
Abstract
Introduction
Clinical reasoning (CR) among healthcare professionals working in emergency medical services (EMS) who focus on ambulance care is a vital part of ensuring timely and safe patient care. The EMS environment continually fluctuates, so clinicians constantly need to adapt to new situations. Organizational support is described as important for CR, but overall, research on organizational influences for CR in an EMS context is lacking. An increased understanding of these influencing factors can assist in the development of EMS by strengthening CR among clinicians. Therefore, the purpose of this study was to investigate the organizational factors influencing EMS clinicians’ CR.
Methods
Using a qualitative single case study design, an EMS organization in southwestern Sweden was explored. Data were collected from participant observations of patient encounters, individual and group interviews with clinicians and organizational representatives, and organizational document audits. Data were analyzed using qualitative content analysis and triangulation of data sources.
Results
The results revealed several organizational influencing factors. Collaboration and information sharing internally and externally were emphasized as essential components influencing CR. Additionally, the structure for the clinicians’ ‘room for action’ appeared confused and created uncertainties for CR related to decision mandates.
Conclusion
The conclusion is that organizational factors do play an important role in clinicians’ CR. Moreover, the EMS community needs to develop suitable forums for discussing and developing these influencing factors across organizational hierarchies. Finally, clarification is needed on clinicians’ ‘room for action’ within their own organization but also with possible collaborators.
Keywords
Introduction
Understanding how an emergency medical services (EMS) organization can support its clinicians’ clinical reasoning (CR) processes is integral to the organization's ability to provide quality care and treatment while maintaining patient safety under the fluctuating and stressful conditions surrounding EMS, with a focus on ambulance care.
CR is defined as a cognitive process for gathering, analyzing and integrating information to make decisions regarding a patient's care and treatment. CR is closely related to clinical decision making in terminology and often used interchangeably. CR is the overall process of thinking during clinical practice, while clinical decision making emphasizes the outputs of decisions made. However, while there are models for decision making styles there is no one model for how CR is conducted. 1 The ability for CR is influenced by individual and group differences, level of experience, as well as organizational and social factors or specific elements in the situation at hand. Previous research on CR in EMS describes this as an iterative or fluid process that involves more than only patients’ care and treatment. The iterative process is reflected in EMS assignments as information can be presented and altered at any point for which the EMS clinician needs to adjust their reasoning. The iterative process is also related to the EMS assignment consisting of a number of tasks of various complexity, where some tasks are present for the beginning to the end of the assignment.2,3 Evidence has shown that creativity is needed to adapt to this fluid EMS environment.3,4
The main purpose of EMS is to provide timely and safe patient care and treatment in a range of settings. 5 Decisions regarding care and treatment emphasize clinicians’ knowledge and real-world experience, as the diverse and fluid context of EMS, can create uncertainties, which, in turn, pose threats to patient safety.2–4
Standards related to the level of care provided, educational demands on clinicians and the staffing of ambulance vehicles differ across countries.5–8 In short, the staffing and care provision standards can be explained as either basic or advanced life support (BLS or ALS), and conducted either by a Franco-German or Anglo-American model or a hybrid of both.6–8 The Franco-German relates to a ‘stay and play’ approach, where EMS clinicians can treat patients at the scene with the potential for referring or non-conveying. It also includes the possibility for by-passing the emergency department, making admission directly to specialist care. The Anglo-American model relates to a ‘load and go’ approach, where EMS clinicians instead transport patients rapidly to an emergency department for physician assessment. Regardless, CR and the quality thereof are key to providing patients with safe care. In addition to differences between individual and group characteristics, CR also differs according to organizational support structures, such as work environment, equipment used, and supportive structures.
