
Abstract
Paramedicine is a constantly evolving field, with paramedic education programmes needing to be adaptable to keep up with changes in the scope of practice. Regulatory frameworks are crucial in guiding university programmes, providing students with the knowledge, skills, and professional attributes necessary to be safe and competent practitioners. This study aimed to identify variations in regulatory structures, the factors that influence those variations, and how they influence curricula. A descriptive-comparative approach was taken to examine paramedic accreditation processes, curricula, and syllabi across five countries using a modified Brady's model and extending the Comparative Education model. The findings suggest that paramedic services, regulatory authorities, and tertiary institutions must adopt a multilateral approach to recognise paramedicine's evolving scope of practice. All three stakeholders are responsible for aligning regulatory frameworks with industry needs and providing curricula guidance to tertiary institutions. This approach will enable paramedic education programmes to remain relevant and adaptable to changes in the field, ensuring that graduates are safe and competent practitioners. In conclusion, this study highlights the need for a collaborative effort between paramedic services, regulatory authorities, and tertiary institutions to recognise paramedicine's evolving scope of practice. The need for recognition of this evolution in both regulatory frameworks and curricula is a significant concern, and a multilateral approach is required to address this issue. This study provides valuable insights into the factors that influence variations in regulatory structures and their influence on curricula.
Keywords
Introduction
Paramedicine is an ever-evolving profession and requires adaptable education programmes that align with the industry's changing scope of practice. There are different models of care of paramedic practice internationally, the Anglo-American model, the Franco-German model, and the hybrid models. 1 Despite the similarities in paramedic scopes of practice in the five core countries of the Anglosphere and South Africa as the sixth country outside of the Anglosphere, variations in educational requirements and regulatory frameworks exist internationally, with considerable diversity. 2 South Africa was included for its alignment with the models of care, scopes of practice, and education found in Australia and the USA. Achieving standardised scopes of practice and registration across different countries has been the vision of many paramedic organisations.3–5 Yet, the differing regulatory frameworks and education of paramedics globally, along with variations of curricula within countries themselves, complicate any standardisation attempts. Consequently, regulatory frameworks guiding paramedicine curricula must be contextualised within the nation, and factors influencing the variations in approach and how they influence curricula must be considered.
This paper aims to synthesise regulatory structures and the factors that influence curricula. The paper envisions a future of international models of paramedic education, regulation, and practice. To achieve this, the regulatory frameworks that guide paramedicine curricula must be reviewed and aligned with industry needs while advising tertiary institutions. This will require a multilateral approach involving paramedic services, regulatory authorities, and tertiary institutions.
The differences in regulatory frameworks and education of paramedics globally and variations of curricula within countries themselves make it challenging to achieve standardised scopes of practice and registration across different countries. In addition, the global variations in paramedicine education qualifications range from 3- to 4-year baccalaureate degrees, 1-year certificates, and 2-year diplomas to single non-award in-house programmes run over a certain amount of time. Although entry-level degree programmes exhibit variations in nomenclature, duration, and curriculum, there needs to be conformity in national and international universal education standards. This can be attributed to the diverse regulatory frameworks within the educational sector.
Furthermore, paramedicine is regulated differently across the Anglosphere, with some countries introducing statutory regulations ensuring safe and competent paramedics. In contrast, others have no regulation or regulatory mechanisms from governments. For example, the Australian Health Practitioner Regulation Agency (Ahpra) regulates paramedics in Australia, while the Health and Care Professions Council (HCPC) regulates paramedics in the United Kingdom.
Given the ability of students to migrate to become paramedics in different countries, the various regulatory and education frameworks may pose a barrier for graduates. 6 Thus, reviewing the paramedicine regulatory frameworks and their influence on curricula requires consideration of national and international perspectives to ensure robust guidance for decision-makers of regulatory frameworks and tertiary institutions.
This research paper aims to delineate the differences in regulatory structures and the underlying factors contributing to such variations and analyse their impact on paramedic curricula. The paper envisions a prospective scenario where paramedic education, regulation, and practice can be harmonised internationally by adopting standardised models. Achieving this vision necessitates a collaborative and multilateral effort among paramedic services, regulatory authorities, and tertiary institutions.
Methodology
An in-depth analysis of international paramedic regulatory frameworks and education is crucial to understand the variations in regulatory structures, the factors influencing these variations, and their impact on curricula. This review of curriculum comparison aligns with the report undertaken by Willis et al. (2009), who identified the need for national and international research and grey literature on contemporary developments in paramedic education that provide best practice models for the twenty-first century. 7 We conducted a content analysis of international documents to achieve this aim, explicitly focusing on the five core countries in the Anglosphere (Australia, New Zealand, the United Kingdom, Canada, and the United States) and South Africa. These countries were selected due to their developed status, close cultural, diplomatic, educational, and military links, and similar paramedic models of care.
We adopted a descriptive-comparative approach, utilising a modified version of Brady's model and a comparative education approach. The first three stages of Brady's model – description, interpretation, and juxtaposition – were applied. The Brady Model provides a systematic and comprehensive approach to analysing paramedicine curriculums. This structured framework ensures a thorough examination of university programmes, offering valuable insights into the nuanced landscape of paramedicine education. The comparative education model involves analysing and comparing educational systems across several countries and has been successfully utilised in nursing education comparative research. 8
In the description stage, we gathered information on paramedic curricula across the six countries by reviewing grey literature such as university handbooks, accreditation documents, and curriculum renewal documents. We also reviewed documents from government bodies, professional organisations, and statutory bodies related to the six countries to find comparable documents that linked paramedic curricula internationally. In the interpretation stage, we collated and charted the collected information from each of the six countries in tables and figures. The third stage, modified from Brady's model, involved an in-depth comparison of regulatory frameworks and education across each country. This stage allowed for a thorough analysis and comparison of the regulatory frameworks and education of paramedics across different countries and is discussed in detail in this paper.
