
Abstract
Gender-based harassment is a pervasive issue in historically male-dominated professions like paramedicine. Despite reaching gender parity, women in paramedicine continue to face everyday sexism and workplace sexual harassment, resulting in psychological distress, career limitations, and underrepresentation in leadership roles. This qualitative study, informed by phenomenology, explored the lived experiences of registered paramedics in Australia who identified as women. The research aimed to examine not only the impact of everyday sexism and harassment on their career progression, wellbeing, and job performance, but also how individuals navigate such experiences. Furthermore, it sought to investigate how the organisational culture of paramedicine shapes and influences these experiences. Data were collected through surveys and in-depth interviews, providing nuanced insights into participants’ lived realities. Thematic analysis was employed to identify patterns related to the complex interplay between systemic sexism, personal coping strategies, and workplace culture. Consistent with prior research and government inquiries, the findings show that everyday sexism and workplace sexual harassment begin early in women's careers, persist throughout, and are tolerated by both colleagues and those in authority. Women were found to endure these behaviours due to fear of retaliation and a perceived lack of employer support. Workplace sexual harassment is as frequent as everyday sexism, highlighting its ubiquitous nature within paramedicine. A critical finding in this study is that the normalisation of sexism within Australian ambulance services fosters a tolerance of incidents among women employees and the belief that meaningful change is unattainable. The organisational culture of paramedicine plays a significant role in shaping women's experiences, often perpetuating systemic sexism through tacit acceptance and institutional inertia. Findings from this study identify that women navigate these challenges by employing strategies such as self-censorship, avoidance, or reliance on peer support, though these approaches may, at times, reinforce the status quo. This culture of tolerance and fear exacerbates power imbalances and fosters disengagement, undermining efforts to create equitable workplaces.
Introduction
Ambulance work originally emerged from military beginnings and has historically been steeped in images of heroic masculinity. 1 Despite undergoing changes during industrialisation, the occupation has preserved its paramilitary structure and association with masculinity.2,3 Even with the expansion of education and training programmes in the formation of St John Ambulance Australia, the presence of military-style ‘ambulance brigades’ persist. These brigades explicitly communicated to their members that women were deemed unsuitable for the work. 4 Not until the passing of the NSW Anti-Discrimination Act in 1977 were women formally allowed entry into the profession.4,5 Since this time, women in paramedicine have consistently reported gender-based discrimination and harassment despite the profession achieving near gender parity.6–8
Investigations into ambulance services in Australia have uncovered high rates of workplace gender-based and sexual harassment.1,6–9 A 2008 NSW parliamentary inquiry found that the Ambulance Service of NSW had an exclusive and discriminatory culture. 6 A subsequent inquiry in 2018 revealed continued discrimination, bullying, and gender-based harassment. 7 Similarly, the independent review into workplace equality at Ambulance Victoria highlighted contemporary issues of everyday sexism and workplace sexual harassment, often downplayed, or covered up within the organisational culture. 8 An analysis of organisational responses to workplace sexual harassment in paramedicine reveals a lack of recognition regarding the seriousness and criminality of such incidents. This suggests a pervasive cultural perception that downplays the gravity of sexism and its consequences. 9
The limited academic investigation into workplace sexual harassment and everyday sexism in paramedicine is concerning.1,8,9 Research is crucial to understanding the embeddedness of the problem in organisational culture and the impact of both.
Research aims and objectives
This study aims to explore the experiences of everyday sexism and workplace sexual harassment among paramedics in Australia who identify as women. Additionally, it explores how these experiences are embedded within the organisational culture of paramedicine.
The specific objectives of this study are as follows:
To explore how everyday sexism and workplace sexual harassment are experienced and navigated by paramedics in Australia who identify as women. To examine the organisational and cultural practices that contribute to the normalisation and toleration of sexism and harassment in paramedicine. To investigate the impact of these experiences on the personal and professional lives of paramedics who identify as women, including their career progression and mental wellbeing. To identify coping strategies, paramedics who identify as women, employ in response to sexism and harassment in the workplace.
In summary, this paper illuminates the prevalence of everyday sexism and workplace sexual harassment in paramedicine, offering a deeper understanding of these issues. The findings outlined here have the potential to inform future research, policies, and initiatives aimed at creating more inclusive and equitable work environments for all paramedics.
