
Abstract
Introduction
Paramedics receive varying levels of training in obstetric presentations. In high-risk, low-frequency cases, clinical guidelines should support clinicians to deliver optimal care. This study analysed publicly available clinical guidelines for obstetric presentations published by ambulance services in Australia and Aotearoa New Zealand to determine consistency of clinical guidance and adherence to nationally recognised standards for the development and reporting of evidence-based guidelines.
Method
Guidelines were sourced from publicly available websites of Australian and Aotearoa New Zealand ambulance services. The text was imported into a custom data collection frame which focused on five predefined specific obstetric presentations. Data were extracted and measured against nationally and internationally recognised best practice standards.
Results
Nine independent sets of clinical guidelines were included in the analysis. There was wide variation in the clinical guidance provided and scope of practice. Aspects were found to be absent, inconsistent, not supported by evidence or having potential to cause harm. None were consistent with recognised Australian best practice standards for guideline development in the areas of referencing and grading of evidence.
Conclusion
This study found substantial inconsistency of clinical guidance, highlighted conflicting and inadequate advice, and assessed the safety of advice provided when compared to best practice standards and evidence-based recommendations. Sustained effort to improve ambulance service clinical guidance regarding obstetric presentations is warranted.
Introduction
It is recognised that paramedics receive limited obstetric training and lack confidence in managing obstetric and neonatal presentations.1–3 The number of obstetric patients managed by paramedics is small, however those that are inappropriately managed and litigated represent almost a quarter of high average value claims. 4
A systematic review found that paramedics attend up to 91.5% of unplanned out-of-hospital births and while most births are uncomplicated there are varying degrees of maternal and neonatal complications. 3 The need for evidence-based guidelines to provide an appropriate course of action to be taken to minimise risks associated with unplanned out-of-hospital births is evident. A 2017 Australian study 5 found that while annual obstetric and neonatal caseload was low (around 0.5%), ambulance service clinical practice guidelines (CPGs) varied and provided incomplete or conflicting information. In this 2017 study, paramedics reported the application of obstetric practices and procedures that were dated and even potentially harmful to patients. 5
CPGs are ‘statements that include recommendations intended to optimise patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options’. 6 To ensure CPGs are transparent and high quality in New Zealand, the Ministry of Health oversees CPG development in conjunction with respective industry partners, 7 and in Australia, the National Health and Medical Research Council (NHMRC) set standards for the development and reporting of CPGs. 8 According to NHMRC Standards for Guidelines (Standard 2), 8 CPGs should be based on the best available evidence, include a strength of evidence statement, and be referenced. Only two ambulance services within Australia and New Zealand publicly publish information regarding their CPG development process. These services report that CPG development includes consultation between an ambulance-based Medical Advisory Committee and internal and external agencies, appraisal of published international guidelines, systematic reviews and existing state health service standards, and a process of clinical audit and adverse event review.9,10
Internationally recognised best practice recommendations for obstetric and neonatal care have been published by the Royal Australian and New Zealand College of Obstetrics and Gynaecology [RANZCOG], 11 World Health Organisation [WHO], 12 and various obstetric and neonatal clinical guidelines published by Australian state health departments. However, in the absence of a prehospital national guideline, little is known about how the CPGs in Australia and New Zealand ambulance services align with the current best evidence in obstetric and neonatal care and whether they adhere to best practice standards of CPG development and reporting.
The aim of this study was to conduct a document analysis of the publicly available guidance for Registered Paramedics on obstetric and neonatal presentations published by ambulance services in Australia and New Zealand. Our purpose was to:
Examine the consistency of guidance. Highlight conflicting, inadequate and potentially dangerous advice in the guidance with respect to the individual service scope of practice. Provide an assessment of the safety of recommendations when compared to systematic reviews and recommendations from national and international authorities; and Review the adherence of the guidelines with the nationally recognised standards for CPG development.
Method
Study design
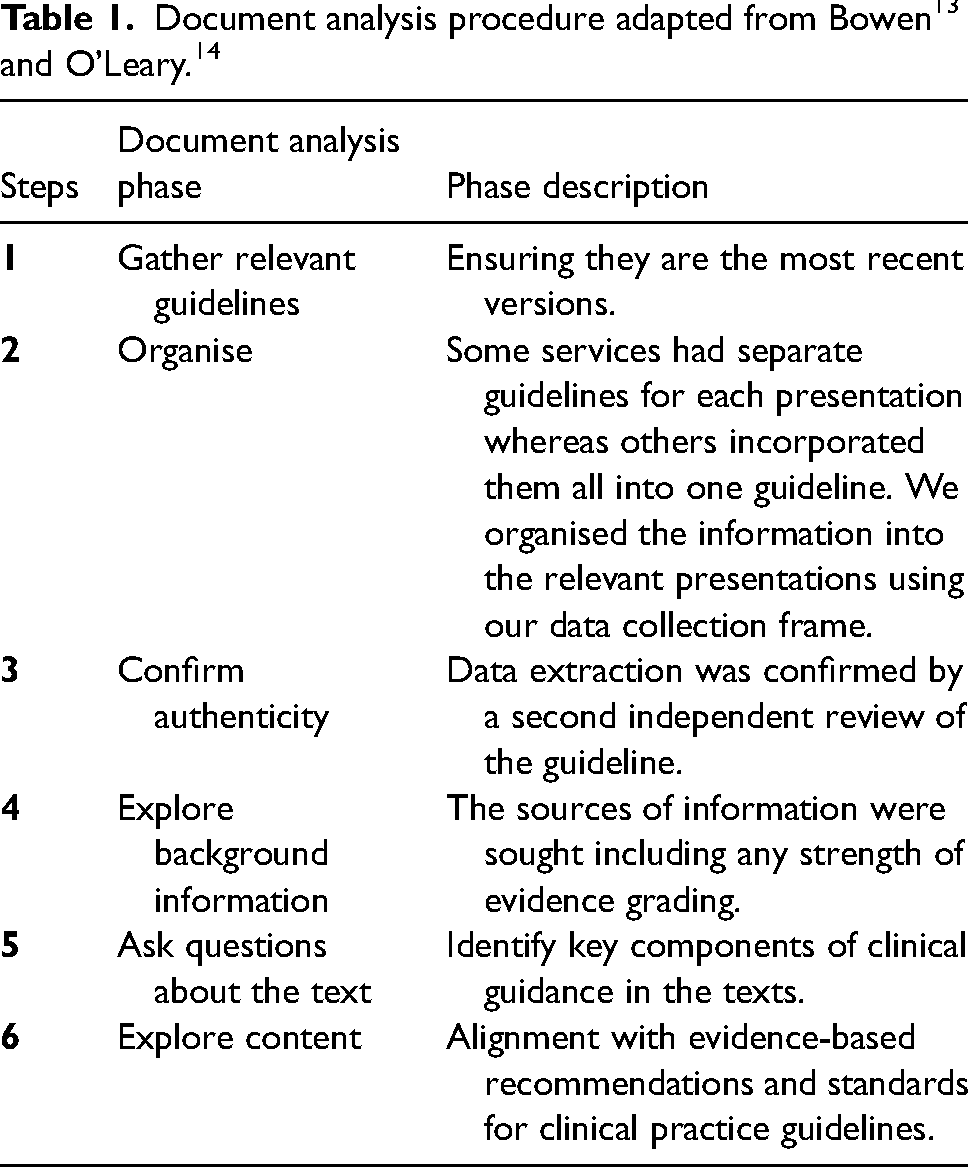
