
Abstract
Traditionally clinicians have been predominantly trained to examine and assess patients with a light skin tone, rather than patients of all skin tones. This bias in healthcare training could be contributing to the known health inequalities which are linked to a patient's ethnicity. Clinical assessment should automatically be inclusive of all skin tones to detect critically unwell patients early, but commonly used terminology suggests that paramedics may be trained to only look for paleness, reddening, mottling, pink or blue skin as areas of concern, rather than for skin changes that apply to all. Delays in identifying unwell patients risk the postponement of appropriate treatment, affecting patient long-term outcomes. To address this, paramedic education needs to advance forward using systematic key changes in the delivery of information, so that students can learn to assess patients in a manner that is habitually inclusive. The aim of this article is to spotlight these concerns, suggest modifications to clinical assessment and recommend changes to educational teaching philosophy.
Introduction
Health inequalities exist in relation to ethnicity1,2 and there is a growing awareness around the historic lack of inclusivity in healthcare education relating to a patient's skin tone.3–5 Whilst ethnicity does not necessarily determine skin tone, it is possible that health inequalities could be worsened if there is a lack of inclusive healthcare training to recognise life-threatening illness in all skin tones at an early stage. The recognition of a deteriorating patient is a key role of paramedics, and a delay in this identification will postpone critical interventions affecting patient outcomes poorly. This is an area for future change, since healthcare training is generally taught from the default perspective of a light skin tone,3–6 and it is probable that paramedic students are not always taught inclusive assessment skills. Using only one skin tone as a perspective to teach from creates the potential for unconscious bias in clinical assessment, and it introduces a lack of surety in managing patients of all skin tones. Healthcare professionals have lower levels of confidence in treating patients with dark skin tones, 7 and whilst the cause of health inequalities is complex (e.g. socio-economic factors, environment and deprivation 8 ) honing the education of healthcare professionals is an opportunity to ameliorate this. Our article aims to demonstrate the issues of unconscious clinical bias, and how it is furthered by standard clinical terminology. It offers recommendations on improvements within paramedic education, with the purpose of promoting an equitable inclusive clinical assessment approach when assessing patients of different skin tones. As a profession, our forthcoming practice could then impact positively on reducing health inequalities.
The unconscious bias of healthcare
Paramedic clinical education should already deliver information on the risk factors for certain ethnicities and different conditions, for example an increased risk of diabetes mellitus in patients from a South Asian group. 9 But, inclusivity is established in the nuances of the teaching delivery, as demonstrated in 2021 by Oozageer Gunowa et al. 10 Pressure injury teaching for nursing students across five sites in the United Kingdom was studied, finding ‘white normativity’ in lectures and ‘tokenism’. Of particular significance, the study commented on how ‘the failure of academics to meaningfully acknowledge differences in skin tone cascaded down to students, who largely failed to see or acknowledge the importance of these differences’. 10 The omission left students not discerning a need for inclusive clinical practice. Introducing slides at the end of a lecture to demonstrate how a medical condition presents in different skin tones could also be perceived as an afterthought, 10 and could perpetuate the unconscious (implicit) bias held by many health professionals around a patients race.11,12 A clinician may aim to counteract their personal bias, but the distractions that can occur within a time pressured, cognitively complex situation can overcome this objective, leading to categorisations such as stereotyping. 11 Assessment bias around skin tone may also partly stem from medical literature and textbooks, with resources tending toward pictures and wording to support assessing a patient of light skin tone.3–5 Added to this, skills and simulation training may have primarily included the use of manikins which are meant to represent white skin. 13 Together prioritisation (bias) of a light skin tone may affect decision making14,15 and worsen health inequalities 16 by creating variability in expertise and clinical confidence, depending on patient skin tone. Clinical confidence in assessing patients of dark skin tones has been found to be low, 7 but increased confidence can be developed by acquiring relevant clinical experience in practice. The level of confidence depends on the geographical area the clinician works within and the diversity of the patients encountered, but if a clinician generally only encounters one skin tone in their practice, it may lower their confidence in managing all skin tones further. 7 If confidence is underpinned by a person's self-perceived knowledge, 17 it indicates that day-to-day knowledge of inclusive assessment skills is insufficient due to inconsistencies in training. A quality improvement project in Michigan 18 highlighted the same issue, and successfully demonstrated that improving the assessment for all skin tones can be easily taught with a subsequent positive impact on patient care. And whilst complex dermatological conditions are not the first area of expertise for paramedics, being able to rapidly identify significant changes to the skin remains critically important. Consider life-threatening presentations involving rashes, changes to skin colour, inflammation, bruising, trauma and more, and how the skin tone of that patient may affect how rapidly a paramedic detects these findings. If – as demonstrated – a light skin tone perspective has been a pervading systematic approach in teaching and learning – then this ethnocentrism has historically existed in our approach to healthcare and will poorly affect patient care. 19
