
Abstract
Introduction
Paramedics encounter and are expected to manage stressful and traumatic situations on a regular basis during the course of their work as emergency medical professionals.1–5 They are also known to experience high levels of stress, anxiety, depression, burnout, and suicide.2,4 This trend was particularly prevalent during the COVID-19 pandemic. 4 Despite these known hazards, only some ambulance services offer robust psychological support for their staff. 5 Recent international research shows paramedics often rely primarily on individual coping strategies to regulate their emotional reactions during and after high-pressure callouts. 6 The identified gap between unmet coping needs and effective mental health support suggests there is an opportunity for growth at a systemic level as well as value in leveraging individual coping styles for optimal benefit.
The specific area of interest for this study was the double-edged quality of detachment, also referred to as distancing, reframing, reappraisal, objectivity, suppression, and compartmentalisation.3,6–8 Psychological literature differentiates between two forms of emotional detachment, one recognised as beneficial, the other as detrimental. 9 For the purposes of this article, detachment is considered an adopted coping style distinct from depersonalisation and burnout. 10 Even a chosen coping style, however, can be applied dysfunctionally. As a helpful template for this study, Denckla and Bornstein 11 authored a study on university students that differentiated between adaptive and dysfunctional forms of detachment. They defined adaptive detachment as ‘the ability to engage in flexible, goal-directed cognitive distancing accompanied by the capacity to moderate affective arousal and maintain functional levels of interpersonal connectedness’ [11 p148]. This version of detachment represents the aspect of the paramedic mindset that allows for the effective execution of tasks during and despite emotive, high-pressure situations. Meanwhile, they defined dysfunctional detachment as ‘a more generalized detached interpersonal style characterized by pervasive social isolation and negative emotionality’ [11 p148]. This version represents the harmful aspects of emotional coldness and negative self-image that may accumulate more generally, leading to devolving interactions with peers, partners, family members, and friends.3,6,7
A further area of interest was any controllable environmental factors that might influence paramedics’ detachment-based coping mechanisms – for example, organisational culture and peer relationships. Research shows that in high-acuity settings, social support between peers is a beneficial form of emotional grounding and stress reduction.12–14 This study therefore adopted McMillan and Chavis’ Sense of Community theory 15 as a framework to measure paramedics’ connections with each other and to provide a basis for investigating any correlations with emotional detachment scores.
McMillan and Chavis's
15
Sense of Community (SOC) theory operates on the idea that community interconnectedness can be subdivided into four dimensions: (i) membership, (ii) influence, (iii) integration and fulfilment of needs, and (iv) shared emotional connection [15 p9]. According to the original article, ‘sense of community is a feeling that members have of belonging, a feeling that members matter to one another and to the group, and a shared faith that members’ needs will be met through their commitment to be together’ [15 p9]. Peterson et al.
16
summarised the definitions of the dimensions as follows:
Membership: a feeling of belonging or interpersonal relatedness; Influence: a sense that one matters, or can make a difference, in a community and that the community matters to its members; Needs fulfilment: a perception that the community will meet its members’ needs by way of rewards, status, reciprocal solutions, interdependence, and the reinforcement of shared values; Emotional connection: a feeling of attachment or bonding rooted in members’ shared history, place or experience.
This framework thus depicts sense of community as a network of distinct connective threads that links paramedics to their colleagues and to their wider organisation. From this perspective, paramedic mental health and coping can be conceived not as separate attitudes in isolation but rather as a shared belief system that may either protect or prejudice its members’ mindset and behaviours.
With this background in mind, this study aimed to investigate potential approaches for understanding and improving coping styles for paramedics through a novel examination of emotional detachment and sense of community in a cohort of Australian and New Zealand paramedics. While this study did not attempt causative explanations, it did speculate on a relationship between emotional detachment and sense of community: specifically, that strong workplace social interconnectedness in a group of paramedics can positively influence their emotional detachment tendencies whereas reduced interconnectedness can negatively affect those same mindsets.
Methods
This study used quantitative, correlational research to measure the relationship between sense of community and emotional detachment in paramedics working in Australia and New Zealand. Findings were interpreted in the context of McMillan and Chavis's 15 Sense of Community theory.