Comparative education is an effective evaluative tool in creating educational programmes as it takes the strengths of one system and incorporates them into another. 9 Comparative education has been used internationally in nursing education to identify dynamic educational systems and comparisons and disparities in education models, similar to paramedicine. 10 In this study, the first three stages of Brady's model are incorporated into the findings section, while the fourth stage is represented in the recommendations section. The modified version of Brady's model and comparative education approach in this study provides a valuable framework for future research in paramedic education.
Findings
Australian context
Regulatory framework
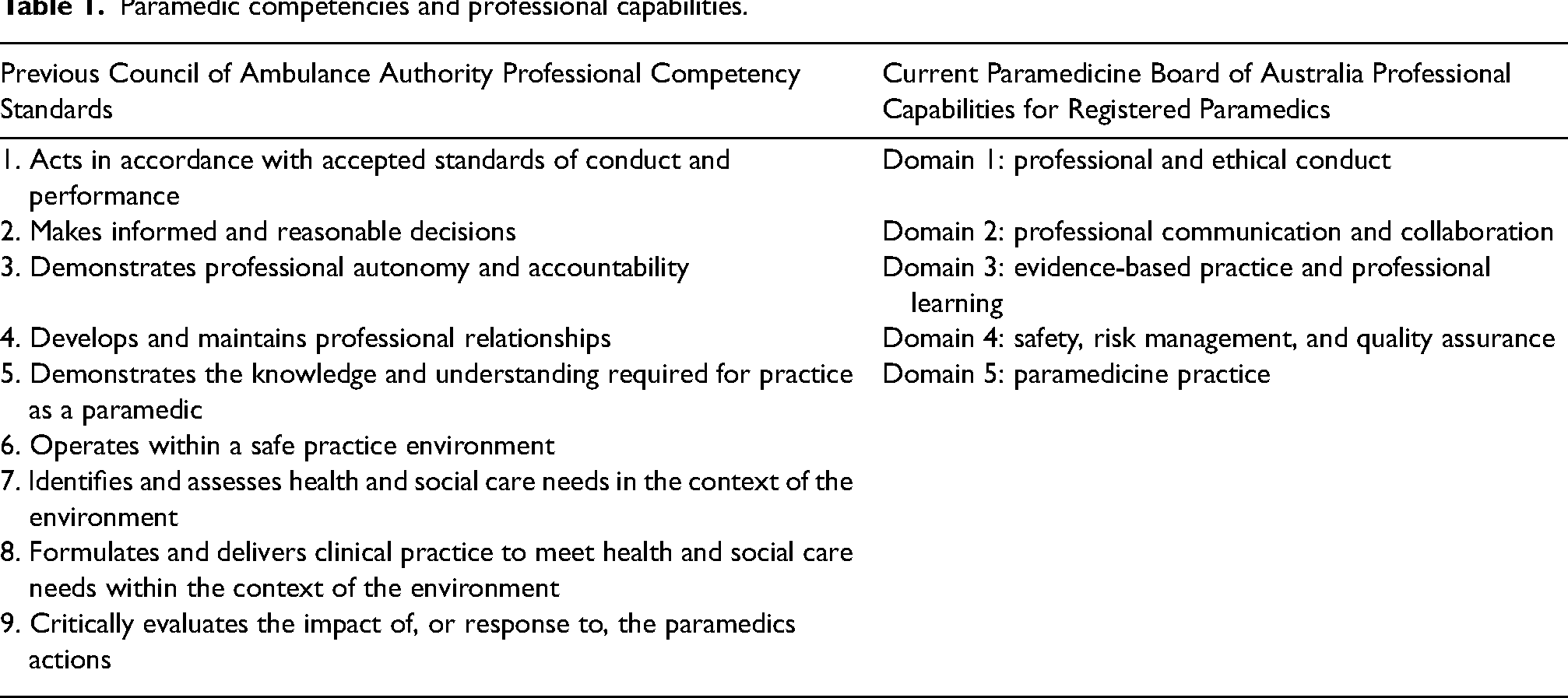
In 2018, paramedicine became a nationally regulated profession, the fifteenth health profession regulated by the Australian Health Practitioner Regulation Agency (Ahpra), with paramedics registered with the Paramedicine Board of Australia (PBA). Like the Council of Ambulance Authorities, the PBA has published standards expected of registered paramedics and has implemented them as professional capabilities for registered paramedics. The competency standards and professional capabilities define the core competence required for paramedic practice (Table 1).11,12 National registration bodies such as the PBA work to improve patient protection by ensuring only those paramedics working within a scope of practice are registered; just as important is the professional identity registration provides paramedics. 13
Paramedic competencies and professional capabilities.
