
Abstract
Introduction
Over 700,000 people die by suicide globally each year. 1 The death of someone by suicide often affects the well-being of those emotionally close to or professionally associated with the deceased.2–5 This phenomenon is called exposure to suicide – witnessing or knowing someone who died by suicide. 2 Cerel et al. 2 suggest there is a continuum of survivorship for people impacted by a death to suicide. Those who encounter suicide through the course of their work are characterised as ‘occupationally exposed’ to suicide since they have a ‘professional’ rather than personal relationship with the deceased.
Previous review on occupational exposure to suicide found that research on the effects of the phenomenon usually focused on mental health professionals, such as nurses or psychiatrists. 6 Fewer studies focused on the phenomenon amongst first responders such as police officers, paramedics, and firefighters, who differ from mental health professionals in that they are less likely to have had a prior relationship with the deceased person. 6 First responders do not receive significant training in mental health, are often directly exposed to the traumatic aspects of the suicide scene, and witness families’ raw grief reactions. It is a growing concern as these professionals are increasingly required to respond to mental health calls and suicide scenes.7,8 Exposure to suicide has been correlated with increased risk of burnout, anxiety, depression, posttraumatic stress disorder (PTSD), interpersonal difficulties, and risk for suicide.3,4,9–14 Therefore, considering the lack of research and the impacts associated with the phenomenon, it is valuable to understand the experience of occupational exposure to suicide among first responders.
Higher rates of suicidality have been reported among first responders compared with the general population in most Western countries.12,15–17 Rates of serious suicidal ideation were reported by 10.4% of ambulance personnel in Norway, and suicide attempts were reported by 3.1%. 18 A study of suicide rates in the US between 2009 and 2015, found that 5.2% of deaths among paramedics and firefighters were by suicide, higher than the 2.2% of suicide deaths in matched non-emergency professionals. 17 In Australia, a study utilising data on suicide from the National Coronial Information Service (NCIS) from 2001 until 2017, found that the suicide rate was 14.3 per 100,000 for first responders and 9.8 per 100,000 for other occupations. 19 Another Australian study examined suicide rates over 12 years (2001–2012), finding suicide risk was 1.4 times higher in male first responders, and almost twice as high in female first responders when compared with all other occupational groups. 20
Petrie et al. 19 reported that across the broad professional categories, differences in suicide rate were not significant once age, gender, and year of death were controlled, suggesting that gender and age might explain the apparent elevated rates of suicidal behaviour among first responders – as males, in general, have an increased risk for suicide and first responders are more commonly male. 19 However, in the paramedic subgroups, the increased risk for suicide persisted even when confounding factors variables were controlled, suggesting being a paramedic is an independent risk factor for suicide. Another study in Australia showed that paramedics reported a higher lifetime prevalence of suicidal ideation compared to police officers. 21 These findings suggest that paramedicine is a profession at increased risk for suicide. Yet, few studies have focused on the phenomenon among the paramedic population. 6
The discrepancy in paramedics’ rates of suicide when compared with other first responders raises questions regarding what factors might contribute to this. Previous research has reported a correlation between occupational exposure to suicide, mental health symptoms, relationship problems, and increased suicide among helping professionals including paramedics.3,13 However, these studies do not scrutinise data for each professional category, limiting the conclusions which can be drawn in relation to paramedics. Nelson et al.'s 22 recent qualitative study with paramedics in England who were exposed to suicide in the course of their work found that suicide callouts were experienced as distressing, and participants perceived they had conflicting roles in relation to this work – they had to provide help as a ‘social service’ and take care of the physical health of patients. Furthermore, paramedics felt that the organisation did not acknowledge the personal impacts of suicide exposure on staff, and they bemoaned the lack of guidance on how best to support colleagues impacted by suicide. 22 This research, however, did not explore subjective and personal accounts of paramedics, rather it focused on their views on practical aspects of service provision such as protocols, training, resources, and relationships with other first responders. In-depth data on the subjective experiences of paramedics is needed to better understand how the phenomenon of suicide exposure impacts this occupational group and to improve workplace interventions to limit their subsequent risk of suicide.
This study addresses these gaps by exploring the lived experiences of paramedics who were exposed to suicide in the course of their everyday work in New Zealand.