Using a pragmatic positivist approach, this deductive content analysis was guided by the works of Bowen 13 and O’Leary 14 and was conducted using publicly available clinical guidelines from Australian and New Zealand ambulance services.
Setting
Australia contains six states and two territories varying vastly in size ranging from over 2358 km2 to over 2.5 million km2 with population densities ranging from 0.2 to 179 people per km2. 15 Each state/territory government operates its own ambulance service with the exception of one state and one territory ambulance service that are operated by non-government charitable organisations. Each ambulance service develops and publishes their own CPGs; there is no national set of guidelines for ambulance services in Australia. New Zealand is over 268,000 km2 and has a population density of 18 people per km. 16 Two non-government run ambulance services operate in New Zealand and both use a common set of CPGs. Therefore, nine sets of guidelines used within 10 ambulance services were reviewed.
Document analysis
The latest versions of CPGs are publicly available online and the versions used in this study were current as of 21st November 2023. Supplemental Table 1 contains the CPG names, latest revision dates, and source URL.
To ensure empirical knowledge was produced we followed Bowen's 13 advice that researchers should determine the relevance of the documents to the research problem, assess documents for completeness, consider the original purpose of the documents, and decide the breadth of documents to analyse. O’Leary 14 supports this method by further stating that a process of gathering evidence, assessing for authentication, interrogation followed by reflection and data analysis should be considered. The iterative process of qualitative document analysis used in this study is outlined in Table 1 and involves identifying the documents for analysis and assessing the content.
The data collection frame was developed and focused on five predetermined areas of obstetric and neonatal clinical management common to most published guidelines:
Physiological cephalic birth Breech presentation Cord prolapse Shoulder dystocia Primary postpartum haemorrhage
The data collection frame development was led by a paramedic/midwife academic and comprised a series of questions relating to the current best evidence and recommendations published by reputable sources about the five clinical management areas.11,12 The focus of these questions was to identify gaps in key clinical information, report inconsistent advice, and identify any practice recommendations that have been found to cause patient harm. To ensure content validity and reliability, data pertaining to these questions and the guideline content were independently extracted from each guideline by two researchers according to the document analysis process described above. The extracted data were then moderated by the whole research team. In some instances, multiple sections of CPGs were relevant to the management of a single condition. Conversely, in some instances individual CPGs were available for each of the five clinical management areas while others incorporated these into a single guideline. As a result, this type of deductive content analysis, that is, asking questions of the guideline, was used to extract data for each of the five topics.
Any concerns regarding the context and meaning of the CPGs were discussed between the research team, comprising Registered Paramedics from four states in Australia, one of whom is triple registered as a nurse, paramedic, and midwife, and two with dual registration as a nurse and paramedic.
CPG content assessment
A quality analysis of the CPGs compared to the NHMRC Standards for Guidelines 2016 8 was conducted. Against these nine standards, a series of themes were developed to identify positive and negative aspects of the CPGs. The guidelines were also examined for referencing and grading of the evidence for the treatment recommendations. Data were extracted that related to each of these components as part of the data extraction process in the document analysis.
Data analysis
Each guideline was assessed by the researchers and classified into one of five outcomes for each question. A classic traffic light colour system was used to indicate weakness at a glance. The outcomes were:
Consistent with current recommendations – Contemporary guidance aligned to current recommendations (green colour to indicate good practice). Inadequate information was provided (amber colour to indicate need for improvement). No advice provided (amber colour to indicate need for improvement). Outdated or had the potential to cause harm (red colour to indicate potentially dangerous advice).
Consensus was required by the research team in order to proceed. Any disagreement was discussed and resolved.
Data storage and ethics
As the data is publicly available only the data extraction frame was stored in a secure server accessible by the research team. An ethics exemption was granted by the University of Sunshine Coast Human Research Ethics Committee (OE20036).
Results
Nine independent sets of CPG guidance were included in this analysis. Key results are presented as a narrative in Tables 2 to 6. The full data extraction tables can be found on the data repository link: https://figshare.com/s/6e8b532c335573859ac7.
