
Abstract
Background
Improved prehospital systems are contributing to increased presentations of CPR-Induced Consciousness (CPRIC). Data registries do not report CPRIC presentations and thus continued lack of evidence exists, causing a significant variation of prehospital CPRIC management guidelines. The result is variation in recognizing and managing CPRIC. Steps are needed to improve knowledge of CPRIC and model evidence-based guidelines.
Objective
An international panel of experts was recruited to create CPRIC definitions, guidelines, and a reporting framework which can be used for reporting purposes.
Methods
A Delphi methodology was used to gain consensus, defined as ≥70% agreement rate, on three domains or areas of interest: Definition, management guideline and data reporting. Participants were invited from the author's professional organizations, as well as social media outlets to recruit as many international clinicians as possible. The study administered four rounds of online surveys. Each round had multiple consensus statements for participants to respond to.
Results
Eighty-two percent of panelists reported seeing or managing CPRIC suggesting either improved awareness or increased exposure. Consensus was achieved in all three domains. There was agreement on a clear definition of CPRIC. The panel developed two subgroups of CPRIC; interfering and non-interfering CPRIC. Ketamine was the preferred choice to treat CPRIC. Panelists overwhelmingly felt CPRIC needed to be included into the Utstein guidelines.
Conclusions
This study successfully created definitions of CPRIC, management guidelines, and a data reporting framework. Using this study as a building block, the study team hopes stronger, evidence-based guidelines can now be researched and published.
Introduction
Over the last twenty years, prehospital medicine has had a continued increase in both presentation and awareness of CPR-Induced Consciousness (CPRIC).1,2,3 A recent scoping review of prehospital CPR-Induced Consciousness guidelines found almost 70% of the available guidelines had been published since 2020. 4 From the published data available CPR-Induced Consciousness is associated with younger, healthier, more viable patients who have increased Return of Spontaneous Circulation (ROSC) rates.5,6,7 CPR-Induced Consciousness occurrence in the prehospital field causes technical and ethical challenges for clinicians both physically and mentally.7,8,9,10
Despite the recent increase in published material, neither significant research nor clinical trials on CPR-Induced Consciousness have occurred.2,10,11 Lack of treatment guidelines, data collection, and an agreed upon definition for CPR-Induced Consciousness have restricted advancements on the topic.2,3,12 A large treatment variation exists between published guidelines, making comparisons between outcomes or management difficult, which further exacerbates the ability to gather evidence or data on the subject. 4 One recent observational study suggests that the use of sedatives, like midazolam, is associated with negative outcomes compared to no treatment at all. 1
Some of the variation in treatment lies in the distinct lack of evidence available on the subject. International resuscitation bodies are yet to produce guidelines on managing CPR-Induced Consciousness for prehospital clinicians. 4 To date, the only resuscitation body to have recognized CPR-Induced Consciousness within their guidelines is the International Liaison Committee on Resuscitation (ILCOR). 13 ILCOR highlights the lack of evidence to produce a consensus guideline, stating to use local sedative protocols until further research can be completed.4,14
Improved prehospital systems and CPR advancements will result in increased rates of CPR-Induced Consciousness presentations.1,15 In the absence of clinical guidelines, prehospital services with more frequent presentations of CPR-Induced Consciousness will develop different treatment protocols resulting in even more varied methods of treatment, making it even harder to collate outcome data and evaluate evidence-based guidelines. 12
A consensus guideline would be expected to benefit paramedics and other prehospital clinicians.6,16 Sound CPR-Induced Consciousness guidelines would improve scene management and reduce the cognitive burden on clinicians.9,10,15,17 This study would be the first consensus guideline based on international expert opinion, a significant improvement from the current assortment of locally developed guidelines based on local sedation protocols. By providing an international consensus definition, management guide and reporting framework to gather evidence, this study creates a building block to further our understanding regarding this confronting presentation and start the process towards stronger evidence-based guidelines.
Aim
To create an international consensus opinion on a CPR-Induced Consciousness definition, prehospital management guideline, and a reporting framework which can be used for reporting purposes via a modified Delphi method.