Organizational development in Western healthcare facilities has been influenced by several management models over the last decades (i.e. lean production or new public management), frequently emphasizing efficiency improvements and/or reduction of costs amongst other elements of safe patient care delivery.9,10 For EMS, this has meant reducing the number of patients transported to the hospital by focusing on referrals to an appropriate level of care, care pathway, or through non-conveyances. However, these referrals and non-conveyances could also be viewed as a more person-centred approach, saving the patients from frequent and potentially unnecessary uncomfortable hospital visit, as well as increasing availability of EMS resources.11,12 These decisions add to the importance of CR with a risk minimizing approach. 13
Research specifically intended to examine organizational factors (i.e. work and healthcare environment, supportive structures, in-service training, workplace culture) related to CR in EMS is lacking, while more research has been conducted within related sectors and professions in public sector service work (i.e. health, welfare and education). It presents that measurability and increased focus on time and cost efficiency undermine professional knowledge and decision-making, leading to an increased standardization, formalization and regulation of methods for work. 14 EMS and other healthcare work is commonly protocol directed,15,16 which is appropriate in certain situations while in others, clinicians’ discretion is of greater importance. However, clinicians must adhere to these protocols to avoid repercussions from their organization and to avoid lawsuits if there would be a poor outcome for the patient. 4 However, these protocols provide limited support for CR4,17 and are utilized in different ways depending on the profession. 18 Other aspects of organizational influencing factors described mostly related to clinicians’ workloads, work environments or lack of supportive structures4,19–21 in relation to their health and well-being. Studies concerning the perspective of healthcare managers have reported restricted decision-making autonomy, 22 which is a challenge in public sector service professions overall. 23 Seemingly, various influencing factors have been studied and reported on in the context of EMS but not in relation to CR.
Supportive structures and awareness of potential influences within the organization are considered vital to providing safe patient care, but it is also vital for clinicians to be able to perform well and to feel satisfied with their work contribution. Thus, both patients and clinicians, as well as EMS organizations, can benefit from investigating the organizational for CR. Therefore, the purpose of this investigation was to explore the organizational influencing factors on EMS clinicians’ CR in a naturalistic environment.
Methods
An explorative, qualitative design was undertaken in the form of a single case study, 24 with a focus on organizational influential factors for clinicians’ CR in a specific EMS organization.
This study encompasses a realistic critical perspective acknowledging that knowledge can be gained through objective and subjective measurements as well as interpretations. 25 To some extent, this differs from Yin's positivistic perspective. 24 With a more generalistic approach than for example Robert Stake's, the authors strive to understand what could aid in building future models or theories using a more encompassing perspective rather than focusing in detail on the specific case. 26
Setting and sample
The case consisted of an EMS organization in southwestern Sweden. It served a 6956 km2 area with a population of approximately 300,000, including both medium-sized cities as well as rural and sparsely populated areas, with populations ranging from 9500 to 114,000. The organization operated 9 stations, with 11 around-the-clock ambulances and an additional 4 daytime ambulances that ran on weekdays. It employed BLS and ALS clinicians for example emergency medical technicians and registered nurses (minimum of one registered nurse is required in every ambulance) and organizational representatives (ORs), which included first line managers, lead physicians, administrative staff (i.e. healthcare developer), and an operations manager. The organization employs a hybrid of the Franco-German/Anglo-American models.
A purposive sampling strategy was used to recruit participants throughout the organizational hierarchy. Clinicians (observations and group interview) were recruited mainly through oral presentations at workplace meetings, informational emails and station bulletins. The ORs (individual interviews) received invitations via email, which contained an information letter. Observations and interviews were booked based on the participant's preferences. All participants received written and oral information regarding the study prior to participation and upon beginning data collection. All participants gave written (observations) or oral (interviews) consent for participation.
