
Abstract
Clinicians in paramedicine are exposed to stressful events at work that have potential to cause negative psychological outcomes. Posttraumatic growth (PTG), resilience and psychological wellbeing, however, are adaptive psychological states that can also occur following trauma and adversity. Synthesis of knowledge on these positive outcomes can provide insight into resources needed to support paramedicine clinicians. To examine and synthesise what is known of PTG, resilience and psychological wellbeing of paramedicine clinicians, including the experience of these phenomena and relationship between them. An integrative review of peer-reviewed empirical literature published in English from 2013 to 2022 was conducted, following Whittemore and Knafl’s method. CINAHL Complete, MEDLINE Complete, PsycINFO, Scopus and Embase databases were searched. Included articles were quality appraised, with data analysed using the constant comparison method. Thirteen articles were included, with results synthesised into four categories. Mean PTG scores were reportedly moderate, and resilience ranged from average to above average. PTG and resilience had positive and negative relationships with specific coping strategies including dysfunctional coping, active coping, planning, venting emotions, social and emotional support and mental and behavioural disengagement. PTG scores were significantly lower for clinicians with longer shift duration and paramedics compared to emergency medical technicians. Resilience scores were higher for clinicians working part-time. Wellbeing was reportedly moderate and associated with the psychosocial climate established by managers. Qualitative findings indicated that workplace culture was perceived as stoic and masculine, which served to undermine staff resilience and willingness to disclose emotions. To support PTG and resilience, organisations should work to reduce stressors in workplace culture, including management and clinical supervision style, and offer employment flexibility. Organisations can upskill clinicians’ capacity for positive adaptation to adversity with professional development targeting identified coping strategies. Future research could examine clinicians’ experiences of PTG, resilience and wellbeing, and the relationship between them.
Keywords
Introduction
In the course of providing emergency care to the community, clinicians in paramedicine such as paramedics and emergency medical technicians (EMTs) are exposed to a unique combination of workplace stressors. These include the mental, physical and emotional demands of the work itself, 1 as well as structural and organisational stressors including high case volumes 2 and shift work. 3 Clinicians can also experience specific events that may result in psychological trauma.4,5 The negative psychological outcomes of this extend to poorer mental health including symptoms of posttraumatic stress, which can be particularly prevalent if paramedicine clinicians’ psychological wellbeing is not supported. 6 Posttraumatic growth (PTG) and resilience, however, are positive psychological responses in the face of trauma and adversity, and provide insight into adaptive processes that can support psychological wellbeing.7,8 Psychological wellbeing involves positive psychological functioning, having a sense of autonomy, purpose, growth, self-acceptance, mastery of one's life and positive relationships with others. 9 As a similar, but conceptually distinct positive outcome following stress and adversity, resilience can be understood as the dynamic process of regaining or maintaining psychological wellbeing through interactions between a person’s adaptive resources and those from their social and physical environment. 8 Posttraumatic growth, however, involves a severe psychological struggle where core beliefs can be challenged after a traumatic event, ultimately leading to positive cognitive transformation and growth. 10 This can include recognising new possibilities in life, as well as changes in perceptions of personal strength, relating to others, spiritual or existential change and overall appreciation of life. 10 It is relevant to note that as these are constructs, there has been some variance in conceptualisations of resilience and posttraumatic growth over time; however, they are distinctly defined and measured in contemporary health literature.7,11 To strengthen paramedicine clinicians’ potential for positive psychological outcomes through trauma and adversity, and guide associated policies, a collective examination of PTG, resilience and psychological wellbeing, and the relationship between them is needed. To date, no reviews have examined the combined evidence for these positive outcomes for this healthcare group.
The nature of paramedicine clinicians’ work and the stress related to organisational policies and structures have well-established repercussions for mental health. 12 In addition to the cognitive demands of the role, clinicians can experience occupational violence,13,14 stress from extended hospital delays, 15 high case volumes, time pressure, 2 and fatigue and social desynchronisation from shift work.2,3,16,17 Fatigue and disordered sleep for paramedicine clinicians exceed that of the general population, 3 and can strain sources of social support, contributing to social disconnection, reduced intimacy with partners and family conflict. 1 Paramedicine clinicians’ elevated prevalence of depression and generalised anxiety disorder have also been established, with a recent systematic review revealing their mean rates to be 20.6% and 20.0%, respectively. 12
Paramedicine clinicians can also be exposed to extreme events that have the potential for psychological trauma. This is known to be an emotional response that may present with intense fear, horror, or hopelessness, which occurs after experiencing or witnessing a highly distressing event, such as an assault, severe injury, threat to life, suicide, death, or a sudden catastrophic medical incident.18,19 The most debilitating of repercussions is posttraumatic stress disorder (PTSD), which is a psychiatric condition characterised by intense distress and impairment following vicarious or direct exposure to one or more traumatic events. 19 With workplace experiences including attending suicides, deaths, family violence, death of a child, grotesque mutilation and threatened or actual assault, 2 more than half of paramedics (54.8%) report being deeply affected by traumatic workplace events. 20 Accordingly, the prevalence of PTSD for paramedicine clinicians is markedly elevated (11–14.6%)4,5 compared to the general population (1.5%). 21
With these known negative psychological outcomes, there has been an understandable focus on measuring paramedicine clinicians’ psychological distress and stress symptoms. However, investigations focused solely on deficits do not necessarily support positive psychological wellbeing. In addition, this narrow focus on deficits is misaligned with principles of trauma-informed care, which recommend a strength-based approach, instead of understanding trauma survivors based on pathology alone. 22 Indeed, research suggests that for survivors of trauma, focussing only on psychopathology may impede recovery and conceal positive changes that have occurred. 23 Resilience and PTG are strength-based approaches to understanding how at-risk groups can have positive outcomes in these settings; 24 however, there are currently gaps in the knowledge regarding these outcomes in paramedicine. Although contemporary understandings of resilience identify the importance of interactions between an individual and their available social and environmental resources, 8 to date, researchers in paramedicine have largely defined resilience as a personal ability or trait rather than an interactive process. 25 In addition, although PTG indicates a positive psychological outcome, it is widely understood that PTG can co-occur with psychological distress and posttraumatic symptoms. 23 The combined examination of PTG, resilience and psychological wellbeing has the potential to provide a more comprehensive insight, to advance understandings of the strengths and positive adaptations that could be supported for paramedicine clinicians within their work environments.