Study design
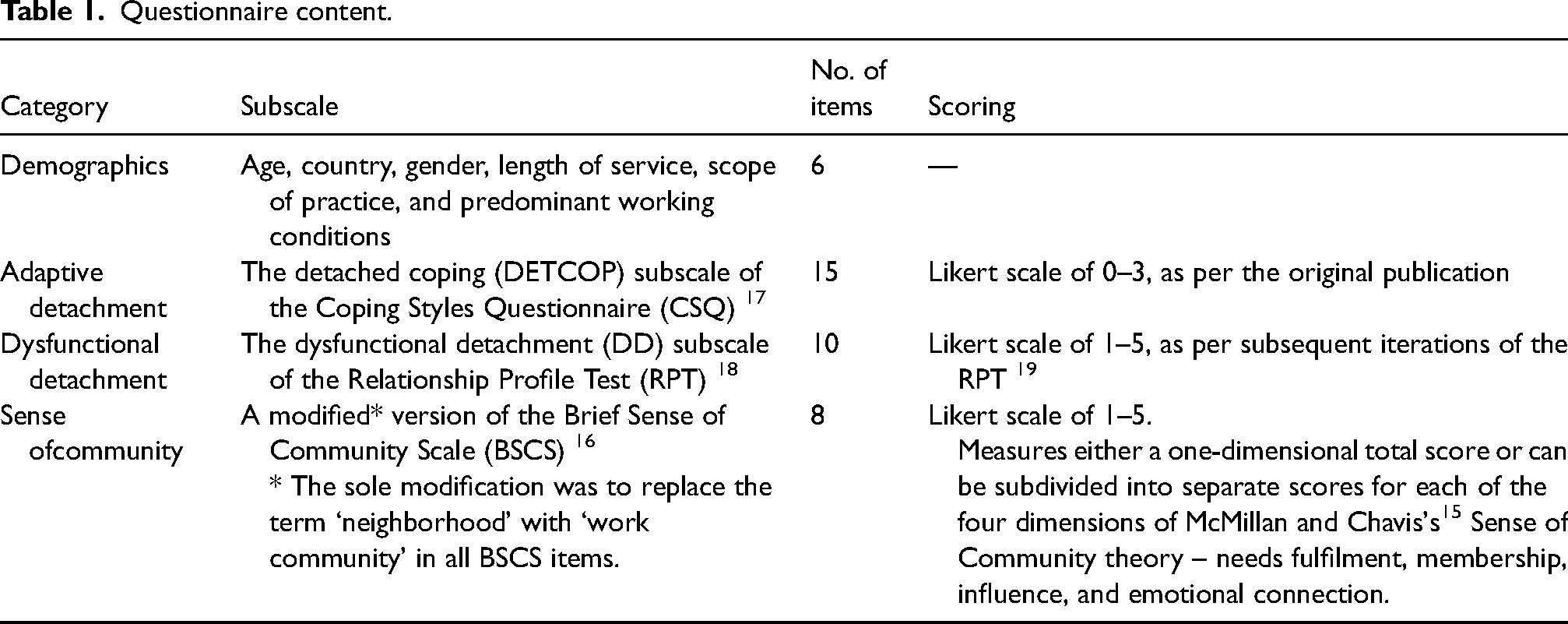
A questionnaire comprising demographic data and three previously validated subscales was created using SurveyMonkeyTM software and disseminated using the FacebookTM social media platform due to its popularity among paramedics. The subscales were selected to assess adaptive detachment, dysfunctional detachment, and sense of community respectively. Table 1 outlines the subscales. Appendix A provides a complete set of questions.
Questionnaire content.
This study is reported in adherence to the Consensus-Based Checklist for Reporting of Survey Studies (CROSS) reporting guideline. 20
Data collection methods
A pilot survey of approximately ten trial respondents was completed over ten days in order to gather initial feedback and assess viability and baseline results. No major issues were reported. On the advice of one trial respondent, the word 'emotional' was added to the survey title to distinguish the type of detachment being investigated.
This study used voluntary response sampling to recruit a convenience sample from an online population of Australian and New Zealand paramedics. Due to unplanned circumstances, data collection occurred during the COVID-19 pandemic at a time when both Australia and New Zealand had closed their borders. Based on a review of the number of members/followers in relevant FacebookTM groups at the time of the study, the total online presence of paramedics working in Australia or New Zealand was approximately 10,000, inclusive of an unknown proportion of student and retired paramedics. According to the tables in Taherdoost, 21 in order to infer reliable results with a confidence level of 95% and a 5% acceptable margin of error, this study needed to recruit at least 370 responses.
Sample characteristics
Recruitment for the main study was achieved through a process of anonymous self-selection on the part of participants. In order to access a representative population, the invitation to participate targeted currently employed paramedics working in either New Zealand or Australia. Paramedic was defined as a person working full- or part-time in the pre-hospital environment in an emergency operational capacity irrespective of authorised scope of practice.
Survey administration
By accessing seeded links to the survey on FacebookTM, potential respondents arrived at a consent and information page outlining the intent and format of the study. Contact information for mental health support services was also provided in the event that the survey content triggered any distress. If willing to proceed, participants checked a consent box and filled in the subsequent questionnaires. Participation was entirely voluntary and subject to no consequences in the event of early withdrawal. No compensation was provided. The survey was open for a period of five weeks from September to November 2020 and closed once the response rate significantly tapered off past the point of expecting further uptake.
Ethical considerations
Prior to its release, ethical approval for this study was obtained from the Whitireia WelTec Research and Ethics Committee (RP243–2020).
