
Abstract
Conveyance decision-making is a critical area for research given the potential patient safety and health system efficiency implications. It is understood that numerous factors can impact clinical decision-making such as organisational policy and procedure, scene safety, and patient assessment, along with considerable changes to paramedic education in recent decades. Using constructivist grounded theory methodology, semi-structured interviews and an online asynchronous focus group were employed for data collection. Both data collection and data analysis occurred concurrently, guided by the principles of constant comparative analysis. Three main themes were constructed: fearing and mitigating the repercussions of a potential patient complaint, the evolving professionalisation and expectations of paramedics, and feeling constrained by the organisation and its culture. These themes contributed to the construction of the theoretical framework. The theoretical framework titled The Tensions between Organisational Culture and Professionalisation details how paramedics make conveyance decisions by navigating the tensions between fears of individual blame posed by existing organisational culture and the evolving professionalisation of paramedics. Paramedics were found likely to forego responsibility for making alternative or non-conveyance decisions when working in a culture of blame, resulting in transporting patients to an emergency department when this may not be clinically required. When working in an organisation with an existing blame culture, paramedics forgo clinical decision-making. Paramedics must be educated and supported to make quality, patient-focused conveyance decisions. The theoretical framework explains how paramedics navigate conveyance decisions.
Introduction
Emergency ambulance services in Australia are the responsibility of one agency in each of the states and territories. Traditionally, when an ambulance responds to an emergency call, the patient is transported to an emergency department (ED). However, in the 2022–2023 reporting period, 15.3% of patients were treated but not transported across all emergency ambulance jurisdictions. 1 It is understood that often patients and their next-of-kin prefer to avoid hospital and strongly desire alternative care options, 2 and there is potential for patient adverse events from ED presentations such as hospital-acquired injury, infection, or delirium.3,4 Moreover, to enable timely and appropriate ambulance response, many ambulance services considered adaptive models of care, such as introducing telehealth and the development of alternative care pathways. 5
In the past two decades, paramedicine in Australia has shifted from a post-employment education pathway to a pre-employment tertiary education model, shifting the need for paramedics to be degree prepared to be employed in most jurisdictional ambulance services. 6 Driven by this significant development in education and increasing skill set of paramedics, which in turn increased the risk to patient safety, 7 in 2018 Paramedics became the 18th health profession to be regulated by the Australian Health Practitioners Regulatory Agency (Aphra). 8 Considering the changes to paramedic education preparation and changes to ambulance service delivery models, associated with increasing demand for health services, it may no longer be appropriate to transport all patients to ED, and paramedics now need to make clinical decisions about appropriate conveyance and care options.
It is understood that paramedic clinical decisions can be influenced by varying factors, including patient clinical assessment, cognitive capacity, patient and carer wishes, access to reliable patient information, and scene safety.9–12 It is also understood that the paramedics own internal influences impact their decision-making, such as role perception and the their perceived value of the patient presentation.13,14 However, it has also been identified that organisational factors contribute to decision-making including, perceived low levels of trust in ambulance services also influence paramedic conveyance decision-making. Further, key performance indicators based on time intervals,13,15,16 organisational protocols, policies and procedures, and guidelines influence decision-making.10,12,16–18 While paramedics may be required to make conveyance decisions, the accuracy and safety of conveyance decisions made by paramedics remains to be inconsistent.19–22 Currently, there is a paucity of evidence understanding how the paramedics in Australia make conveyance decisions, 23 and it is therefore important to understand how Australian paramedics make conveyance decisions. Conveyance decision-making is a critical area for research given the potential patient safety and health system efficiency implications. This paper aims to provide clinicians, policy writers and education providers a theoretical framework to answer the research question: how do paramedics navigate conveyance decisions? The resultant theoretical framework contributes to understanding professionalisation of paramedics this substantive area.
Methodology
Constructivist grounded theory methodology is well suited to areas that are largely unexplained, 24 as it provides flexible yet rigorous qualitative methods that enable the construction of a theoretical framework from the data to explain the phenomenon 24 which in this research is conveyance decision-making, rather than providing a descriptive account of the data. Constructivist grounded theory developed by Charmaz, considered the third development of grounded theory methodology, applies ontological relativism and epistemological subjectivism. 24 The researcher is acknowledged as a co-contributor to data collection, unable to separate their knowledge and past experiences during data collection. 25 When choosing an approach to grounded theory, Rieger suggested researchers’ philosophical beliefs should influence the choice of the grounded theory methodological iteration along with the pragmatic considerations of applying the methods. 26 Constructivist grounded theory places the researcher within the research, and acknowledges that the themes to be constructed between the participant and the researcher cannot be separated from the context in which the data is situated. 25 The researchers’ felt these considersations were important considering as the worldview of the primary researcher (AM), identifying as female, has been influenced by the completion of an undergraduate paramedicine degree, 16 years spent as an operational paramedic working for a jurisdictional ambulance service and 8 years as an academic within a bachelor of paramedic science programme. This constructivist approach strengthened the overall research through a priori identification of potential influences of the researcher and analysis and reflexivity at front of mind during concurrent data collection and analysis methods. To enable reflexivity the researcher maintained a reflective record of their collection, interpretation, and coding of the data and the influences that their prior experience, attitudes, and beliefs may have to ensure that the data was collected and analysed in a way that captured and respected the subjectivity of the participants’ accounts. This process acknowledged the undeniable influence of the researcher's interpretations. The lead researcher's previous experience contributed to theoretical sensitivity, the ability to identify and extract relevant data for the theoretical framework.