Education
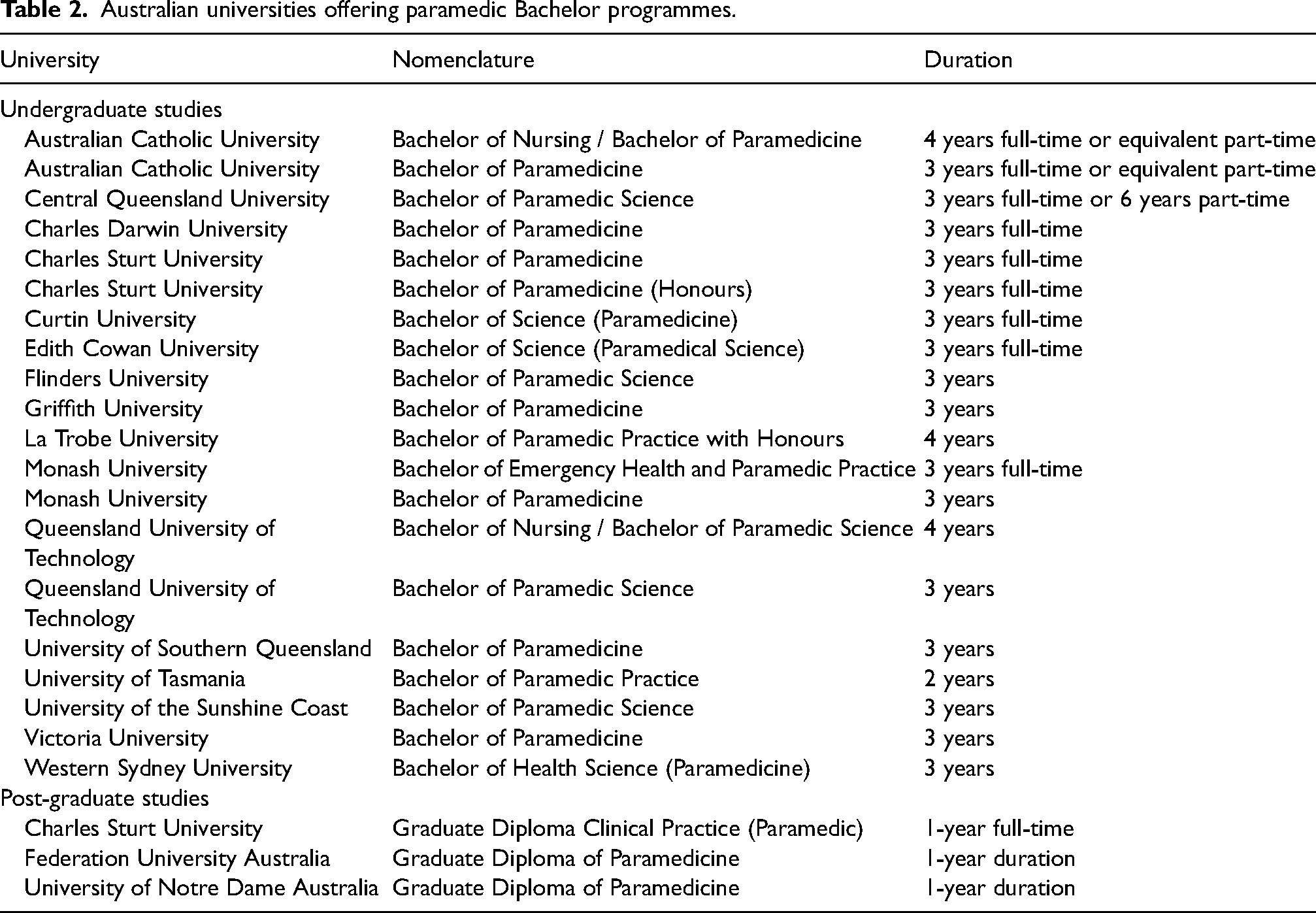
A search was conducted on the Australian Health Practitioner Regulation Agency (Ahpra) website for Australian undergraduate pre-registration paramedicine programmes leading to registration. 14 Twenty-three programmes of study revealed entry-level paramedic qualifications with varying nomenclatures and study durations available across 19 universities. There were 10 universities with the nomenclature containing Paramedic, Paramedicine or Practice, and seven qualifications had terminology that included Science, Paramedic Science or Health Science. Two universities’ qualifications were dual degrees with nursing, while there were five qualifications at either an Honours or post-graduate Australian Qualifications Framework (AQF level), Table 2.
Australian universities offering paramedic Bachelor programmes.
New Zealand context
Regulatory framework
The regulation of paramedicine as a profession is crucial to ensuring that the highest standards of practice and care are upheld. In New Zealand, the Health Practitioners Competence Assurance (HPCA) Act (2003) was introduced to regulate healthcare professions, including paramedicine. 15 With effect from 1 January 2020, paramedics were officially recognised and registered under the updated HPCA Act (2003). 16 As part of this process, the paramedic council in New Zealand, Te Kaunihera Manapou, has been established to develop the scope of practice for paramedics under the Act.
The Te Kaunihera Manapou has embraced the clinical competence standards developed by the PBA. 17 This commendable decision highlights the importance of international collaboration and standardisation in regulating paramedicine. This signifies an acknowledgement of the need for a unified effort to ensure that paramedicine's regulatory practices remain up-to-date with the latest developments and advancements in the field. 17 By adopting an integrated approach, it will be possible to establish a consistent framework for regulating paramedicine across the globe, thereby ensuring that the profession can provide safe, effective, and efficient care to patients worldwide.
In light of these developments, it is important to recognise the significance of effectively regulating paramedicine to promote public safety and trust. As paramedicine continues to evolve and expand, the role of regulatory bodies like Te Kaunihera Manapou in maintaining education standards and fostering innovation will be essential to ensure that the profession continues providing high-quality care to needy patients.
Education
The fundamental objective of the Te Kaunihera Manapou Paramedic Council is to ensure the protection of public safety. To fulfil this goal, as mandated by the Health Practitioners Competence Assurance Act 2003, the council regulates paramedic qualifications and establishes educational benchmarks for institutions that offer paramedic programmes. 17 Auckland University of Technology and Whitireia New Zealand have been granted the status of authorised providers of the Bachelor of Health Science in Paramedicine. This privilege was valid until March 2022.