Methodology and methods
Methodology
This study draws on a qualitative methodology, Interpretative Phenomenological Analysis (IPA), which at its core is focused on understanding lived experience. This methodology reflects the constructivist position that reality is not fixed but is socially constructed, while also focusing on the inner experiences of participants drawing on phenomenology. 23
IPA seeks to make sense of people's subjective experiences of their personal and social world. 24 The goal is to get as close as possible to the lived experiences of participants, generating insights into what it is like to experience the phenomenon from their perspective, the underpinning emotions, and the meaning-making of the experience by the participant. 25 The IPA methodological approach used in this study aligns with that described by Smith et al.. 24 The research project was approved by the Human Research Ethics Committee from the University of Otago (reference 20/111).
Method
Recruitment
Participants were recruited via a University of Otago press statement published in May 2021 and picked up by the media. This statement profiled earlier research and invited first responders interested in participating in the current study to contact the first author. Snowball sampling was also used, with one participant disseminating this invitation through professional networks. All interviews were held in person.
Typical IPA studies focus on ‘homogeneity’ in the experience of a given phenomenon, utilising one single relatively homogeneous purposive sample to achieve this.24–26 Thus, participants were included if: they were retired or active paramedics; and had experienced at least one suicide exposure during their work as paramedics.
Setting and context
To be eligible for the study, participants had to be (or have been) registered paramedics employed by a New Zealand paramedic organisation in a frontline role. For context, there are two paramedic organisations operating in New Zealand: St John Ambulance (SJA), and Wellington Free Ambulance (WFA). SJA covers around 97% of New Zealand's territory, while WFA covers the remainder. 27 To qualify as a registered paramedic in New Zealand requires a Bachelor of Health Science (Paramedicine major) or a comparable international qualification. The number of single-staffed ambulances is relatively high in New Zealand and staff shortages are common.28,29 Since January 2020, paramedics have been regulated under the Health Practitioners Competence Assurance Act 2003, and the industry has had its council (Te Kaunihera Manapou – Paramedic Council). The Council's 2021 Annual Report reported there were 489 registered paramedics in New Zealand. 30
Data collection
Potential participants contacted the lead author who checked for eligibility. After potentially interested participants reviewed the participant information sheet and provided written consent, interviews were scheduled to take place in person in a private room on the university campus. Participants’ willingness to proceed with the interview and its recording were re-checked before it commenced (and all agreed). Interviews lasted between 45 and 60 min. After each interview, participants went through a debriefing procedure conducted by the interviewer and first author. The debriefing procedure included questions about how the participant was feeling after the interview. Information was provided on available services for ongoing support if this was needed.
The semi-structured interview schedule was developed based on the gaps identified by a scoping review of existing studies on paramedics’ exposure to suicide. 6 Questions focused on the following topics: previous training for dealing with suicide; first experience of suicide at work; most distressing experience of suicide on the job; the personal and professional impact of occupational suicide exposure; beliefs about suicide; coping mechanisms; positive outcomes – if any; and personal experiences of suicide. The questions were built to facilitate a ‘conversation with a purpose’ with themes that mainly served as narrative prompts while probing questions were used to elicit further talk in more depth. 24 Following the ideas of Benjamin, 31 the sequence of questions was scheduled to start with benign questions and move gradually toward more confronting material to build rapport and trust within the interview setting. The interview protocol is available in Supplementary File 1. Debriefing and follow-up protocols are available in Supplementary File 2. Interviews were held in person between May and June 2021. Interviews were digitally recorded and transcribed verbatim utilising an online software (temi.com), before being reviewed and checked for accuracy by the researchers.
Data analysis
Analysis was conducted using the framework by Smith.24,25 Interviews were individually analysed and coded using NVivo 12 qualitative software. The research followed Smith and Nizza's 25 suggested four steps for data analysis. The first step involved reading and writing exploratory notes – establishing a first approach to the interview data and making descriptive, linguistic, and conceptual notes. The second step involved formulating ‘experiential notes’. 24 In the experiential notes step, initial comments evolved toward addressing the experience described in each relevant statement. The third step sought connections and involved clustering experiential notes. The last step was compiling a table of ‘experiential themes’. Although Smith 24 suggests not utilising software for these steps, we decided to use NVivo as a tool to aid analysis. The first step was undertaken in NVivo, with the ‘memos’ function used to create exploratory notes. Each code within NVivo was then understood as the experiential notes – referring to the experience of participants within each developing theme. Finally, the experience of each participant was summated into a code book composed of high-level codes and lower-level codes.
The first author coded all the interviews, while the ‘emerging’ themes were discussed in the research team meetings. The initial theme ideas were revised and reworked with codes reorganised as necessary after an agreement was reached through the research team. The final themes were built narratively, focusing on the shared experience between the group of participants, while also paying attention to the divergencies in each individual experience. To preserve the anonymity of participants, identifying information was removed from the transcripts by the researchers, and pseudonyms were used.