Key recommendations for the management of a Physiological Birth.
Key recommendations for the management of breech birth.
Key recommendations for the management of a cord prolapse.
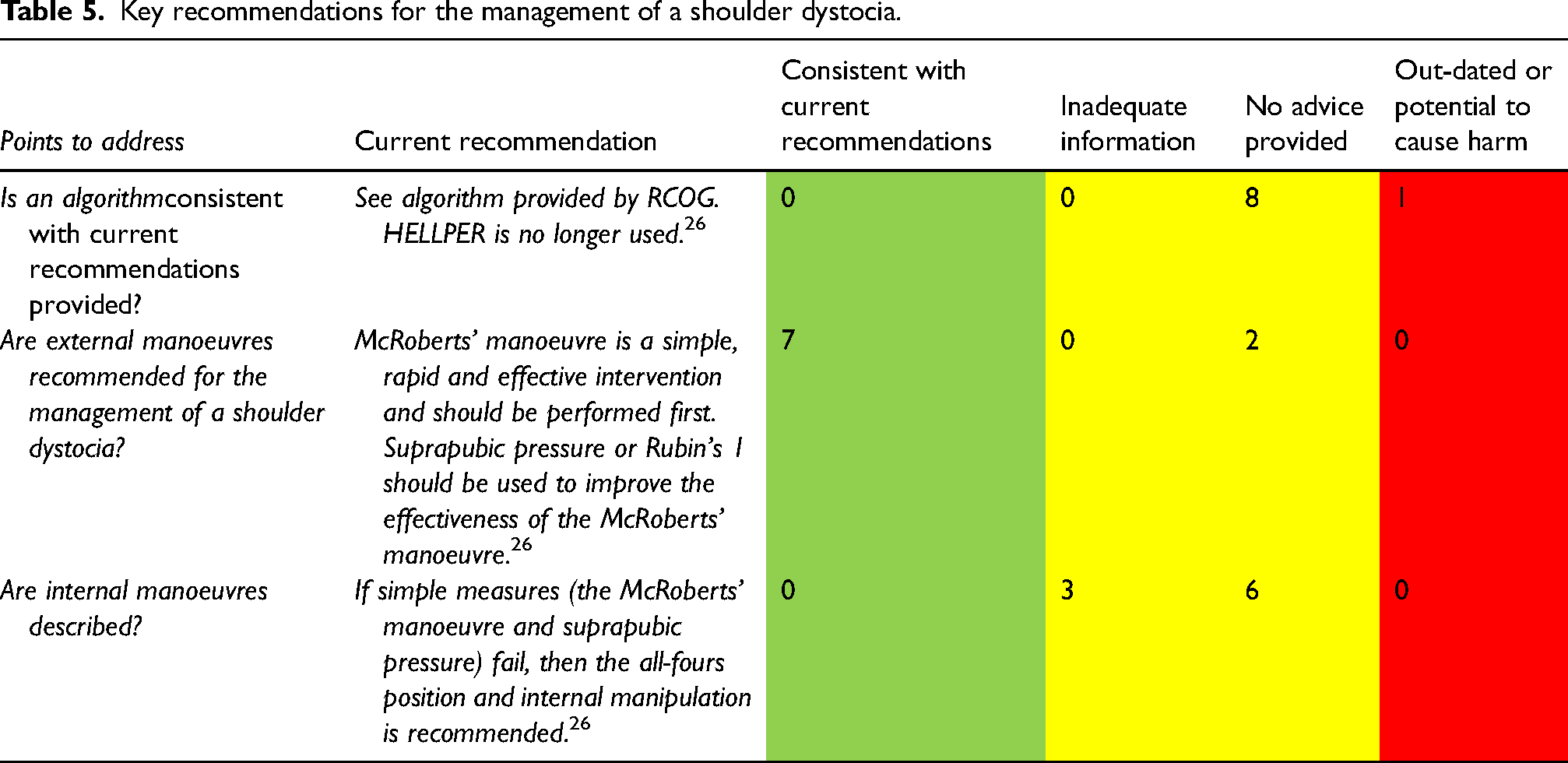
Key recommendations for the management of a shoulder dystocia.