The United Kingdom context
Regulatory framework
The United Kingdom (UK) National Health Service (NHS) is accountable for monitoring and governing ambulance services. The NHS is the central governing authority for ambulance services in implementing its national health policy. 18 Paramedics in the UK are regulated by the HCPC and have been registered with the HCPC longer than their counterparts in Australia. Nonetheless, paramedics in the UK have yet to embrace university-based education fully.
In the UK, paramedics must be registered with the HCPC, which ensures that paramedics meet the required standards of proficiency and conduct. HCPC maintains a register of paramedics to protect the public by ensuring that only competent and ethical practitioners provide healthcare services. 19
Education
Within the United Kingdom (UK) paramedic scene, the professional body, the College of Paramedics, has been a strong supporter and reformer for changes in education that evolve when there are changes to the delivery model for paramedicine. 19 Initially, Paramedic education in the UK involved in-house, apprenticeship-style training. As an integral component of the National Health Service reforms, there was a paradigm shift in the educational training of paramedics, which transitioned towards a more academic orientation through establishing university-based undergraduate programmes. 20 In reaction to the displacement of short-course service-delivered training programmes by baccalaureate programmes, the College of Paramedics created a paramedic curriculum guide that offered higher education institutions a comprehensive model for developing paramedic students and a consistent curriculum framework.
The standardised approach to paramedic education was developed in response to the changing scope of paramedics’ practice, allowing students the clinical judgement skills to manage patients safely and provide the confidence and independence to be competent as new practitioners. 21 Achieving standardised content delivered across all higher education institutions in the United Kingdom, the following are fields of study recognised by the College of Paramedics: Physical Sciences, Life Sciences, Social, Health and Behavioural Sciences, Clinical Sciences, Ethics and Law, Patient Assessment, Care Delivery, Leadership Attributes, Public Health and Wellbeing, all of these domains supported by Evidence-Based Practice and Research (Figure 1). 21

UK curriculum model.
The Canadian context
Regulatory framework
Provincial authorities oversee paramedic registration and regulation in Canada. The Paramedic Association of Canada (PAC) had developed the National Occupational Competency Profile (NOCP) to establish a standardised framework for paramedicine. This document outlined the necessary competencies and tasks for paramedics at different clinical levels. The NOCP served as a professional consensus and provides a uniform reference for Canadian jurisdictions. 22 Each province has its own regulatory body responsible for ensuring that paramedics meet the required standards of practice and conduct. In addition, provincial paramedic regulatory bodies determine the scope of practice for paramedics within their respective jurisdictions.
In Canada, provincial authorities empower paramedic regulators to grant registration, licensure, or certification, allowing individuals to practice as paramedics. The specific requirements and standards for regulation, registration, licensing, and certification vary across provincial jurisdictions.
As of 2023, the NOCP has been replaced by the National Occupational Standard for Paramedics (NOSP), managed in partnership with the CSA Group. This new standard is developed following accredited processes established by the Standards Council of Canada, providing updated guidelines for paramedic practice in Canada.
Paramedics in Canada operate under two distinct regulatory models: self-regulated or government-regulated. Provinces such as Alberta, Saskatchewan, Manitoba, Nova Scotia, and New Brunswick follow a self-regulated approach. Meanwhile, British Columbia, Ontario, Quebec, Prince Edward Island, and Newfoundland and Labrador adhere to government regulation. Paramedics in the Territories are not yet subject to regulation. 22
The NOSP emerges as a vital framework. This innovative system establishes a standardised approach to paramedicine practice across Canada, delineating competencies and tasks expected at different clinical expertise levels. The NOSP becomes a cornerstone, ensuring a consistent standard of care for all Canadians, irrespective of their location, by setting clear performance expectations for paramedics.
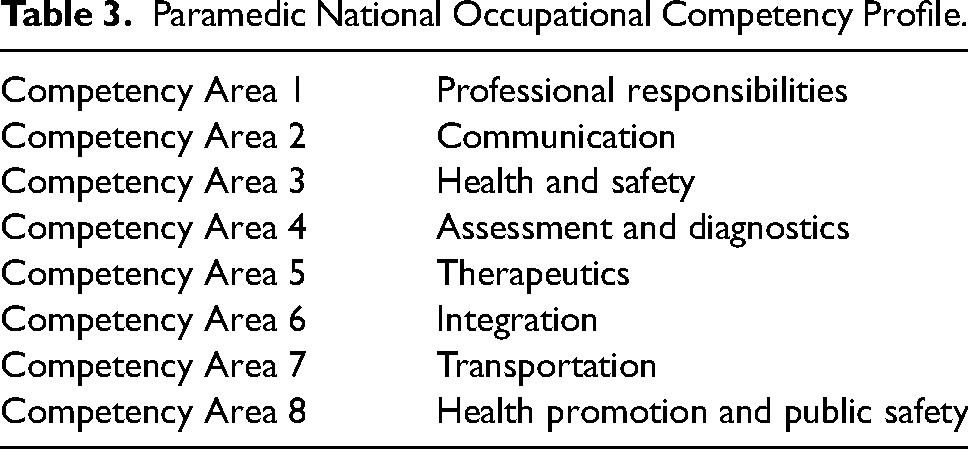
Crucially, the NOSP doesn't just exist in isolation; it continues to play a pivotal role as a guiding reference for regulatory bodies. These bodies will leverage the NOSP to shape educational programmes, certification standards, and licensure requirements, aligning them with the outlined competencies. Consequently, the NOSP becomes instrumental in harmonising paramedic education and practice throughout Canada, guaranteeing that all paramedics adhere to the same standards of excellence and professionalism, Table 3.
Paramedic National Occupational Competency Profile.