Positionality and reflexivity
The lead author conducted all the interviews. He is a male Brazilian psychologist who was living in New Zealand at the time of this research. The first author has a background in clinical practice and research with suicidal clients. The second and third authors are female social scientists with experience in suicide research and qualitative methods. The last author is a female academic psychiatrist.
Results
Participants’ age group and length of service are detailed in Table 1. The sample comprised nine participants (three male, six female), aged from their twenties to their sixties (M = 48 years; IQR = 23.5). All participants self-identified as New Zealand/European ethnicity, and all had at least five years of experience working as paramedics.
Participants pseudonym, age group, and length of service.
Suicide encounters were described by interviewees as part of their routine work. These callouts included attending suicide deaths, life-threatening situations, and managing individuals experiencing suicidal crises. Participants encountered calls related to threatened or attempted suicide more often than instances of deaths by suicide. Yet, all participants believed they did not have enough training to deal with these calls.
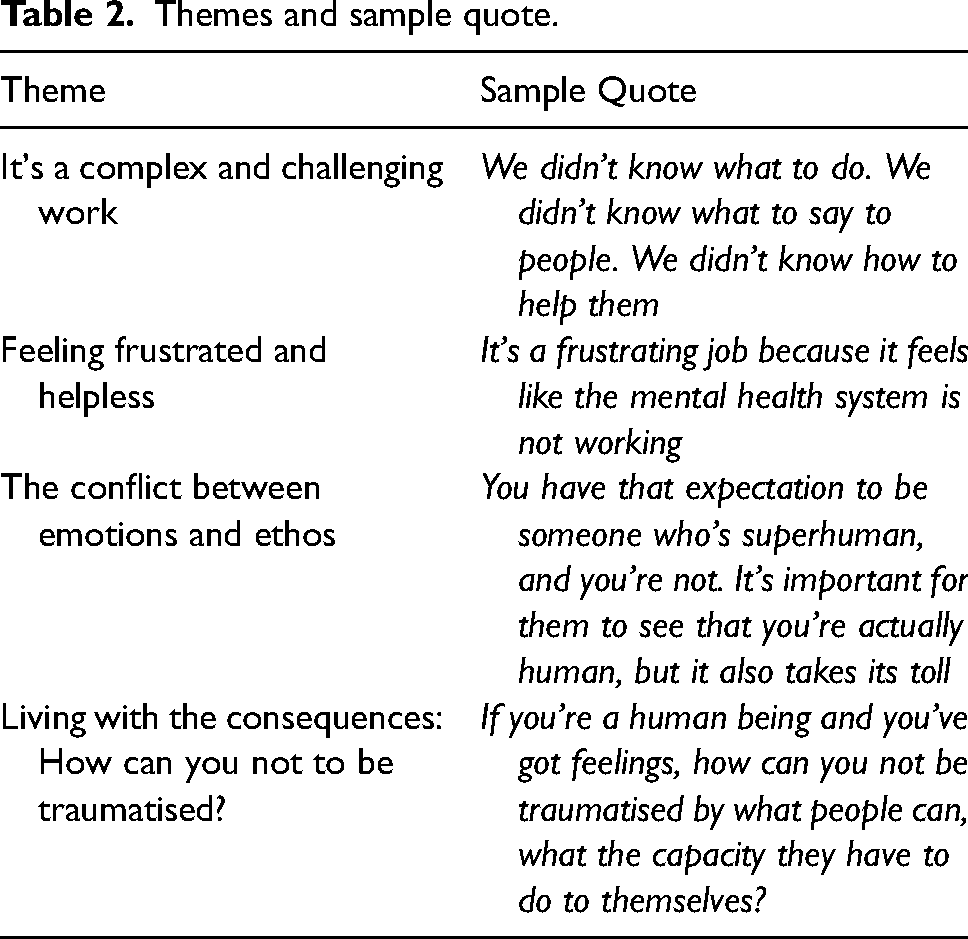
The analysis resulted in four themes in terms of relation to paramedics’ exposure to suicide. (1) It`s complex and challenging work; (2) Feeling frustrated and helpless; (3) The conflict between emotions and ethos; (4) Living with the consequences: How can you not be traumatised? Table 2 provides a summary of the themes with illustrative quotes.
Themes and sample quote.