While there have been reviews on risk factors for posttraumatic stress symptoms26–28 and coping strategies in paramedicine,17,29 there are no current reviews on PTG, resilience and psychological wellbeing, and their relationship. With resilience and PTG research providing an insight into unique dimensions of wellbeing and positive adaptation, understanding the evidence on these states will provide important information to direct future policies, practice and research. To address this gap in knowledge, this integrative review aims to examine and synthesise what is known regarding the PTG, resilience and psychological wellbeing of paramedicine clinicians, including the experience of these phenomena and the relationship between them.
Methods
Design
An integrative review was performed to enable a systematic search process and comprehensive synthesis of evidence from qualitative and quantitative literature. To uphold methodological rigour, the 5-stage framework outlined by Whittemore and Knafl 30 was employed, ensuring the resulting synthesis of evidence on PTG, resilience and psychological wellbeing was reliable. The protocol was registered with Open Science (registration DOI: https://doi.org/10.17605/OSF.IO/8WH9Q), and reporting of the systematic search and screening of relevant studies followed the Preferred Reporting Items of Systematic Review and Meta-Analyses (PRISMA). 31
Search strategy and inclusion/exclusion criteria
The phenomena of interest and sampling frame were established in accordance with the problem identification stage of integrative review methodology. Search terms were developed in collaboration with an experienced research librarian (see Table 1), and then titles and abstracts were searched with Boolean operators in CINAHL Complete, MEDLINE Complete, PsycInfo, Scopus and Embase databases on 6/01/23. To capture evidence on contemporary roles and work environments of paramedicine clinicians, empirical peer-reviewed articles that focused on the phenomena mentioned in the aim and were published in English between January 2013 and December 2022 were included. To address the international variation in models of care and terminology, studies were included if they focused on civilian, specialist out-of-hospital roles whether paid or volunteer, including paramedics and EMTs. Research with a focus on university students, military medics, or ambulances that were nurse, firefighter, or physician-led were excluded. Studies that focused on emergency retrieval or response to a natural disaster or terrorist event were also excluded, due to the exceptional nature of these situations. Literature reviews, editorials and grey literature were excluded.
Search terms.
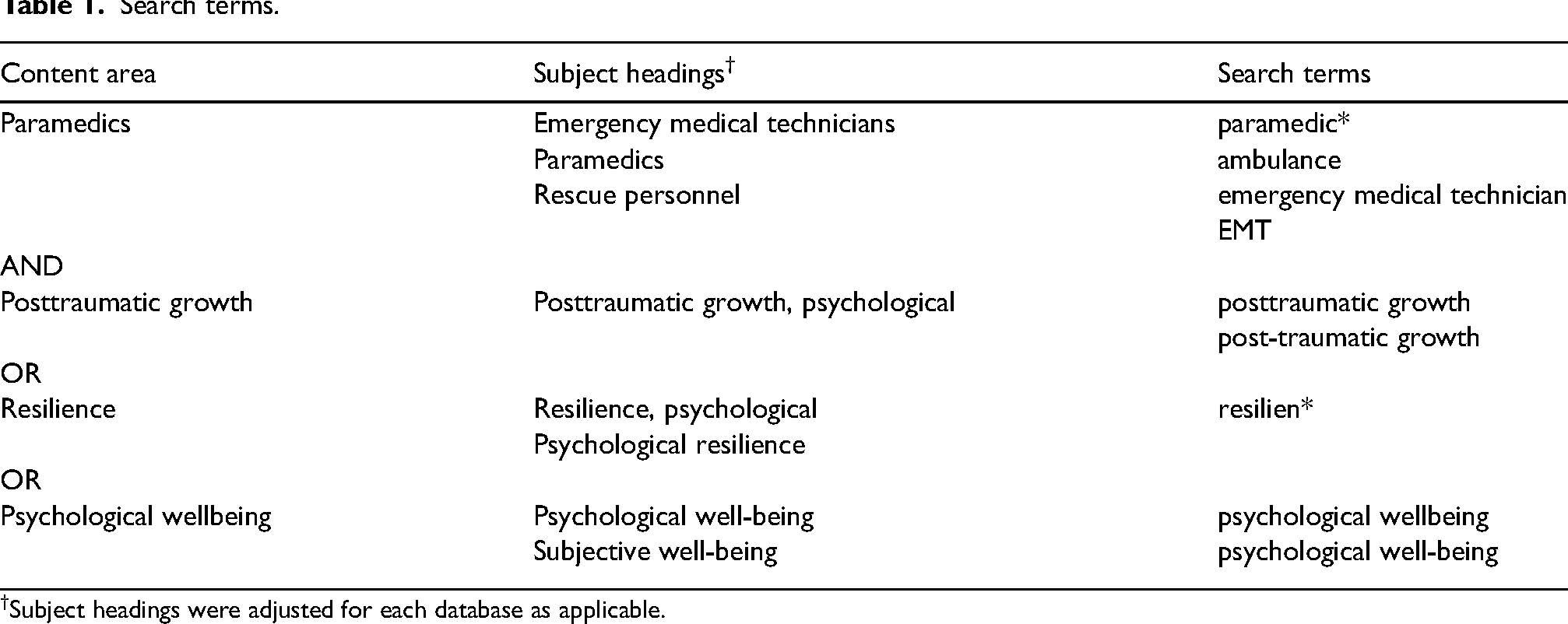
Subject headings were adjusted for each database as applicable.