Literature and conceptual framework
Everyday sexism is frequent gender-based harassment that is socially normalised and can contribute to a hostile work environment. The term refers to the everyday nature and frequency of gender-based sexism10,11 and encompasses negative commentary, discriminatory language, diminishment of women, sexually objectifying remarks, crude comments, sexist jokes, and gender stereotyping. 12 This type of sexism permeates ordinary life, its normalisation rendering it subtle and invisible.13,14
Nichols argues that everyday sexism is often viewed as harmless ‘laddish’ behaviour, a ‘boys will be boys’ perspective where sexism is constructed as ‘having a laugh’. 15 Sexist, insulting and demeaning comments, attitudes, and stereotypes are therefore conveyed as humorous. As Das and colleagues 14 argue, everyday sexism is a ‘micro-aggression’ and is therefore, easily dismissed as ‘inconsequential, harmless and frivolous’. These behaviours in the workplace are associated with the reduced wellbeing of staff 16 and tolerance of broader gender inequalities, such as social exclusion, gender discrimination, stereotyping, 17 and workplace sexual harassment.
While the terms ‘everyday sexism’ and ‘gender harassment’ 18 are sometimes used interchangeably, 19 we have opted to use ‘everyday sexism’ in this study to emphasise its ubiquity and frequent occurrence. It is important to acknowledge that intersectional identities further exacerbate everyday sexism and workplace sexual harassment, with women of colour, diverse sexual orientations, gender identities, and disadvantaged classes being more vulnerable.18,19 While everyday sexism may not meet the classic definition of sexual harassment or discrimination, research shows its effects can be equally harmful.17,20,21
Sexual harassment is defined as unwelcome conduct of a sexual nature that is offensive, degrading, intimidating, or hostile. 22 It is a prevalent issue in Australian workplaces. 23 According to a national inquiry by the Australian Human Rights Commission in 2018, 39 per cent of women in Australia had experienced sexual harassment at work. 23 In gendered organisations, everyday sexism and sexual harassment more broadly are used as a form of control that enforces and reinforces gender norms. This occurs through expressions of ‘contempt for women who step out of place by violating standards of stereotypical femininity. Examples may include scorn for those not behaving or appearing “womanly” enough or who display traditionally masculine interests’. 24 Research has also shown that women who exhibit masculine traits, i.e. conforming to the masculine norm, may obtain a level of acceptance by becoming ‘one of the boys’.1,19
Acker's theory of gendered organisations highlights how gender distinctions contribute to patterns of inequality, even within seemingly gender-neutral processes. 25 This provides a rich, heuristic device to explore gender inequality in paramedicine and associated issues of everyday sexism and sexual harassment. Acker's work challenges the idea of gender neutrality in all aspects of professional life and demonstrates how inequalities are consistently reproduced through organisational or professional values, beliefs, and culture. 26 These dynamics are deeply entrenched in occupations linked to masculine gender identity, constructing an ideal worker based on cultural stereotypes of masculinity while actively rejecting femininity as an acceptable norm.26–28
Methodology
Research design and paradigm
This study employs a qualitative design grounded in an interpretivist ontological approach, which views reality as socially constructed and subjective, shaped by individual experiences and interpretations. Aligned with this, the study utilises principles of Interpretive Phenomenological Analysis (IPA), a framework specifically designed to explore how individuals make sense of significant phenomena in their lives. Rooted in phenomenological and hermeneutic traditions, IPA emphasises understanding the lived experiences of participants, capturing idiographic insights that reflect the uniqueness of each participant's perspective.29–31
The framework further aligns with the study's aims and research questions, centring on the subjective experiences and perceptions of everyday sexism among paramedics identifying as women. Phenomenology within IPA plays a critical role in allowing participants to narrate their experiences from their perspectives, thereby validating their lived experiences as legitimate data for analysis. Unlike research methodologies that seek generalisability, IPA focuses on exploring the depth of individual accounts within a homogenous group, while acknowledging that the inclusion of varied perspectives was an intentional strategy to enrich the analysis and provide nuanced insights. 31
Research setting
This study was conducted within the Australian paramedicine profession, which operates under a statutory ambulance service model and is nationally regulated by the Australian Health Practitioner Regulation Agency (AHPRA). Paramedics in Australia must hold a degree qualification (or recognised equivalency) and be registered with AHPRA to practice. 32 While the workforce has reached gender parity in recent years, with women comprising approximately 50% of registered paramedics, systemic barriers to career progression and workplace equality persist. 1 Participants in this study worked across various Australian ambulance services, including metropolitan, regional, and rural settings, providing insight into how organisational structures and workplace culture shape their professional experiences. By situating this study within the broader regulatory and workforce context, the findings offer a nuanced understanding of how everyday sexism and harassment may manifest within the profession.