Data collection
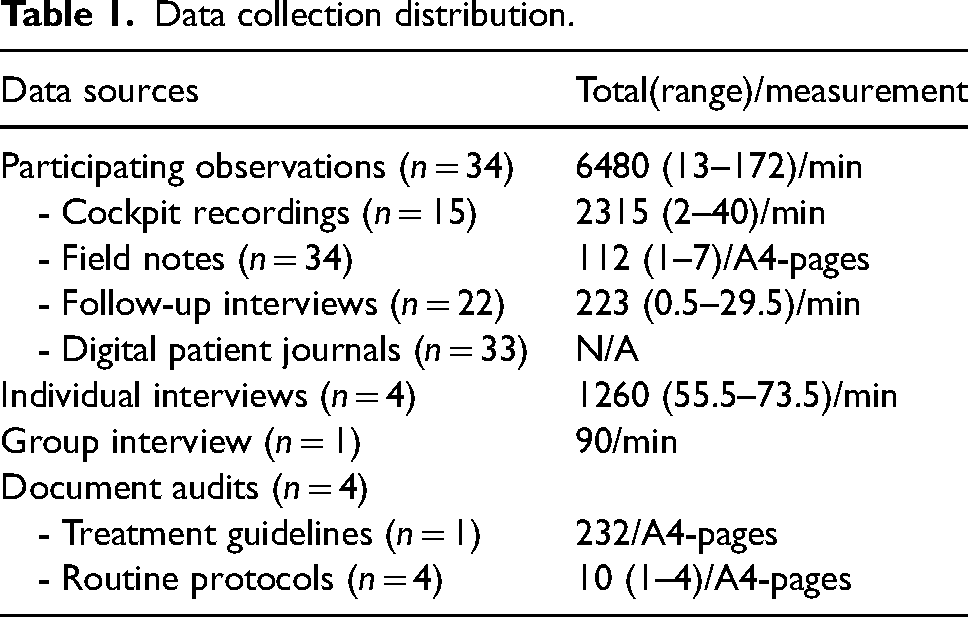
A variety of sources were used for data collection (Table 1). The focus of data collection was on documenting various organizational influencing factors for CR. Field notes and recordings were transcribed verbatim, numbered accordingly, and identifying information altered to maintain confidentiality of the participants.
Data collection distribution.
Observations
Participant observations were conducted between September 2019 and May 2020. Initially, an observation protocol was pilot tested to evaluate a possible structure for recording field notes during the observations. The pilot study indicated that the protocol was too rigid and that field notes should be captured spontaneously, referring to the protocol for reminders. The pilot also confirmed the need to audio record the ambulance cockpit en route to the patient. Clinicians were observed for their full work shift (8–14 h, night/day) and were asked to work as usual and ignore the observer. Several sources such as audio recorders and observer fieldnotes were used to catch audible and visible aspects of organizational influencing factors for CR. After each observation, if operational demands permitted, a follow-up interview was conducted, during which questions from the observed patient encounter were addressed (Supplemental material). A digital patient journal linked to the observations was audited for descriptions related to influential factors.
Interviews
All interviews (individual and group) were carried out through a videoconference program 27 due to the COVID-19 pandemic. Audio was recorded through the program and with a digital voice recorder (Olympus-WS-210S); and saved on a local computer hard drive in a password-protected file. Before starting the interviews, the following description of CR was provided to the participants: ‘CR is a reasoning process that involves gathering, analyzing, discarding and utilizing information to make decisions about care, treatment or other vital aspects of the mission’. Participants were allowed to ask questions for clarification, if needed. All interviews included open-ended questions along with suitable follow-up questions (Supplemental material). To maintain the integrity of the ORs whilst providing the possibility to share potentially negative critique, these interviews were individual. However, with the clinicians a group interview was employed to see if there were other influential factors which might had gone unnoticed or unencountered during observations.
Data analysis
Basic qualitative, inductive and manifest content analyses were conducted, along with a triangulation of the data sources. 24 Data were entered into a computerized software program, ATLAS.ti (v.8.4.25, 2018), 28 for qualitative analysis. The transcribed material was read and inductively coded based on its content in relation to described or observed influential factors; examples of categories are information sharing, collaboration and the work environment. The analysis grouped similar descriptions into clusters, which formed the foundation for subcategories, and later, for main categories. Based on Yin's 24 recommendations for case study research, the coded materials were triangulated, where the data from multiple sources were compared to provide nuanced descriptions in which influential factors are coherent between or contradicted by clinicians and ORs, or in relation to what is stated in policy documents. The first author was responsible for the organization, clustering and initial analysis of the data, while the authors as a group engaged in frequent discussions about the interpretation and the content of the subcategories and categories. This process ended with a common understanding of the results.
Ethical considerations
The study received ethical approval from the Regional Ethics Approval Committee in Gothenburg (reference number: 453-18 and amendment: 2021-06430-02) and adhered to ethical principles of the Declaration of Helsinki, 29 and the Swedish data protection act. 30 The standards for reporting qualitative research guideline 31 have been utilized (Supplemental material).
Results
Participating in this study were clinicians (all RNs with and without specialization) and ORs (Table 2); ORs represented different sections of the organizational hierarchy.
Participant demographics.