Quality appraisal
During the data evaluation stage, the screened articles were appraised for methodological quality. Qualitative studies were evaluated using the Checklist for Qualitative Research 32 and quantitative studies were evaluated using the Critical Appraisal Checklist for Cross-Sectional Study. 33 Two authors independently appraised the articles, with a consensus discussion with a third author to resolve discrepancies. Consistent with Soikkeli-Jalonen et al., 34 appraisal criteria were scored as either yes (1), or no or unclear (0), with a total score calculated for each article as an indication of relative quality. Although a range in quality was identified, due to the limited existing research in the field, no papers were excluded based on this appraisal. However, the quality ratings and limitations are reported for each study.
Data extraction and analysis
Data analysis was performed by sequentially progressing through the stages of data reduction, display, comparison, conclusion drawing and verification. Data from each of the included studies relevant to PTG, resilience, or psychological wellbeing of paramedicine clinicians were extracted by one author independently. Extracted data were confirmed with the other authors and compiled into a data matrix. To guide the analysis, the constant comparison method was applied, 35 with data continually compared across studies and against previously analysed information. This enabled categories to be systematically developed and iteratively refined until final categories and sub-categories were determined. The four main category findings are reported using narrative synthesis.
Results
Search outcomes
The initial search returned 405 articles, which were managed using Covidence software. 36 Titles and abstracts were scrutinised against the inclusion and exclusion criteria by two authors independently, to yield 61 studies for full-text extraction. Full-text articles were then screened against the criteria, with consensus discussion with a third author. Thirteen relevant studies were included in the review (see Figure 1).
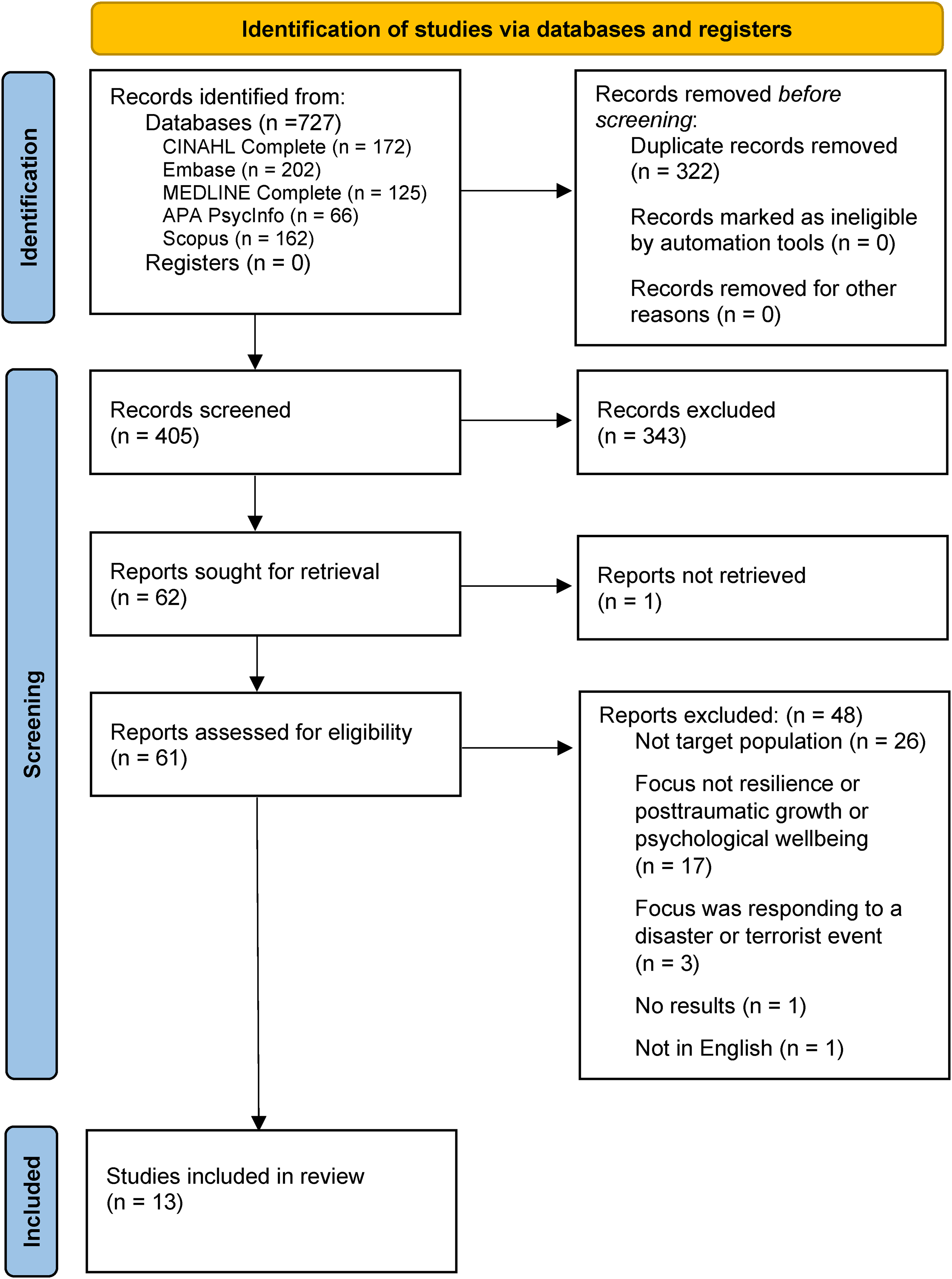
PRISMA flow diagram of the included studies.