With regard to privacy and confidentiality, the questionnaires were completed anonymously, and the collected demographic data were insufficient to identify individuals.
Statistical analysis
Results for this study were calculated using descriptive and correlational statistical analysis. Independent T-tests, one-way ANOVA and Tukey post-hoc tests were applied using IBMTM SPSSTM (v. 27) statistics software. The data adhered to the required distribution for each analysis. Incomplete responses were excluded on a pairwise basis as per standard correlation calculations. P-values indicated the probability of the relationships occurring by chance. Pearson's correlation coefficients measured the strength of the relationships between the variables in this study. Cronbach's Alpha measured the reliability of the subscales.
Results
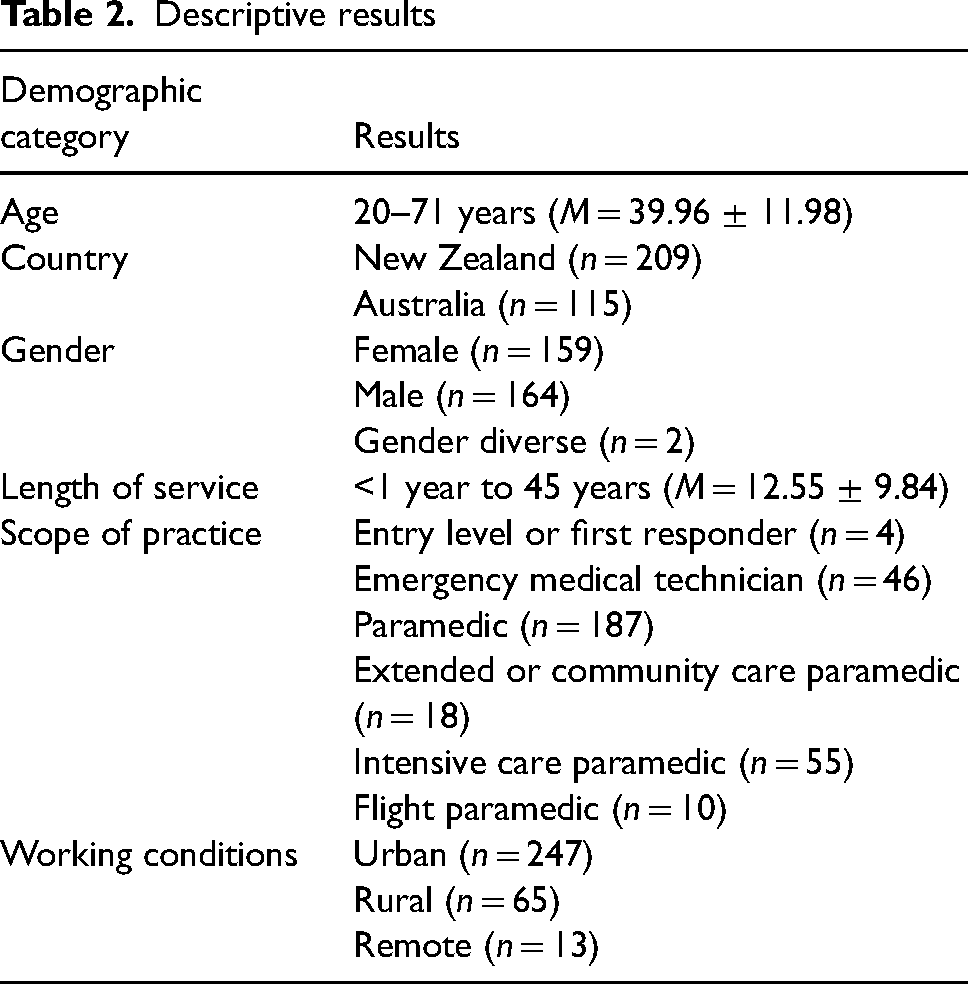
Based on a process of anonymous self-selection, a total of 335 participants responded to this survey. Overall, 282 were complete responses and 53 were partial responses, for an 84% completion rate. This sample size did not reach the target of 370 responses (seeking a 95% confidence level and a 5% margin of error); however, it exceeded the number of responses required for a 6% margin of error. 22 The typical time spent completing this survey was 5 minutes and 10 seconds. Descriptive results are collected in Table 2.
Descriptive results
Main findings
Data analysis from the three subscales yielded the following results.
Adaptive detachment
In this study, DETCOP scores ranged from 4 to 45 (M = 24.71 ± 7.09) out of a possible total of 45, where a high score represents an effective coping style that is able to adapt to changing emotional states. The value for Cronbach's Alpha was α = .89, indicating good reliability over the fifteen questions.
There was a significant statistical difference (P ≤ .001) between genders in terms of DETCOP scores, with females (M = 22.91 ± 7.02) scoring significantly lower than males (M = 26.31 ± 6.80).