Recruitment and sampling
Participants were recruited via social media advertising through the Australasian College of Paramedicine. Recruitment materials invited women to share their perspectives on workplace culture and gender-related issues in paramedicine. It was explicitly stated that women did not need to have experienced direct or indirect instances of everyday sexism, sexism or sexual harassment to participate. This approach aimed to create an inclusive and diverse sample that could provide a range of insights into the profession. Interested individuals were directed to a research-specific website for further information and were required to complete a 2-min screening questionnaire to confirm eligibility. The screening questionnaire collected demographic and professional data, including age, current position, duration of employment, education, specialist qualifications, and geographical location. Eligible participants were those who identified as women, had at least 1 year of employment as a paramedic, and worked in either a jurisdictional or private ambulance service. From the 105 responses received, eight participants were selected based on their ability to provide diverse perspectives representative of the profession's geographical, educational, and role-based variations. This approach aligns with IPA's idiographic focus, which values depth over breadth in participant selection. 31
While the recruitment strategy aimed for inclusivity, it is acknowledged that women with experiences of sexism or harassment may have been more motivated to participate. This self-selection could contribute to the richness of data but also raises the possibility of selection bias. The study's intent was to explore these phenomena through the lived experiences of participants, making this focus both appropriate and valuable for qualitative research.
No men were included in this study as its purpose was to understand women's experiences. However, it is important to note that men also encounter sexism and harassment, driven by gender hegemony and perceptions of feminisation, non-traditionality, homosexuality, or weakness. 24
Data collection and analysis
The study was centred on gaining insights into everyday sexism within paramedicine from the perspective of women paramedics. The interviews in this study were, in-depth, one-on one and semi-structured in nature. All interviews were conducted via an online platform to ensure consistency across the data collection process. Using an online platform was crucial for promoting equitable access among participants, allowing individuals from diverse geographical locations and varying circumstances to participate without barriers. Additionally, this approach minimised variability in the interview environment, which could have arisen from using alternative modes of communication, thereby enhancing the reliability and comparability of the data collected. The interviews were completed by one interviewer for consistency, lasted approximately 1 h and were recorded and transcribed. To ensure rigour and mitigate potential limitations inherent in qualitative interviews, several strategies were employed:
Semi-structured interview guide: A standardised guide was developed to ensure that all participants were asked core questions while allowing for follow-up questions based on their responses. This approach minimised variability in data collection and maintained alignment with the study's objectives. This guide was informed by prior research undertaken by Hanna-Osborne
1
and was reviewed for relevance and appropriateness by the supervisory team. Member checking: Participants were provided with their interview transcripts and preliminary findings to review and validate. This ensured that the data accurately represented their experiences and interpretations, enhancing the credibility of the study. Interview transcripts were systematically coded following Braun & Clarke's six-phase framework for thematic analysis.
32
Coding was conducted manually, enabling the researcher to engage with the data in a flexible, nuanced, and rigorous manner. To ensure rigour and transparency, all codes were reviewed by the supervisory team.
This study complies with the standards for reporting qualitative research equator guidelines and recommendations.
Researcher characteristics and reflexivity
The research team comprises of three members with diverse yet complementary expertise. Two of the researchers bring extensive experience as paramedics and educators, providing valuable insights from both clinical and educational perspectives. The third researcher, with significant experience in social sciences and in the gendered organisational space, offers a critical lens on the sociocultural dynamics within the profession. This interdisciplinary approach enriches the study, allowing for a comprehensive analysis of the issues at hand.
As interpretivist researchers, we also acknowledge our own perspectives are inevitably subjective. 33 Our researcher subjectivity is shaped by our diverse disciplinary and personal knowledges and experiences. We recognise that our positionality inherently shapes our approach to this research and that our awareness and transparency ensures we critically examine how power, gender, and work influence women's experiences in the profession.