Description of studies
Of the 13 included studies (11 quantitative, 2 qualitative), two examined PTG and resilience,37,38 one resilience and psychological wellbeing, 39 and the remaining studies examined one outcome: PTG (n = 2),40,41 resilience (n = 6),42–47 or psychological wellbeing (n = 2).48,49 Studies were from Australia (n = 2), the United Kingdom (n = 2), Germany/Austria (n = 2), and one from Saudi Arabia, USA, Portugal, Slovakia, New Zealand, Poland and Switzerland/Liechtenstein. Participants fulfilled paramedicine clinician roles at a range of clinical levels, with most studies including paramedics (n = 9) or EMTs (n = 5). Three studies included volunteers and paid staff and three reported participants to be operational ambulance personnel, without further specification (see Table 2 for a summary of included papers). Findings are reported under four main categories, wherein three focused on PTG, resilience and psychological wellbeing, each with their respective sub-categories, outcomes, associated factors and experiences. As per the aim, the fourth main category addresses the relationship between the three phenomena of interest.
Summary of the included papers (n = 13).

AO: ambulance officer; AP: ambulance personnel; CSD: cross-sectional design; EMT: emergency medical technician; F: female; FT: full-time; ICP: intensive care paramedics; Ma: male; Para: paramedics; SR: self-report; vol: volunteers.
* Critical Appraisal Checklist for Cross-Sectional Study. 33
** Checklist for Qualitative Research. 32 Item 12 of the Cross-Sectional Study tool (‘Can the results be applied to your organization?’) was omitted as it was not relevant to this review.
Posttraumatic growth
Posttraumatic growth outcomes
All four studies investigating the PTG of paramedicine clinicians were cross-sectional and used the Posttraumatic Growth Inventory (Table 2). 10 Mean overall PTG ranged from 43.38, SD = 15.03 41 to M = 68.52, SD = 17.99, 38 with scores typically reported as moderate.37,40,41 The PTG domains where clinicians showed the most growth were Appreciation of life,37,38,40 Personal strength37,40 and Changes in self-perception. 38 Most studies did not identify the types of traumatic events that elicited growth; however, Ogińska-Bulik and Kobylarczyk 38 indicated that the most common categories were injury, dying, death of a child (30.63%) and threatening or aggressive patients (11.29%).