Rationale
There is a significant amount of uncertainty on the management, definition, and knowledge of CPR-Induced Consciousness.2,5,6 A lack of available evidence has arisen due to the variation in management guidelines and lack of reporting data. A Delphi study is a suitable way to create a CPR-Induced Consciousness definition, guideline, and reporting framework. 18 The Delphi method is widely utilized for healthcare research to provide consensus on complex issues where there is uncertainty or lack of agreement. 19
Methods
Criteria for the selection of expert panel
Selection of an expert panel in a Delphi study is challenging,19,20 especially on a medical condition that is published anecdotally as “rare.” CPR-Induced Consciousness is not only thought to be rare in occurrence but authors on the subject are exceedingly uncommon as well. However, the selection of a robust panel, one which has knowledge on the management of CPR-Induced Consciousness, would result in a consensus that holds weight and legitimacy amongst the medical community. Currently, there is no accepted consensus of what constitutes an expert in a Delphi study. 20
The authors reached out to practitioners and specialists known for their expertise in prehospital medical care. To involve as many experienced international clinicians as possible for the first round, additional participants were recruited by posting invitations to the study via online EMS specialty networks. The authors were also able to boost recruitment by contacting professional prehospital associations to send out invitations to their members. The authors also directly recruited experts who have previously published on this topic. Clinicians who were self-selected to take part in the Delphi survey were invited to participate in the recruitment round. From this list, the formation of an expert panel could be achieved to take part in subsequent rounds. Those invited were asked to spread the invitation for recruitment on social media platforms to gain widespread international recruitment, also known as snowball sampling. 21 The technique allowed the study to come into contact with as many experienced prehospital clinicians as possible to take part in subsequent rounds.
Originally, the author team drafted the following criteria to ascertain a prehospital CPR-Induced Consciousness expert for the purposes of participation in this Delphi study:
Must retain a job title of Paramedic, Intensive Care Paramedic, prehospital physician or Medical director Have personally managed a cardiac arrest with CPR-Induced Consciousness occurring Been present at least two prehospital scenes with a patient exhibiting CPR-Induced Consciousness
However, it became apparent that the above criteria were flawed. At least three medical directors of state-wide prehospital services would be excluded from the study on the grounds they had never managed or seen prehospital CPR-Induced Consciousness in the field. These participants were doctors with greater than 15 years of medical experience and knowledgeable in implementing or creating guidelines. The authors of the study felt that this was not in the best interests of the study and so this approach was abandoned. The relative obsquerity of CPR-Induced Consciousness was hampering the efforts to select a true “expert” panel. It is important to not only develop guidelines with consistent evidence but also seek input from experienced clinicians to ensure that the developed guideline is applicable and can be integrated into the community.22–24
Thus, a new criterion was proposed by the author team and was agreed to by all parties. Due to the undefined nature of CPR-Induced Consciousness, the author team wished to select a diverse panel of clinicians who have experience in the prehospital field, or those with experience creating clinical practice guidelines.
By using this criterion, the study recruited a broad set of opinions and perspectives ranging from prehospital medical directors to qualified paramedics. This comprehensive set of perspectives introduced study participants and authors to views they may not have thought of or considered previously, after each round when the results were collated and disseminated back to the participants. The broad recruitment to the study panel is based on the fact that CPR-Induced Consciousness is thought to be a rare phenomenon and the number of clinicians who could be counted as true experts on the topic is few and far between.
Conduct and reporting
This study was conducted and reported as per the recommendations for the Conducting and REporting of DElphi Studies (CREDES). 20
Ethics statement
This study has received ethics approval from Monash University Human Research Ethics Comittee on the 18th of July, 2022. The project ID number is 33375. Each participant was given an explanatory statement and asked to electronically sign an informed consent form prior to the start of the study.
Preparatory steps
As part of participant recruitment, a preliminary definition was presented by taking CPR-Induced Consciousness symptoms observed by clinicians from published case reports and including these symptoms in a list of selections. This definition was further broken down using a suggestion from a paper by Olaussen et al., 3 in which the terms Interfering and Non-Interfering CPR-Induced Consciousness were described.
There is little published material on the topic of CPR-Induced Consciousness around consensus management.6,14,25,26 Most of the evidence synthesized was taken from a scoping review by Howard et al., 4 in which international prehospital CPR-Induced Consciousness guidelines were collected and compared. Study authors were then able to ascertain commonly used medications, dosages and guidelines to treat CPR-Induced Consciousness. This information was collated together and then included into the recruitment round of the study. Instead of requesting participants to choose from a standard sedation regime, participants were asked to provide their own opinions and experiences when encountering CPR-Induced Consciousness.
There is no current data reporting of CPR-Induced Consciousness outcomes or management to create a survey. Instead, the most recent update of the Utstein guidelines for out-of-hospital cardiac arrests was used as a guide, 27 specifically the idea behind having broad main domains to report on, such as patient or outcome, before branching into smaller sub categories within each domain.
