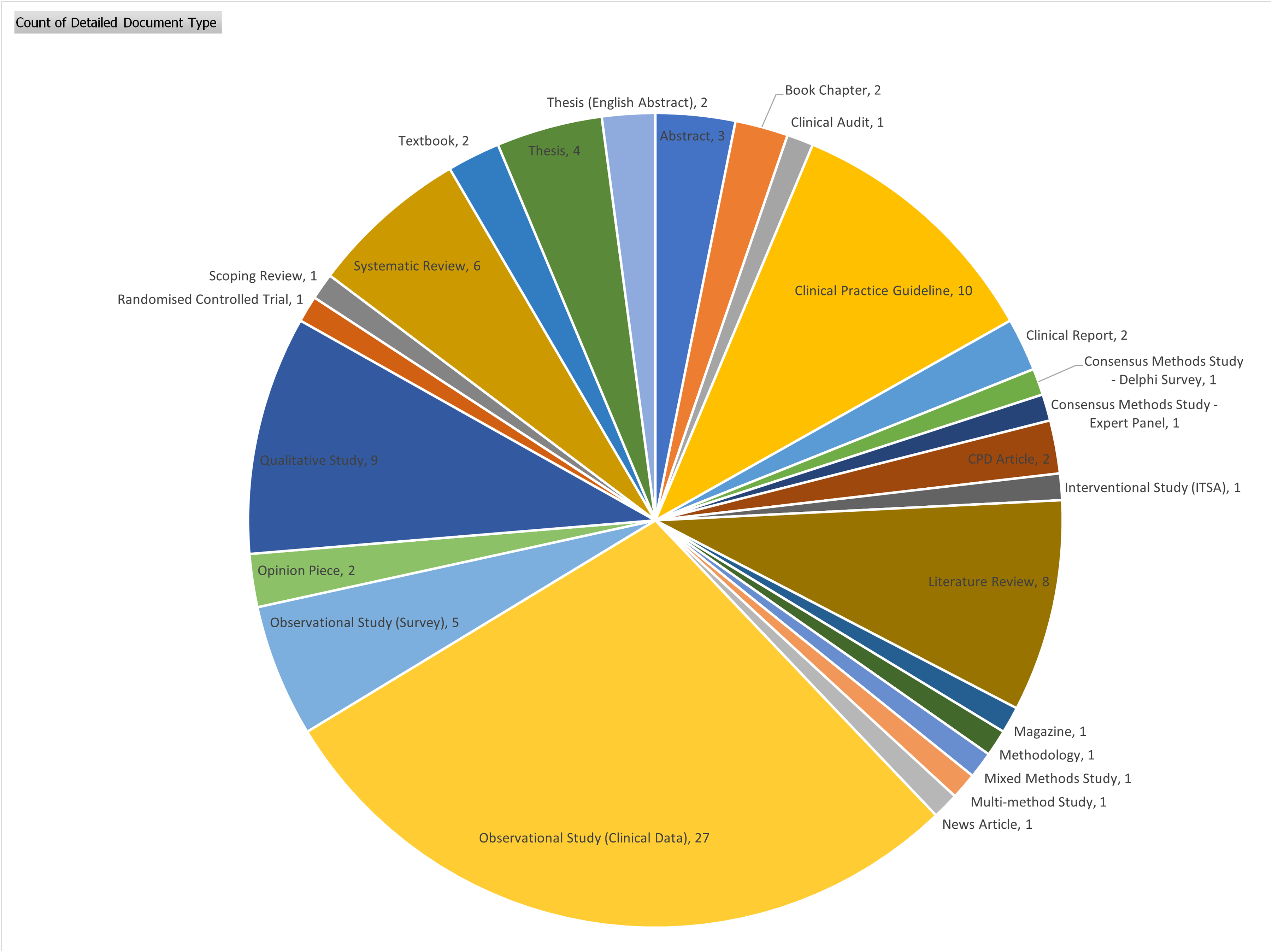
Included documents. ITSA – interrupted time series analysis.
As the figure shows, 32 observational studies were identified and included in this review, illustrating the prevalence and relative ease at which these studies can be conducted. The table of included documents, along with the rigour assessment at the level of the data source, can be found in the Supplementary File.