Factors associated with posttraumatic growth
Studies examined PTG in relation to demographics (n = 3),38,40,41 as well as variables related to the role, trauma exposure and coping or dispositional style (n = 3).37,40,41 The demographic variables reported did not have a significant relationship with PTG, including gender40,41 and age. 38 Role-related factors were significant, with EMTs demonstrating higher levels of PTG than paramedics (M = 55.6, SD = 24.4 and M = 42.6, SD = 22.8, respectively, p = 0.03). 37 A shorter shift duration was also associated with higher levels of PTG (r = −0.16, p < 0.01). 41 Conversely, the length of service was consistently not found to be significantly related.37,40,41
In the wake of a traumatic event, the amount of time that had passed was not found to have a significant relationship with PTG, 40 although a positive correlation was found between PTG and a positive change in outlook (r = 0.62, p < 0.001). 37 Regarding posttraumatic stress, when examining a low-scoring PTG subset, those with higher posttraumatic stress symptom scores showed significantly higher PTG than those with fewer posttraumatic stress symptoms (M = 42.29, SD = 13.36 and M = 24.71, SD = 9.52, respectively, p < 0.05). 41 However, PTG was typically found to be independent of posttraumatic stress symptoms.41,50
Coping-related variables included participants’ expression of interest in coping training, 37 coping strategies, 40 and sense of coherence. 41 Paramedicine clinicians who expressed interest in coping training were found to have significantly higher PTG than those who did not (M = 57.62, SD = 22.36; M = 36.24, SD = 20.30, p = 0.001). 37 When examining coping strategies, Jurišová 40 reported significant positive correlations with PTG and Active coping (r = 0.400), Planning (r = 0.355), Focus on and venting emotions (r = 0.371, p < 0.01), as well as Suppression of competing activities (r = 0.307), Seeking social support (r = 0.290), Use of emotional support (r = 0.303) and Behavioural disengagement (r = 0.256, p < 0.05). Positive correlations were found with Restraint (waiting for an appropriate time to act), and the PTG domain New possibilities (identifying new possibilities in life) (r = 0.272, p < 0.05), and also between the PTG domain Spiritual change (understanding spirituality, strength of faith) and both Religious coping and Substance abuse (smoking) (r = 0.524; r = 0.354, p < 0.01). 7 In addition, Self-efficacy and Positive affectivity (feeling enthusiastic, active) moderated the relationship between situational coping strategies and PTG.40,51 Positive correlations were found between the dispositional orientation Sense of coherence (capacity to manage stressful events and find meaning) and PTG (r = 0.27, p < 0.01). 41 The only significant negative correlation with PTG and a coping strategy was between Mental disengagement (distraction) and the PTG domain Personal strength (confidence responding to challenges) (r = −0.0263, p < 0.05).7,40
Experience of posttraumatic growth
No qualitative studies explored paramedicine clinicians’ experiences of PTG.
Resilience
Resilience outcomes
Seven quantitative studies examined resilience using a variety of measures, including versions of the Resilience Scale (n = 4) (RS-11, RS-14, RS-25), 52 Brief Resilience Scale (n = 2), 53 and Resiliency Assessment Scale 54 (Table 2). Studies that reported scores against control groups or population means indicated that paramedicine clinicians’ resilience ranged from average38,45 to above average.37,42,46 In describing the distribution of clinicians’ resilience scores, Fonseca et al. 43 reported that 47.4% were high, 46.2% moderate and 6.4% low.
Factors associated with resilience
Of the seven quantitative studies reporting factors associated with resilience, two examined demographics,42,46 five coping and disposition-related variables,37,38,43,46,47 two role-related factors,37,45 and five burnout and response to trauma.37,42,43,46,47 There were mixed results for gender, with some evidence of significantly higher resilience scores in females (females M = 66.91, SD = 6.17; males M = 65.60, SD = 6.82, p < 0.05), 46 but no significant difference found by other researchers. 42
Personality traits positively correlated with resilience included Bold (unusually self-confident) and Diligent (meticulous, critical) (r = 0.23; r = 0.15, p < 0.001), as well as Colourful (expressive, dramatic) and Imaginative (creative, unusual) (r = 0.12; r = 0.10, p < 0.05). 47 Sense of coherence was also positively correlated with resilience (r = 0.52, p < 0.01), 46 and clinicians who expressed interest in coping training had significantly higher resilience scores than those not interested (M = 23.3, SD = 3.59; M = 22.22, SD = 4.40, p = 0.02). 37
Conversely, negative correlates of resilience included Dysfunctional coping (r = −0.19, p < 0.001), with dimensions of resilience significantly explaining 5.1% of Dysfunctional coping’s variance (p < 0.001). 43 Similarly, Treglown et al. 47 found resilience was negatively correlated with the self-defeating behaviour Moving away (socially isolating under stress) (r = −0.29), and also with the three sub-traits Cautious, Excitable and Reserved (r = −0.35; r = −0.30 and r = −0.19, p < 0.001).
Regarding role-related variables, several characteristics of employment were found to be impactful on resilience, with Sense of workplace belonging significantly predicting 9.8% of its variance (p < 0.001). 45 The nature of employment was also identified as a factor relevant to resilience, with part-time participants reporting significantly higher scores than full-time (M = 25.27, SD = 2.94 and M = 22.21, SD = 3.97, respectively, p = 0.005). 37 There was some evidence of a relationship with the length of service, with a multiple regression analysis finding this as a significant negative predictor of resilience, although explaining only 1% of variance (p < 0.001). 45 No significant relationship was found with the length of service in other research. 37 Regarding support in the workplace, Streb et al. 46 reported that although access to psychological help after a traumatic event was linked to less severe PTSD symptoms, access did not significantly affect resilience. They also found no significant relationship between resilience and receiving trauma training. However, this was a retrospective self-report of various types of training, ranging from external to internal, multi or single session rather than one standardised intervention.