Piloting and general design of the survey rounds
All survey rounds were created using the online software program, Qualtrics. 28 Pilot drafts were provided every round for the author-team to complete. In each round, the author-team reviewed and edited the structure and design of the survey. The survey round could not be released until approval was met by all authors.
The surveys were designed in a linear fashion and separated into three domains: definitions, management, and data reporting. In the recruitment round, questions were mainly designed around free text comments. In the subsequent rounds, multiple choice was the preferred method of questioning for ease of data collection. Free text boxes were provided for most questions and domains to allow for further elaboration. Upon analysis of a survey round, participants would be invited into the next round if they had completed the previous round.
Number and design of survey rounds
The study was conducted across four rounds. All rounds were designed to have a completion time of less than 20 min. Each individual round was closed approximately 3 weeks after being opened. The first-round survey was opened on 18/08/2022 and the last survey round was closed on 30/11/2022. Participants were sent a reminder email once a week to complete the survey until the survey was closed.
The Delphi method sometimes will conduct meetings between rounds for participants to resolve uncertainties around questions. Given the online nature and international participant group, holding such meetings would be difficult to conduct. Instead, participants were given the collated data from the previous round of questions. This collated data informed participants of the previous rounds’ voting patterns. A graph would be provided comparing frequencies and percentages for each question from the previous round. Free text answers were collated, and the three most common answers were listed along with the reasoning for those answers. Articles would be provided to show the evidence around topics, especially those causing a divide in participant opinion or questions that were close to achieving consensus.
Recruitment round: identification of experts
The first round of the survey was designed to establish how the international prehospital community broadly defined, managed, and wanted to report CPR-Induced Consciousness. The difficulties around identifying experts in the field or general management trends of CPR-Induced Consciousness led to the creation of this “recruitment round”. The first round would form the basis of subsequent survey rounds. The questions were designed to be open-ended to stimulate qualitative feedback. This allowed the data obtained to be a true reflection of the participants’ opinions. The questions were either free text boxes or participants could select from several options already listed.
A demographic section was inserted into the start of the survey to identify a participant's prehospital position, experience, and the number of times they had witnessed or treated CPR-Induced Consciousness. A text box was positioned at the end of the survey, where an email could be typed if a participant was willing to be enrolled in subsequent rounds.
Round 1: establishment of broad consensus opinion
Having recruited a panel of experts, the objective of the next round was to narrow down participant consensus on the three subject domains. The three most popular responses to each question from round zero were presented as options in round one. Participants were then asked to choose between these options and were given the option of providing comments to expand or show their thinking behind their selection. For example, the three most popular choices to manage interfering CPR-Induced Consciousness in round zero were Ketamine, Fentanyl and Midazolam, making up more than 90% of the overall vote. In round one participants were asked to choose between the three and provide any extra comments in a free text box underneath the question if required.
Round one was made up of Likert scale questions. 29 The Likert scale questions, through descriptive analysis of answers, allowed the study to identify the consensus percentages of the participant group more accurately. The Likert-based questions were scaled across five points, with 1 being strongly disagree to 5 being strongly agree. Any answers scoring either a 4 (somewhat agree) or 5 (strongly agree) counted as agreeing with the statement.
Round 2: formation of a CPR-induced consciousness definition, management guidelines, and data reporting framework
If in the previous round, consensus was achieved across most domains. This would allow the presentation of an almost completed CPR-Induced Consciousness definition, management guidelines, and data reporting framework to participants in round 2. Participants were asked questions in the same Likert style as the previous round.
Round 3: endorsement of a CPR-induced consciousness guideline
If consensus thresholds were achieved in all three domains during round two. A completed guideline could be presented, and participants would be asked to agree or disagree with the document.
Methods of data analysis
Multiple methods of data analysis were used over the four rounds of the study. Round zero, with its open-ended question design, used inductive thematic analysis30,31 to identify popular patterns or themes from respondents. Rounds one and two used a combination of descriptive analysis (frequencies and percentages) 32 for the Likert based questions and thematic analysis for the free text boxes provided throughout the surveys. The final round used purely descriptive analysis (frequencies and percentages) to analyse the data.
Flow chart
The procedural flow chart for the Delphi study has been inserted below in Figure 1.