The current inequities in clinical assessment
Ethnocentrism develops from how we each see the world – our own lens – and we could assume (given the approaches and terminology in healthcare) that the term ‘global majority’ represents people of a light skin tone. But, ‘global majority’ was first used by Rosemary Campbell-Stephens in 2003, with the definition referring to ‘people who are Black, Asian, Brown, dual-heritage, indigenous to the global south, and or have been racialised as “ethnic minorities”’. 20 It emphasises how light skin perspectives have been prioritised and links into health inequalities which are well documented in relation to ethnicity. 21 In the United Kingdom the NHS Race and Health Observatory (RHO) was set up in April 2021 in response to the global narrative around racial discrimination in health. 22 The intersectionality within health inequalities makes it complex to attribute the issue to any one cause, 1 but the terminology used in healthcare could be a further strand within the wider concern of unconscious clinical bias. The issue is indicated in the RHO review 23 on using the tool APGAR 24 (activity, pulse, grimace, appearance, respiration) when assessing newborn infants. The tool uses ‘pink’ and ‘blue’ as terminology to describe the skin colour (appearance) of the newborn, but RHO state this approach is ‘limited and not fit-for-purpose’ for certain ethnicities. 23 They also identify that detecting cyanosis and jaundice in newborn babies commonly relies on techniques which relate to assessing infants of light skin tones, 23 rather than looking for skin changes that apply to all skin tones. Every newborn will have an unknown combination of melanin determining the infant's individual skin tone, but without clinical knowledge of how all skin tones present in hypoxia, there may be delays to treatment if the baby does not overtly present as ‘blue or pale’.
Another tool that uses terminology to describe the skin colour of a patient in acute deterioration is the ABCDE (airway, breathing, circulation, disability, exposure) assessment. It is a widely used approach, designed to identify a deteriorating patient to enable early clinical intervention. 25 Historically though, this systematic framework has included the use of terminology for examining patients of a light skin tone, and anecdotally, clinical practice is reflective of this. For example, terms such as pale, pink, blue, mottled or flushed are frequently applied, but a patient with a dark skin tone may not present in this way. The severity of mottled skin in septic shock can be scored to provide predictions around survival 26 but since mottling is not easily seen in dark skin tones it may not be identified, particularly if only a rapid assessment of the skin is undertaken. Assessing for specific skin changes, such as examining for pallor to the palmar creases (rather than a change in facial colour) maybe more useful in providing tangible evidence of patient deterioration. 27 Examining the fingers closely under good lighting (without fluorescence in the bulb to create a blue tinge) should support detecting peripheral cyanosis in all skin tones early,27–29 rather than unknowingly delaying interventions until central cyanosis appears. Relying on pulse oximetry to detect hypoxaemia is insufficient, as in the United States, concerns have previously been raised on the efficacy of pulse oximetry for all skin tones since 2020.30–32 By March 2024, an independent review set up by the UK government agreed that pulse oximeters ‘overestimate true oxygen levels’ in patients of a dark skin tone. 33 Literature suggests that pulse oximetry can overestimate to the extent of detecting readings of around 92% to 96% whilst simultaneously blood gases found readings of less than 88%. 32 Discrepancies of this nature occur for patients of all skin tones but are more profound and frequent in patients of a dark skin tone. 34 These inaccuracies are due to the melanin content of the skin, with a higher level affecting the near infra-red light which impacts accurate detection of blood oxygenation levels. 35 ‘Silent hypoxia’ (low pulse oximetry readings with no obvious breathing difficulties) were a feature of patients with the SARS-CoV-2 infection during the COVID-19 pandemic 36 so there was perhaps a reliance on pulse oximetry to aid clinical decision making. It would be impossible to know definitively if the unreliability of pulse oximetry impacted on patient outcomes, but it is known that certain ethnic groups – Black, Caribbean, Black African, Bangladeshi and Pakistani – had a higher mortality rate during the COVID-19 pandemic in England, up until January 2022.37,38 This trend in mortality relating to certain ethnic groups with dark skin tones was similar in the United States 39 and for Australia the highest rates of mortality (2021–2022) were documented for those born in the Middle East. 40 Multifaceted reasons behind these statistics are likely to exist, but the commonality suggests there is a need for change. Pulse oximetry is only one factor during patient assessment, but if other clinical signs are not easily observed then there may be reliance on the readings rather than considering the patient's overall picture.