The five studies that investigated resilience’s association with burnout and the response to trauma consistently found negative correlations with resilience and perceived stress (r = −0.32, p < 0.0001), 43 secondary stress (r = −0.66, p < 0.001), 37 PTSD severity (r = −0.225, p < 0.01), 46 and Negative change in outlook (r = −0.65, p < 0.001). 37 Resilience also moderated or mediated the relationship between specific personality traits and burnout, with the trait Bold being mediated by resilience and the trait Diligent being moderated by it (p = 0.011 and p < 0.001, respectively). 47
Experience of resilience
Two qualitative studies explored the experience of resilience.39,44 Personal and early life challenges could be a double-edged sword, equipping clinicians with emotional reserves and strengths that were useful in their workplace; however, family and childhood memories could be triggered by resonant cases, causing distress. 39 When describing the coping strategies used to maintain resilience, paramedics discussed using humour to alleviate tension, as well as compartmentalising and focussing on medical interventions to emotionally distance themselves from traumatic scenes. 39
Clompus and Albarran 39 also found that role-related factors were pertinent, with non-medical cases such as mental health or alcohol-related incidents negatively impacting paramedics’ resilience and contributing to emotional fatigue. The authors linked this finding to the emotional labour of attending such cases, as well as masculine cultural norms in the workplace, which value traumatic physical injuries and critical illnesses, while devaluing non-medical cases related to mental health or substance use. 39 In addition, while coping with workload challenges, an overbearing managerial gaze was described by paramedics as detrimental to their ability to provide care and contributed to exhaustion. Similarly, clinical supervisors’ mentoring style was described as either supportive or detrimental to resilience, with Coaching (briefing, ensuring comfort, modelling) seen as positively contributing, and other styles such as Bossing (short, blunt orders) and Criticising (publicly critiquing decisions) perceived to be damaging. 44
Informal and formal support, either in the workplace or externally, was also found to be related to resilience. Paramedics reported that organisational support and peer networks were invaluable to help process emotions, and described how support from family and friends was important in this setting. 39 However, paramedics also felt unable to disclose feelings, both from a desire to shield others from distress, but also because of shame associated with masculine-dominated workplace culture, where feelings were not discussed. 39
Psychological wellbeing
Psychological wellbeing outcomes
One qualitative and two quantitative studies reported on paramedicine clinicians’ psychological wellbeing (Table 2). One quantitative study adapted a survey previously used by the World Health Organization regarding healthcare worker wellbeing, 48 and the other used a validated measure of psychological wellbeing, the Short Warwick–Edinburgh Mental Well-being Scale (SWEMWBS).49,55 The SWEMWBS indicated that paramedics had moderate psychological wellbeing scores (M = 25.25, SD = 4.53).49,55
Factors associated with psychological wellbeing
The two quantitative studies that investigated psychological wellbeing48,49 did not report results against demographic variables. However, they identified relationships between wellbeing and the internal workplace environment, and external support. Within the workplace, Manager psychosocial safety climate and Manager behaviour were both found to have significant positive linear relationships with wellbeing, respectively, explaining 13% and 10% of psychological wellbeing variance (p < 0.01). 49 A significant association was also found between having time for friends and paramedics’ perception of being welcomed by them (χ2 = 6.893, p = 0.009). 48
Experience of psychological wellbeing
One qualitative study with a small cohort (n = 7) from the United Kingdom explored paramedics’ experience of psychological wellbeing, and identified the importance of internal and external support. 39 Internal support from peers was described by paramedics as instrumental to wellbeing, such as receiving constructive feedback on their clinical performance after challenging cases, ultimately helping them resolve concerns that they would otherwise ruminate upon. 39 Externally, family and friends were also perceived as essential sources of support. 39
Relationship between posttraumatic growth, resilience and psychological wellbeing