Education
In Canada, the education of paramedics is primarily overseen at the provincial level by the regulatory bodies responsible for ensuring that paramedics meet the required standards of practice and conduct. 23 While there has yet to be a standardised approach to the education of paramedics across Canada, most provinces have implemented a competency-based approach to education. This approach ensures that paramedics possess the knowledge, skills, and abilities to provide safe and effective patient care.
The educational requirements for paramedics vary depending on the level of practice. 23 Entry-level paramedics typically complete a diploma or certificate programme at a community college or technical institute. Advanced care paramedics usually have a higher level of education and may have completed a bachelor's degree or advanced diploma in paramedicine.
The United States of America context
Regulatory framework
The regulatory landscape governing paramedics in the United States is intricate and multifaceted, with oversight extending from both federal and state levels. While the National Highway Traffic Safety Administration (NHTSA) assumes a pivotal role in establishing and promoting nationwide standards for emergency medical service (EMS) systems, encompassing paramedic education and certification, it's important to note that NHTSA's influence lies more in the realm of guidance and coordination rather than direct regulatory control. 24 NHTSA primarily operates by convening experts and providing financial support through federal grants.
A significant milestone in this domain occurred in 2000 when NHTSA unveiled the EMS Education Agenda of the Future: A Systems Approach, which introduced five foundational pillars for EMS development. 25 These pillars comprise the EMS Core Content, EMS Scope of Practice, EMS Education Standards, National Certification, and Paramedic Program Accreditation. Among these, the National Registry of Emergency Medical Technicians (NREMT) has emerged as a crucial player, assuming responsibility for certifying entry-level competence for EMS practitioners across all levels, including paramedics. With over 500,000 registered clinicians under its purview, the NREMT has solidified its role in this capacity. 25 It's worth clarifying that neither the NREMT nor the National Association of Emergency Medical Technicians (NAEMT) have pursued licensure endeavours. The authority to grant licensure rests exclusively with individual state EMS agencies.
Addressing the variability in scope of practice across states, the EMS Compact emerges as a noteworthy development. This Compact encompasses more than half of all states, allowing for licensure reciprocity among participating states. This means that paramedics with licensure in one state can seamlessly practice in another state within the Compact, fostering mobility and continuity of care.
Education
In the past, the education of paramedics in the US has faced significant challenges, as highlighted in the review of the literature. This led to a concerted effort to standardise the training curriculum, involving collaboration among diverse stakeholders, including federal and private EMS authorities and legislative bodies. 26 This evolution reflects a commitment to enhancing the paramedic profession and is mirrored in the complexity of the curriculum, mirroring the multifaceted nature of paramedic practice within the country.
The process of consolidating 500 distinct training programmes into a unified and standardised curriculum has been a necessary endeavour. This transformation emerged from meaningful cross-disciplinary discussions, a fruitful collaboration involving both public and private EMS authorities, and legislative modifications. The newly introduced areas of study within paramedic education in the United States are anticipated to elevate the standards of the profession. The intricacy of the curriculum documents mirrors the intricacies of the scope of practice across the nation. Guidelines for these scopes of practice are established within legal frameworks, regulatory statutes, and policy documents. While certain states incorporate precise language within their legal, regulatory, or policy documents, others adopt a different approach known as ‘incorporation by reference’ by referring to a separate document. 26
The Practice Model plays a pivotal role in establishing a mechanism to achieve consistency in EMS scopes of practice among different states.27,28 Through this model, the skills and responsibilities undertaken by paramedics in the United States are defined and aligned with specific certifications and educational prerequisites. It is important to highlight the role of the Commission on the Accreditation of EMS Programs (CoAEMSP) in this context. CoAEMSP holds the responsibility of verifying and validating paramedic programmes across all states within the US, including those within the US military. 29 This accreditation body serves as the benchmark for paramedic programmes to adhere to, superseding the influence of NHTSA. 26 For a paramedic student to attain certification and eventual licensure within a state, it is imperative that they graduate from a programme approved by CoAEMSP, or from one that has received an approved letter of intent from CoAEMSP.
The review also identified that this curriculum for courses or study programmes was typically 1000–1200 h. Table 4 identifies the domains of study offered in the USA and South Africa. The literature identified that the USA EMS had influenced other countries, such as the United Kingdom, South Africa, and the Middle East. In particular, South Africa mirrored the United States EMS.
USA and South African national curriculum (National Highway Traffic Safety Administration, 2009).