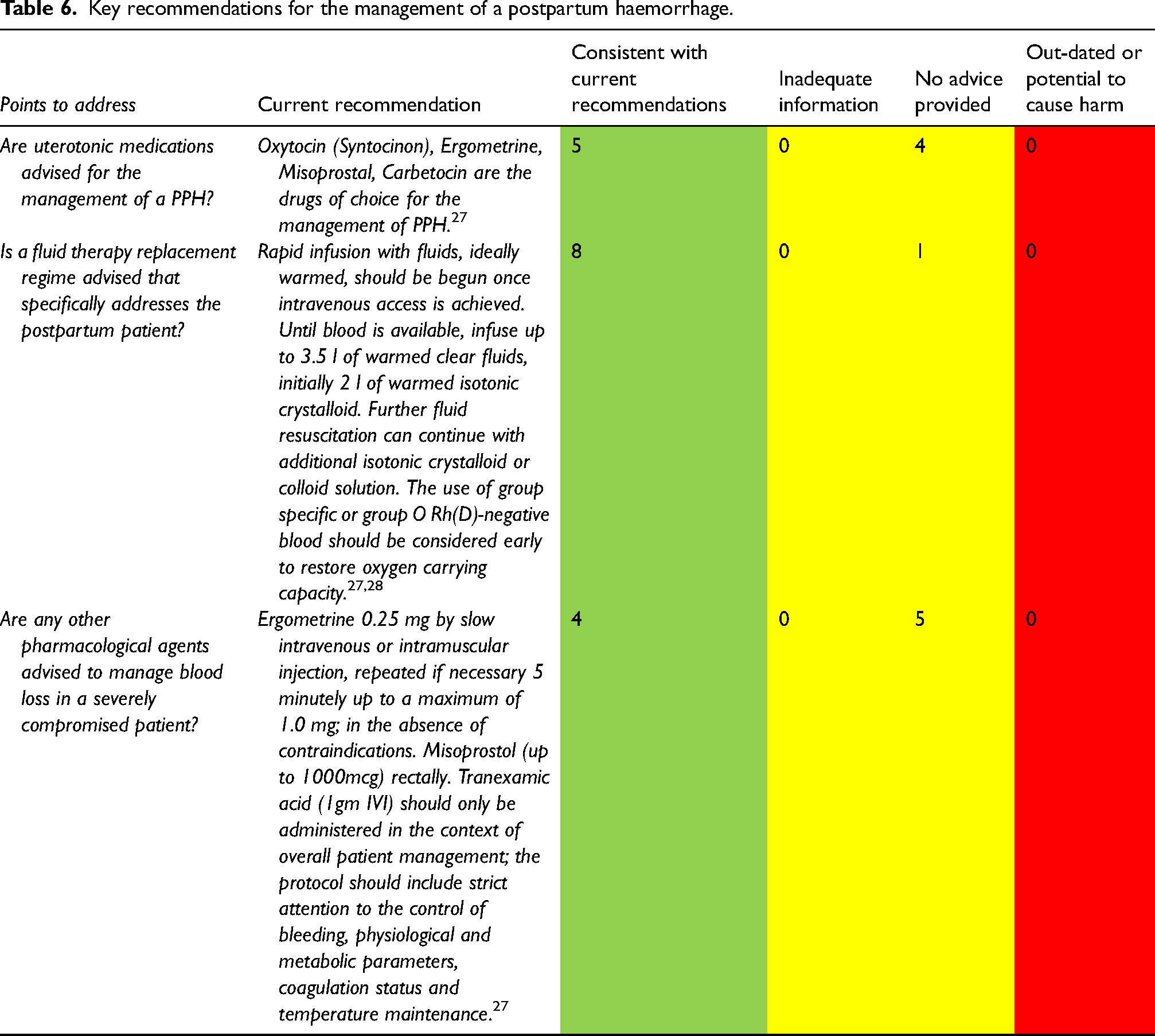
Key recommendations for the management of a postpartum haemorrhage.
Content analysis of recommendations
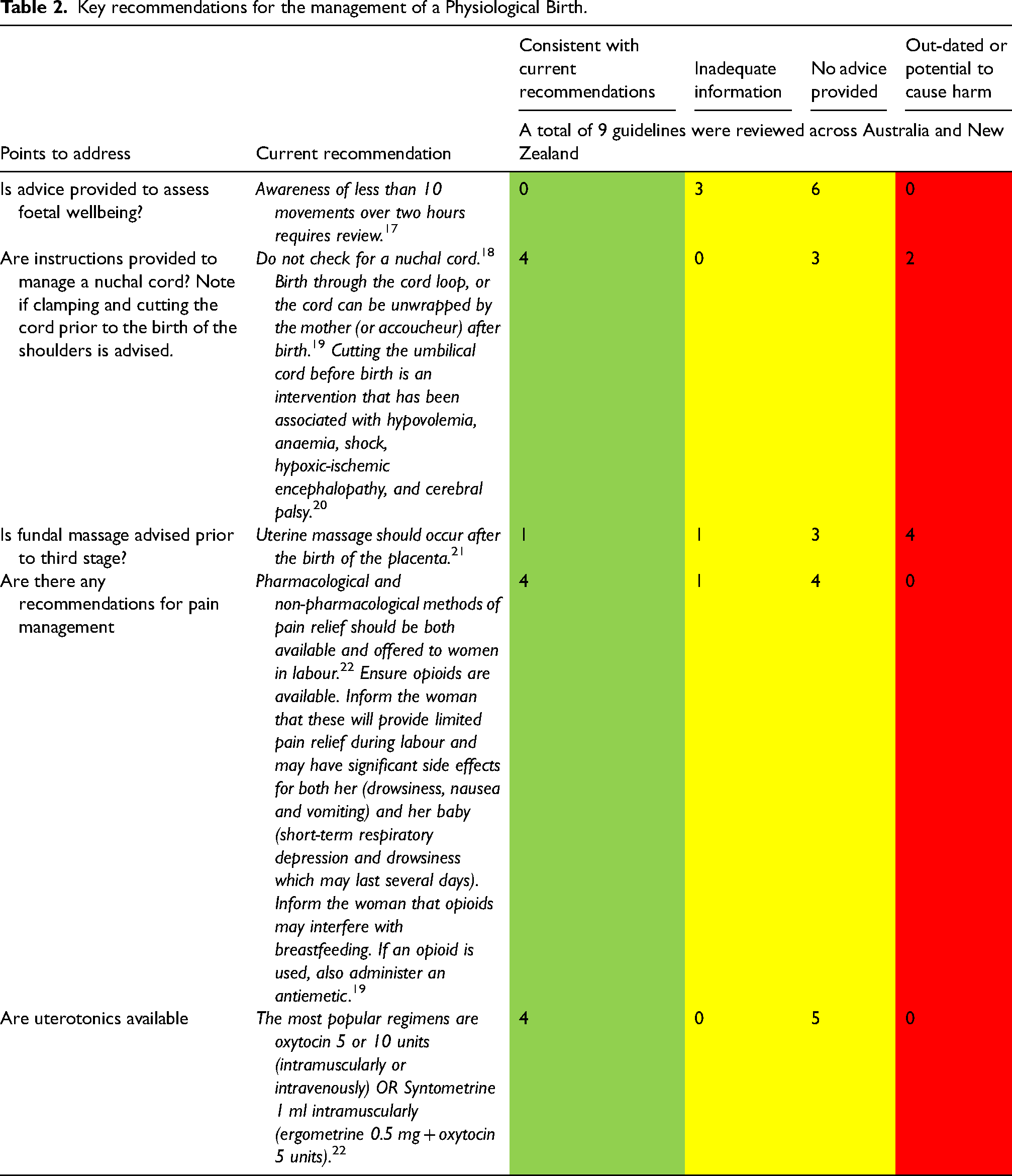
Physiological birth
All nine available CPGs from Australian and New Zealand ambulance services provided guidance on physiological birth. None included advice to assess foetal wellbeing consistent with current best-practice recommendations (Table 2). Four CPGs provided instructions regarding the management of nuchal cord; however, three service CPGs provided no advice. Two CPGs provided outdated or potentially harmful advice on the management of a nuchal cord (cord around the neck), namely, to clamp and cut the cord before the birth of the shoulders, and four provided potentially harmful or outdated advice regarding fundal massage prior to third stage (birthing of the placenta). The use of uterotonic medications in the management of third stage was inconsistent, some services recommended active management while others opted for physiological third stage management only.