Ethical considerations
This study was approved by the Human Research Ethics Committee at Charles Sturt University (Approval No. H20368). Written informed consent was obtained from all participants, and pseudonyms were used to ensure anonymity. The study adhered to ethical guidelines, protecting participants’ confidentiality and rights, particularly given the sensitive topics of sexism and harassment.
Findings
An overview of the final sample of participants is represented below (Table 1).
Participant characteristics.
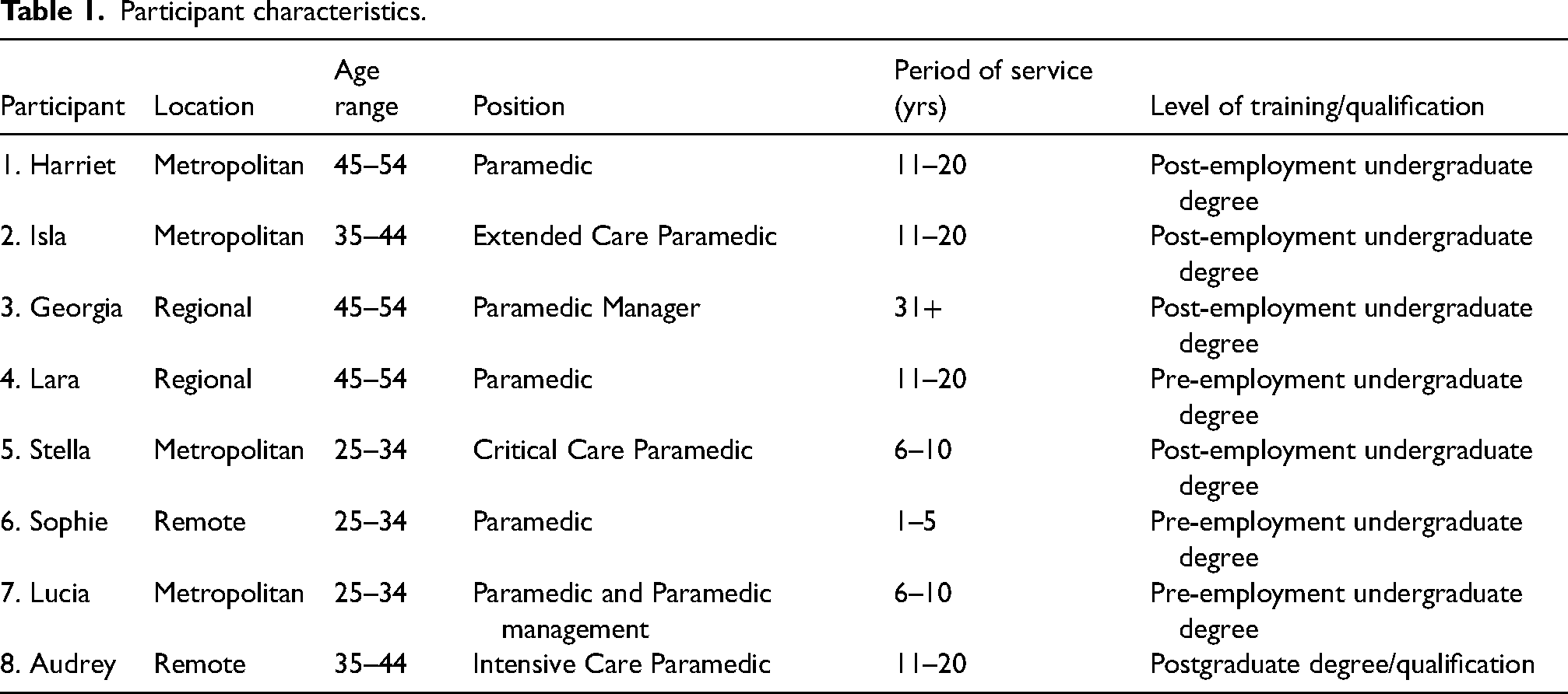
All participants in the study directly experienced everyday sexism and all reported incidences of workplace sexual harassment. Everyday sexism and workplace sexual harassment were found to start early in a woman's career through a process of enculturation, whereby new employees are gradually socialised into the prevailing workplace culture, learning to accept and tolerate discriminatory sexist behaviours as part of the profession. A critical finding in this study is the normalisation of sexism within Australian ambulance services, leading to a concerning degree of acceptance of such behaviour among women employees. The women interviewed expressed a sense of helplessness, indicating that they felt unable to effectively address these issues within the organisational culture of ambulance services in Australia. Practices that acted as mechanisms to normalise everyday sexism and workplace sexual harassment included:
the habitual verbal description of women as inferior and inappropriate for the paramedic role the frequent sexualisation of women (that also escalated everyday sexism into workplace sexual harassment) the toleration of sexist practices by male colleagues, those in positions of power, and, to some extent, by women themselves.