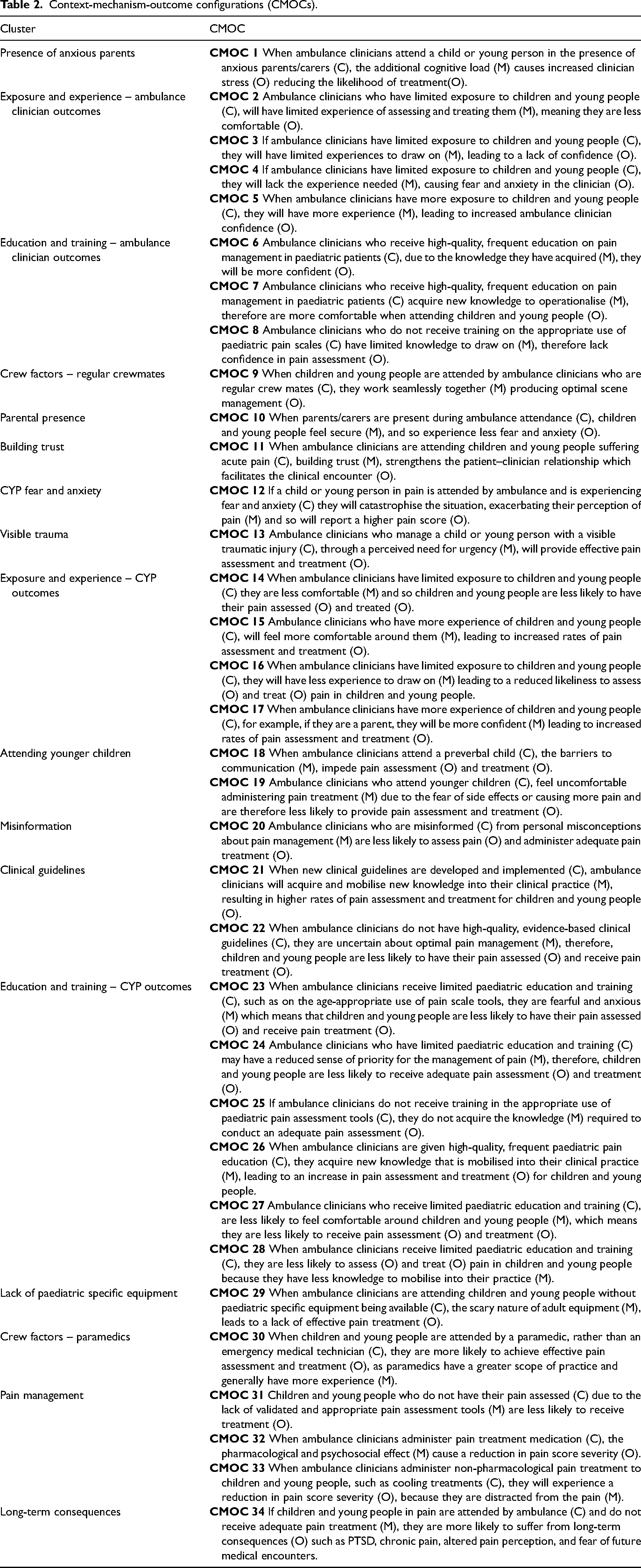
After data extraction, organising and analysis, 34 CMOCs were developed, see Table 2.
Context-mechanism-outcome configurations (CMOCs).
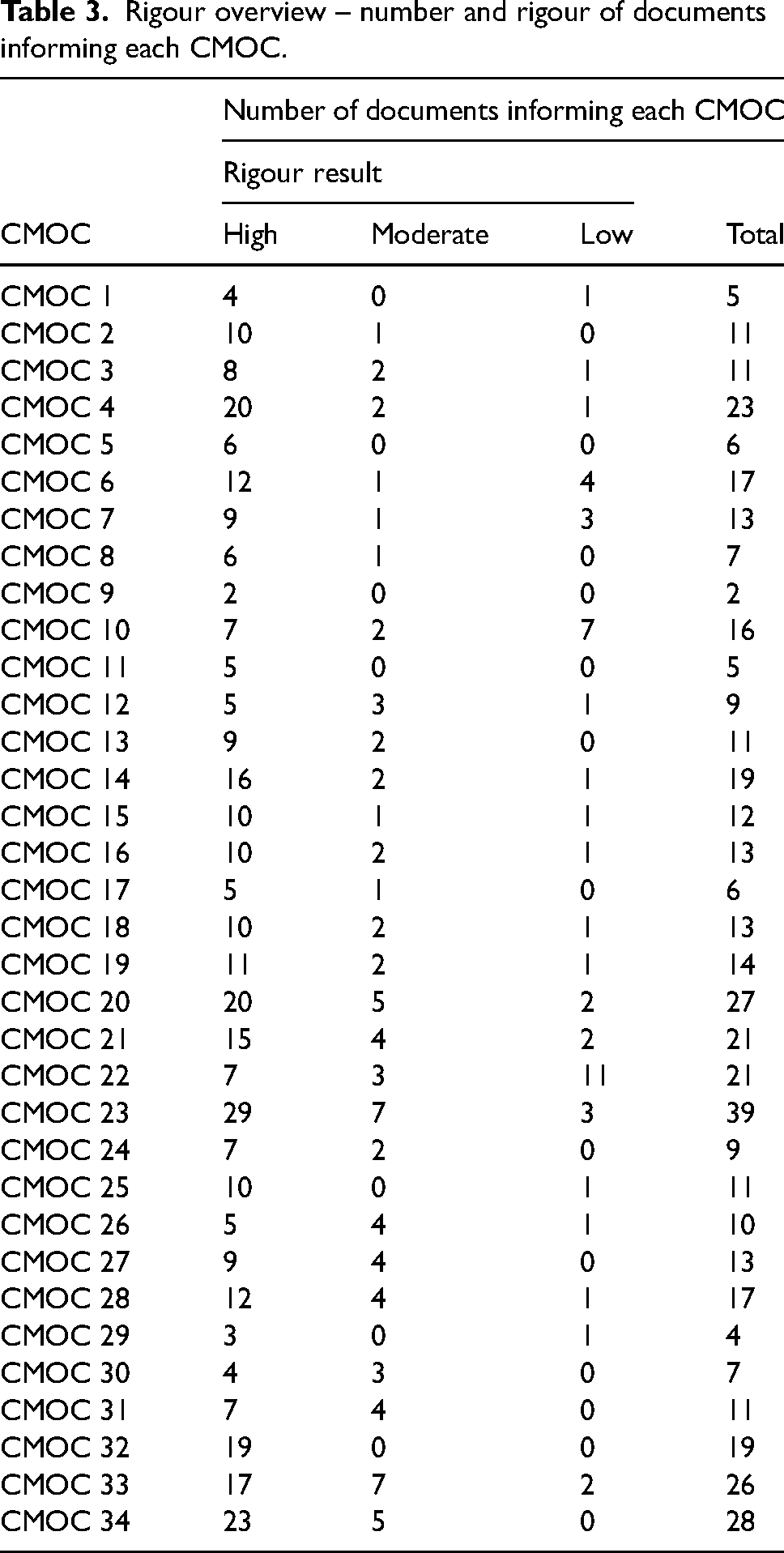
To visualise the rigour of these CMOCs, we have cross-referenced the document rigour assessment with the CMOCs to show a) how many documents supported each CMOC and b) the rigour of those documents, see Table 3. The vast majority of CMOCs are substantiated by several high rigour documents, except CMOC 22 which is substantiated by a large number of clinical guidelines – these were deemed low rigour.
Rigour overview – number and rigour of documents informing each CMOC.
Programme theory
The initial PT was tested and substantially refined into the final realist programme theory, see Figure 5. The CMOCs supporting the programme theory can be traced back to Table 2, and the supporting data for each CMOC can be traced back to the Supplementary File, enabling full transparency.
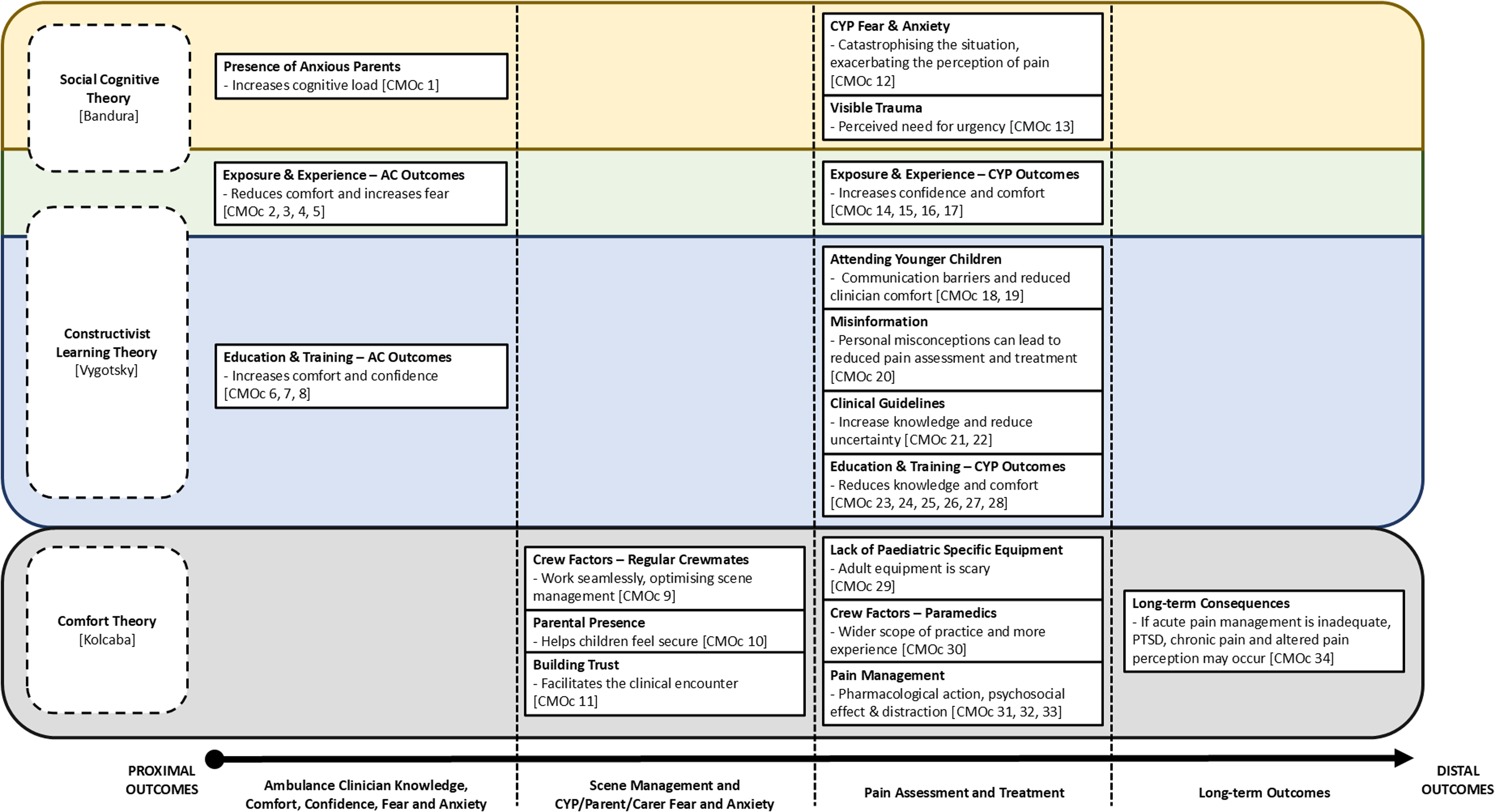
Programme theory. Key: CMOC = context-mechanism-outcome configuration, AC = ambulance clinician, CYP = children and young people, PTSD = posttraumatic stress disorder.
The programme theory is illustrated with the CMOC clusters (from Table 2) segregated into four columns. Each column represents a different level of outcome, from proximal (related to the ambulance clinicians) to distal (post-incident consequences).