Setting
Australia is serviced nationally by jurisdictional ambulance services, which provide either fee-for-service or government-funded services. The jurisdictional service, which is the context for this research, is government-funded and responds to 1.2 million incidents annually. 1 The state in which it operates is geographically vast, with an area of 1,723,030 km2 (665,270 square miles), with half of the population residing in the greater metropolitan area of the capital city. 27 Paramedics employed by the ambulance service are a mixture of post-employment diploma trained and pre-employment degree trained. Paramedics in this service operate within organisational clinical practice guidelines with varying scopes of practice. However, all paramedics operate within the same conveyance decision guideline.
Participants and recruitment
Recruitment for this study was purposive, as commonly used in grounded theory, identification of participants who could contribute to unsaturated areas of the data, facilitating data collection and analysis.
14
The inclusion criteria for participants in this research were:
Registration with the Australian Health Practitioner Regulation Agency to practice as a paramedic in Australia; Current employment in a role providing emergency care and transport of people in the community; and Employment based in the jurisdiction of where this study took place.
It was important to the research that participants were paramedics actively engaged in the direct provision of emergency care to ensure an accurate understanding of current practices. The third criterion was important to ensure data were appropriate for aggregation as each Australian jurisdictional ambulance service operates within its own legislative obligations and determines its own clinical scopes of practice and operational procedures.
Following ethical approval, the Australia and New Zealand College of Paramedicine (now the Australasian College of Paramedicine), agreed to email all members from the included state of Australia on one occasion, providing them with the research advertisement and research participation information sheet. To enhance the visibility of the study to paramedics who may not be members of the professional association, social media was also used for recruitment. A social media advertisement was posted to the primary researcher's personal Facebook, Instagram, and LinkedIn sites on the 28th March 2019. A paid advertisement was created on Facebook, for inclusion in Facebook user's feeds for those who met the specified selection metrics. The advertisement included information about the aim of the research and invited participation in the research study. Ethical approval was granted by the University of the Sunshine Coast Human Research Ethics Committee (S191288).
Data collection methods
Data was collected between April and July 2019, through a combination of telephone, asynchronous online, and face-to-face data collection methods which were scheduled at mutually convenient times and locations with only the participant and primary researcher present. All participants were provided with the opportunity to select their preference for interview or focus group participation at the time of consent. As there was limited interest in focus group participation, only one focus group was conducted, which occurred in the middle of data collection as depicted in Figure 1. Interviews lasted between 29 and 63 minutes with the average interview duration of 43 minutes. No participants withdrew from the research.
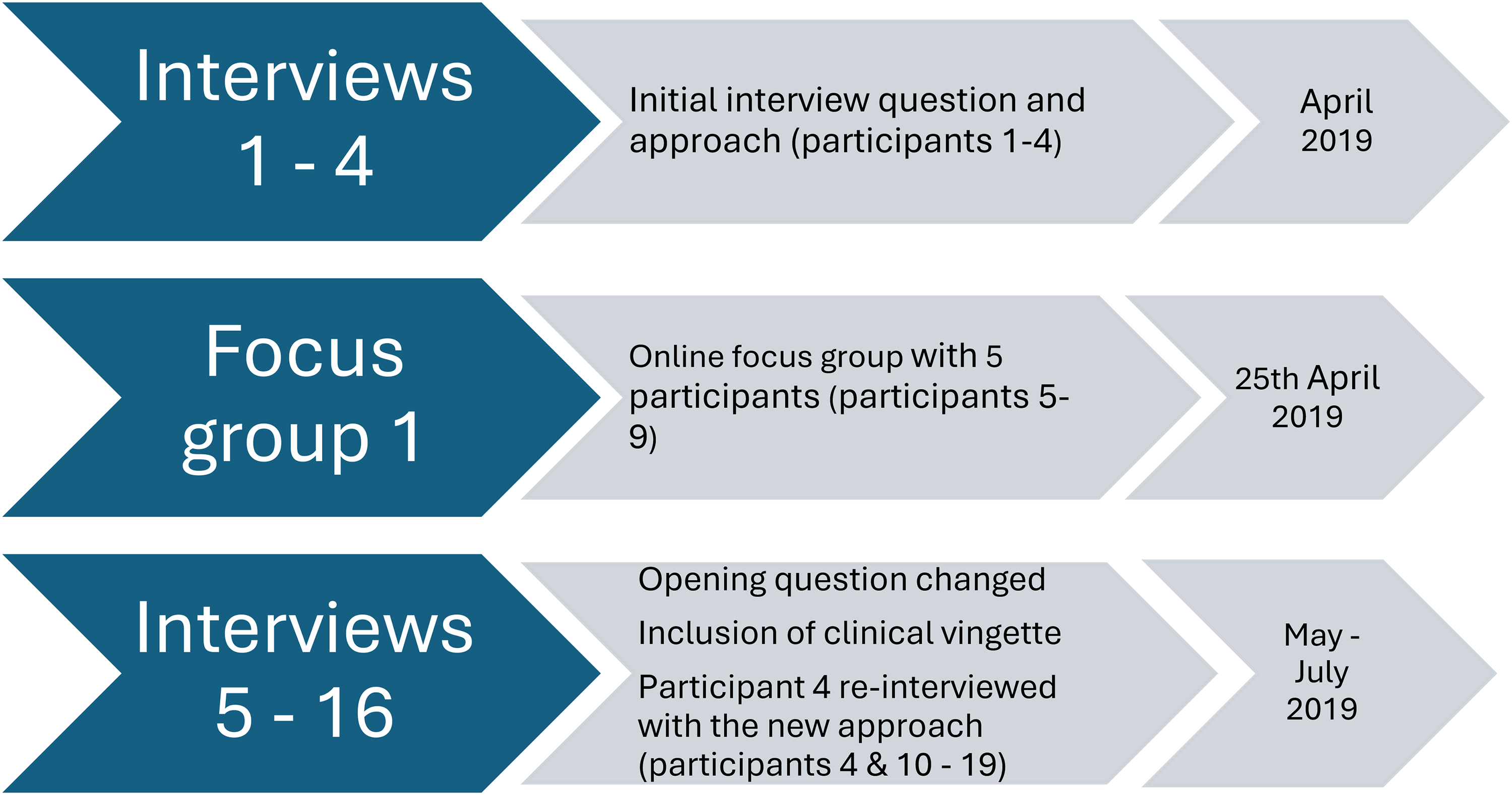
Depiction of data collection approach and timeline.