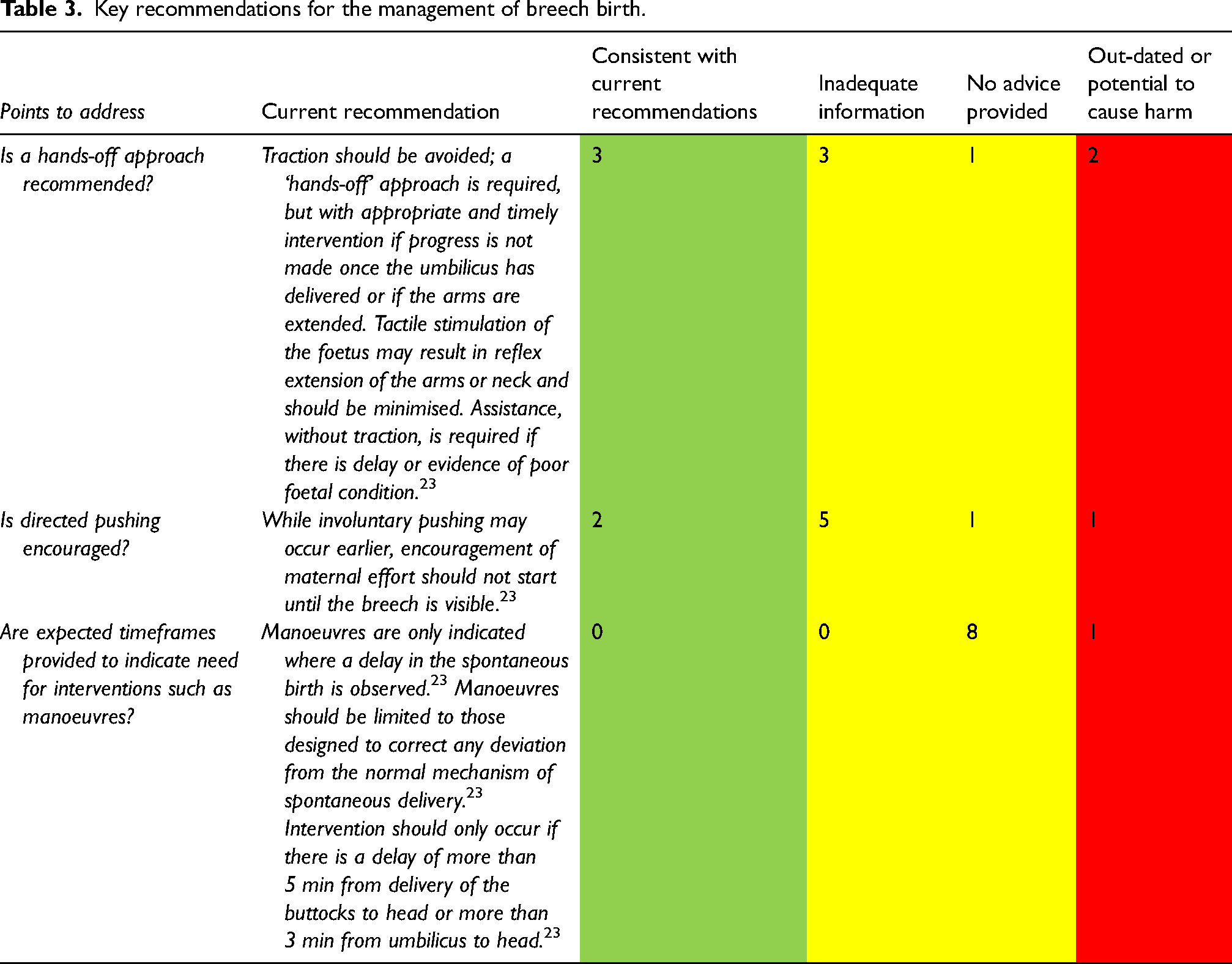
Breech presentation
Six of the nine guidelines addressed breech presentation (Table 3). While somewhat consistent, many guidelines provided insufficient advice regarding aspects such as the timing of interventions to resolve intrapartum complications related to breech management. For example, guidance referred to manoeuvers such as Løvset or Mauriceau-Smellie-Veit to manage the birth of the shoulders and head respectively however, it was not made explicit that these manoeuvers are only required if the newborn does not born spontaneously within a specific timeframe. 23 This potentially promotes early intervention of procedures that may interfere with normal birth physiology.