Its complex and challenging work
Participants reported that attending suicide-related callouts was one of the hardest things they had to do. They often experienced these as a significant challenge to their professional knowledge. They found attending mental health calls often required different skill sets to those they learned in emergency health training. For example, in critical situations, the focus of paramedics is generally to stabilise vital signs and keep the patient alive using protocol-based approaches, whereas mental health situations demand intuitive skills on how best to approach and de-escalate a person in crisis.32,33 For many participants, relying on these more intuitive social skills created anxiety and fear of incompetence: We didn't know what to do. We didn't know what to say to people. We didn't know how to help them […]. We only have an agitated delirium protocol in our “to-do” with the behaviour and how they're behaving. And so, we can treat them that way. But if they are not under that protocol, that pathway, what do we do? (Leila).
Leila felt uncertain about how to provide proper help. She liked having protocols and felt they provided safeguards, giving her confidence that her approach was appropriate to the situation. In their absence, she felt unsure about her ability to help patients experiencing suicidal crises.
In Anne's experience, the fear of showing ‘clinical incompetence’, in front of bystanders added more complexity. Her fear related to being negatively appraised by the public, the media, or the authorities in situations that were likely to attract coronial or other inquiries. These fears not only concerned ‘failing’ the patient but also appearing incompetent in the eyes of others. Anne talked about experiencing ‘impostor syndrome’ in which she felt the paramedic uniform conveyed a level of knowledge that she felt she lacked: [In her first ever call] I was wearing this uniform, and I felt this need to, you know, like I should know all the stuff and I only knew this [much] stuff. So, the kind of expectation from others, but also an expectation on myself (Anne).
Although specific training in interventions with people in suicide crises was considered useful, participants had not universally received such training. The on-duty ‘trial-and-error’ experience was described as the usual way that participants developed the necessary skills to handle suicide-related callouts: You kind of rely on your own knowledge and your own experiences, and what other people have told you on how you should be managing the situations (Ella). You do the job in front of you, you do the best you can, and then you learn to do it better (Ben).
According to Ben, even a ‘failure’ was an opportunity to learn. Perceiving those encounters as an ‘opportunity’ may be interpreted as functioning as a healthy coping mechanism to mitigate the negative feelings associated with a bad outcome. This process can be understood as a positive reframe of their experiences.
Participants’ concerns were predominantly based on the idea that the wrong approach to the subject of suicide with patients could aggravate the crisis. This concern reflected the common misconception that talking about suicide could induce or amplify someone's suicidal behaviour: I do remember initially not knowing really what to do with people [in crisis], how to talk to people that had attempted because… I did not want to talk to them or not touch them. You know, “do I ask them or not?” (Julie). When I'm with someone that's suicidal or threatening, I'm very cautious on what I say… I'm always worried I'm going to say the wrong thing and make it worse (Emma).
Emma went on to talk about how she felt that deficiencies in her training meant she did not know how to communicate with people experiencing mental health crises. This led to her investing time in trying to teach herself these skills. … I went to a suicide that I felt I didn't handle it right, because I didn't have the training. So, then I did some research about talking to people that are suicidal so that I could use it, so, I felt more comfortable (Emma).
It is clear then, that suicide encounters on duty posed a challenge to the professional skills of participants. The lack of training and absence of suicide-related protocols that prescribed the recommended interventions left them dealing with such situations based on their own experiences and knowledge, which they found anxiety-provoking. Some participants coped by accepting each encounter as an opportunity to learn and improve – even when they believed they ‘failed’ – while others embarked on their research to improve and validate their performance in these situations. Besides the challenges to their professional knowledge, suicide encounters also challenged their emotional equanimity, which is discussed below.
Feeling frustrated and helpless
One of the key emotions that arose when participants talked about their work with suicide was the frustration this engendered towards the mental health system. Participants believed they were filling the gaps in a deficient mental health system and, thus were overwhelmed by the frequency and severity of mental health-related crises: We shouldn't be doing this all the time. We shouldn't be going to suicides as frequently as we do (Amanda). The problem is that there's too many people who should be getting help who can't get into the right streams of help. And so, they act out and they end up coming to us, and it's not really our job (Jeff).
Jeff believed that due to the difficulty in accessing help through the ‘right streams’, patients used paramedics as a gateway to gain access to services. Therefore, in his perception, suicide callouts (or at least the ones that did not involve medical intervention) should not be under their job remit but covered by the ‘mental health system’. He thought some people threatened suicide as a way to access the support they needed. He believed that the people experiencing ‘real’ suicide crises were the ones who did not seek help – a common belief about suicidal behaviour that is out of line with suicide prevention practices.