How we can improve inclusivity in clinical assessment
The clinical decisions paramedics make in stressful situations are supported by experience and education, but the speed of these decisions can also cause unconscious stereotyping and discrimination. 41 For example, if prior learned habits create the expectation that a rash is easily seen, a clinician may only undertake a cursory assessment. But, rashes can be difficult to detect in a dark skin tone especially in incorrect lighting, so rashes, or inflammation, or bruising can be potentially overlooked. Consider a study by Sommers et al. in 2008 42 which examined women following consensual sex to explore if the women's skin tone affected the detection of injury. The participants were assessed by experienced forensic sexual assault examiners with findings suggesting that there were three times as many injuries found to the external genitalia in women with a light skin tone, than with a dark skin tone. The authors concluded that this was due to injuries not being detected by expert professionals, rather than a woman with a dark skin tone developing less injury. 42 It demonstrates how easy it might be to overlook skin injury, but also how healthcare myths develop that link to race, skin tone or ethnicity. Clinicians could begin to believe that certain ethnic groups do not bruise easily or do not feel pain in the same way as other groups. 43 It also demonstrates that a systematic inclusive approach to skin examination is needed so that life-threatening purpuric rashes, or hives in anaphylaxis are immediately found and properly assessed.
The Wounds International consensus document 28 produced in 2023 suggests that a good skin examination requires the right lighting – daylight preferably, or a non-fluorescent light if not – to look for all possible changes in skin colour as these may be subtle. Erythema is caused by an increased blood flow to an area, which would historically suggest a clinician examines the patient for reddened or pink skin. It is perhaps simpler to teach a student to examine the patient closely for any areas of darkened skin (whether red, pink, purple or maroon) which as a technique applies for all skin tones. Teaching students to always gently palpate the area to establish if there are unseen rashes, localised changes in skin temperature or subtle oedema will also lower the risk of missing changes to the skin too. Understanding that stretched skin can become shinier, and that moistening unbroken skin with tap water can help examination should be part of the learning too. Part of an ABCDE approach 25 is to expose a patient at E, and to examine their skin. If this is a superficial glance in poor light, the subtle inflammation to an infected area, the rash or the bruising might be missed without small significant changes to examination technique.
Recommendations
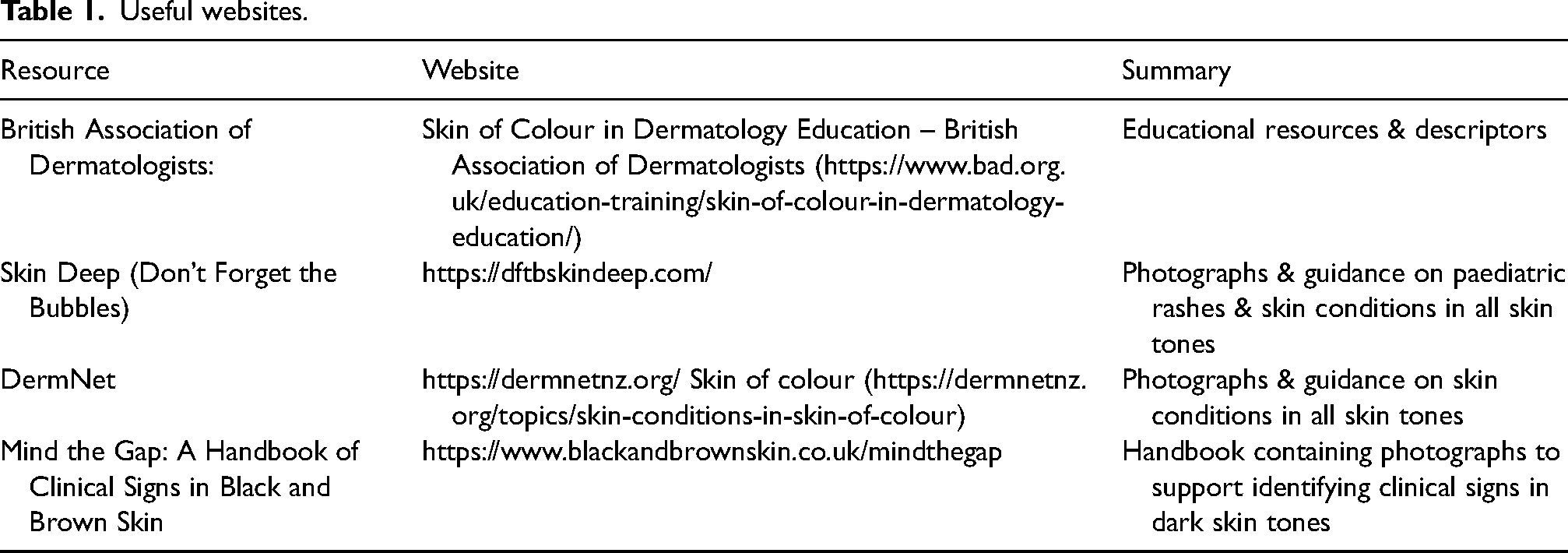
Higher education providers have a responsibility to teach contemporary clinical practice in line with the expectations of future employers, regulatory and professional bodies.44,45 To improve the inclusivity delivered in education, the teaching needs to weave equity considerations into sessions as an overall ethos, to avoid a system that only highlights inequalities as an additional consideration. For an enhanced ethos to translate into teaching, a university educational team could first review their teaching philosophy. The process requires examination of the common team pedagogical goals, how to achieve them in teaching practice and also in each educator exploring their own beliefs. 46 It will improve teaching quality for the student, and also increase the educator's confidence, motivation and competence due to the personal reflection required. 47 Consider how to avoid stereotypes and tokenism within teaching delivery; and instead promote self-criticality and acknowledge where there may be implicit bias in teaching. 