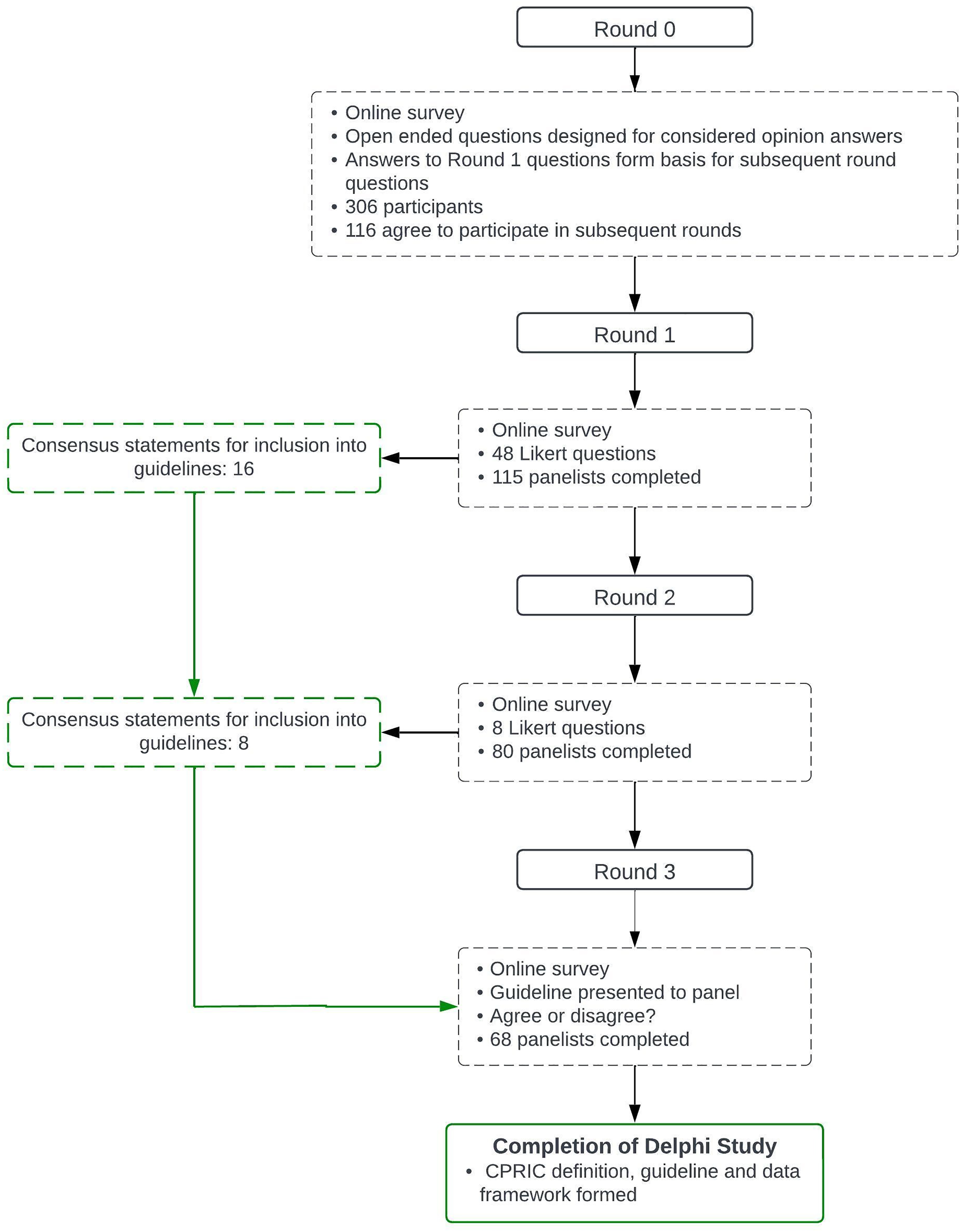
Delphi study flow chart
Definition of consensus
Consensus was required and defined by study authors prior to commencement. 33 Consensus was to be obtained when a statement earned a 70% agreement rate amongst participants. This number was chosen based off similar Delphi studies and was deemed acceptable to the authors. 20
Strategies for non-consensus were addressed by study authors prior to the commencement of the study. For each round, statements that were close (<20%) to achieving a 70% agreement rate would receive alterations based on free text comments from the previous round, and were then included in the next round. Statements that received less than 50% agreement rate in successive survey rounds were removed from subsequent rounds.