No other significant differences among demographic categories were found in terms of adaptive detachment. That is, no statistically significant relationships were found within age, country, length of service, scope of practice, or predominant working conditions.
Dysfunctional detachment
In this study, DD scores ranged from 15 to 50 (M = 31.47 ± 7.17) out of a possible total of 50, where a high score represents a dysfunctional level of emotional disconnectedness. The value for Cronbach's Alpha was α = .83, indicating good reliability over the ten questions.
No statistically significant differences among demographic categories were found in terms of dysfunctional detachment.
Sense of community
Sense of community was measured according to a one-dimensional total score and also subdivided into separate scores for each of the four dimensions of McMillan and Chavis's 15 Sense of Community theory (needs fulfilment, membership, influence, and emotional connection).
In this study, total single-dimension scores ranged from 8 to 40 (M = 28.81 ± 5.31) out of a possible total of 40, where a high score represents a strong general connection with workplace communities. The value for Cronbach's Alpha was α = .89, indicating good reliability over the eight questions. When Pearson correlation coefficients were calculated, total SOC scores correlated positively with adaptive detachment scores (r = .188; P = .002) and negatively with dysfunctional detachment scores (r = −.279; P ≤ .001). That is, a high sense of community correlated significantly though weakly with a high level of adaptive detachment and a low level of dysfunctional detachment. Conversely, a low sense of community correlated significantly though weakly with a low level of adaptive detachment and a high level of dysfunctional detachment.
Meanwhile, scores in each of the four dimensions ranged from 2 to 10 out of a possible total of 10, where a high score represents strong satisfaction within the given dimension. The following mean scores were obtained for needs fulfilment (M = 6.94 ± 1.65), membership (M = 7.62 ± 1.61), influence (M = 6.71 ± 1.46), and emotional connection (M = 7.52 ± 1.61).
When correlational analysis was applied between the four dimensions and adaptive and dysfunctional detachment, more nuanced results took shape. Variations in the dimensions produced statistically significant correlations in terms of both adaptive and dysfunctional detachment scores (see Table 3 and Table 4).
Adaptive detachment and SOC dimensions
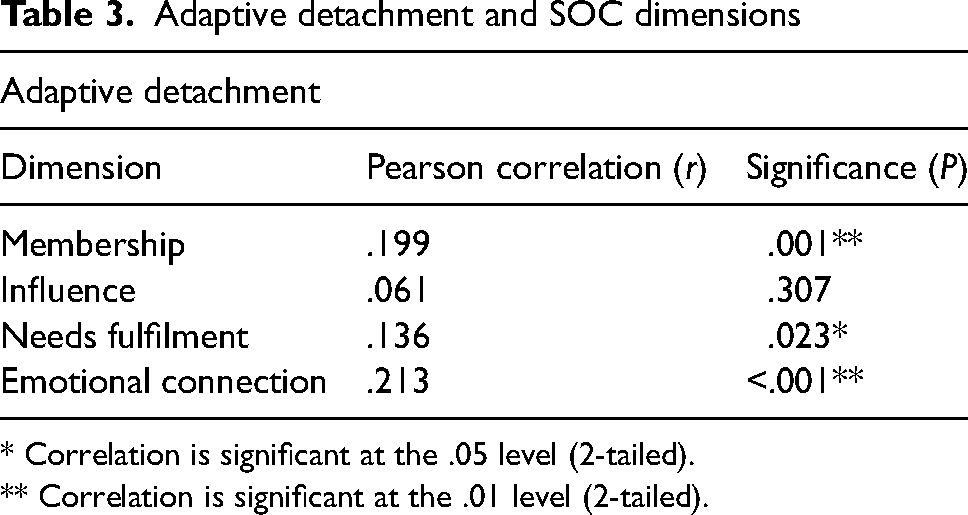
* Correlation is significant at the .05 level (2-tailed).