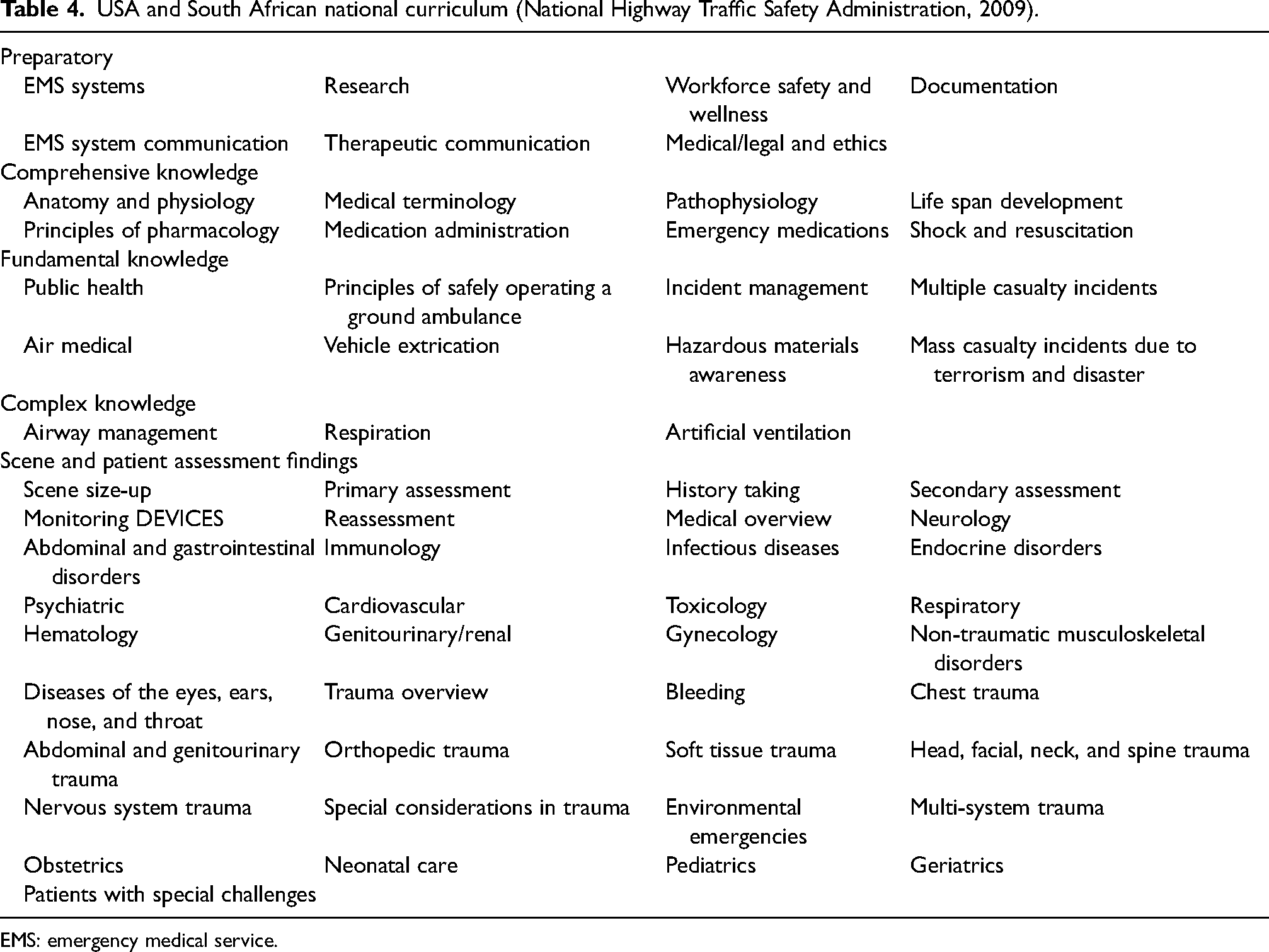
EMS: emergency medical service.
The South African context
Regulatory framework
During the late 1980s in South Africa, the registration of paramedics was a pivotal development that facilitated the recognition of paramedicine as a legitimate healthcare profession. The Health Professions Council of South Africa (HPCSA) established the Professional Board for Emergency Care (PBEC), which mandated that all paramedics be registered before practising in the country.
However, despite this progress, the global evolution of paramedicine has also impacted South Africa. The changing nature of paramedicine and advancements in technology and clinical practice has necessitated ongoing education and training for paramedics to remain current and competent. As a result, South Africa, like other countries, has had to continually adapt its paramedic education and certification programmes to meet the evolving demands of the profession. 30
Over the past three decades, paramedic education in South Africa has progressed from short-course training to undergraduate university qualifications, as supported by the National Emergency Care Education and Training (NECET) policy. This policy, in turn, seeks to advance the transformation of Paramedicine and to provide clinical practice guidelines to ensure quality patient care in South Africa, as evidenced by the work of Sobuwa and Christopher (2019).
In South Africa, the scope of practice for paramedics aligns with their educational framework, which includes different levels of clinicians. The amalgamation of clinical levels comprises five distinct scopes of personnel practice, corresponding to the mix of short-course and higher education qualifications. 30 As with other Western countries, the changing demands on the healthcare system and the evolving roles of Paramedicine and the medical evidence supporting clinical care necessitate the educational framework to follow these scopes of practice.
Education
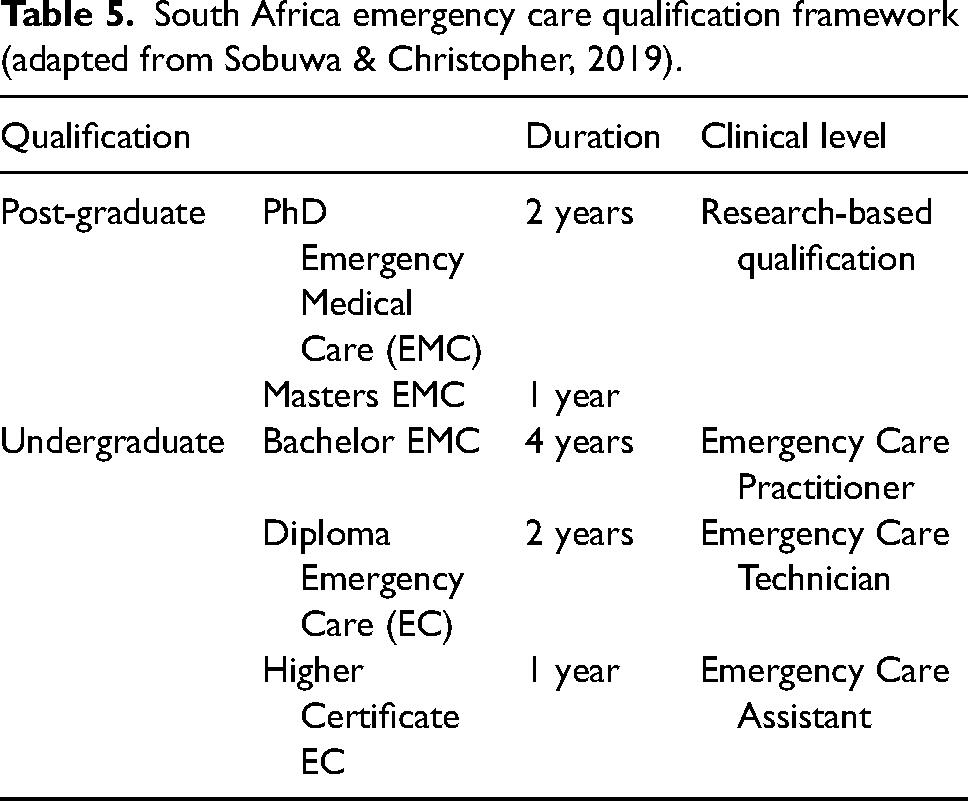
The South African qualifications authority registers paramedics programmes at a Bachelor's degree level. This follows a three-tier approach to the education of paramedics in South Africa. The National Qualifications Sub-Framework for South African paramedics involves an entry-level Higher Certificate, then a Diploma, then a Bachelor's degree. 30 The purpose of the registered qualifications is to maintain consistency in the units of study provided by institutions to meet the competency standards of students before employment. 31 Their qualifications have followed the USA national curriculum and are consistent with 4-year Bachelor's degrees offered in the USA. 31 In addition to the U.S.A, the South African Curriculum focuses on the basic medical sciences such as anatomy and physiology, paramedic-specific medical and trauma conditions, and a wide range of related paramedical disciplines such as rescue and communications. 32 Table 5 identifies the qualifications per the Emergency Care Qualification Framework for South Africa.