Results
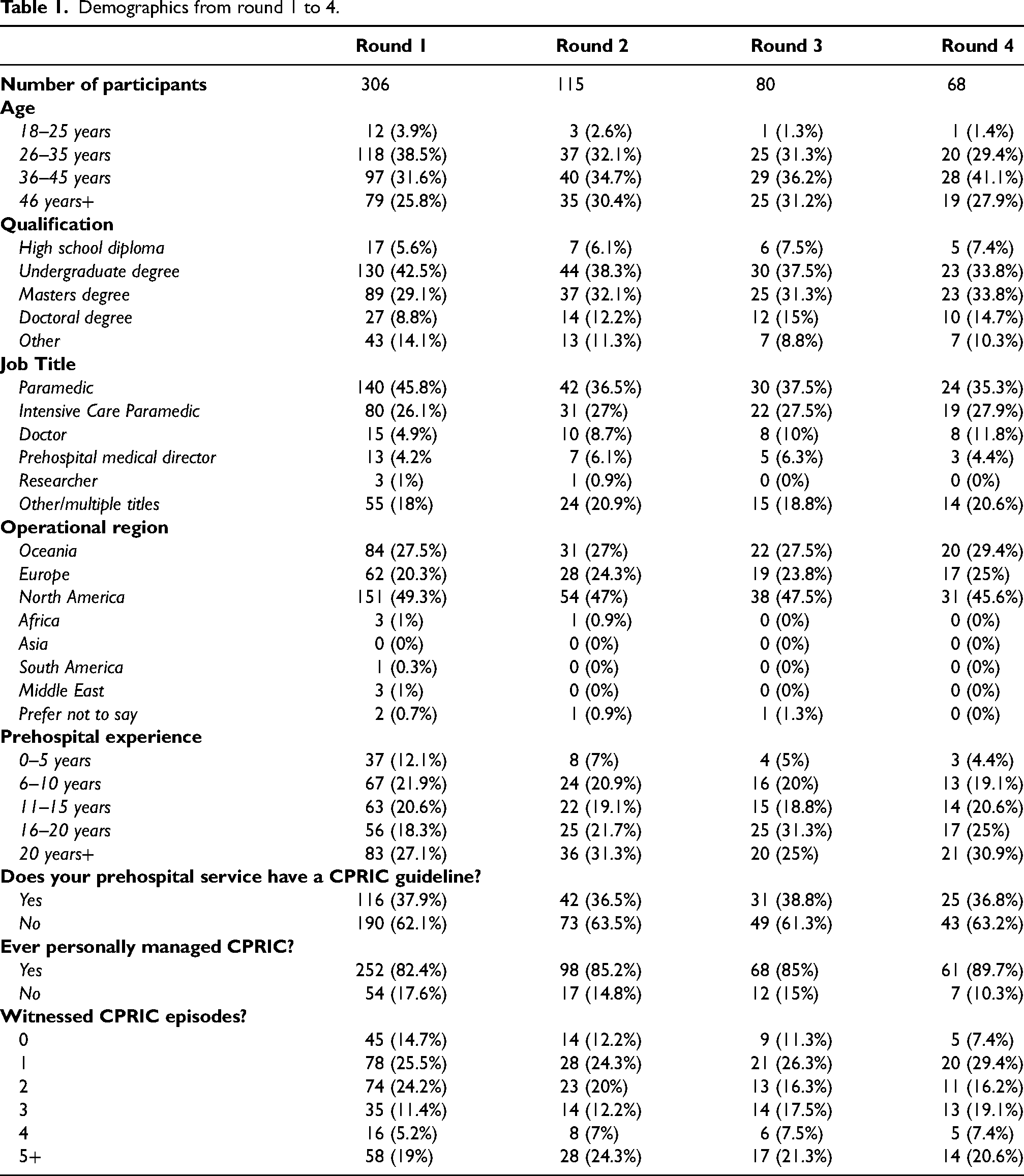
The study participants included paramedics, doctors, researchers, and prehospital medical directors. Every continent was represented in the study. The most experienced group of prehospital clinicians (>20 years experience) were the most numerous of the participant cohort. Recruitment demographics can be seen below in Table 1.
Demographics from round 1 to 4.
Round 0
Round zero consisted of 306 participants. The definition domain in round one received consistent responses from study participants. There was agreement amongst participants as to which characteristics were exhibited during both CPR-Induced Consciousness subtypes. A majority of participants, 87% (n = 271), felt the definition and sub-definitions of CPR-Induced Consciousness were appropriate.