Semi-structured interview questions were developed that focused on the topic of the research yet were flexible to allow further exploration of ideas and issues as they emerged. To increase the rigour of the research methods, a mock interview was conducted with one co-researcher to confirm the appropriateness of the interview questions and telephone interviewing skills. The initial opening question posed to participants was Can you describe an instance when you attended to a patient and as the treating paramedic you decided not to transport the patient to a healthcare facility? However, in early interviews, this question only elicited superficial data and responses that overtly referenced ambulance service clinical practice guidelines. To provide an opportunity to access more experiential data from participants, the opening interview question was changed to: Can you describe a case where you transported a patient when your gut told you that they could have stayed at home? and a clinical vignette was included as a focus for discussion to extend the discussion into unexplored areas of the data.
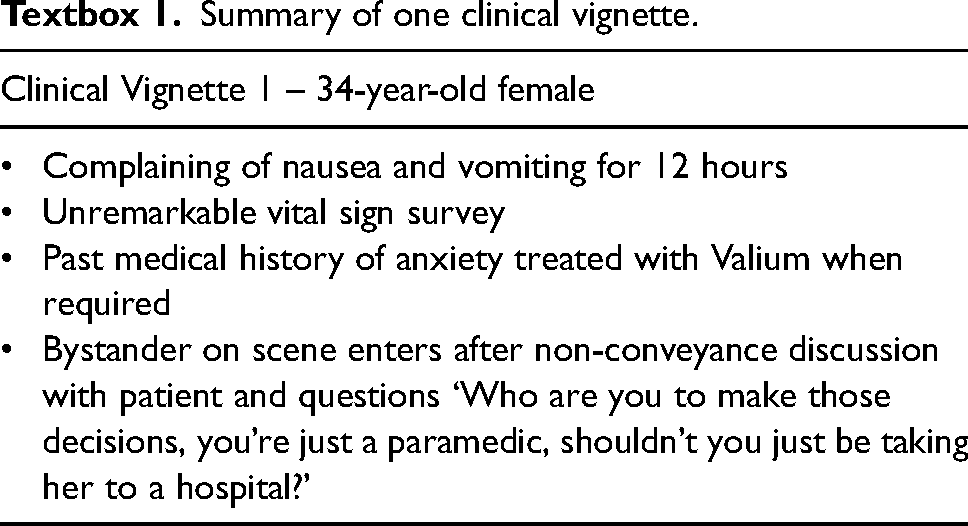
Vignettes have proven useful in health and decision-making research as they allow the participant to comment from a less threatening perspective which may allow the researcher to better examine participants’ perceptions, beliefs, and attitudes. 28 Four clinical vignettes were developed in line with the 15 recommendations from Evans and colleagues 29 and informed by early data analysis. This allowed the researcher to choose a vignette with a clinical and/or psychosocial presentation that had different characteristics to those the participants had discussed in response to the initial interview questions (Textbox 1). By changing the opening interview question and providing a clinical vignette to the participants, richer data was elicited, which contributed to theoretical saturation of the codes, categories, and developing framework. Final interview questions were available in Supplemental Material 1.
Summary of one clinical vignette.
All interviews were digitally recorded and transcribed verbatim by a transcription service, allowing the primary researcher to return to the data and undertake concurrent analysis after each interview. The primary researcher listened back to audio recordings, to cross-check the accuracy of the transcriptions, and become immersed in the data. Computer software NVivo 10 was employed to manage the data.
Data analysis
A detailed description of the analysis process is reported in Morrison, 2023 and a summary is provided here. In line with the tenets of constructive grounded theory methodology, a constant comparative method was used to analyse the data. Throughout this process, data collection and analysis occurred concurrently, allowing the researchers to move back and forth between data collection and the developing analysis. 30 In this study, initial coding commenced with line-by-line coding using gerunds, verbs acting as nouns that describe the active process that is happening, and where possible, maintaining the participants’ own language in the code. At this early stage, creating memos of developing analytical ideas and constructs occurred, integral to constant comparative analysis. 25 The researcher recorded ideas, assumptions, and curious elements within the data. As data analysis progressed to focused coding, the researcher analysed and synthesised the significance of initial codes and the connections between codes. This enabled the researcher to make conceptual leaps in the analysis, leading to the creation of categories. Memoing at this stage assisted moving from inductive analysis to an abductive approach to assist in explaining surprising and unexpected findings from the earlier stages of data collection and developing analysis. During this later stage of data analysis, purposive sampling transitioned to theoretical sampling, central to grounded theory which allows the researcher to explore categories from various angles and to clarify any unexplained areas of the data. Throughout the analysis period, the researcher returned to the data at every stage to test that the developing codes were grounded in the data, and ensure the data was representative of them through the development.