South Africa emergency care qualification framework (adapted from Sobuwa & Christopher, 2019).
Summary of findings
The three-stage approach modified from Brady's model was to expand and compare regulatory frameworks and education across the Anglosphere counties. It included South Africa due to the similarity in models of care, scopes of practice, and education to Australia and the USA. Internationally, comparative education identifies educational systems that recognise the comparisons and disparities between education models. 10 Comparative education is a useful evaluative tool for creating educational programmes by taking one system's strengths and incorporating them into another. 9
The analysis and comparison against international paramedic regulatory framework and education standards identified differences in the regulatory frameworks and various undergraduate paramedic degrees, and it has also demonstrated varying time frames in which ambulance organisations, training providers and universities undertake paramedic education (Table 6). The review's scope did not encompass specialist roles such as Critical Care Paramedics, High Acuity Response Unit Paramedics, Flight Paramedics, or Extended Care Paramedics and Community Paramedics.
Comparison of paramedic registration and qualifications.
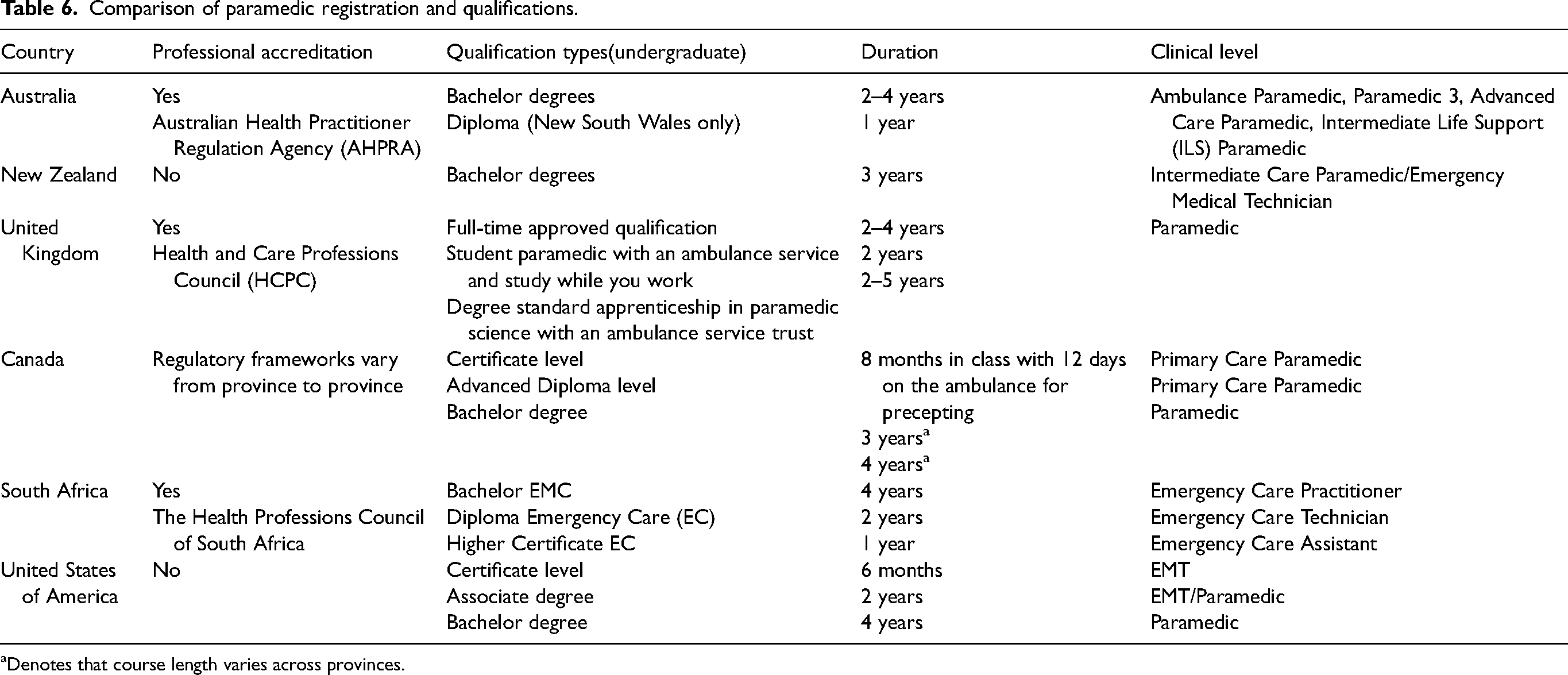
aDenotes that course length varies across provinces.