There were no studies that directly investigated the relationship between wellbeing, resilience and PTG; however, two quantitative studies investigated the relationship between resilience and PTG.37,38 Although Austin et al. 37 did not establish a significant direct correlation between the two outcomes, Ogińska-Bulik and Kobylarczyk 38 did find that a number of coping strategies significantly affected their relationship. When examining how the predictor variable resilience was associated with the dependent variable PTG, coping strategies Venting and Denial were found to suppress the relationship between PTG and resilience and their subfactors (p < 0.05). Furthermore, the coping strategy Planning was found to mediate the relationship between PTG and resilience (p < 0.05).
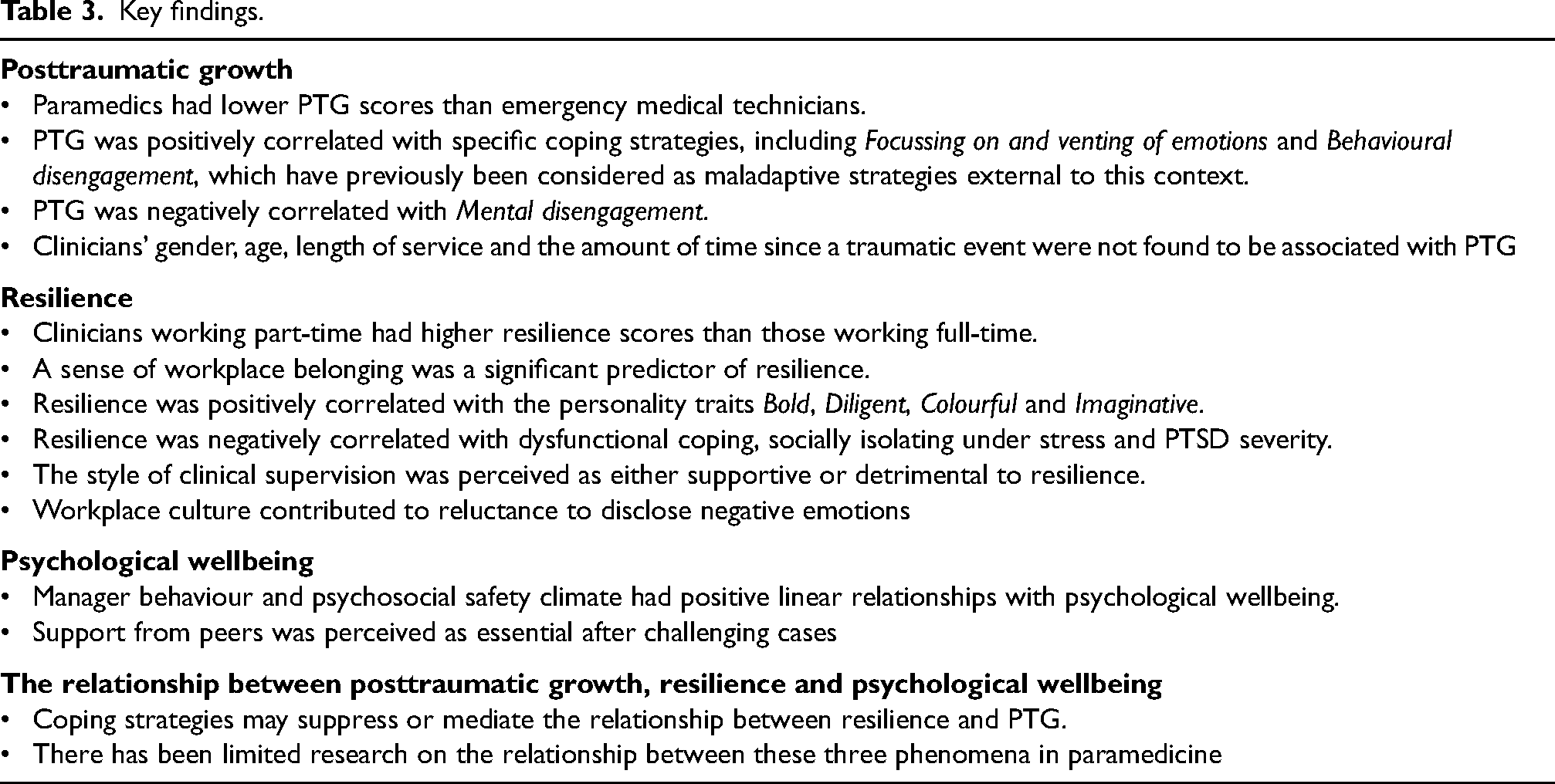
There were several key findings from the review across all four categories, which are summarised in Table 3.
Key findings.
Discussion
This review synthesised evidence on the PTG, resilience and psychological wellbeing of paramedicine clinicians, including the experience of these phenomena and their relationship. Paramedicine clinicians can experience workplace stress and psychological trauma directly and vicariously, and it is evident from this review that a number of factors are involved in strengthening or reducing their PTG, resilience and psychological wellbeing. The quality of included studies varied, with all meeting at least 45% of the appraisal criteria. Shortcomings were primarily noted in the reporting of response rates, statistical power of samples and acknowledgement of researchers’ cultural and theoretical position. The determined appraisal scores suggest the need for increased rigour in design and reporting of future research in the field. There was some variation in the quality of scales used; however, Cronbach’s alpha scores were in the optimal range, between 0.79 and 0.94 (Table 2). 56 Although adaptation and translation of some scales can pose a threat to their previous validation studies, alpha scores for those measures remained within desirable parameters.
With regard to PTG, the correlation of role-related factors shows that workplace demands and employment structure can be impactful. While further research is needed to confirm relevant causes of paramedics’ poorer PTG compared with EMTs, studies have found that paramedics have a higher risk of anxiety, stress, depression, 57 and burnout. 58 Suggested contributors to this disparity include pressure from paramedics’ greater clinical scope and responsibility, as well as increased exposure to critically unwell patients. 58 There is also evidence that paramedics experience workplace incivility more frequently than EMTs, with organisational culture and coping mechanisms of co-workers experiencing high stress suggested to be contributing factors. 59 In addition, although working longer hours is known to be associated with mental distress, depression and anxiety, 60 the finding in this review that longer shift duration is associated with lower PTG demonstrates a potential risk to paramedicine clinicians’ capacity for growth after trauma. From these findings, it is evident that the development of PTG can be either supported or undermined by malleable organisational factors and is not purely reliant upon the personality traits or dispositions of individual paramedicine clinicians.
The relatively stable dispositional variables found to be pertinent to PTG outcomes, such as Sense of coherence and Positive affectivity may steer optimal recruitment; however, organisations and paramedicine clinicians also have agency in the pathway to PTG, through utilisation of the identified coping strategies. These include Active coping, Planning, Focus on and venting emotions, Suppression of competing activities, Seeking social support, Use of emotional support and Behavioural disengagement. Although connections have been found between paramedicine clinicians’ personality types and coping skills, 61 psychoeducation can positively impact the underutilisation of adaptive coping strategies in the healthcare setting. 62 Interviews with paramedics have suggested that supportive programs such as this should not only be embedded in early career education, but should be ongoing, as new experiences give personal relevance to the targeted skills. 63 Coping skills identified as supportive of PTG in this review, such as Focus on and venting emotions and Behavioural disengagement, have been considered less adaptive outside of this context, 64 and subsequently may be overlooked in professional development design. The positive role of venting emotions also provides evidence to support the reform of workplace culture, where expression of emotion can be considered a taboo.