As data analysis progressed, focussed coding transitioned to theoretical coding where the relationships between codes and categories were synthesised and integrated into a theory. 31 For this research, theoretical coding occurred as the theoretical framework was being developed and allowed for the confirmation of ‘fit’ of the framework 32 and ensure the analysis had not been forced. In this research, data collection continued until data no longer contributed new information to the developing categories, the researcher had tested the theoretical framework against new data and no new data was identified, this is known as theoretical saturation. 31
Reflexivity
The researchers’ role and familiarity with the participants may influence the representations of the participants’ experiences expressed through their narratives, a recognised limitation of constructivist grounded theory. 33 This influence is acknowledged but is also consistent with the form of Grounded Theory used that recognises that the researcher and the participants often occupy the same domain and hence can be mutually influencing. The process of reflexivity helps to acknowledge that participants who are known to the researcher may provide responses to questions that they feel are wanted, resulting in both participant influence on the researcher and researcher influence on participants. Reflexivity through memoing was used to acknowledge rather than eliminate these influences. To ensure the transparency and trustworthiness of this research the researcher created an extensive audit trail using memoing, as described above. The lead researcher recorded any preconceived ideas and thoughts before data collection commenced, and during data analysis, the researcher returned to these memos to ensure previous knowledge and opinion was not forcing data. 23 Through ongoing memoing and discussions with co-researchers, any subjectivity of the data analysis was challenged ensuring transparency of the data. This was demonstrated by another researcher from the team (BL) reviewing three transcripts, reflecting on the coding together to ensure the data was not forced. Further, one participant was interviewed twice to test the opening interview question and the clinical vignette(s) to substantiate developing findings. This aligns with grounded theory tenets which prompt the researcher to return to participants should they need to follow up lines of enquiry and supports both reflexivity and rigour in the process. 25 The findings at the later stages of development were shared with several participants who reported that the findings resonated with them.
Findings
Sixteen individual interviews (one participant was interviewed twice) and one online focus group with five participants were completed; 10 participants were known to the researcher through a professional context. The construction of the core category ‘constraining’, the most significant code determined through data collection, encapsulated how the categories integrated into the theoretical framework the tensions of organisational culture and professionalisation. The framework was constructed using three themes: fear and mitigating the repercussions of a potential patient complaint, the evolving professionalisation and expectations of paramedics, and feeling constrained by the employing organisation and its culture.
The theoretical framework illustrates how the organisational culture of blame culture contradicts the evolving professionalisation of paramedicine, and this contradiction is causing tension for paramedics. The tension experienced by paramedics is illustrated in Figure 2 with the red circular highlight on the green road, reflecting the constraints on paramedic professionalisation as the profession progresses along the professionalisation continuum. The framework highlights that the organisational culture of blame attempts to minimise or remove discretionary behaviours using policies and procedures and constraining autonomous decision-making of paramedics. Further, the organisational culture that has led to fear and mitigation of potential patient complaints has constrained the developing professionalisation of paramedics. This misalignment between professionalisation and organisational culture confuses role perceptions for paramedics and impacts conveyance decisions.
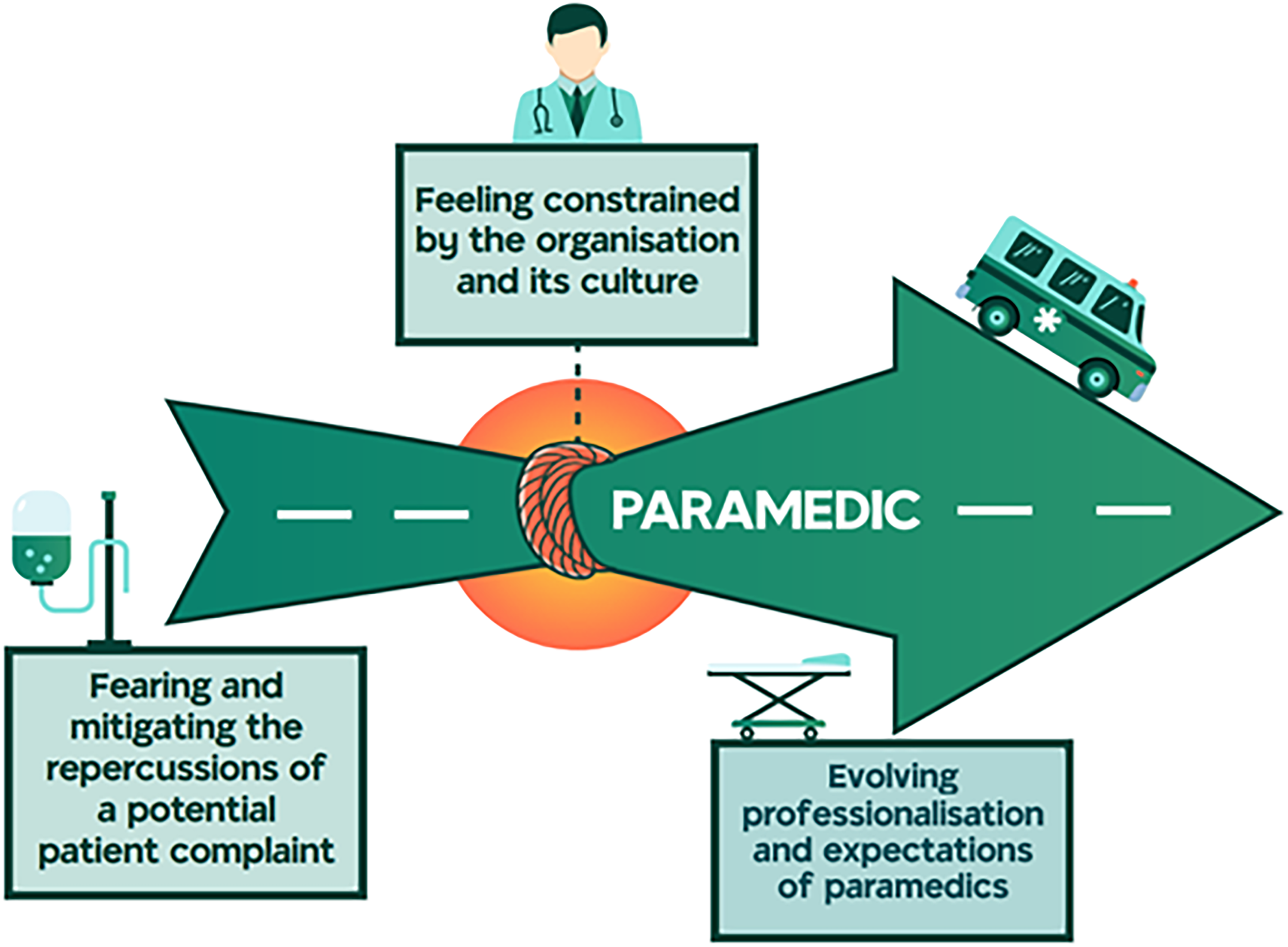
Theoretical framework – the tensions of organisational culture and professionalisation.