The programme theory also has cross-cutting substantive theories, and CMOC clusters have been organised according to substantive theory, with Social Cognitive Theory and Constructivist Learning Theory overlapping. The incorporation of these substantive theories helps to give the programme theory more validity. Multiple substantive theories were needed due to the distinct clinical, cognitive, and learning aspects of the programme theory.
Comfort theory
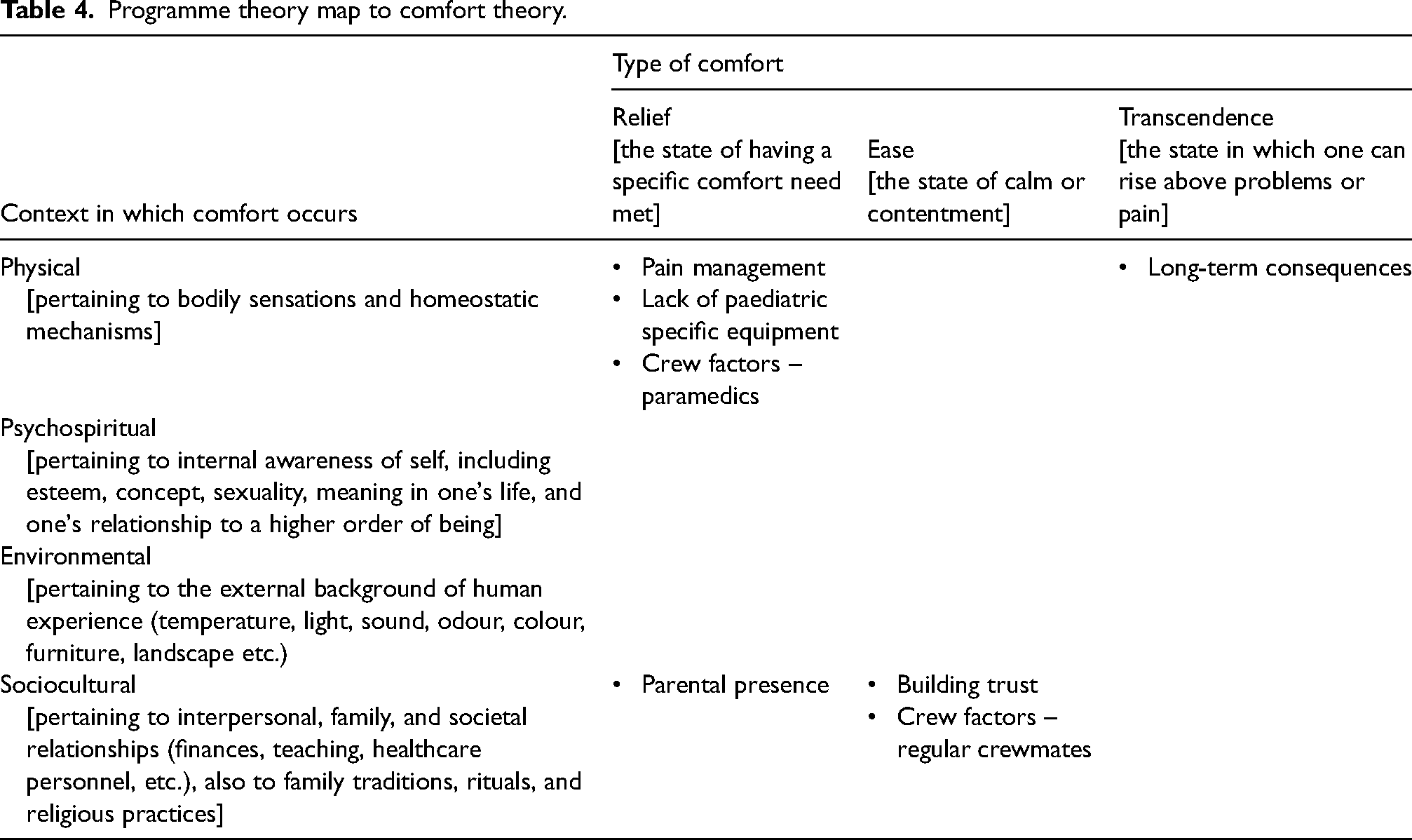
Kolcaba developed Comfort Theory33,34 in the context of nursing as a framework to better understand the basic human need for relief, ease and transcendence arising from stressful healthcare situations. The three types of comfort are: Relief – the experience of having had a specific need met or mediated; Ease – the state of calm or contentment; and Transcendence – the state in which one rises above problems or pain. 34 Cross-cutting these three types of comfort are four contexts in which comfort is thought to occur: Physical – pertaining to bodily sensations or functioning; Psychospiritual – pertaining to internal awareness of self; Environmental – pertaining to light, noise, ambience, colour and temperature; and Sociocultural – pertaining to interpersonal, family, healthcare professional and societal relationships.33–35