Content warning
The following section contains direct accounts of workplace and gender-based harassment, including descriptions of crude behaviour and censored explicit language. These narratives are presented to authentically reflect participants’ lived experiences and highlight the severity of the issues discussed. Reader discretion is advised.
Habitually describing women as inferior and inappropriate for the paramedic role
Women interviewed for the study encountered everyday sexism and workplace sexual harassment early in their careers and as part of their training. This initial phase of women's professional careers was marked by derogatory remarks that questioned the competence of women relative to men in performing paramedic duties. To illustrate, one participant recounted an incident where an instructor responsible for her driver training questioned her driving skills based on her gender: During driver training he made me drive everywhere because [he said] I needed the most experience because women tend to need more training for driving. He said that to me in front of everyone in the group… This person then went on to make several [similar] comments throughout the following week of training. (Sophie)
In this incident, the trainer framed the act of driving as gendered, explicitly stating that women's driving abilities were inferior to men's. In doing so, he perpetuated a cultural stereotype that women were less competent in a professional setting. During Stella's first days as a qualified paramedic, she was subject to her Station Officer relegating her to a domestic cleaning role because of stereotypes about her gender. He said, ‘[Stella] you need to go clean the cars because that's a female's job’.
Similarly, Stella recounts a male colleague explicitly discounting her professional competence, saying, ‘Well, you just drive my car because that's all you’re good for’. Audrey also recalls her gender and professional suitability being questioned early in her career. She details being ‘painted as the overly emotional female who just can’t let go of something that they [she] raised’.
Lucia, Harriet, and Isla each observed that sexist remarks were made by both superiors and colleagues. These comments were often delivered in group settings, where they were heard by others. Harriet recounted one such experience that referred to women's incompetence causing extra work for male colleagues: Maybe they shouldn’t be in the job, if men were there, we wouldn’t have to call for back up. (Harriet)
Isla found that male colleagues would outwardly express the opinion that women did not belong in paramedicine: They would just say women don’t belong in this job. (Isla)
When sexist comments are made by colleagues, particularly by those in positions of authority and in public forums, they serve to normalise sexism within the workplace. These brief but frequent interactions demonstrate how the normalisation of a sexist workplace occurs through constructing women as incompetent, inferior to male colleagues, and inappropriate for the paramedic role.
Frequent sexualised comments and encounters that can escalate into workplace sexual harassment
All women in this study encountered frequent sexualised comments. Georgia described them as ‘inappropriate’ comments with a ‘sexual undertone’. The frequency and casual nature of these remarks contributed to an enculturation process where the sexualisation of women escalated into workplace sexual harassment. Stella recounted conversations in the workplace where male colleagues used language to discuss women that she described as ‘crass’ and ‘horrific’:
…so, the helicopter base is 100% male… if you want to talk about women being objectified, I’ve never worked in a more crass, horrific environment where conversations about c***s, spit roasting, sexual preferences, sexual conquests were rife…. (Stella)
Stella went on to say that this objectification of women distanced her from her work role, colleagues, and the workplace itself. She said, ‘It is no longer my workplace, it is ‘their’ workplace’.
Sophie recounted incidents where male colleagues encouraged her to rate female colleagues and patients based on their physical appearance and sexual appeal: Sharing (not necessarily) nude pictures of females, “oh this is a 10, this is an 8”, sometimes related to staff, sometimes just generally or patients. I would smile and giggle or just not contribute and walk away. (Sophie)
Sophie responds with humour and tolerance to shield herself from being included in the objectification of women. Incidences such as these demonstrate how everyday sexism, and the sexualising of women can create a sexist organisational culture where everyday sexism and incidents of workplace sexual harassment become commonplace.