The core category ‘constraining’ was identified in each theme, constraining paramedics’ abilities to apply their knowledge and skills to clinical practice and make conveyance decisions.
Fearing and mitigating the repercussions of a potential patient complaint
The first theme, fearing and mitigating the repercussions of a potential patient complaint details a sense of fear driving paramedic conveyance decision-making. This theme was constructed from four contributing categories including, organisational management of a compliant, fearing the impact of a complaint on professional registration, deferring to the ED in the absence of clarity, and mitigating the repercussions of the patient complaint. This theme was very emotive for participants who articulated fear of the organisational complaint management process, should a patient complain after being discharged at the scene. Many participants described transporting patients to an ED in the absence of a clinical need to obviate a potential complaint. It's not worth the potential complaint. Let's just shove them in there [the ambulance] and let's go. So, I don’t even enter into the idea of leaving people at home without really making sure that this is not going to come back and bite me in any shape or form. (P2)
Participants stated that the organisation took a punitive approach to complaint management which drove them to avoid decision-making entirely. If whatever decision you’ve made has had even a remotely negative outcome, that's it; it almost feels like you’re being raked over the coals. So, once bitten, twice shy in that regard. It's just easier not to have to deal with that. (P10)
The category fearing the impact of a complaint on their professional registration detailed how participants expressed feeling solely accountable for any adverse patient outcome resulting from a patient encounter, concerned that if a patient suffered an adverse outcome, it could result in the loss of their professional registration and loss of employment. Well, primarily loss of registration. If there is a bad outcome and if I was found to be at fault for the patient's bad outcome, then I’d be afraid of losing my job. (P7)
Notably, in this research, a negative outcome was only considered possible with a patient who had not been transported to an ED and when a complaint had been received from either the patient or a person known to the patient.
The combined fear of organisational complaint management, and fear of loss of professional registration, contributed to the category deferring to the ED in the absence of certainty. This category revealed that participants would assess the level of certainty of the patient's presentation and the reliability of the presenting information such as past medical history. When any doubt was cast over the reliability of the information, or patient outcome, then the patient was transported to an ED. Revealing that lack of certainty contributed to paramedics deferring decision-making to another clinician. If someone is unwilling or if I can’t extract the relevant information in the timeframe I have on scene, I’ll be more likely to not necessarily pass it [the patient] on to someone else [another health clinician] but take them to an appropriate hospital where they can have an assessment by a doctor. (P1)
When paramedics faced these uncertainties and deferred patients to the ED, this action assisted in the mitigation of risk for the paramedic, leading to the category mitigating the repercussions of the patient complaint. The data identified several ways in which paramedics mitigated their risk and the repercussions of a potential patient compliant, for example ensuring that the patient had a trustworthy adult remaining with the patient, ensuring that the patient would call for an ambulance should their condition change, or they become concerned or worried and, some paramedics organising follow-up care on behalf of the patient. I think it takes away that risk, or it adds to leaving them at home, but you know that they’re going to get that follow-up care. It's not like, ah, go – tell them to go to the GP and hope for the best. You know that they’re going to get that follow-up and education. (P7)
The evolving professionalisation and expectations of paramedics
The second contributing theme was the evolving professionalisation and expectations of a paramedic, constructed by three categories, namely the evolving knowledge and professional scope of the paramedic, professional recognition for psychosocial patient assessments and the growing needs, and expectations of the community. The data contributing to this theme details that participants felt that a paramedic's professional knowledge and scope of practice has changed rapidly in recent years and that their preparatory education did not provide them with the knowledge they subsequently required. It was evident that transporting patients to a hospital had been ingrained in paramedics, during their preparatory and employer-delivered education, and that they had little, if any, training in assessing, triaging, and referring patients to alternate healthcare providers. Participants expressed a desire to be trained in safe scene discharge and referral pathways. I think it's just the expectation that we go to the hospital. We've never been taught; I know when I was going through the Diploma we were never told to go to a GP [general practitioner]. I think it's an education thing. I think people need to be educated … to thinking outside the box so you don't have to go to the hospital, could this person be referred to [other services]. (P12)
Contrary to this, changes in the nature of patient presentations which have occurred over time were reported as an excellent opportunity to redirect some training to include specific psychosocial assessment and patient safety training to enhance the paramedic management and referral pathways for the benefit of the community. That social aspect really does provide a perfect opportunity for paramedics to improve our scope of practice, and, to me, it is the future, to need to have that caring approach and looking at holistically, what we do. (P15)