The management domain had mixed responses across all statements. Ketamine dominated the medication choice to treat CPR-Induced Consciousness across all presentations. However, as can be seen in Appendix A, consensus was not common elsewhere. The decision to treat non-interfering CPR-Induced Consciousness was a divided choice amongst participants with 44% (n = 137) electing not to treat and 56% (n = 171) advocating to treat.
The data reporting domain received a consistent response amongst participants. Greater than 94% (n = 291) of respondents felt CPR-Induced Consciousness should be reported to cardiac arrest data registries and included in the Utstein guidelines. Participants cited four common elements for data reporting: outcome, management, length of resuscitation, and epidemiology.
Round 1
Round one consisted of 115 participants. All four statements in the definition domain received consensus in the second round. “Talking to rescuers” almost received a consensus vote in round one and so was altered, using information gathered from comment boxes. During the second round it received 71% (n = 82) agreement from participants.
The management domain received variable responses amongst participants. There was a strong consensus to use ketamine in interfering CPR-Induced Consciousness (89%, n = 102) and Non-Interfering CPR-Induced Consciousness (81%, n = 93). Variability in choice for a second line medication in interfering patients was notable, to the point consensus would be difficult to achieve within the desired four-round length of the study. Non-interfering CPR-Induced Consciousness (68%, n = 78) management did not achieve consensus due to participant group concern, in the free text boxes, as to the dose size and the effects this could have on perfusion in this cohort of patients. Participants were asked about the subject of length of resuscitation and whether they felt that the presence of CPR-Induced Consciousness should extend a resuscitation to a minimum of 45 min. This was based on studies investigating the ceiling limit of neurologically intact cardiac arrest survivors with a duration of resuscitation of at least 45 min.34–36
All four statements in the data reporting domain received >90% consensus rates.
Round 2
Round two consisted of 80 participants. The uniform agreement of panelists on the definition of CPR-Induced Consciousness in the round two questionnaire meant few changes were needed in round three. Minor word changes were made to definitions, mostly from commonly cited suggestions from round one. These changes increased the percentage of consensus for all three definitions.
Participant consensus for the management domain was strong. A change in ketamine dosing for first line management of interfering CPR-Induced Consciousness resulted in an increased respondent vote (90%, n = 72). The decision to leave second line management to local preferences due to divided opinion between fentanyl, midazolam, and paralytics, resulted in an 81% (n = 65) consensus. The change to reduced dosing of ketamine for Non-interfering CPR-Induced Consciousness provided a consensus vote of 84% (n = 67).
The data reporting domains strong consensus from round two allowed the formation of a completed framework to participants. The four reporting elements were continued in round three and specific examples of those elements were listed. This resulted in a 100% (n = 80) consensus for the entire domain.
Round 3
Round three consisted of 68 participants. Every statement from round three achieved a > 70% consensus vote, so participants in round three were presented with the completed guideline and asked if they agreed or disagreed with the guideline. The guideline received a 94% (n = 64) agreement rate.
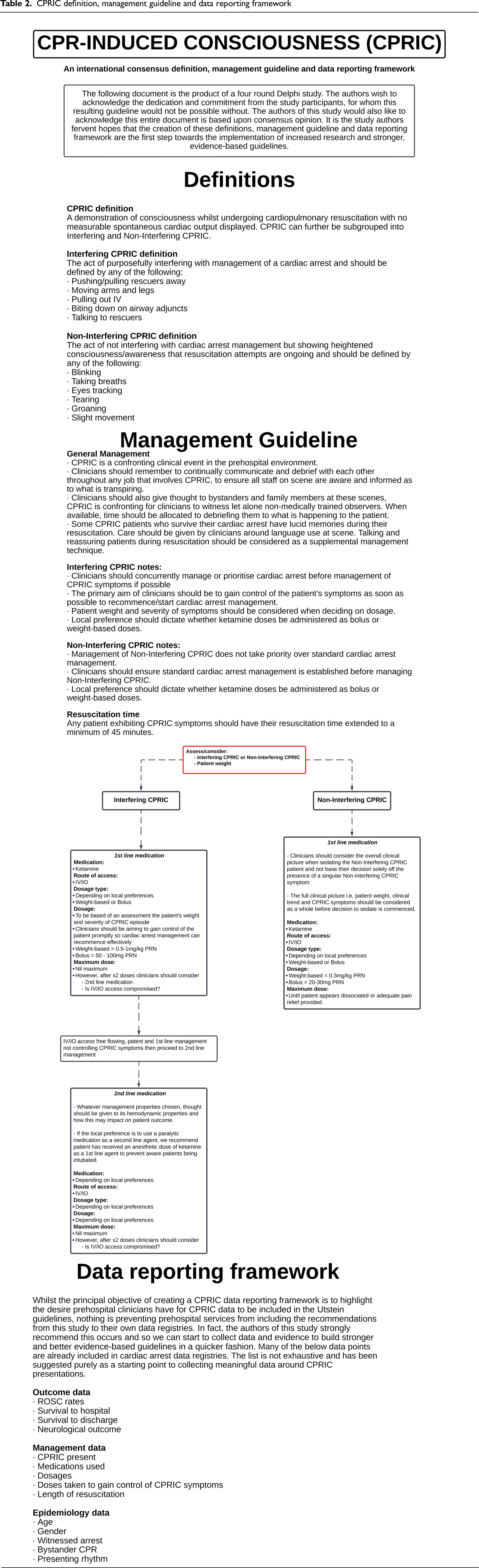
The full surveys can be seen in Appendix A, B, C, D which can be found online at cicm.org.au/journal.php. The completed CPR-Induced Consciousness definiton, management guideline and data reporting framework can be seen below in Table 2.