In the context of prehospital pain management in children and young people, the pharmacological action, psychosocial effect and distraction techniques [Pain Management], along with adult equipment being scary [Lack of Paediatric Specific Equipment] and paramedics being on scene with a greater scope of practice and more experience [Crew Factors – Paramedics] were all influencing factors in the provision of Relief in the Physical context. Children and young people feel secure when their parents are present during a stressful incident [Parental Presence], enabling Relief in the Sociocultural context. When ambulance clinicians build trust with CYP, it facilitates the clinical encounter [Building Trust] and when ambulance clinicians work together as regular crewmates, scene management is optimised [Crew Factors – Regular Crewmates], both facilitate Ease in the Sociocultural context. When acute pain is not managed well, CYP may suffer PTSD, chronic pain or altered pain perception [Long-term consequences], inhibiting Transcendence in the Physical context. See Table 4 for the programme theory map to Comfort Theory.
Programme theory map to comfort theory.
Constructivist learning theory
Constructivist learning theory, which stems from the work of Vygotsky (1962), posits that people construct their own understanding and knowledge of the world through social learning and experience, reconciling information from past and current knowledge and experience into new personal knowledge and understanding.36,37 Learning is considered an active process that is constructed over time and built on the foundation of previous knowledge. If ambulance clinicians have high quality education and training [Education & Training – Ambulance Clinician Outcomes] they feel more comfortable and confident attending children and young people suffering acute pain, whereas if they have limited education and training [Education & Training – CYP Outcomes] children and young people are less likely to have their pain assessed and treated adequately. Ambulance clinicians who are misinformed (through social learning) carry misconceptions about pain management that negatively impact pain assessment and treatment [Misinformation]. Clinical guidelines are used as part of the learning process, and where new clinical guidelines are developed and implemented, knowledge acquisition and mobilisation increases, while uncertainty decreases [Clinical Guidelines]. When ambulance clinicians attend younger children, the barriers to communication and lack of comfort administering pain treatment [Attending Younger Children] impede pain assessment and treatment – this in part may be due to lack of social learning and experience caused by limited exposure to younger children. Ambulance clinicians who have more exposure to and experience of children and young people [Exposure and Experience – CYP Outcomes] feel more confident and comfortable, therefore are more likely to assess and treat pain. Whereas those with limited exposure to and experience of children and young people [Exposure and Experience – Ambulance Clinician Outcomes] feel less comfortable and more fearful.