Overwhelmingly, the data revealed that paramedics believed transportation to an ED was the safest option for the patient. In addition, participants felt they didn’t have sufficient training to safely make decisions regarding alternate patient disposition when patients presented with a low acuity complaint. I think most patients, I would always say that, you know, obviously, the safest approach is to go to the hospital or to seek further medical care because we don't have enough experience or ability to be able to assess a patient over a period of time, to be 100 per cent certain of any diagnosis, or be 100 per cent certain that they're going to be fine from hereon in. (P4)
If the paramedic anticipated that the patient would likely call for an ambulance later for the same complaint, then the paramedic would transport regardless of whether the patient's clinical condition needed to be assessed at an ED. This was explained by participants as necessary as it was believed that the jurisdictional ambulance service required any patient who called an ambulance a second time were transported to an ED regardless of clinical complaint. Because once she's been left behind by the ambulance once, you automatically win a trip to hospital, essentially, regardless of your clinical decision-making. (P10)
Through professional knowledge, paramedics have identified the requirement to be able to assess patients who may not appear to be acutely unwell. This resulted in paramedics conducting a psychosocial assessment in addition to the initial clinical assessment of the patient which built the category the professional recognition for psychosocial patient assessment.
Once participants were satisfied that the patient didn’t require transport to the ED for their clinical presentation, paramedics would address the patient's vulnerability status by assessing the patient's capacity for self-care, the safety of their living environment, and their access to alternate modes of healthcare. This assessment contributed to the paramedic's conveyance decision. If paramedics were not assured that the patient had sufficient skills, a safe environment, and available support, they would not consider discharging the patient at the scene, even in the absence of the clinical need for transport. Somebody who I think isn't even able to manage their bare day-to-day living, then they're not going to be in a good position to manage their illness, so I think they need help in terms of managing this current crisis. I would also hope that it would get them in contact with the services that will manage their discharge [allied health and social support services often only accessible in or through hospitals]. (P13)
In conjunction with assessing the scene safety and patient's capacity to self-care, participants assessed the availability of support networks to which patients had access. Support networks included family and friends, community networks, and allied health supports who would provide care services in the home. I think their social situation as to how much support they have in terms of family either with them, or the access to their family, or access to community support. (P8)
The patient's capacity to access alternate healthcare options such as General Practitioners, allied health, and other hospital services was also assessed by paramedics before deciding to transport the patient or discharge at the scene. If participants could not facilitate sufficient support in the patient's living environment, they would defer to transporting the patient to an ED.
The accessibility of alternate healthcare options proved to be a defining element in paramedic conveyance decision-making, however, participants often faced barriers such as limited alternate care pathways available or restricted opening hours and costs. This resulted in participants transporting patients to an ED irrespective of the appropriateness of the ED presentation. …especially after hours, there's no option but to take them to the hospital. So, the gut feeling might be this person doesn’t need to be in hospital, but I have no other option because I don’t feel - I know they need to see somebody, but the hospital is the only option at this point in time. (P8)
The last category constructing the theme is the growing needs and expectations of the community. Participants identified they navigate the expectations of the patients, others on the scene, their employer, and the receiving facility. Many participants explained the challenges inherent in managing the expectations of those on the scene, with the reality of the healthcare system and the role of the paramedic. When patients called an ambulance for certainty on a diagnosis, participant paramedics felt they were underqualified to provide and not resourced to do so. Therefore, the only option to provide certainty was through transport to definitive care. ‘We can't give you any specific answers’. A lot of the time, that would lead to a patient going ‘oh well I think maybe go up to hospital then’. (P4)
On arrival at the ED, paramedics explained that often they had to justify and defend transporting subacute patients to the triage nurse, who questioned the arrival of patients. It does become quite difficult. You feel like you've got to justify to the hospital staff, go, ‘look I'm so sorry but literally, look at it from my point of view. I can't do anything either’. (P9)
Paramedics communicated that they often waived their clinical decision-making during a patient encounter to oblige the patient's expectations or requests. She'd already organised someone to come look after the kids that was there, so from my point of view the decision was made by the patient before we even arrived, that they needed to go to the hospital, and my feeling is, if they're insisting on going to the hospital, we're not really in a position to refuse, even if their vital signs are normal. (P4)
Participants defended this practice as they didn’t feel they had the authority to refuse transport if a patient requested it, going as far to say that access to healthcare is a basic human right. Patients have a right to make decisions about their own care and if they want to go to hospital, then who am I to tell them that they can't? They have a right to healthcare, and I know that the broader government would agree with that. So, from my point of view, if they're dead set on going to hospital, I'm certainly not going to tell them they can't. (P4)
Feeling constrained by the organisation and its culture