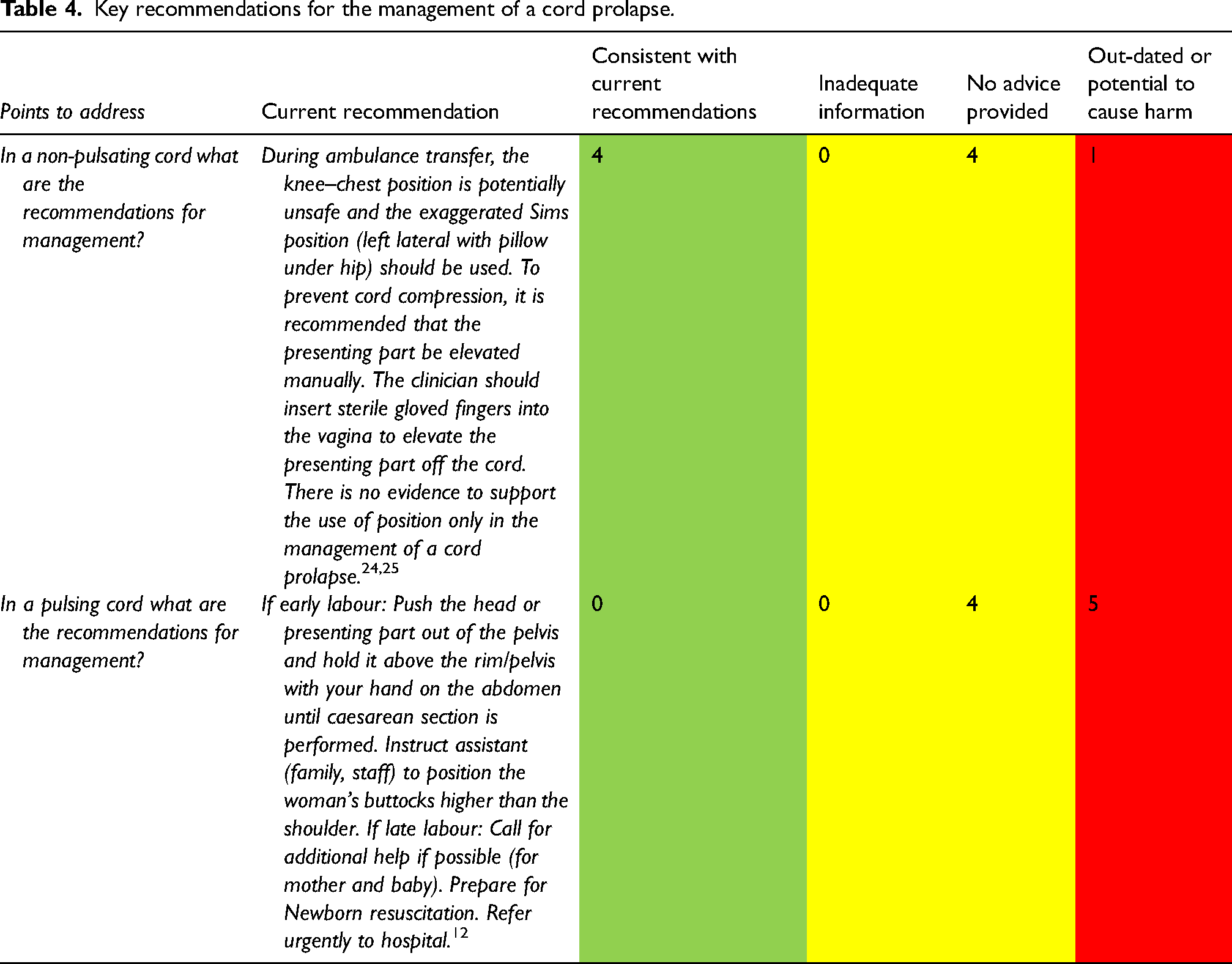
Cord prolapse
The five CPGs addressing cord prolapse were inconsistent in their management of either a pulsating or non-pulsating exposed cord (Table 4). Despite a lack of evidence proving any benefit 24 many recommendations included the use of moist towels to stop the cord from ‘drying out’. No guidance was found that recommended reassessment of the cord during transport. Some CPGs accurately recommended the immediate application of digital pressure on the foetal presenting part to alleviate cord compression and rapid transport. However, in all cases this was limited to a non-pulsating cord.
Shoulder dystocia
There was inconsistency in the intervention recommended in the six CPGs for shoulder dystocia (Table 5). Shoulder dystocia is a time critical presentation that requires prompt recognition and management. 26 Evidence suggests that in the absence of timely management, foetal hypoxic ischaemic injury or foetal death may occur within minutes. 26 While seven CPGs recommended external manoeuvers, six did not contain internal manoeuvers as a recommendation for the management of a shoulder dystocia when external manoeuvers fail to resolve the complication as it was outside their scope of practice. 26
Primary postpartum haemorrhage
For the management of a primary postpartum haemorrhage (PPH) inconsistencies occurred in three respects (Table 6). The first, was if guidance existed or not, the second was the availability of a uterotonic or antifibrinolytic medication, and the third was the ability to initiate external (external abdominal aortic compression) and internal manoeuvers (such as bimanual compression) to stop the haemorrhage in the case of an atonic uterus. Five services included uterotonic medications within the paramedic scope of practice for PPH, and varied between the type of drug available and whether it was considered a higher-level skill which required backup from a paramedic or other health professional with further clinical expertise. The guidance also varied depending on the method of third stage management. Four services did not provide any advice as to how to manage the third stage. This instruction is critical for paramedics as incorrect management causing a PPH is a major cause of maternal mortality and morbidity worldwide and a number of evidence-based studies have found an increasing incidence of PPH in developed countries over the past 15–20 years. 27
Content analysis of CPGs against the NHMRC standards
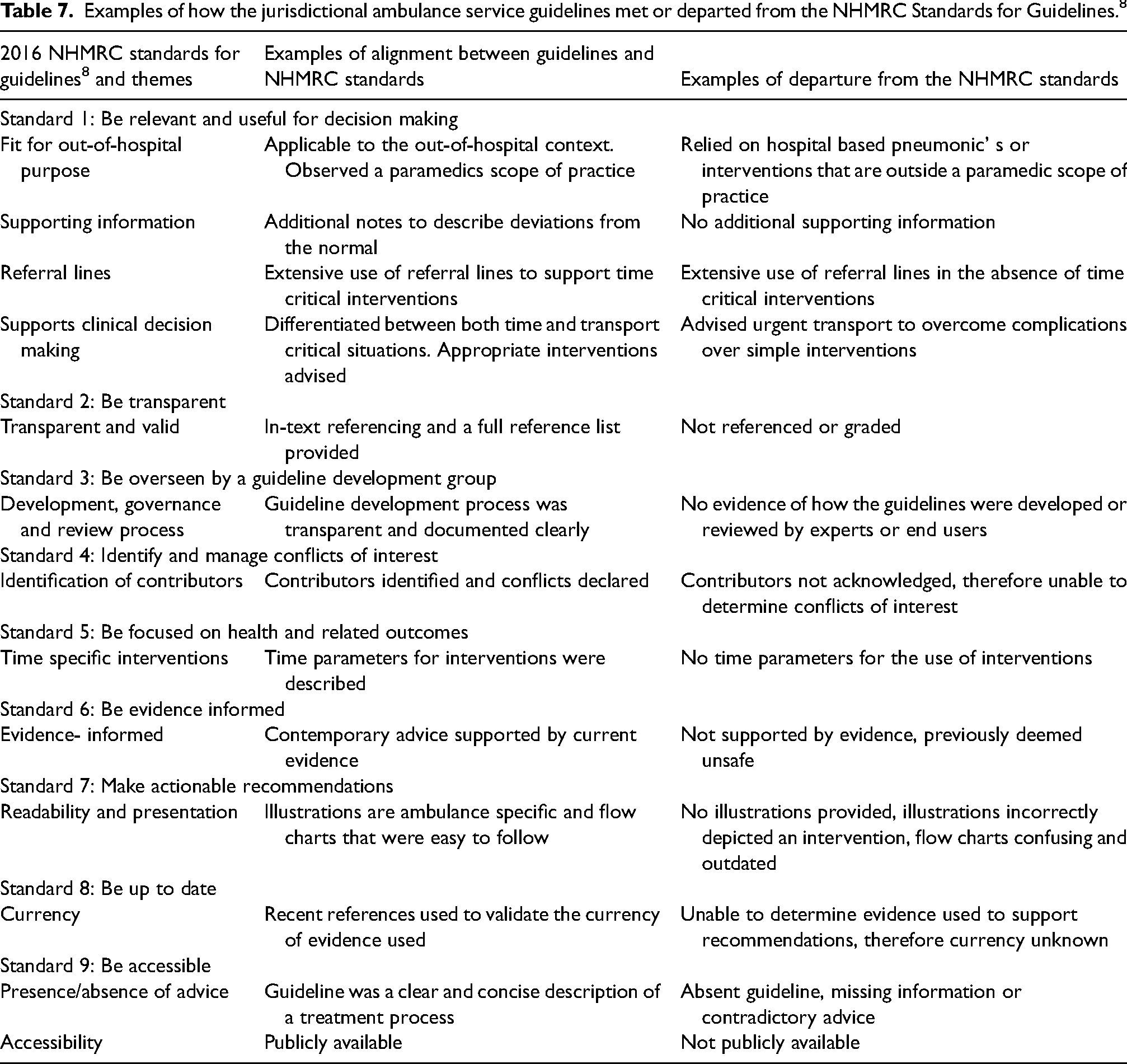
No guideline fully met the nine NHMRC standards for guideline development (Table 7). 8 While some guidelines met aspects of the NHMRC standards, most guidelines were deficient across multiple areas and the deficiencies were not homogenous. Table 7 describes aggregated examples of how the guidelines met areas of the NHMRC standards and where deficiencies exist.