Although the resilience scores of paramedicine clinicians were typically average and above average, the measurement of resilience across the studies varied (Resilience Scale, Brief Resilience Scale, Resiliency Assessment Scale). These measures differ in their conceptualisation of resilience as either a stable trait or adaptable ability of an individual. Importantly, none of these measures adequately take external factors into account, such as clinicians' interaction with the workplace environment. 65 This indicates an opportunity for future research to align with contemporary understandings of resilience and implement a resilience measure designed specifically for the workplace environment, such as the Resilience at Work Scale. 66 This may highlight underexamined external factors of resilience in the workplace, and help to address issues of workplace culture including stigmatised views of resilience as solely a personal responsibility.
Similar to the findings for PTG, higher resilience scores were associated with some relatively stable factors, such as Sense of coherence and personality traits Bold, Diligent, Colourful and Imaginative. However, a number of manipulable correlates were found, including dysfunctional coping strategies, providing guidance for optimising professional development programs. Future investigation of the efficacy of the current training programs is required, specifically those targeting resilience for practicing paramedicine clinicians, as this has not been addressed in the literature. At this stage, programs have been effective for paramedic students67,68 and other healthcare workers. 69 Further research is also required to explain the lower resilience scores for full-time paramedicine clinicians; however, full-time shift work in healthcare has been linked to reduced coping with work demands, poorer mental health, poorer social relationships and work/family conflict.70,71 In addition, paramedics have reported significantly lower perceived social support compared to some other public safety personnel. 72 Irrespective of the cause, providing flexibility in employment fractions may allow organisations to support resilience for some clinicians.
Despite females often accounting for an increasing proportion of the paramedicine workforce,73,74 this review identified that masculine cultural norms for paramedicine clinicians to be stoic and perform heroic work 75 not only persist, but also are detrimentally linked to resilience and psychological wellbeing. With effects including the invalidation of mental health and substance-use-related cases, suppressing the disclosure of emotions, and potentially detrimental interactional styles of managers and clinical supervisors, cultural reform programs should target all staff from frontline to managerial.
Recommendations
From the review of the emergent literature, it is recommended that organisations take a proactive role and support clinicians with tailored continuing professional development programs that target the identified coping strategies. These include Active coping, Planning, Focus on and venting emotions, Suppression of competing activities, Seeking social support, Use of emotional support and Behavioural disengagement. Dysfunctional coping styles such as socially isolating under stress should also be targeted for behavioural change. This ensures programs are aligned with the evidence on how to best support PTG and resilience for this group. This review has also identified a need for further research evaluating the implementation and outcomes of wellbeing, resilience and PTG interventions for this workforce. In addition, future research could explore the relationship between PTG, resilience and psychological wellbeing and pursue in-depth qualitative exploration of how paramedicine clinicians maintain wellbeing and resilience in the face of psychological trauma and workplace adversity. Due to the lack of prior qualitative literature on paramedicine clinicians’ experiences of positive outcomes following adversity, there is a need for further understanding of these phenomena.
Strengths and limitations
This integrative review was systematically conducted and contributes new synthesised understandings of how paramedicine clinicians can best be supported through trauma and adversity, by identifying the known factors important for PTG, resilience and psychological wellbeing. These findings can guide the development of evidence-based programs for paramedic staff and students, and be informative for future research in this field. The evidence on wellbeing, resilience and PTG is emergent in the field, so results are bound to the limited current literature, which primarily comprised cross-sectional studies that used convenience sampling. Due to this, as well as the conceptual variation evident in the existing literature in paramedicine and the heterogeneity of resilience and wellbeing measures in the included studies, a meta-analysis was not feasible.
Conclusions
This review synthesised what is known on PTG, resilience and psychological wellbeing of paramedics and other clinicians in paramedicine. These distinct, but interlinked outcomes underpin a strength-based approach to how paramedicine clinicians can persevere and flourish after workplace adversity. To strengthen clinicians’ PTG, resilience and psychological wellbeing, paramedicine organisations may consider providing employment fraction flexibility or reducing shift duration. Operational organisations and educational institutions can also implement professional development programs that are aligned with the evidence regarding adaptive and dysfunctional coping. In addition, masculine paramedicine culture and managerial styles that disrupt psychological safety have been found to undermine positive outcomes for paramedicine clinicians, adding weight to existing calls for systemic cultural reform. For a comprehensive understanding of paramedicine clinicians’ positive psychological adaptations, further investigation is needed into the relationship between PTG, resilience and psychological wellbeing, as well as the efficacy of interventions to strengthen them.
Supplemental Material
sj-docx-1-pam-10.1177_27536386231206501 - Supplemental material for Resilience, posttraumatic growth and psychological wellbeing of paramedicine clinicians: An integrative review
Supplemental material, sj-docx-1-pam-10.1177_27536386231206501 for Resilience, posttraumatic growth and psychological wellbeing of paramedicine clinicians: An integrative review by Benjamin Coyte, Vasiliki Betihavas, Scott Devenish and Kim Foster in Paramedicine
Footnotes
Acknowledgements
There are no acknowledgements.
Author contributions
All authors listed in this manuscript meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors. All authors agree with the content of this manuscript.
Declaration of conflicting interests
Scott Devenish is an Associate Editor with Paramedicine; the other authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.