The final theme, feeling constrained by the organisation and its culture, details how organisational policy and procedure define numerous elements of the paramedics’ role. Two categories constructed this theme, the influence of organisational policy and procedure and interpreting unwritten expectations of the employing organisation. This theme highlights the influence of organisational policy and procedure demonstrating how such directions remove paramedic clinical decision-making. Participants also reflected on a political commitment of ensuring all residents have access to free ambulance services. State government move to say that if you want an ambulance, you will get one and they will take you to hospital and it's all for nothing. (P10)
Participants explained that organisational policy or documents such as circulars or newsletters were perceived by paramedics as clinical directives overriding autonomous decision-making. There are policies there and procedures we must follow, and I will do that to the letter every time. The only time I’ll ever go outside my scope of practice is usually via the doctor consult. (P15)
Further, participants stated that the organisation's clinical guidelines pertaining to non-transport may remove the paramedics’ capacity to make conveyance decisions from their scope of practice. Pretty much our guidelines now is [sic] if someone calls an ambulance, that's enough reason to transport. (P2)
Finally, should the paramedic wish to deviate from the perceived directive they would need to seek permission before making an alternative decision. By not following that policy, if something was to happen, the issues with - I would say that the repercussions of that would be amplified because essentially, they could refer to a direct policy which covers what you’ve done and you’ve gone against that, and that's - if that results in a poor outcome, well I’d say that would be viewed very dimly. (P4)
The second category to construct the theme, interpreting the unwritten expectations of the employing organisation, identified various undocumented expectations of paramedics. Specifically, participants identified that during individual performance appraisals, non-conveyance rates would be raised with paramedics. When you go to do your performance appraisal and that, the stats do get brought up. ‘Oh, you’ve done an awful lot of non-transports, are you sure that's a good idea?’ You do get questioned on that. (P9)
It was evident that overall, regardless of there being no policy or written instruction in place, paramedics felt the employer expected paramedics to transport all patients to an ED. Without a doubt, if there was support for leaving people at home, or there were more rigorous alternative pathways that we could access, [I] definitely wouldn’t be transporting people to emergency departments if I didn’t feel that they needed to. (P10)
Discussion
The findings provide an understanding of how paramedics navigate conveyance decision-making, through the theoretical framework, the tensions of organisational culture and professionalisation. This framework has been constructed from three themes, fearing and mitigating the repercussions of a potential patient complaint, the evolving professionalisation and expectations of paramedics, and feeling constrained by the employing organisation and its culture.
There was no discussion surrounding any risk in instances of a negative outcome or complaint from a patient unnecessarily transported to an ED. This narrow view of the sequelae of patient care may indicate factors, such as a lack of education about the risks associated with unnecessary transport to an ED. Further, paramedics felt that transporting a patient to an ED negated the paramedic's accountability for patient outcomes. 15 This is surprising as there is an abundance of research identifying risks to patients unnecessarily presenting to ED.16,34,35 These risks are particularly prominent for older adults and vulnerable populations, including increased mortality, delays in receiving care, adverse events, increased intervention rates, and increase in delirium and healthcare costs.16,34,35 Despite the evidence surrounding the risks of transport to an ED, few participants acknowledged these risks. When patients are transported to an ED in the absence of the clinical need, this may limit the accountability of the paramedic, impact hospital ramping, delay in assessment times, and place undue strain on the ED. 36
In this research paramedics feared the organisational complaint management process, which was identified as punitive. The reported experience can be equated to individual blame logic, commonly seen in healthcare when a health service investigates a patient complaint or medical error. 37 Individual blame logic is prevalent in workplaces with punitive work cultures, and those who wish to appease the community, as it seeks to identify an individual to blame for a mistake and apply restrictions or sanctions to the individual. 38 This approach is based on the assumptions that individuals have sole responsibility and the autonomy to choose between safe and unsafe practices and, that the individual was not paying enough attention.38,39 However, individual blame logic does not account for the organisational, and management factors that impact decision-making, resulting in the perpetuation of a fear-based culture rather than improving the organisational and management factors that would prevent the action from occurring again.36,39
The low level of confidence in organisational culture found in this study has been reported before, in a grounded theory study undertaken in NSW, Australia, that examined clinical decisions regarding the care of older people. Simpson et al. found that low confidence in their employers strongly influenced paramedics’ clinical and conveyance decisions. 13 In particular, and consistent with the findings in this research, the authors identified how adverse outcomes surrounding non-transports were handled by middle managers, and informed the paramedics’ concerns of organisational reprisal. 20 Evidence of low confidence in employers is not unique to paramedicine in Australia and has been reported in other ambulance services in the UK and Finland during the early stages of professionalisation.10,13,17,36,39
Further, while paramedics spoke to assessing risk for the patient, risk stratification tools to support their decision-making were not evident in their decision-making processes. This finding is supported by Halter et al. 10 who reported that despite their participants having been educated in using a decision support tool, all except one participant used the tool retrospectively rather than at the point of care and considered it largely for documentation rather than decision support.