** Correlation is significant at the .01 level (2-tailed).
Dysfunctional detachment and SOC dimensions
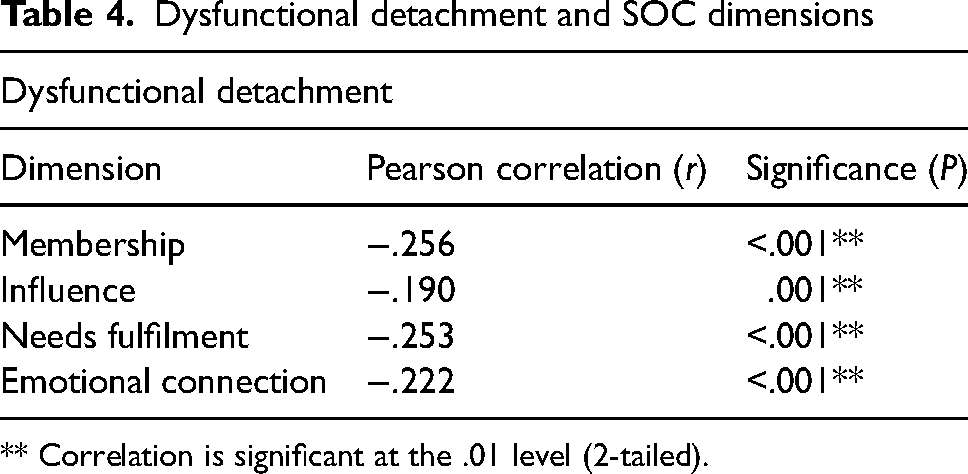
** Correlation is significant at the .01 level (2-tailed).
Specifically, higher levels of membership need fulfilment, and emotional connection indicated higher coping scores in terms of adaptive detachment.
Conversely, dysfunctional detachment correlated negatively with membership, emotional connection, needs fulfilment, and influence. In other words, lower levels in all four dimensions indicated more concerning levels of dysfunctional detachment and vice versa.
Overall, Pearson correlation values indicate fairly weak relationships in these areas. Although care should be taken not to inflate implications, they are nonetheless intriguing in terms of directions for further research.
Discussion
This study explored emotional detachment and sense of community in the paramedic workforce, collecting data from paramedics of all genders working throughout New Zealand and Australia in a variety of organisations, roles, and workplace conditions across a wide range of ages and experiences. As such, it provides insights into the paramedic mindset and also, by extension, has generalised applicability to paramedics and emergency service and allied healthcare professionals working elsewhere around the world.
In general, findings showed that gender and the four dimensions of SOC theory had significant, though muted, relationships with emotional detachment scores. Female paramedics had significantly lower adaptive detachment scores than males, suggesting opportunities for further education and research. On average, the results do not appear to represent extremes of either adaptive coping or dysfunctional detachment. Meanwhile, SOC showed significant relationships with emotional detachment at single and multi-dimensional levels alike. Sense of community scores correlated positively with adaptive detachment scores and negatively with dysfunctional detachment scores, implying a supportive relationship between SOC dimensions and detachment-based coping styles in paramedics working in Australia and New Zealand. Although correlations were relatively weak, there is now a basis for inferring that social interconnectedness does indeed play a part in the emotional detachment tendencies of paramedics.
An examination of the findings from this study in the context of existing literature identified three key themes: levels of adaptive and dysfunctional detachment in Australasian paramedics compared with other studies; female gender and adaptive detachment; and the benefits of a sense of community in the paramedic work environment.
Paramedic levels of emotional detachment
Adaptive detachment
No other paramedic or healthcare provider studies that used this scale were found for comparison. However, mean adaptive detachment scores in this study were generally comparable with data sets from contemporary studies, including a cohort of Western Australian police officers.23–27 There was some variability, however. The standardised scores published in Roger et al. 17 appeared particularly low. Whether due to the student population used, potential generational changes since the early nineties, or other factors, it seems the Australasian paramedic sample scored particularly highly compared with this original norm. In terms of more recent studies, a population that came closest to representing a heterogenous spread of adults was investigated in the context of internet dependency. 25 Their results provided some context for viewing the paramedic scores in the present study as below average, as they were lower than those of a typical internet user.
Dysfunctional detachment
No other paramedic or healthcare provider studies that used this scale were found for comparison. However, the mean DD scores in this study were somewhat higher than the non-clinical norms determined by Bornstein et al., 18 where averages for males and females were M = 30.58 ± 5.37 and M = 29.84 ± 5.78, respectively. Compared with other studies using the same scale, however, scores in this study were generally comparable. For instance, average scores for this cohort were lower than those for substance abuse inpatients 28 and low-income urban women in a US city. 29 They were comparable to the DD scores of the married control group in Denckla et al. 30 Therefore, by this measure, paramedics in this study had DD scores generally consistent with those of an average married adult. At the same time, a proportion of DD scores in the present study were ≥ 38, which exceeds the mean DD score for adults suffering prolonged grief due to the loss of a spouse. 30 The implication is that a subset of paramedics may have a severe level of dysfunctional detachment.
Female gender and adaptive detachment
Results from this study showed a significant difference between male and female mean coping scores, with females scoring much lower than males in adaptive detachment. This is a known trend in coping studies, with women generally reporting a more complex relationship with emotions.31–33 The discrepancy between genders appears in Roger et al.'s 17 original benchmark norms for this subscale, which gave an average score of M = 18.71 ± 6.42 for males and M = 16.01 ± 4.87 for females. Similar gender-based discrepancies appear in results from other studies that employed the same subscale.23–27 This theme has implications for mental health. For instance, Kelly et al.'s 31 results showed that less use of the adaptive technique of positive reframing correlated with higher depression scores in women compared with men. The question then becomes why female paramedics may have more difficulty regulating their emotions.