Social cognitive theory
Bandura developed Social Cognitive Theory and articulated the concept of ‘self-efficacy’ which relates to one's belief and confidence in their ability to perform a particular behaviour.38,39 In this case, the child or young person will have a certain belief in their ability to cope with acute pain caused by a medical illness or injury. This self-efficacy may be modelled on observing others in similar situations (such as parents, siblings or friends), informed by previous painful experiences, by social persuasion, or based on physiological experience (such as the anxiety or pain itself). If a child or young person has little self-efficacy, they are likely to experience more fear, anxiety and increased pain associated with the problem, resulting in catastrophising [CYP Fear & Anxiety]. Bandura also described socio-cultural factors, where environmental, political, economic and health systems influence one's goals. For example, increased anxiety displayed by parents in the context of acute pain diminishes the goal setting ability of a child or young person to have a positive outcome, due to increased catastrophising, but also due to the increased cognitive load and subsequent reduced ability of the ambulance clinician to perform rapid, safe pain assessment and management [Presence of Anxious Parents]. Whereas the urgent assessment and treatment of a visible injury by ambulance clinicians facilitates the child or young person in achieving their goal of having a positive outcome [Visible Trauma].
Once the final programme theory was produced, the final stage of the rigour assessment was completed. The rigour of the programme theory was deemed high because the theory explained the data well (evidenced in the Supplementary File), made a few assumptions about the data, and aligned with existing credible theories (as described above), making the programme theory coherent. 31
Discussion
The aim of this realist review was to understand how ambulance clinicians can provide improved prehospital acute pain management for CYP. The programme theory we have developed from the synthesis of 95 included documents has generated knowledge and insights regarding positive and negative effects on the acute pain management process in CYP attended by ambulance. These effects range from proximal outcomes that impact the ambulance clinician, through outcomes regarding scene management, CYP/parent/carer fear and anxiety, pain assessment and treatment, to distal outcomes that impact CYP after the acute phase of care. Encouraging these positive effects and discouraging the negative effects should lead to improved prehospital acute pain management. This programme theory is presented at the middle-range theory level of abstraction, which permits empirical testing. While this is useful in some ways, it is difficult for individual ambulance clinicians, educators and organisations to implement. 40 Therefore, we developed a clinically focussed model from this programme theory, which can be found later in this paper (see Figure 6).
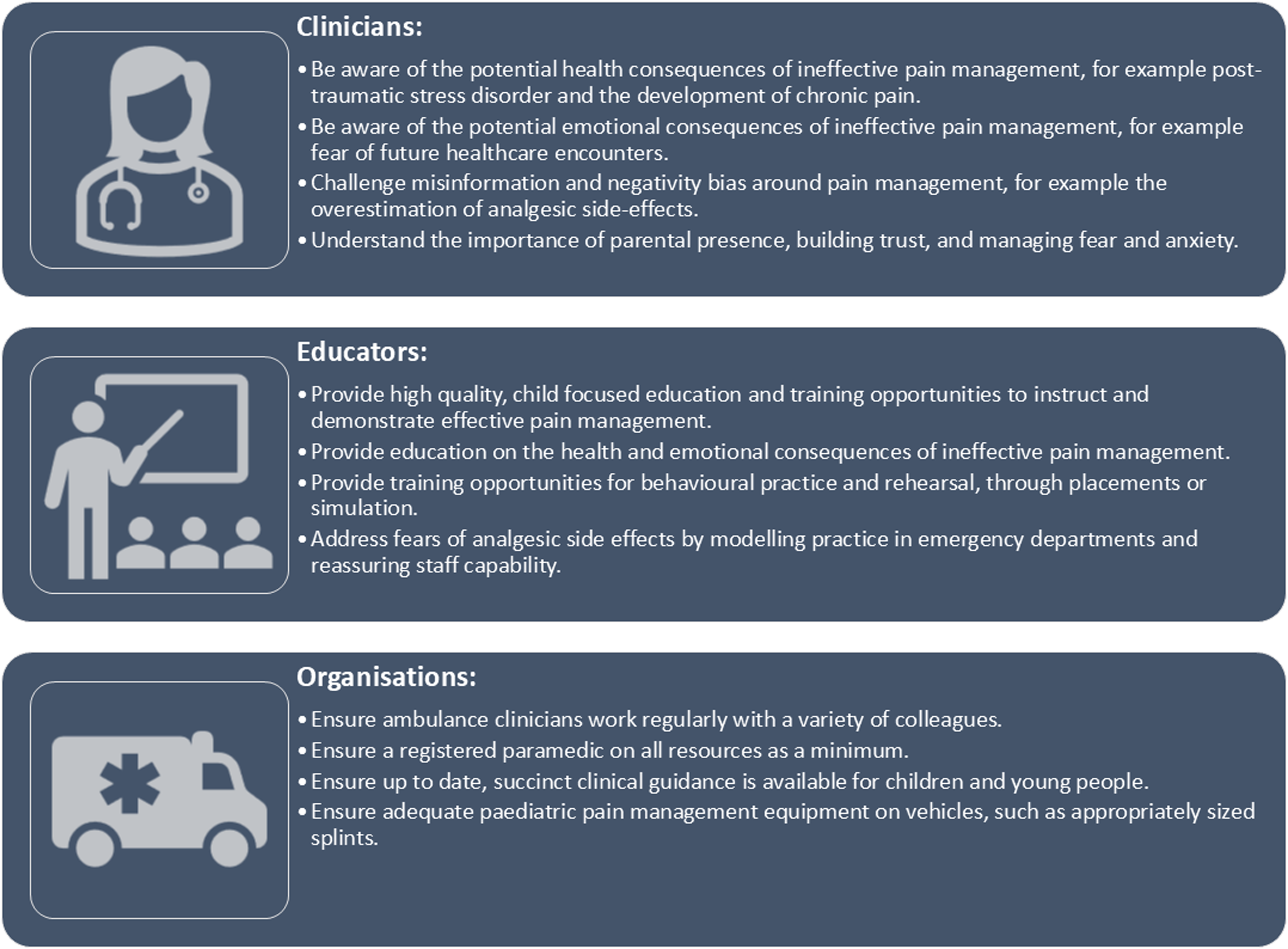
Model to improve acute pain management of children and young people attended by ambulance.