CPRIC definition, management guideline and data reporting framework
Discussion
This study successfully attained a consensus on a CPR-Induced Consciousness definition, management guidelines, and data reporting framework by international prehospital clinicians. This is the first step towards standardized care, data reporting, and further research.
The data reporting framework had consistently strong agreement rates from the first round. It was the only domain to have a clear consensus from the start of the study and reflects the demand of prehospital clinicians for a clear explanation of the CPR-Induced Consciousness phenomenon. The paradoxical situation of not collecting data on CPR-Induced Consciousness presentations, yet being unable to provide guidelines due to lack of data or evidence, could start to be reversed should CPR-Induced Consciousness presentations be included in the Utstein guidelines. 27
Prehospital clinicians still face significant ambiguity when managing CPR-Induced Consciousness. Almost 83% of participants had managed a CPR-Induced Consciousness presentation; however, only 38% of these participants had a guideline to manage this phenomenon. The confronting nature of CPR-Induced Consciousness presentations, coupled with this paucity of guidelines, will only exacerbate the cognitive burden CPR-Induced Consciousness brings to a scene. Prehospital services without a published CPR-Induced Consciousness protocol can integrate this guideline to reduce the psychological burden CPR-Induced Consciousness creates.
The study offers indirect evidence that the prevalence of CPR-Induced Consciousness may be higher than previously stated. Traditionally reported CPR-Induced Consciousness presentations statistically occur less than 1% of out-of-hospital cardiac arrest (OHCA).1,5 However, in our first round, out of 306 responses, 82.4% (n = 252) had managed a CPR-Induced Consciousness presentation. The discrepancy between reported CPR-Induced Consciousness events in the registry studies and cross-sectional surveys has previously been demonstrated3,37 clearly the need for rigorous data collection and epidemiological research to establish a more accurate prevalence figure is required.
There was a strong consensus from study participants to treat CPR-Induced Consciousness with Ketamine. The positive haemodynamic and rapid dissociative properties of ketamine 38 were commonly cited as the reason for its use to manage CPR-Induced Consciousness, participants cited the need to gain control of patient management quickly as a driving force behind creation of this guideline. There was participant concern throughout the study about ketamine's impact on perfusion in high shock index patients. 39 However, finding a dose that will quickly and effectively sedate a CPR-Induced Consciousness patient who is preventing CPR, defibrillation or distracting prehospital clinicians was also strongly advocated for. Clearly, a balance needs to be attained between the two conflicting requirements. Further research into ketamine's effects on perfusion in high shock states needs to be considered.
There was a lack of clear consensus for a second line agent to treat Interfering CPR-Induced Consciousness. Participants were unable to come to a majority for either Fentanyl, Midazolam or Rocuronium. North America and Europe had strong tendencies towards Midazolam, yet clinicians from Oceania preferred paralytics or Fentanyl. Despite its negative cardiovascular side effects,40,41 Midazolam captured a large section of the vote. Some participants stated the reason for their choice was that Midazolam was part of their practice whereas paralytics were not authorized, and they did not feel comfortable advocating for a medication they can’t use. In contrast, Oceanic participants felt that it made more sense to follow an anesthetic dose of Ketamine with a paralytic due to their own local guidelines. It is important to note that ILCOR recommends sedation for CPR-Induced Consciousness be given prior to the administration of paralytics, to which these guidelines also recommend. An interesting finding from the study was the division amongst clinicians in managing Non-Interfering CPR-Induced Consciousness. Opinion was almost evenly divided during the first round on whether to sedate this cohort or not. Participants justified in the free text box that there was no need to risk side effects via sedation as the patient was not interfering, while other participants felt it inhumane to leave patients with heightened awareness under-sedated. These sharply divided opinions of experts further solidifies the need to have CPR-Induced Consciousness cases reported to resuscitative data registries, in order to ascertain whether sedation regimes negatively affect outcomes. Recent work by Parnia et al. 34 highlights a significant portion of cardiac arrest patients have increased awareness during resuscitation and suffer psychologically because of this. While the debate around sedation during resuscitation continues, patients are suffering negatively and this topic needs to be addressed.