Stella described situations where inappropriate touching by a superior occurred. Importantly her account highlights how instances of workplace sexual harassment during training might be discreetly disguised as part of paramedic education or professional development aimed at enhancing clinical practice: He would be driving in the car, and I would be the passenger, him putting his hand on my leg and squeezing’ coming up behind you uninvited with shoulder rubs and to the point where he would be doing scenarios and wanting to show how you do a chest examination on a female and him doing it [to me]. (Stella) I remember him saying, he was driving, and he goes, you know what, “All I want to do is go down on you”. (Isla) …he literally looked at me and said, “It smells like fish in here”. (Lara)
Toleration and endurance of sexist practices by colleagues, leadership, and women themselves
Our findings show that toleration can be part of how everyday sexism can escalate into the more dangerous and recognisable behaviours of sexual harassment. The study found that tolerance of both everyday sexism and workplace sexual harassment by male colleagues, those in positions of power, and by women themselves results in the normalisation of both within organisational culture.
Tolerating sexism and harassment occurs for several reasons including the fear of challenging those in leadership and management positions and of career and personal repercussions. There were limited incidences within the interview data where colleagues stood up for women when they were experiencing discrimination or harassment. Standing up to perpetrators may put victims and bystanders at risk, particularly when perpetrators are in positions of power. As Lucia recounts, when women challenge sexism, they do so with the knowledge that those who influence their career opportunities and progression may retaliate: And at the time I did push really hard back against his comments, and I got into this heated argument for quite a long time. In the days afterwards, I realised, you know that this is my line manager who's going to be scoring my selection criteria and giving me feedback for the positions I apply for, so there's no way I could believe I was being fairly evaluated when he had told me that he believes women do not belong in some workplaces. (Lucia)
The normalisation of everyday sexism and sexual harassment can occur when leadership responds to incidences by moving perpetrators to another area of the organisation rather than disciplining them: There was being called the c word in front of all of your colleagues and he goes and gets a promotion. Not me but another female gets harassed by this male colleague in front of staff. And then he gets moved for a little bit and then when he brings him back, puts him in a promotion role. (Isla)
Toleration has significant consequences. As well as normalising sexism, it shields wrongdoers and increases the chance of retaliation against the victims. Our research revealed that the fear of this retaliation often compels women to endure instances of everyday sexism and sexual harassment.
As Sophie recounts, she tried to ignore incidences and framed them as humour to avoid humiliation and becoming a target for further mistreatment. … most people kind of laughed it off and pretended it was a joke. Everybody else just stayed quiet. I did what I think most females do which is sink small into the corner. (Sophie)
Sophie's response to the collective silence around her was to self-silence in an effort to shrink away from the environment and from her colleagues. Such a response protects her from further harm and as Isla points out below, also protects the perpetrator from becoming humiliated by being called out: I know for a fact I would have awkwardly laughed, because I still do it now. It would have been really uncomfortable. You don’t talk about sexual harassment or anything like that, you just go with it [and] don’t humiliate any of the older (male) paramedics. I made a conscious effort just to be friendly and joke around, engage in the jokes, whether they were appropriate or not. (Isla)
Tolerating everyday sexism was found to contribute to the escalation into workplace sexual harassment. Georgia described an instance in which she felt trapped in a paradoxical dilemma. Her male colleagues were engaging in the verbal sexualisation of women, and she felt that walking away would signal her opposition, potentially isolating her from the group. Remaining, on the other hand, condoned the behaviour. ‘The way I look at it is, if you stay involved in the conversation, you’re condoning the conversation, if I remove myself from it … I’m showing my thing by leaving it’. The latter position conflicted with her personal values; the former aligned her with workplace values.
When Lara reported incidents of sexual harassment she experienced ‘retribution from the male management colleagues’. Her line manager explicitly threatened her, saying that he knew she had children at home. ‘You’re a single mum, you got kids to get home to, don’t you? … well yeah … I can make you stay there as long as I f****n’ like’. When she reported the issue, the harassment escalated, and leadership advised her to treat the behaviour as though it was a joke. ‘And the highest manager in my sector, his response was literally word for word, “you need a certain kind of sense of humour to work in this job”’.