48 The aim is to align the teams core teaching principles, but it can be challenging to address a subject such as skin tone. People may worry about causing offence 48 but without open teaching conversations health inequalities will continue. Schönwetter et al. 46 might be one model to consider using as part of a teaching teams philosophy re-valuation process as it integrates goals, practice and beliefs against another six criteria, such as the student-teacher relationship expectations. This model is not aimed at healthcare teaching specifically though, whereas Yeom, Miller and Delp 49 suggest an alternative simpler model with a four-step approach developed for nursing faculty. Simulation based education should seek to avoid the overuse of tired cliches and non-inclusive terminology (e.g. ‘a white, overweight 50-year-old male, who is pale with crushing chest pain’) and offer a range of patient presentations which would all fit (in this example) under a possible acute coronary syndrome event. The increasing availability of a range of medical manikins (e.g. https://simbodies.com/) should support diverse scenarios without stereotyping in relation to a patient's fictional name, gender, clothing, environment or skin tone. Challenging myths, discussing risk factors relating to ethnicity or skin tone, and altering clinical terminology will support inclusivity, but changes to frontline practice may take time as habits in examination skills can be challenging to alter. 50 The COM-B model looks at methods to influence embedded Behaviours, citing Capability, Opportunity and Motivation as the three underpinning pillars. 50 Students could boost transformation as they would have the capability (knowledge) and opportunity (in clinical placement) to inspire motivation, and alter clinical behaviours in practice. But, a barrier consisting of the theory–practice gap51,52 creates a challenge for students to innovate change without the support of inclusive clinical guideline updates, such as those already demonstrated within the UK's Joint Royal Colleges Ambulance Liaison Committee 53 (JRCALC). Raising awareness of website resources such as those seen in Table 1 may be helpful, but clinical guidelines can provide the robust evidence-based source to propel forward inclusive practice for all clinical educators.
Useful websites.
We have the opportunity to enhance patient care by educating paramedic students to take an inclusive approach to clinical assessment as standard. Systematic changes to terminology and teaching approach can be made after aligning a core teaching philosophy, in order to improve the confidence of students (and thus clinicians) when managing patients of all skin tones. If we reflect that a paramedics role is traditionally set in the environment of pre-hospital emergency care, then the early identification of deteriorating critically unwell patients is absolutely at the core of what we do. We should be experts in this area.
Summary
Ethnocentrism from a light skin perspective has dominated healthcare. Applying equity in all clinical examinations should already be the norm, but unfortunately the evidence suggests that the knowledge to undertake this is not yet universally in place. Altering a teaching philosophy to train students to take an inclusive approach as standard and to be aware of the limitations of pulse oximetry, the misdirection of commonly used terminology and the risks of only undertaking a cursory examination of the skin is important for change. Health inequalities are multi-layered with many areas contributing, but one straightforward future improvement is in promoting equity within clinical assessments and making this standard.
Footnotes
Acknowledgements
The author would like to thank Joseph Copson and Hafsa Mahumud.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.