The lack of (perceived) efficiency across the entire health system in providing care for mentally distressed patients was a subject that came through in many of the interviews. For example, Amanda described being not only frustrated with the number of suicides she attended but also with the lack of efficiency across the entire system in providing care for mentally distressed patients: It's a frustrating job, it's a frustrating job because it feels like the mental health system is not working (Amanda).
Participants were often confused that the people they transported to hospital who were experiencing suicidal crises were discharged without any apparent plan in place: You bring them to hospital and then you find out that they've just been discharged and nothing's happened. And so, you just feel broken and let down (Ella). They need to be followed up, and proper things put in place, or they just keep coming round and round (Jeff).
The perception that their suicidal patients were being sent home without support caused frustration and feelings of helplessness to participants, particularly when paramedics attended the same person in subsequent shifts. The volume of suicide-related work was, in part, viewed as a consequence of the lack of mental health resources available for people in crisis, which then led paramedics to become de facto support people to frequent callers – something that they had not always appreciated as being part of their role.
The conflict between emotions and ethos
Overall, the paramedic ethos was seen to encompass being calm, controlled, and effective during emergencies. Participants described some tension between having a public front as a health professional and the private reality of being vulnerable and affected by encounters with suicide: The persona that we project in an emergency in a lot of circumstances is emotionless… (Anne). You have that expectation to be someone who's superhuman, and you're not. It's important for them to see that you're actually human, but it also takes its toll (Leila).
The ‘toll’ that Leila referenced was the emotional distress she often experienced after attending a suicide-related callout. Participants generally believed that retaining emotional control was essential to perform well on the job and exhibiting emotions would be perceived as a threat to their competency. However, suicide scenes by their nature evoked intense emotions that they feared might overwhelm their capacity to compartmentalise feelings: And then there's that fear that sadness is going to get in the way of your clinical ability to do the job, you know. And so that just feels really stressful… Makes me wonder when all of the stuff will get too much, and I won't be able to do the job anymore (Anne).
Anne also attended a traumatic suicide scene, which led her to question her career choice. A few years before the interview, Anne had attended a high-profile suicide in a public space. She stated feeling intense fear of not being able to manage the situation correctly at the scene and being perceived as incompetent by the public during and after the event – as the case attracted the attention of the media. She also felt sadness for the person, especially after learning more about them in the post-event media coverage. All those factors made the situation upsetting and traumatic and triggered existential anxiety about her job. She feared the cumulative emotional distress would eventually overload her capacity to remain in control and would jeopardise her performance. Other participants described similar tensions. The greatest factor contributing to this was the unanticipated disturbing nature of suicide-related events and witnessing the reactions of family members. To manage emotional distress, participants would often detach themselves from the scene they were attending, facing it in a ‘detached-technical approach’ – focused on the procedural aspects of their job: For me, everything's within a box. I didn't know the person before the call came in, and I'll probably never see them again after the call. It's what's happening now that I deal with. And because every job is like that, you can't take them all on board or you don't last very long in your job (Jeff). You're having to do your job, and part of you is trying to rationalize what's going on. And then the other part is ‘I need to be professional. I need to act as though this is normal… you just kind of detach yourself from the situation and put it to the back of your head (Ella). I've learned to… get out of the scene as quick as I can. There's no point in looking and staring. So… They look dead, call it, do your tests if you need to, and then leave the room (Amanda).
These quotes highlight the ‘box-ticking’ approach utilised by participants. The ‘detached-technical approach’ was utilised by participants as a key strategy for maintaining emotional composure during calls and reducing their exposure to the traumatic experience and emotions by controlling the time spent at the scene – a way to not ‘take them all on board’. However, this emotional detachment was difficult to maintain when families were present at the scene, as participants often felt a deep level of empathy for the bereaved family member, sometimes even identifying themselves with the family’ suffering: If it was my daughter [dead] there, then yeah, I know how I'd probably… [I] Can imagine how I [would] feel with it (Julie). The suicide itself, to me, it doesn't have a big effect […] It's the family's reaction to it, the distressed partner or the distressed mother or something. That's what we deal with more than the dead (Jeff).
The shock, despair, and anger experienced by families who had lost a loved one to a suspected suicide could be directed toward paramedics. Leila disclosed how awful it was to deal with the families at scenes where they expected the paramedics to ‘do something’ impossible such as perform successful cardiopulmonary resuscitation (CPR) despite it clearly being too late. In her experience, the desperate hope of loved ones that paramedics revive someone who was deceased increased the distressing nature of the situation. Leila worried that families thought she was not doing her job properly, which upset her even more.