One study that used fMRI to compare brain activity in men and women found that women exhibited a neurological tendency to use more brain power when regulating emotions. 32 The authors linked these findings to the fact that women are known to conceptualise their emotions more complexly than men and so their regulatory efforts may therefore be more impeded by fatigue. 32 This relationship may in fact help to explain lower mean adaptive detachment scores in female paramedics. In the pre-hospital environment where fatigue is prevalent and emotions are often already highly complex, emotion regulation may just be harder work for women.
The implications fall in at least two possible directions. Firstly, if female paramedics statistically trend towards a reduced capacity for adaptive detachment, then they are at heightened risk of depression and anxiety. 31 Secondly, if coping style can be influenced by learned strategies, 33 then adopting new strategies ought to increase adaptive detachment scores in this group. Evidence shows that positive reappraisal would be a particularly helpful strategy to teach and apply in the paramedic context.6,31,33,34 An even more progressive solution would be to teach meta-coping – the use of a mental coping engine, so to speak, that continually adjusts coping strategies in response to real-time encounters.35,36 Encouragingly, findings from a meta-analysis by Aldao et al. 37 suggest that the absence of adaptive coping strategies is less detrimental than the presence of maladaptive ones. Therefore, addressing this imbalance in gender coping styles becomes less pressing than regulating dysfunctional tendencies.
Benefits of sense of community in the paramedic environment
Single- and multi-dimensional SOC scores in this study correlated significantly with adaptive and dysfunctional forms of detachment. These findings bore out the initial hypothesis that SOC has a beneficial role to play in affecting paramedic coping styles. While this finding in no way proves causative or protective value, it is nonetheless insightful and paves the way for future research into methods for regulating emotional detachment techniques in paramedics and other emergency frontline personnel.
The fact that different SOC dimensions correlated differently with the two forms of detachment was an unexpected finding. The practical advantages of linking specific social needs to specific coping responses can allow workplaces and individuals to design and apply effective development options in all four dimensions, thereby improving overall well-being.
Membership
Membership had a statistically significant relationship with both adaptive and dysfunctional detachment in this cohort. Of all the four dimensions, membership had the strongest combined associations, indicating that a sense of belonging within an organisation or shift group, whether present or lacking, coincided with both adaptive and dysfunctional tendencies.
The implication is that the attributes of membership – whether provided by the group or withheld, whether accepted by the individual or rejected – have a direct link to emotional detachment preferences and mindsets in paramedics. 13 Ultimately, membership appears to be a collective attribute worth fostering in professional organisations. 38 Along with ensuring higher morale in personnel, there is now evidence that it may contribute to enhanced detachment-based coping strategies as well.
Influence
Influence had a statistically significant relationship with dysfunctional detachment, but not with adaptive detachment. With regard to adaptive detachment, differences between the least adaptive and most adaptive scores were practically non-existent, implying that a sense of influence, control, or agency within the larger paramedic work community did not in fact have any association with capacity for adaptive detachment. In a way, that is reassuring news, as it suggests that the ability to teach or apply adaptive detachment coping techniques is equally possible in both disaffected and cohesive workplace cultures alike. 33 Ultimately, however, the influence was the least impactful of the dimensions in terms of emotional detachment, and therefore redirects a stronger focus onto the other three dimensions.
Needs fulfilment
Needs fulfilment had a statistically significant relationship with dysfunctional detachment and to a lesser degree with adaptive detachment. Alongside membership, it had the most statistically significant association with dysfunctional detachment in this study, indicating that rewards, status, reciprocal solutions, interdependence, and the reinforcement of shared values played a crucial role in social connection and detachment tendencies.
Although causation cannot be presumed, there is a sense in the idea that unmet needs at work would predispose personnel to disengage as a form of avoidance-based coping. 39 From a tripartite coping theory perspective – where coping is considered to be either problem-focused, emotion-focused, or avoidant 40 – unmet needs at work would arguably impair the first two styles and heighten the attraction of the latter, resulting in an impulse to withdraw. After all, in an environment like paramedicine, where individual paramedics often have minimal control over the content of their jobs or the busyness of their workload, where they may feel they have neither influence nor energy to enact change, and where they simultaneously engage in exhausting emotional labour on a regular basis on a background of disrupted sleep cycles – in such an environment, their resources are prone to being depleted.1–5 Therefore, neither problem-focused nor emotion-focused coping may be appealing, leaving avoidance-based coping as the main recourse. 1 In such an environment, where individuals can become easily overburdened by emotional demands, the onus must shift to organisations to help fulfil or bolster those needs.38,39 Consequently, the reverse may also be true: in a work environment where core needs are generally met, the prospect of emotional engagement may seem less daunting overall.