A review of pain management in children in the emergency department highlighted the important role of parents: they can provide comfort and calm their child enabling them to feel secure, or if they are over anxious they can have a negative impact on the child. 41 The review stressed the importance of a comprehensive pain treatment regime, including both pharmacological and non-pharmacological interventions. The review team also commented on the fear and anxiety a child may experience, explaining that distraction techniques are often more effective than verbal reasoning, particularly for younger children. 41 These findings map well to our programme theory, which also made similar claims.
Strengths and limitations
The focus of this review on the prehospital ambulance service setting is a key strength, considering the importance of context within realist research, and the unique setting. The diverse review team and stakeholder input was also a key strength, drawing on not only paramedic experience, but experience from the fields of psychology, general practice and nursing. This review has maintained transparency, a key component of realist reviews, by registering the review, publishing the protocol, and supplying a comprehensive supplementary file. Diligent coding within NVivo allowed all supporting excerpts to be coded to each respective CMOC, allowing us to produce a thorough codebook (see Supplementary File).
Due to time and resource constraints, we were not able to conduct any additional searches to pursue weaker parts of the programme theory, such as aspects around scene management and longer-term outcomes. We will address this by collecting data specific to these areas within the subsequent realist evaluation. Due to the relatively new field of realist research, and continuing rapid expansion of realist methods, there were some uncertainties around the rigour assessment – which appears to be a point of uncertainty among the realist and wider evidence synthesis community. We adopted the approach proposed by Dada et al. 31 but still found the process highly subjective – therefore we ensured this was conducted in duplicate, with a third reviewer assessing a 10% sample. There was little evidence regarding parent/carer and CYP expectations, therefore this area of the initial programme theory could not be tested or refined. We plan to address this gap in the upcoming realist evaluation. The pain assessment tools used on children and young people in the prehospital setting may have limitations in their validity, impacting the quantitative data synthesised in this review. There is no gold standard for assessing pain severity, therefore this will remain a limitation for some time.
Implications for policy, practice and research
We mapped the programme theory (Figure 5) to the Behaviour Change Wheel 42 and identified behaviour change techniques 43 that would facilitate change in clinical practice. While we are planning to undertake this operationalisation later in the PANDA study programme of research (see Figure 1), we felt it was important to provide clinically relevant insights at this early stage. The mapping process is described in more detail in the Supplementary File.
As part of the mapping process, we undertook a small group meeting (GN, GAW, SR, JH) to discuss the process and review a draft model tailored toward clinicians, educators, and organisations. This was reviewed by wider members of the realist review team, members of the Ambulance Clinician Advisory Group, the Young Persons Advisory Group, and the Healthier Aging Patient and Public Involvement group. The model was refined iteratively through several rounds of review (see Figure 6).
Recommendations for clinical practice include being aware of the potential health and emotional consequences of ineffective pain management (including post-traumatic stress disorder, the development of chronic pain, fear, anxiety, and negative impact on future healthcare encounters). This active awareness should help to raise the perceived priority of pain management. Clinicians should challenge misinformation and their own personal misconceptions through reflection and high-quality education. 44 Such misinformation may be around the overestimation of analgesic side-effects, the proper use of pain assessment tools, and the underestimation of pain severity in children. Parental presence (where possible), building trust, and managing fear and anxiety should be considered a high priority when managing CYP. 45
Ambulance clinician educators should provide high-quality focussed education and training opportunities on the topic of pain management in children and young people. 46 Such education should include information on the potential health and emotional consequences of ineffective pain management, with training opportunities provided for behavioural practice and rehearsal through placements, or simulation. Addressing fears of analgesic side-effects through education and modelling of other healthcare settings (such as paediatric emergency departments) should help to address the overestimation of analgesic effects that often prevents adequate analgesic dosing and administration. 47
Where possible, ambulance services should facilitate the crewing of staff members on a regular basis, as evidence from this review suggests regular crewmates provide optimal scene management. 48 Having a registered paramedic on all frontline vehicles should improve care due to their extended scope of practice and knowledge. 49 This requires long-term commitment to staff development, recruitment, training, and retention. Ensuring up to date and comprehensive clinical guidance on the topic of pain management in children and young people is essential for clinical staff to provide high-quality care, and ensuring an adequate range of paediatric equipment is available on vehicles, such as immobilisation equipment, safety harnesses, and monitoring equipment (such as oxygen probes and blood pressure cuffs).