Discussion
This study highlights that the participants in this research frequently encountered everyday sexism and sexual harassment within paramedicine. Both begin early in a woman's career and are part of their initial and ongoing enculturation within the profession. While these experiences continue throughout a woman's career and are tolerated by colleagues and those in positions of power, this study reveals that they are also somewhat accepted by women themselves. Women in the study expressed concern that it is impossible to address these issues in ambulance services in Australia.
Women in paramedicine, through various workplace, parliamentary, and ambulance service inquiries,6–8,23 have consistently reported that men in the profession view women paramedics as incompetent, inferior, and inappropriate for the paramedic role. Importantly, these cultural attitudes and beliefs position women as outsiders, or tokens, 34 which in turn enables the sexualisation of women.35,36 Everyday sexism and workplace sexual harassment are consistent with the gendering of power relations in workplaces.
Connell's gender and power theory 37 proposes that the social construct of patriarchal power and subsequent gender inequality arising from it leads to sexism and the sexual harassment of women. Connell and Messerschmidt 38 further contend that the enculturation of such practices asserts early domination and power within the workplace. Such behaviours ensure masculine hegemony is preserved and women remain subordinate to men within the profession. Hegemonic masculinity is constructed within organisational culture through values, beliefs, and practices that reinforce the idea that men have a legitimate claim to a dominant position 38 and that, in an organisational context, they are entitled to dominate women. The sexualising of women thereby becomes a strategy that de-legitimises women in their work roles.18,19,39
Furthermore, Acker's 25 contention that the cultural marginalisation of women occurs through the gendering of occupational identity rings true. A gendered culture normalises aggressive masculinity through sexist practices. Those from within the organisation seek to sustain power by enculturating a new generation of paramedics into tolerating and replicating the same organisational culture. This gendered organisational culture has been found to influence career and training opportunities, impact feelings of self-worth and taint social interactions and gender relations within the workplace.28,36,39,40 In this sense, everyday sexism and workplace sexual harassment operate as gender policing and maintain traditional gender roles and hierarchies.40–42
Studies indicate that women in paramedicine, 1 firefighting, 40 policing, 22 critical care medicine, 43 construction, 36 and military roles 44 face similar challenges when integrating into masculine organisational cultures. In their study of gender harassment toward women pilots and automotive tradespeople in Australia, Foley et al., 19 (p.1682) found that ‘sexist remarks and banter from male colleagues were the most frequent form of gender harassment’ and that male managers and peers habitually turned a blind eye or joined in on sexist behaviours. These normalising behaviours were also found by Batty & Burchielli's 40 in their research into the experience of women in Australian firefighting. These experiences were compounded by being sidelined and belittled by male supervisors. These studies indicate that organisations fail to adequately protect women. Batty & Burchielli's revealing significant deficiencies in complaints and dispute-resolution processes (319). The authors argue that sexist practices contribute substantially to ongoing gender segregation issues and undermines the perceived professionalism of the firefighting occupation. Foley et al. 19 contend that the implications of everyday sexism in automotive and pilot occupations are that women's abilities are diminished, their ‘confidence and sense of belonging’ eroded and ultimately workplace inequality perpetuated.
While studies concerning women's integration into masculinised workplaces agree that many of the problems and implications are similar, there is also agreement that sectors that fail to reach gender parity do not perform as well as those that do. The business case for gender equity and diversity in areas such as forestry and mining shows that equality enhances performance, resilience, and economic renumeration.45–47 And while there is growing evidence that inclusive and diverse workforces are more efficient and productive and improve employee engagement and retention, 47 it is also apparent that simply increasing numbers of women does not suffice. Rather, as Johansson & Ringblom 46 contend, the benefits of diversity are increased when women's skill sets are recognised and valued which can prove to be a challenge in masculinised cultures.