Emotional connection
Emotional connection had a statistically significant relationship with both adaptive and dysfunctional detachment. In fact, it was the most statistically significant dimension in terms of adaptive detachment in this cohort. The implication is that, of all the dimensions, emotional connection links most strongly with paramedics’ capacity to constructively detach from emotionally intense situations. Participants who felt seen and understood by their peers were better able to intentionally separate themselves from stressful encounters and view problems or reactions objectively.
MacMillan and Chavis 15 explicitly included shared resolution of crises or problems in their definition of emotional connection. Perhaps the assurance that any stressful encounters will be met with understanding and assistance from peers and/or managers enables paramedics to externalise their coping through cooperative problem-solving.12,13 This idea matches up with the ‘get things into proportion’ item on the DETCOP subscale [17 p7]. Logically, problems viewed from multiple points of view with the help of input from others are less likely to become overwhelming and more likely to be seen objectively. In short, this study showed that emotional connection in paramedic communities should not be disregarded by organisations. Instead, the natural connections between staff should be seen as a powerful force that can be leveraged to improve capability and wellbeing. 38
Even stronger associations were present when looking at dysfunctional detachment scores. In the same way that emotional connection at work may be seen to bolster coping, it also appears that a lack of it is linked to feelings of social isolation, although the influence of personal factors outside of work cannot be discounted.12,13 Ultimately, paramedics have much to gain by actively seeking and inviting emotional connection with their colleagues.12–14 Reassuringly, the choice to do so rests with each person individually, circumventing any organisational or managerial barriers. It is then up to organisations to decide whether to utilise these connections for the benefit of their workforce and patients or to discount the value of emotional kinship despite a growing body of evidence as to its material advantages.
Recommendations
The findings from this study provide early evidence for paramedic organisations and individuals to cultivate adaptive detachment skills and maximise their sense of workplace membership, influence, needs fulfilment, and emotional connection. Efforts to do so are likely to enhance the coping mechanisms and psychological well-being of all personnel, both within and outside the workplace, while minimising dysfunctional behaviours.
To date, the literature suggests that in healthcare and paramedic settings, coping tends to be person-driven rather than assisted by organisations on a formal level.6,7,12,14 This trend implies room for significant improvement in how organisations support coping. The results from this research provide quantitative evidence that the fulfilment of needs at work is not merely a luxury, but has significant flow-on consequences for paramedics in all areas of their lives. Their responses to stress both at work and in their personal lives are directly linked to – and potentially moulded by – how well their workplace community supports their needs. This finding should be a clarion call to organisations to create better processes for staff – better teaching around effective coping strategies, better organisational responses to incident debriefs and high workloads, and a better culture around mutual support. With these improvements, coping can become more than an individual endeavour enacted in the privacy of each paramedic's personal psyche or siphoned onto friends and family without the benefit of guidance or support. Instead, coping can involve a reciprocal arrangement between paramedics and their organisations: the performance of high-demand patient care in exchange for adequate fulfilment of staff needs, leading to better outcomes all around.