Living with the consequences: how can you not be traumatised?
Participants talked in-depth about the traumatic nature of suicide callouts, their own emotional reactions to these experiences, and the consequences on their mental health and well-being, and their personal lives. For some participants, difficult emotional reactions arose from one single traumatic encounter that they could recall in detail; for others, the emotional toll was a cumulative effect of numerous traumatic encounters with suicide. Talking about these times during the interviews still brought up intense emotions: I can get a bit anxious… Excuse me, I'm having a hot flush at the moment… I can get anxious. I can become [deep breath] tearful (Leila).
Several participants described the tension they experienced between having a public front as a health professional skilled in emergency response and the private reality of being a vulnerable human like anyone else. This apparent dichotomy was explained by Leila: If you're a human being and you've got feelings, how can you not be traumatised by what people can, what the capacity they have to do to themselves? (Leila).
The interviews often revealed the experience of emotional numbness. This phenomenon was previously reported as a frequent characteristic of first responders’ presentations of PTSD, which can be understood as a result of the frequent exposure to trauma and the overuse of emotional control strategies.
34
This process of emotional numbness was described as gradual and cumulative: It's something you become unaware of, that you start to not be human in some ways. You're a robot and you're just not feeling much. It's a weird thing because you can't tell what's happening (Amanda).
Amanda described feeling confused as she started to notice having difficulties in experiencing empathy or finding joy in relationships outside work. Her description of perceiving herself as ‘a robot’ resembles the notion previously described of the paramedic ethos of overly controlled emotions. However, for Amanda, this was related to being exposed to suicide rather than the incorporation of the ethos: When I'm affected by these jobs too much, I'll start losing…feeling empathy, and you go to your family's house and you're not quite [yourself] … They're all the same, and they're finding things fun and happy, but you'd struggle to just stay with them in that space at the time (Amanda).
Due to the cumulative emotional distress, Amanda felt isolated as she was emotionally disconnected from her family and friends. These difficulties led her to ‘lose’ many relationships she had before joining the organisation. Other participants also talked about withdrawing from social interactions as a way to avoid ‘spreading trauma’ to others: [After a suicide exposure] I sort of had just like withdrawing and doing individual activities, cutting myself off. And that's like, what I was saying before about the ‘not wanting to put things on to other people’ as well (Anne). I don't talk to my partner. It's not fair on him, I don't want to re-traumatize someone else (Leila).
Regarding mental health challenges, only Emma and Amanda disclosed that they had formally been diagnosed with a mental health condition (PTSD and generalised anxiety disorder). However, other participants described symptoms that were consistent with anxiety disorders or PTSD such as flashbacks, nightmares, and avoidance of places where the scene occurred: I'm waking up more in the middle of the night, but then with these flashbacks that have been happening for years (Leila). It was only two weeks ago, did I realised that I actually have a little bit of PTSD from it [a suicide scene] (Ella).
It's the images that stick on me (Amanda).
Emma's most traumatic exposure happened on a central road under a bridge in the city, which she thought about every time she drove by. She reported choosing alternative routes when driving the ambulance, without explaining to her colleagues out of fear of being perceived as fragile. I got really bad anxiety after that. Like every time we drove past the bridge, and someone would lean over, I would like, feel really panicking. And I'd just feel anxious driving in the ambulance. I still think about it every day (Emma).
Ella described being very distressed after attending the suicide of someone who stepped in front of a truck. Afterward, she visited a mental health professional, who she recalled telling her this was just a ‘normal’ part of the job. She felt her distress was ‘brushed off into the too hard pile’, thus Ella and other participants were often left questioning the extreme nature of paramedic's work: Nothing prepares you for seeing [retracted]. So those bits, they stay with you and you're like, “that's not normal, we’re not meant to see this” (Ella).
Emma disclosed she had experienced suicidal ideation herself. When asked about the influence of dealing with suicide so frequently and her suicidal thoughts, Emma acknowledged that the job had negatively impacted her mental health but pointed out that paramedics learn how to hide their mental distress due to the stigma that exists in their workplace around suicide and mental illness. Hence, the perceived organisational culture within her workplace also influenced Emma's help-seeking behaviour. She considered that patients in suicidal crises were often judged by professionals as ‘attention seekers’ and had their struggles negated. Therefore, when she experienced distress herself, her concern was that she would be mistreated and invalidated by her colleagues if she sought help, as ‘that's how I'm going to be treated’ (Emma).