Examples of how the jurisdictional ambulance service guidelines met or departed from the NHMRC Standards for Guidelines. 8
Strength of recommendations
From a total of 35 individual instances of clinical recommendations analysed, only seven included any references in support of the recommendation provided. All of these were from the same ambulance service. None of the recommendations provided any type of grading of the evidence that informed the advice provided.
Discussion
This document analysis compared the CPGs for the paramedic management of obstetric and neonatal presentations from ten Australian and New Zealand ambulance services. Eight were from Australia and one set used by both New Zealand services. It revealed two important overarching findings that will be discussed in further detail. Firstly, across services there was wide variation in clinical guidance provided for the paramedic management of obstetric and neonatal presentations and that some of the guidance had the potential to cause harm. Secondly, most of the recommendations provided by ambulance services for these presentations did not meet the recognised national standards for CPG development processes and publication. 8
Wide variation in clinical guidance and scope of practice was noted across the presenting conditions analysed, which is consistent with previous findings regarding ambulance service clinical guidelines. 29 It is concerning that procedures such as delayed cord clamping, assessing foetal wellbeing, and algorithms for shoulder dystocia that are included in best practice guidelines are omitted from some of the individual service recommendations. For example, with reference to clamping and cutting of the cord immediately post birth, four of the nine services provided insufficient, out-of-date or no advice as to the promotion of delayed or late cord clamping, a procedure considered best practice by both the WHO 30 and Royal College of Obstetricians and Gynaecologists 31 as it is known to increase neonatal blood volume, improve neonatal and infant iron stores and decrease neonatal and infant anaemia.
Furthermore, recommendations known to increase the risk of infant morbidity and mortality were included in two of the nine guidelines whereby clamping and cutting a nuchal cord prior to birth of the shoulders was advised. This is known to contribute to hypoxic ischaemic encephalopathy, cerebral palsy, hypovolaemia, anaemia and shock.20,32 Similarly, the three services who provided either no guidelines or insufficient information regarding nuchal cord management could be considered equally remiss.