The data collection consisted of various sources (Table 1) recording and describing CR and organizational influences. Participant observations included 34 patient encounters across 11 EMS teams (22 EMS clinicians). The semi-structured interviews with individual ORs (n = 4) were conducted January to March 2022, and the group interview took place in May 2020 with three (n = 3) EMS clinicians who had not participated in observations.
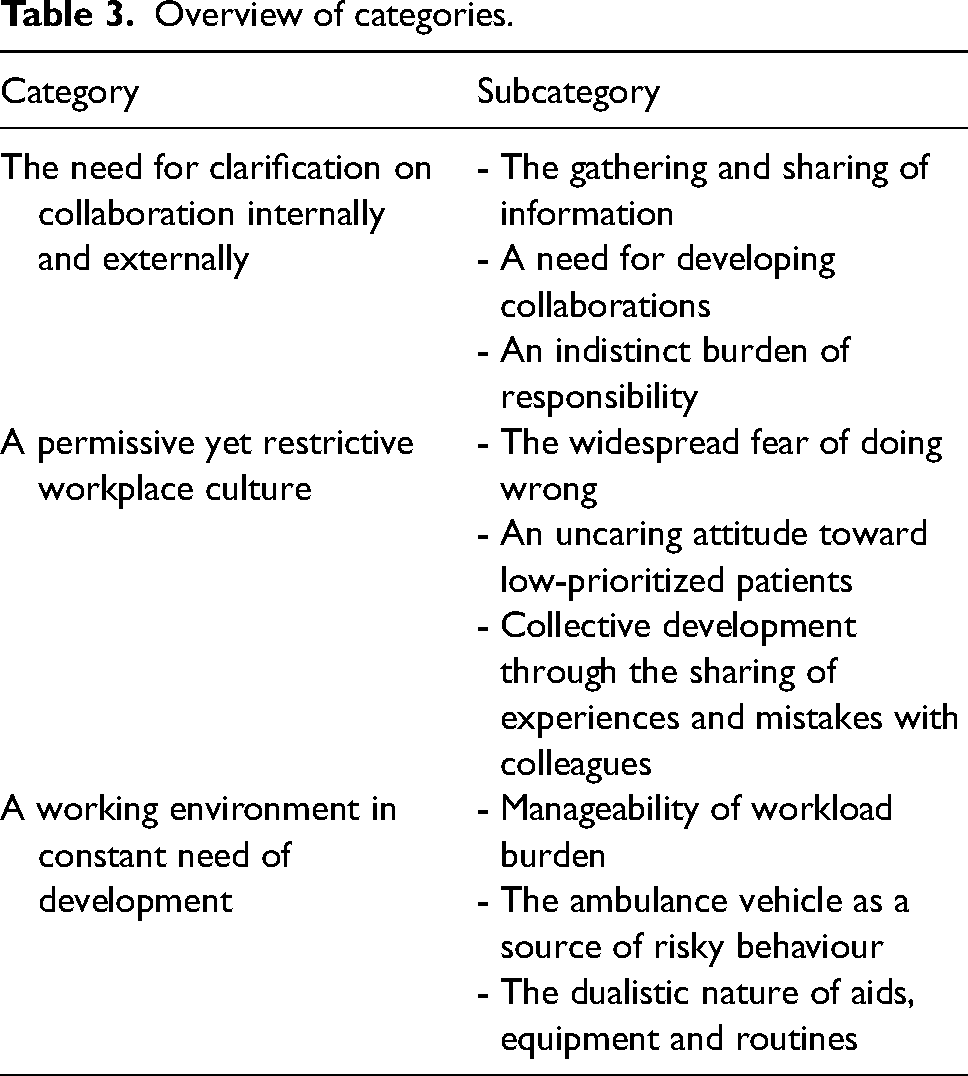
The results present organizational influential factors for CR in a Swedish EMS organization. Overall, communication and openness were described as key elements to a successful internal organizational environment and external collaboration partnerships. The organizational economy was found to have an influence on the development of CR. The results are presented according to three categories with three subcategories each (Table 3).
Overview of categories.
The need for clarification of collaboration internally and externally
Collaboration occurs continuously within the EMS but also with other healthcare organizations, police, fire departments or municipal organizations. The potential for collaboration is a prerequisite for passing CR on to others but also for enabling clinicians to follow through with suitable actions.