In the theme, evolving professionalisation and expectations of paramedics, self-taught psychosocial assessment was identified as pertinent to paramedic practice although absent from their preparatory or ongoing professional development education. Psychosocial assessment has been reported in research exploring paramedics’ perspectives of the psychosocial support needs of older patients in the out-of-hospital setting 40 whereby all participants agreed or strongly agreed that older patients needed more than physical care alone and wished they could do more for their patients. Most (10 of 14) participants identified they were unable to meet the needs of older patients. 40 Interestingly, we found instances where participants remarked that while they complete psychosocial assessments daily, they had never considered the degree to which this assessment contributed to conveyance decisions. This finding may reflect a deficit in education regarding the psychosocial needs of patients and available support options contributing to the theory-practice gap.40,41
Paramedics in Australia have gained national registration under the National Health Law however, the clinical activities an Australian paramedic can perform are only permissible through the organisation's internal scope of practice policies as governed by the employing organisation's medical director, and, further, the ability to obtain and administer drugs is governed by the jurisdictions government body. 42 While medical dominance has become less entrenched in today's society, it continues to exist in many areas of healthcare and is still strongly embedded in paramedicine. 43 Seminal work by Bucher and Strauss argued that professional registration and legislation are an exercise in power and authority; similarly, it is expressed that doctors continue to be the gatekeepers to healthcare.43,44
Professional autonomy is a pivotal element of professionalisation of an occupation, allowing the profession to define its scope of practice, role, and place within a healthcare system. 45 Central to professional autonomy are critical thinking and clinical-reasoning skills, which paramedics develop as cornerstones of their professional knowledge. Further, autonomy is an important element of creating a positive working environment. 46 Research with registered nurses has identified that professional autonomy enhanced patient advocacy. 47 Hence, the continued dominance of a medical director for paramedics may curtail their ability to explore the autonomy embedded throughout their education and demanded by professionalisation. When the work culture is saturated with policies, procedures, directives, and circulars, professional knowledge is constrained, and clinicians become checklist-orientated and task-focused rather than autonomous critical thinkers. 48
Many participants voiced their frustration about not being able to act differently because of feeling bound to abide by both organisation and community expectations. The cultural expectation – that all patients should be transported to a hospital – has been perpetuated either through paramedics’ education or experiences within the ambulance service, an example of tacit knowledge. It could be surmised that paramedics are demonstrating risk mitigation strategies because of the heavily protocolised organisation in which they are employed, contributing to their feeling constrained. The resultant behaviour of paramedics is not demonstrative of professional clinical reasoning; rather, it is the application of tacit knowledge born out of fear of reprisal should a paramedic not obey the organisational expectations or directions. This may be a result of paramedics feeling a low level of trust from the employing organisation and the personal risk associated with making their own decisions, rather than following a direction provided by the employing organisation. Paramedics must acknowledge that with autonomous practice, they must accept the responsibility aligned with autonomy, which, in this case, has some risk of organisational ramifications. For paramedics to achieve autonomous practice, an attitudinal shift and demonstration that they can be accountable for their clinical decisions are required. 49 This acceptance of personal accountability challenges an organisational culture based on fear.
Despite the significant advances in paramedic education, scope of practice, clinical reasoning and judgement, and the addition of national registration reflecting the advancement of the profession, the expectation of transport has prevailed. Simpson et al. 13 identified ‘you call, we haul’ (p. 9) as a theme of their research, articulating that the role identity held by paramedics in NSW was to transport all patients to a hospital. Interestingly, some years after Simpson's work, the exact words ‘you call, we haul’ were used by participants in this study and may have become part of the vernacular to describe the nature of their job, another example of tacit knowledge.
Limitations
Grounded theory studies do not aim to be generalisable as the findings are specific to the context and population of the research. 50 The population and context of this research are specific to paramedics working for the ambulance service in one state of Australia. The findings have been constructed from the experiences and knowledge of the paramedic participants with those of the researcher, however, the lead researcher was also an experienced registered paramedic contributing to theoretical sensitivity.
Similarly, participants may have consciously or subconsciously presented themselves in a manner that they thought the researcher desired or that they wanted to portray, they may not have accurately recalled their knowledge and may be unable to identify personal or unconscious bias. While this limitation is acknowledged, the application of methods, particularly constant comparative analysis, and the process of ensuring rigour throughout the research aimed to mitigate this impact. Finally, data collection occurred immediately pre-COVID-19 pandemic. During the pandemic, healthcare services experienced rapid shifts in healthcare delivery requirements for example, the introduction or expansion of virtual care and referral pathways. Such changes in healthcare delivery may lead to different findings should the same investigation be undertaken again at a different point in time. However, the theoretical framework, the tensions of the employing organisational culture and professionalisation is relevant despite the increase in virtual care models.
Conclusion
This research examined how paramedics navigate conveyance decisions, resulting in the construction of the theoretical framework, the tensions of the employing organisational culture and professionalisation. Paramedics working in a blame culture that is highly critical of their actions are at risk of forgoing their critical thinking to identify the need for transport, or the potential for alternative referral options based on their assessment of the patient, and instead default to transport patients to the ED. It is recommended that, paramedics must be appropriately educated and supported by the organisation to make safe, patient-focused decisions. Further research is needed to examine how organisations can support paramedic decision-making to refer patients to alternative care pathways or be discharged at the scene. This will further promote the professionalisation of paramedicine.
Supplemental Material
sj-docx-1-pam-10.1177_27536386251335406 - Supplemental material for The tensions between organisational culture and professionalisation and their influence on paramedic conveyance decision-making: A constructivist grounded theory framework
Supplemental material, sj-docx-1-pam-10.1177_27536386251335406 for The tensions between organisational culture and professionalisation and their influence on paramedic conveyance decision-making: A constructivist grounded theory framework by Alannah Morrison, Alison Craswell, Fiona Bogossian and Bill Lord in Paramedicine
Footnotes
Author contributions
All authors have been involved in the preparation of the manuscript and have approved this version for submission. Study design: AM, AC, FB, BL; data collection: AM; data analysis: AM, AC, FB; study supervision: AC, FB, BL; manuscript writing and editing: AM, AC, FB, BL.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The KJ McPherson foundation, a non-profit organisation supporting out of hospital research and staff development. Funding from the Australian Government Research Training Program Scholarship also supported this research.
Ethical approval
Ethical approval was granted by the University of the Sunshine Coast Human Research Ethics Committee (S191288).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.