Managing risks associated with maternal morbidity and mortality also showed variation between the CPGs. RANZCOG recommend ‘active’ management of the third stage of labour with prophylactic oxytocics followed by assisted delivery of the placenta to reduce the risk of PPH by approximately 50%. 27 Only two services explicitly advocated this approach, and two others included it as an option depending on patient preference. Further research should be undertaken to determine if physiological third stage management is appropriate in the prehospital context due to the unique care environment limitations. Buckley 33 suggests that a cold environment and/or a mother who is worried or distracted will have continuing high levels of adrenaline which can counteract oxytocin's beneficial effects on her uterus, and may increase the risk of haemorrhage. In his research of physiological third stage management, Odent 34 stresses the importance of not interrupting the mother and baby, even with words, and believes that ideally the new mother feels unobserved and uninhibited in the first encounter with her baby. This level of non-interference is uncommon in paramedic practice.
Overall, the quality of evidenced-based recommendations for paramedics was poor and inconsistent and in the context of managing obstetric patients relatively infrequently, this can expose both mother and baby to potential harm through inappropriate practices. 5 An example of this was found in the guidance regarding shoulder dystocia where the technical advice was out-of-date and referenced mnemonics that included procedures that were out of the paramedics’ clinical scope of practice. For example, advice given for the technique of providing suprapubic pressure for shoulder dystocia needed to be more explicit and provide further information on the correct location and technique. This advice was varied and in some instances the information provided could cause a ruptured uterus. Also, within the example of shoulder dystocia, critical information was missing regarding traction, internal manoeuvres, and one of the nine services who provided a shoulder dystocia guideline did not include time frames for each of the required manoeuvres. 26 Inaccuracies within the recommendations increase the risk of adverse patient outcomes, particularly when the complication is time critical, life threatening and infrequently seen by paramedics.
As it stands, the current clinical guidance provided by ambulance services to a large extent did not meet the definition or criteria to be called CPGs. They are largely only the ‘recommendations’ section of what would be included in a comprehensive CPG. CPGs must have clear statements of when to use, evidence of systematic review of the literature, graded recommendations, and evidence of who was involved in the development (ideally a broad range of experts). 8 None of the CPGs analysed in this study included all this information. The Joint Royal Colleges Ambulance Liaison Committee (JRCALC) CPGs are an example of paramedic clinical guidance which to a degree adheres to international best practice standards for CPGs. 35 To resolve the issue of poor or inconsistent clinical guidance, guideline developers should use internationally and nationally recognised standards for the development and reporting of methodologically rigorous CPGs which support best practice, such as AGREE II 36 and the NHMRC Standards for Guidelines. 8
Paramedicine may also benefit from the harmonisation of CPGs at the national level for all patient presentations, including obstetric and neonatal presentations. There are certain barriers to the development of such guidelines, including a need to recognise both the evidence base and the idiosyncrasies of the prehospital setting. Moreover, national guidelines would also need to recognise differences in state and territory law and be aligned to state and territory health departments to improve safety and quality in care. Finally, they should also provide guidance around culturally safe care which in some jurisdictions such as Australia, is a required professional capability of the registered paramedic. 37 In order to achieve this, CPG development would require the involvement of experts in CPG development methodology, subject area experts such as a consultant obstetrician, and engagement with stakeholders such as indigenous and culturally and linguistically diverse representatives.
Limitations
This type of document analysis has both advantages and disadvantages. The method is efficient as it requires data selection from existing, contained sources, rather than data collection which may introduce concerns around the representativeness and comprehensiveness of the collection. The information is available in the public domain and obtainable without further permission. It is cost-effective and stable; that is the documents examined and conclusions drawn are not influenced by the researcher's presence. However, a disadvantage of this type of document analysis is that the information may exist alongside other corporate policies and procedures that are not available in the public domain and therefore insufficient detail is available. Unlike most clinical guidelines in healthcare that are published publicly to allow for transparency, as recommended by the NHMRC, 8 ambulance services are not legally required to do so. Nonetheless, the nine CPGs reviewed provided sufficient evidence of the need for further research and updating of the guidelines.
Conclusion
This study has identified substantial differences between the obstetric guidance provided by ten ambulance services to inform their respective workforces that included significant deficiencies and inaccuracies that are inconsistent with evidence-based advice. Sustained effort to improve ambulance service clinical guidance regarding obstetric and neonatal presentations is warranted and future research should endeavour to produce national standards for out-of-hospital clinical practice for obstetric emergencies.
Supplemental Material
sj-docx-2-pam-10.1177_27536386231223761 - Supplemental material for A document analysis of clinical guidelines for the paramedic management of obstetric and neonatal presentations in Australian and New Zealand ambulance services
Supplemental material, sj-docx-2-pam-10.1177_27536386231223761 for A document analysis of clinical guidelines for the paramedic management of obstetric and neonatal presentations in Australian and New Zealand ambulance services by Belinda Flanagan, Nigel Barr, James Pearce and Kathryn Eastwood in Paramedicine
Supplemental Material
sj-pdf-3-pam-10.1177_27536386231223761 - Supplemental material for A document analysis of clinical guidelines for the paramedic management of obstetric and neonatal presentations in Australian and New Zealand ambulance services
Supplemental material, sj-pdf-3-pam-10.1177_27536386231223761 for A document analysis of clinical guidelines for the paramedic management of obstetric and neonatal presentations in Australian and New Zealand ambulance services by Belinda Flanagan, Nigel Barr, James Pearce and Kathryn Eastwood in Paramedicine
Footnotes
Author Contributions
All authors have met the requirements for authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Eastwood was funded by a Heart Foundation Postdoctoral Fellowship (No. 106158).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.