Limitations
Participation numbers were drawn mainly from Western regions. The study was not able to build many contacts in other regions, despite multiple attempts to assert some. The study acknowledges the unintentional bias this may cause. In addition, the voluntary nature of the study may have biased the participation cohort to contain a far greater number of clinicians who have experienced CPR-Induced Consciousness or an interest in the subject matter. This non-randomised recruitment could have biased the responses of participants towards a particular management pathway.
Participant attrition between survey rounds, although expected, is a limitation. Representation for or against a consensus statement can be altered in either direction with significant participant attrition. However, as can be seen in Table 1, the study maintained a broad representation of experience and job title until the final round. This consistency helped balance consensus opinion in each survey round.
Whilst the above limitations may have had a negative impact on the study, the generalizability of the study results naturally lend themselves to further research into CPR-Induced Consciousness. Specifically, the effect pharmacological management of CPR-Induced Consciousness has on patient outcomes.
Conclusion
This study successfully created an international prehospital consensus definition, guideline, and data reporting framework. There is a clear consensus towards a CPR-Induced Consciousness definition, use of ketamine to manage CPR-Induced Consciousness presentations, and a desire for CPR-Induced Consciousness presentations to be included in the Utstein guidelines or local prehospital cardiac arrest data registries. This consensus guideline will help alleviate the challenges involved with treating and understanding CPR-Induced Consciousness. The study authors hope that, with this clear definition and data reporting framework in place, further vital research can be undertaken.
Supplemental Material
sj-pdf-1-pam-10.1177_27536386231215608 - Supplemental material for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study
Supplemental material, sj-pdf-1-pam-10.1177_27536386231215608 for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study by Jack Howard, Eystein Grusd, Don Rice, Nikiah G. Nudell, Carlos Lipscombe, Matthew Shepherd and Alexander Olaussen in Paramedicine
Supplemental Material
sj-pdf-2-pam-10.1177_27536386231215608 - Supplemental material for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study
Supplemental material, sj-pdf-2-pam-10.1177_27536386231215608 for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study by Jack Howard, Eystein Grusd, Don Rice, Nikiah G. Nudell, Carlos Lipscombe, Matthew Shepherd and Alexander Olaussen in Paramedicine
Supplemental Material
sj-pdf-3-pam-10.1177_27536386231215608 - Supplemental material for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study
Supplemental material, sj-pdf-3-pam-10.1177_27536386231215608 for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study by Jack Howard, Eystein Grusd, Don Rice, Nikiah G. Nudell, Carlos Lipscombe, Matthew Shepherd and Alexander Olaussen in Paramedicine
Supplemental Material
sj-pdf-4-pam-10.1177_27536386231215608 - Supplemental material for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study
Supplemental material, sj-pdf-4-pam-10.1177_27536386231215608 for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study by Jack Howard, Eystein Grusd, Don Rice, Nikiah G. Nudell, Carlos Lipscombe, Matthew Shepherd and Alexander Olaussen in Paramedicine
Supplemental Material
sj-docx-5-pam-10.1177_27536386231215608 - Supplemental material for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study
Supplemental material, sj-docx-5-pam-10.1177_27536386231215608 for Development of an international prehospital CPR-induced consciousness guideline: A Delphi study by Jack Howard, Eystein Grusd, Don Rice, Nikiah G. Nudell, Carlos Lipscombe, Matthew Shepherd and Alexander Olaussen in Paramedicine
Footnotes
Acknowledgements
The authors are grateful to the participants of this Delphi study, without whom these definitions, guideline and reporting template would not be possible.
Credit author statement
Data sharing statement
Declaration of interest statement
The author team declares no conflicts of interest. No sources of funding were associated with the conduct of this research and preparation of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.