Discussion
This study draws attention to how frequently participants were exposed to suicide-related events during their work. Participants felt more challenged by violent death and suicide encounters than most other types of work (e.g., cardiac arrests), finding suicide-related callouts required skills that went beyond the medical emergency skills they had originally been trained for. These encounters also required a high level of emotional control, to which many participants utilised a ‘detached-technical approach’ to compartmentalise their emotions at the scene. Consequently, participants often experienced emotional distress or numbness that affected their social and personal relationships, along with experience of mental health symptoms.
It was common for participants to question the worthiness of attending to people who were suicidal, which was often perceived as a waste of ambulance time and resources. Paramedics saw themselves as filling a gap in the health system. However, the volume of suicide events and the frequency of re-presentations left participants feeling they made little ‘real’ contribution to addressing people's distress. This perception of the ‘failure’ of the health system and the challenge suicidal callouts pose to professional skills was also reported by previous research internationally and in New Zealand, which highlights how these factors can lead paramedics to feel frustrated and to question their professional knowledge.7,35
Besides the challenges that suicide calls put to professionals’ feeling of competency; participants often felt challenged by the lack of opportunity for tangible ‘action’ that these situations provided. Medical emergencies that require technical procedures to be performed, such as cardiac events, are often accompanied by strong positive feelings – as they validate the professional's skills – whereas mental health calls can put the paramedic in a position as a passive witness of the ongoing emotional distress. 36 Moreover, the use of technical skills is also a way paramedics may cope with the stress of the job, as performing interventions keeps them ‘distracted’ from the emotions that might otherwise become overwhelming. 36 Participants often felt that suicide calls were more emotionally intense, and it was harder to maintain emotional control – which could be partially explained by the lack of ‘action’ to emotionally distract themselves. They often felt unprepared to care for people in mental health crises, reflecting the findings of previous research.33,37,38 This unpreparedness arises from the belief that mental health care was out of their scope of expertise, as these patients did not require the same degree of essential physical medical care, but rather empathy, reflective listening, or educative orientation. 37
In a survey of NZ first responders, most paramedics reported struggling to keep up with the demand of mental health and suicide-related emergencies, finding the work challenging and frustrating. Fifty-nine percent of ambulance staff said they had insufficient mental health training, and a significant minority (21%) said they often felt unsafe during such work.7,8 Besides the emotional aspect, another risk is that the more a job evokes frustration, the more likely it will be perceived as unworthy of the responder's time. As other authors argue, the emotional aspects of paramedic work – that is, whether staff feels fulfilled afterward – can directly affect attitudes towards suicide-related work. 39
Participants were of the view they would benefit from better training and the provision of protocols related to suicide callouts. The absence of protocols on how best to manage suicide calls made paramedics feel more individually responsible for the decision-making – what to do, where to take the patient, and they felt more personally responsible for the outcomes. Of course, the development of a protocol to be applied by paramedics when approaching suicide situations is challenging, as these involve a wide range of different scenarios. A study in Iran 40 has developed and tested a protocol for paramedics working with suicide. Such models could be useful as concise guides to support paramedics’ work to evaluate the risk of suicide while providing emotional support to patients.
Although a high work intensity is a normal part of a paramedic's job – and often even sought out by those who choose the profession – it is clear that the emotional interpersonal difficulties experienced by participants were often not considered. 41 While the job was seen as having intrinsic value in providing help to others, participants were unprepared for the emotional intensity of the job and the effects it had on their mental health. Emotional labour is a concept frequently associated with first responders, referring to their need to maintain professional posture in the face of traumatic situations, and the distress that might arise from them.42–45 The suppression of distressing emotions has previously been shown to restrict the trauma processing abilities of first responders, contributing to mental health consequences such as PTSD. 44
Emotional labour is the suppression of emotions that are not aligned with the organisation's expectation, replacing those emotional expressions with feelings that fall under the organisation's rules for the effective and efficient completion of tasks. 46 The definition encompasses two strategies, surface acting – hiding the feelings that are unsuitable and faking inauthentic ones considered more acceptable – and deep acting – the work to change personal feelings to align with the organisation's expectations.46,47
Previous research has found paramedics considered emotional labour helpful and important to their work performance. 42 In the sense of deep acting, paramedics recognised the need to maintain an emotional distance between themselves and the patients; viewing the patient as an object rather than a person was one strategy used to maintain emotional control. 42 But there may also be costs to emotional labour. The present study suggests that emotional labour may lead to difficulties in paramedics’ personal lives. The inability to experience positive emotions or express them towards a partner has been reported in other research to lead to diminished quality in intimate relationships. 48 Furthermore, other studies have shown that relationship difficulties for first responders exposed to trauma can increase distress and risk for suicide.12,49
Paramedics have several of the key risk exposures for work-related suicide: Psychosocial exposures, exposure to trauma on the job; access to means of suicide through work; and potentially, adverse experiences arising from work-related injury or illness (or mental distress). 50 Therefore, it is important that workplace mental health interventions acknowledge that work conditions can influence suicidal behaviour and the risk at the individual level. 50 Taken together, this suggests organisations need to consider the wider-reaching impacts of first responders’ exposure to suicide on the job.