Discussion
Paramedicine education and regulation are critical aspects of ensuring the health and safety of communities. According to the World Health Organisation (2019), an evidence-based and contemporary national accreditation scheme can be effective for health professional education, including paramedicine. 33 However, despite discussions by paramedics’ professional organisations, achieving global accreditation standards for paramedic education has been challenging, given the global variations in curricula.
The lack of a standardised curriculum is mainly because paramedics worldwide need to be registered, making it difficult to sustain a standard-based curriculum. In Australia, paramedic education has evolved more rapidly than in other countries, with almost all education currently at the baccalaureate level. In the United Kingdom and South Africa, education is moving entirely into higher education, with university-based diplomas and 3-year and 4-year baccalaureate programmes. In contrast, paramedic education in the United States and Canada remains divided, with a historical emphasis on independence across different states and provinces.
In Australia, higher education institutions provide curriculum guidance, strengthening paramedic professional identity and providing educational reform for Paramedicine. 34 Education is at the forefront of identifying Paramedicine as a profession, leading to higher level educational qualifications, prospectively or retrospectively, as seen in Australia and New Zealand. 35 The nursing profession provides an excellent example of establishing a bachelor's degree as an initial qualification for nurses, with specialisations such as midwifery, intensive care, and emergency nursing provided at the post-graduate level.
There are provisions for regulating paramedicine in the United States and Canada. However, the government still needs concrete federal or state-level regulations or rules. Instead, the regulation of paramedicine in these countries is primarily carried out through various systems and processes.
In the United States, the regulation of paramedicine is primarily the responsibility of individual states. Each state has its own regulatory body, typically a state EMS office or board, responsible for establishing and enforcing rules and regulations for paramedics operating within that state's borders. The specific requirements for certification and licensure can vary widely from state to state, but generally, they involve a combination of education, training, and clinical experience.
Similarly, in Canada, the regulation of paramedicine is primarily carried out at the provincial level. Each province has its own regulatory body responsible for establishing and enforcing rules and regulations for paramedics operating within that province's borders. The PAC has also developed the NOCP, which outlines the competencies and tasks that paramedics should possess at various clinical levels, ensuring a consistent care level across Canada.
The regulatory frameworks supporting curricula also vary across countries, with registration being the recognition by the professional regulation body that the paramedic student has completed all educational requirements to practice as a paramedic in countries such as Australia and the UK. A recent article identifying the transition of Australian graduates into the United Kingdom determined that parallels occur between the practice and education of paramedics across these two countries. 6 Conversely, licensure by examination is required to practice as a paramedic in countries like the USA.
Paramedicine's globalisation goes beyond Australia and the United Kingdom and should include other Commonwealth countries such as Canada and South Africa. However, lacking evidence-based regulatory frameworks supporting curriculum design leads to poor outcomes and variations in graduate attributes and abilities. 36 Thus, an evidence-based regulatory framework supporting curriculum development can provide minimum standards through graduate competencies or prescriptive curricula development and the continuous evolution of curricula.
Limitations
Several challenges arise when attempting to comprehensively address and compare paramedic regulations, education systems, and credentials across jurisdictions, particularly in places like Canada and the USA. The intricate nature of paramedic regulations in these countries, with their varying breadth and depth, presents a complexity that goes beyond the scope of this paper. Additionally, the heterogeneity of education systems and credentials in these regions, in contrast to more homogenous systems in Australia or the UK, adds another layer of difficulty in presenting meaningful comparisons within the confines of this paper.
Moreover, the lack of a common definition for ‘paramedic’ across the Anglosphere further complicates comparative analyses. The existence of multiple paramedic levels within jurisdictions, each with its own set of regulatory and education nuances, poses a significant challenge.
Conclusion
In light of the recent registration of paramedicine with the Australian Health Practitioner Regulation Agency (Ahpra) and new guidelines for education standards, the timely comparison of curricular content and regulatory frameworks for entry-level paramedic qualifications has become increasingly important. As such, benchmarking curricula in paramedicine is critical to establish best practices and translate evidence into practice. Previous studies in nursing literature have reported the development of curriculum guidance for higher education institutions through benchmarking best practices. 35 A regulatory framework supporting curricula is crucial to paramedicine as it ensures that graduates are equipped to teach current and evolving practice scopes safely and effectively and are prepared for ongoing contemporary practice.
Through our comparative study, we've identified variations in regulatory frameworks and education within paramedicine globally, potentially influencing current and evolving practice scopes. Further exploration is required to examine consensus on the scope of practice internationally and academic perceptions in curricula. This involves in-depth analyses of various curricula, the professional scope of practice, and the role of education and regulatory frameworks in an expanded scope of practice. Additionally, a multilateral approach aligned with current and evolving practice could be supported by an international accreditation scheme, guiding curricula in higher education institutions. Overall, this research highlights the need for continued investigation and development of paramedicine's regulatory and educational frameworks to ensure practitioners are well-prepared for safe and effective patient care. While creating consistency across the Anglosphere is important, defining our profession and its nomenclature is equally crucial. Furthermore, when defining an international standard of paramedic education, a key decision will be whether graduates are novice learners or work-ready professionals.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Professor Scott Devenish is an Associate Editor.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.