Further research is needed to explore the experiences of children, young people, parents and carers, as their voices are missing from the published literature. The expectations of care, as developed in our initial programme theory (Figure 2), likely play a key role in the overall care experience and require urgent exploration.
The programme theory developed from this realist review will feed into the second stage of the PANDA study programme of research (see Figure 1) and will be further tested and refined within a realist evaluation. Gaps from the initial programme theory (around expectations) and final programme theory (around scene management, and CYP and parent/carer fear and anxiety) will be addressed within the realist evaluation. This will lead to a more robust, substantiated programme theory that will be operationalised into a complex behaviour change intervention within consensus workshops, and then tested within a feasibility study.
Conclusion
This realist review has laid a foundation on which future empirical testing can be conducted to improve prehospital acute pain management of children and young people attended by ambulance. It has also offered a clinically focussed model on which to effect change in practice, targeted to ambulance clinicians, educators, and ambulance service leaders.
Supplemental Material
sj-pdf-1-pam-10.1177_27536386251356690 - Supplemental material for A realist review of acute pain management in children and young people attended by ambulance
Supplemental material, sj-pdf-1-pam-10.1177_27536386251356690 for A realist review of acute pain management in children and young people attended by ambulance by Georgie Nicholls, Michael Baliousis, Tatiana Bujor, Georgette Eaton, Jessica Hodgson, Paul Leighton, Bill Lord, Marishona Ortega, Sarah Redsell, Aloysius Niroshan Siriwardena, Kacper Sumera and Gregory Adam Whitley in Paramedicine
Supplemental Material
sj-pdf-2-pam-10.1177_27536386251356690 - Supplemental material for A realist review of acute pain management in children and young people attended by ambulance
Supplemental material, sj-pdf-2-pam-10.1177_27536386251356690 for A realist review of acute pain management in children and young people attended by ambulance by Georgie Nicholls, Michael Baliousis, Tatiana Bujor, Georgette Eaton, Jessica Hodgson, Paul Leighton, Bill Lord, Marishona Ortega, Sarah Redsell, Aloysius Niroshan Siriwardena, Kacper Sumera and Gregory Adam Whitley in Paramedicine
Footnotes
Acknowledgements
We acknowledge the following individuals and groups for their contribution to the PANDA study: members of the Young Persons Advisory Group (YPAG), Queen Elizabeth's High School (QEHS), Gainsborough, for their active participation in the design and delivery of the PANDA study; Michael Betts (QEHS), Adrian O’Neill (QEHS) and Rick Eastham (QEHS) for setting up the YPAG group and for their ongoing support; members of the Healthier Ageing Patient and Public Involvement (HAPPI) group for their active participation in the design and delivery of the PANDA study; Martin Esposito (Scottish Ambulance Service), Ashley Scaife (University of Huddersfield), Emily Hoyles (South East Coast Ambulance Service NHS Trust) and Sharon Young (East Midlands Ambulance Service NHS Trust) for their roles as members of the PANDA study Ambulance Clinician Advisory Group; Tom Waterfield (Queen's University Belfast), Samina Ali (University of Alberta), Michael Smyth (University of Warwick), Alison Porter (Swansea University) and Amanda Brewster (University of Lincoln HAPPI Group) for their roles as independent members of the PANDA study steering committee; Gemma Squires (East Midlands Ambulance Service NHS Trust) and Robert Spaight (East Midlands Ambulance Service NHS Trust) for providing governance oversight as sponsor and expert advice. We acknowledge Despina Laparidou for involvement in the PANDA study realist review working group.
Data availability
All supporting data can be found in the supplementary file.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Georgette Eaton is a deputy editor at Paramedicine. She played no role in the editorial decision making process, which was conducted in adherence to the journal's peer review policy.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Gregory Adam Whitley, Advanced Clinical and Practitioner Academic Fellow [NIHR302875] is funded by Health Education England (HEE)/NIHR for this research project. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS or the UK Department of Health and Social Care.
Georgie Nicholls was funded by the Advanced Clinical and Practitioner Academic Fellowship [NIHR302875].
Tatiana Bujor received reimbursement for involvement in line with NIHR INVOLVE rates, funded by the Advanced Clinical and Practitioner Academic Fellowship [NIHR302875].
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.