Strengths and limitations
This study makes several original contributions to the field of occupational exposure to suicide among first responders. To the best of our knowledge, this is the first study utilising IPA to explore the lived experiences of paramedics regarding suicide exposure. Lived experiences provide unique insights by including the perspective of first-hand accounts of the emotional toll, the meaning-making, and the impacts of the phenomenon of occupational suicide exposure. Thus, the present research provides insights that are contextualised in the subjective reality of being a paramedic.
In terms of limitations, as a Brazilian-born psychologist, the interviewer was a foreigner/outsider both in New Zealand and to the paramedic profession. On one hand, this may have provided participants more comfort in explaining their experiences to an outsider without apparent preconceptions about New Zealand or paramedic culture. On the other, cultural aspects may have influenced the lead researcher's understanding of the accounts (e.g., as a non-native English speaker he may have missed some of the nuances while navigating the flexible nature of semi-structured interviews). His previous experience with suicide as both a researcher and psychologist may have also biased his interpretation of the participants’ experiences. Furthermore, the research team did not include a paramedic, which may also have influenced interpretations.
Unfortunately, the sampling method was unsuccessful at recruiting paramedics who identified as Māori (the First Nation people of New Zealand) paramedics. This may have been partly due to the underrepresentation of Māori in ambulance services, and also that Māori participants may have been less inclined to engage with the lead researcher as a ‘double foreigner’. Māori cultural identity is highly likely to influence the way people make sense of the experience of exposure to suicide, considering factors such as Tikanga (Māori concept of values, culture, and customs), identification and kinship, and is of critical importance in the New Zealand context.
The last limitation of the research concerns the generalisability of the findings. IPA is based on an epistemological perspective in which the scientific endeavour is not to test hypotheses and generalise the findings to a population, but rather the focus is on gaining insights with the uniqueness of the experience of a given individual in a contextualised time and circumstance. 25 Therefore, while the findings from this study may not be generalisable to the wider paramedics’ population or other occupational groups, it still contributes to the understanding of the experiences of paramedics who work and are exposed to suicide as part of their job. These insights can inform the community who advocate for increased awareness of paramedics’ mental health and well-being.
Questions that remain to be addressed in future research include the relationship between organisational culture and the impacts of trauma among paramedics (e.g., the role of emotional labour and coping mechanisms). Ongoing research should address the phenomenon of suicide exposure amongst other professional categories (e.g., firefighters, emergency personnel, coroners); groups for whom little research has also been conducted in this context.
Conclusion
The research explored the phenomenon of occupational exposure to suicide among paramedics. The findings demonstrate how suicide exposure was experienced as a major challenge for paramedics, and affected interpersonal relationships, and mental well-being.
Supplemental Material
sj-docx-1-pam-10.1177_27536386241283986 - Supplemental material for ‘How can you not be traumatised’: Experience of paramedics occupationally exposed to suicide
Supplemental material, sj-docx-1-pam-10.1177_27536386241283986 for ‘How can you not be traumatised’: Experience of paramedics occupationally exposed to suicide by Renan Lopes de Lyra, Sarah K. McKenzie, Gabrielle Jenkin and Susanna Every-Palmer in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386241283986 - Supplemental material for ‘How can you not be traumatised’: Experience of paramedics occupationally exposed to suicide
Supplemental material, sj-docx-2-pam-10.1177_27536386241283986 for ‘How can you not be traumatised’: Experience of paramedics occupationally exposed to suicide by Renan Lopes de Lyra, Sarah K. McKenzie, Gabrielle Jenkin and Susanna Every-Palmer in Paramedicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a University of Otago Doctoral Scholarship.
University of Otago, (grant number Postgrad Publishing Bursary).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.