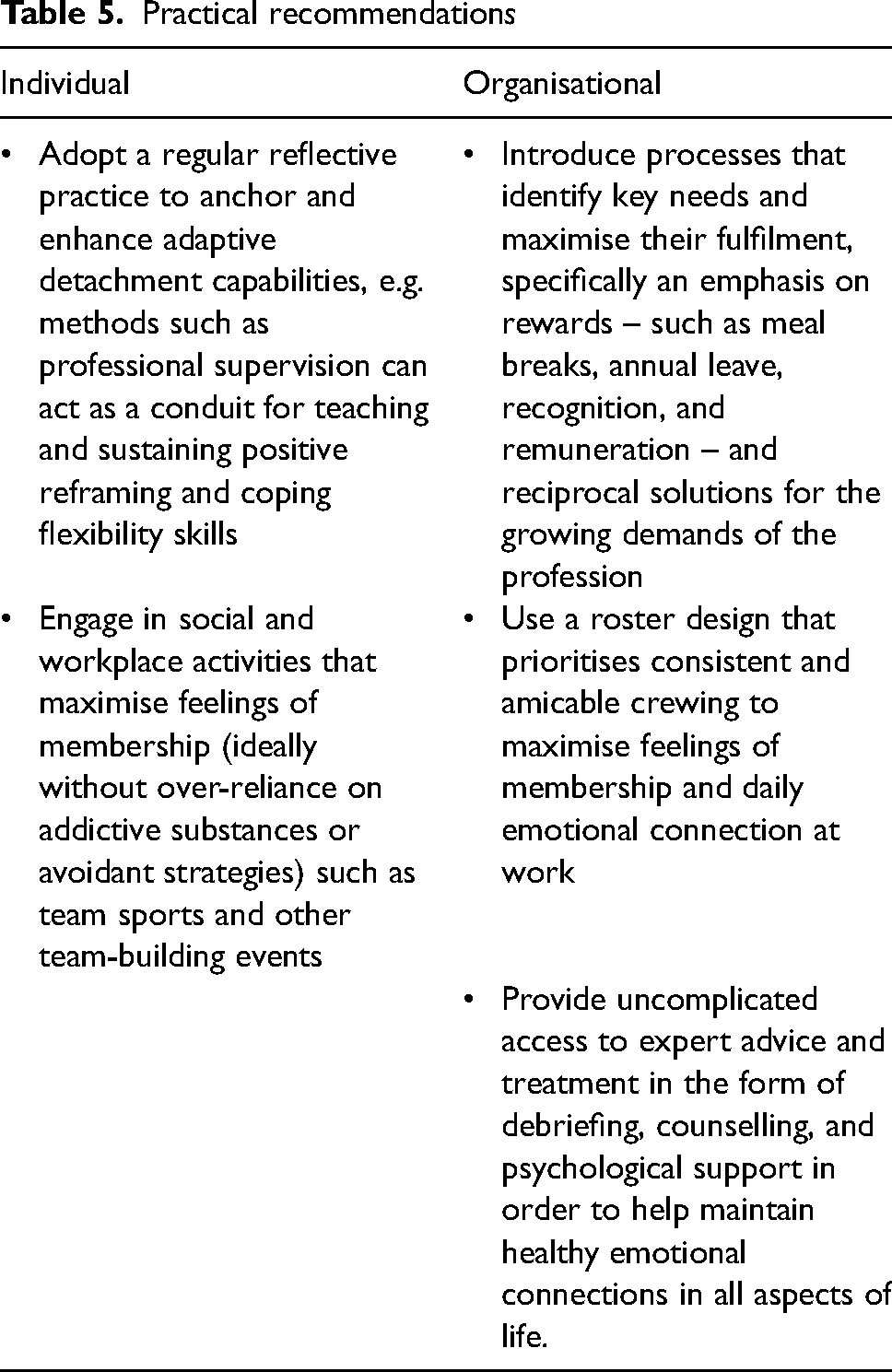
For specific practical recommendations drawn from this discussion and other sources, see Table 5.
Practical recommendations
Limitations
The participants in this study self-selected, implying a pre-existing interest in their own well-being and that of their paramedic colleagues. A more accurate sampling of this paramedic population would include paramedics of all mindsets, including those whose levels of disinterest, scepticism, or dysfunctional detachment might preclude them from engaging voluntarily with such a survey.
Recruitment was based on a convenience sample from an online social media platform. As a result, the sample size may not provide enough power to generalise to the given population. Therefore, results may not adequately represent the experiences and opinions of paramedics in Australia and New Zealand.
Unintentionally, this research took place during the COVID-19 global pandemic. The unique nature of the COVID-19 backdrop means that these participants were not typical of Australian and New Zealand paramedics during normal conditions. 4 Any future studies or reviews would need to take into account the distinctive environment of the COVID-19 pandemic and its potential effects on paramedic coping when using or comparing against the results obtained in this study.
The DETCOP subscale includes almost no items that can be interpreted as positive reframing, arguably compromising its full ability to measure adaptive detachment. An improved scale is warranted, perhaps including the two pertinent items from the Brief COPE Inventory: ‘[I try] to see it in a different light, to make it seem more positive’ and ‘[I look] for something good in what is happening’ [40 p96].
Finally, the nature of ‘work community’ in the BSCS was not specified, so participants may have conceptualised this differently (e.g. shift group vs. frontline workforce vs. larger operational workforce vs. entire organisation). More information around what respondents consider their community would provide a clearer lens of paramedic social connection.
Conclusion
Results from this study suggest that paramedics may be able to improve their ability to manage workplace stressors through appropriately integrated detachment-based and social connection strategies. By engaging with the themes suggested in this article, organisations and individuals have the opportunity to enhance their emotional coping skills and processes based on contemporary research that applies directly and sensitively to paramedics. In a climate of global uncertainty in the aftermath of a pandemic, where frontline emergency and healthcare workers are experiencing ever-growing demands for their services while facing increasing burdens of stress, PTSD, depression, and burnout, any evidence-based methods for improving emotional survival skills may not only preserve careers, but save lives as well.
Supplemental Material
sj-docx-1-pam-10.1177_27536386241306140 - Supplemental material for Sense of community and its relationship to emotional detachment in Australasian paramedics
Supplemental material, sj-docx-1-pam-10.1177_27536386241306140 for Sense of community and its relationship to emotional detachment in Australasian paramedics by Suzanne Hocking and Elizabeth Asbury in Paramedicine
Footnotes
Acknowledgements
Thank you to my supervisors, Dr. Elizabeth Asbury and Alan Wilson. Thank you to Drs. Bornstein and Denckla for their support of this project, the teaching staff in the Master of Professional Practice post-graduate programme at Whitiriea WelTec, the board of the Australasian College of Paramedicine, and all of the paramedics who contributed to this research.
Competing interests
None.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Appendix A
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.