Masculine cultures are prevalent when work roles are understood to be aligned with gender identity and when masculine qualities and attributes are constructed as superior to feminine qualities and characteristics. Research has shown that everyday sexism and sexual harassment are systemic issues within workplaces with masculine cultures. 23 Women working in male-dominated and masculinised work cultures have been found to experience heightened and more aggressive forms of sexism but as Bridges et al. 36 found, the prevalence and normalisation of sexism with a culture means that women themselves are ‘more likely to normalise it’. Women in our study also acknowledged sexist practices were a serious problem but similarly ‘adjusted expectations because the culture of the industry demanded this of them’. 36
Although all the participants in the study differed from one another in background, age, and work experience, there were commonalities in their experiences of sexist practices. All participants reported encountering comments that questioned women's physical capabilities and suggested they were unsuitable for the profession, as well as frequent sexualised remarks. This environment highlighted the women's awareness of the prevalence and tacit acceptance of everyday sexism and sexual harassment within their workplace.
Fear that perpetrators would retaliate if women outwardly resisted or reported sexism, and sexual harassment, drove women's attempts to adjust to the sexist culture. Fear of retribution and concern about inaction by line managers prevented them from discussing or reporting incidents. Indeed, our findings concur with and reinforce findings from inquiries in paramedicine that there is a high level of tolerance of sexism and sexual harassment in ambulance organisational cultures. Inquiries have also established that there are issues regarding poor organisational response and retributive action that deter victims and bystanders from reporting.6,8
Women in this study developed coping strategies that helped them assimilate and survive in a workplace where everyday sexism and workplace sexual harassment were normalised as part of the culture. Women reported the use of humour and making themselves invisible as coping mechanisms to reduce the frequency of incidences, to mitigate their impact, and avoid retribution. When coping strategies include collusion, such as engaging in the sexualisation of other women, laughing off sexual harassment, or self-silencing, they interfere with wellbeing and job satisfaction. Additionally, women's coping mechanisms were also found to contribute to and reinforce the ‘normalisation’ of everyday sexism and workplace sexual harassment in the workplace culture.15,48
Limitations
This study provides valuable insights into everyday sexism and workplace sexual harassment among women paramedics in Australia. However, there are some limitations to consider.
The sample size of eight participants aligns with the depth-focused approach of IPA. While the diversity of participants’ backgrounds – including age, geographic location, and professional roles – enriches the findings, the small sample may not fully capture the breadth of experiences within the profession. Additionally, as participation was self-selected, those with direct experiences of sexism and harassment may be overrepresented, potentially narrowing the range of perspectives. However, this does not diminish the significance of the insights gathered.
Another consideration is the reliance on participants’ retrospective accounts, which may be shaped by memory and personal interpretation. While these narratives provide valuable qualitative data, future research could explore these issues in real time to offer additional depth and immediacy. Furthermore, despite efforts to maintain reflexivity, the research team's backgrounds and perspectives inevitably influenced data collection and analysis. While this does not invalidate the findings, independent coding in future studies could further enhance objectivity.
The study's focus on women paramedics was intentional and aligned with its objectives. However, examining the experiences of men and non-binary individuals could offer a more comprehensive understanding of organisational culture and gender dynamics in paramedicine. Lastly, as this research is specific to Australian ambulance services, its applicability to other regions or healthcare systems may be limited. Cross-cultural studies could help determine the extent to which these findings resonate in different professional and societal contexts.
Conclusion
This study explored the pervasive experiences of everyday sexism and workplace sexual harassment among women paramedics in Australia. Through IPA, it was found that these behaviours are deeply embedded within the organisational culture of paramedicine, beginning early in women's careers and persisting throughout. Such experiences have significant psychological, professional, and social impacts on women in the profession.
The normalisation of sexism and harassment perpetuates a culture of tolerance, sustained by leadership and organisational practices that often fail to address these behaviours effectively. These findings emphasise the critical need for systemic changes, including improved leadership accountability, policy reforms, and gender sensitivity training, to foster equitable and respectful work environments.
While the small, homogenous sample aligns with the methodological aims of this study, it also highlights the need for broader research. Future studies should aim to explore these issues across diverse populations and organisational contexts to build on the insights provided here. By addressing the systemic issues identified in this study, organisations can begin to dismantle the structural barriers that perpetuate sexism and harassment, paving the way for a more inclusive and supportive paramedicine profession.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all those who contributed to the completion of this research project. Your support, insights, and dedication were invaluable throughout the study. We extend our thanks to our research participants for sharing their experiences, as well as our colleagues and fellow researchers for their guidance and encouragement.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.