The gathering and sharing of information
Clinicians encounter various operators during fieldwork, which creates the need for not only gathering but also sharing information influencing both ongoing and the continuation of patient care. Such information is not restricted to purely medical details but also involve initiating or planning for a patient to receive additional assistance in the home. All collaborative efforts depend on a proper and smooth transfer of information between operators. To aid this function, clinicians are provided with several routines and guidelines, such as reporting structures or triage tools; providing clinicians and other professional carers with a common language. These tools provide security in knowing what information is expected to be gathered and shared. C1: Today, we got the uniform triage system; it provides a structure for all patients. You have a sense of what the minimum requirement of assessment in any given patient care [situation], and it does not matter who does it. (Group Interview)
Clinicians conveyed uncertainty about emergency departments outside their own organization relative to open hours and the kind of patients they accept. Furthermore, they described a flaw in the information sharing structure between other EMS and hospital organizations in the vicinity, resulting in a lack of awareness about recent changes in routines or restrictions in these organizations. Also, the monitoring equipment utilized lacked capability to send data outside of their own organization, which hinders smooth collaboration and information sharing.
The organization has a structure for internal information sharing that is based on video meetings during shift changes, weekly emails, and a web page. Here, clinicians and ORs can get information of practical matters and news. Although positively viewed, limitations were also mentioned; for example, the video meetings rely on clinicians’ availability to attend. In addition, all three information channels can only be accessed through computers at the stations. Also, they create the need for clinicians to keep this information in their minds which burdens the working memory. However, video meetings did provide participants with opportunities to take part in addressing issues related to CR and to discuss practical solutions. For example, discussing treatment intervention of new drugs encountered among intoxications or current problems with equipment and how to work around these during assignments.
A need for developing collaborations
There are differences in the possibilities for collaboration depending on patient location. For instance, gaining access to social services, home care, or the local healthcare centre in the larger and urban municipalities was easier than from the rural areas. However, the clinicians in rural areas did seem to make use of private and personal knowledge to arrange solutions outside of the formal collaboration guidelines and routines. For CR this means that resource availability differs by geographical areas and has to be known or accounted for.
Having the opportunity for exchange or shadowing various collaborators provided a chance to develop and enhance knowledge and improve CR relative to specific care provision. Exchanges also provided both sides with an understanding of the other's areas of expertise and work processes. Finally, there is a desire for enhanced collaboration between EMS organizations, suggesting a national standardization of work routines and equipment. This is something that is believed to reduce the amount of information clinicians need to keep in their mind, easing the related CR.
An indistinct burden of responsibility
All personnel were viewed as a unit that needed to take collective responsibility for the operations and development of the organization. The organization provided structures and tools to shape this activity, as well as the formalities with mandates. However, these structures and formalities were not clear on the matter of responsibilities in clinical work and, thus, influenced CR in terms of insecurity. This presented itself mainly through interactions with patients, bystanders and other healthcare personnel, where EMS was perceived as a transportation unit and questioned the need for assessment. This influences CR and the execution of suitable care activities and decisions, as information may not be provided as expected. Additionally, the organization places emphasis on clinicians to conduct proper assessments and to make decisions regarding the most suitable level of care and transportation. However, the clinicians’ decisions seemingly could be overruled by other operators, such as physicians at the local healthcare centre or a police officer who might insist on transportation by ambulance. These overruling could influence clinicians to become insecure in their CR process, making less effort in the future, however, it could also make them more confident to stand their ground. EMS seemingly was one of few collaborative partners that did not have the mandate to say ‘no’ to an assignment, regardless of its healthcare-related vagueness. OR: Clinicians had been called to an address only to arrive there to find a healthy person who had lost their home keys. They called the dispatch for clarification, who said they received the call from the police, who claimed that the person had a simple mental illness and diabetes, and therefore, it would be a healthcare related assignment. (Individual interview 2) OR: There is great focus right now on referring or non-conveying patients, which puts a lot of stress on clinicians. Even if we always say that: ‘This is not a competition and all who need to go to hospital should do so’, it still influences decisions. (Individual interview 3)
Apparently, these fiscally motivated decisions are made by both political and hospital management and are quite common. However, there are uncertainties related to who is going to carry the responsibility if something goes wrong. Participants ‘collectively say that this burden should not be placed upon the individual clinician’ and ORs do all they can to create supportive structures for clinicians to relieve some of the stressors this responsibility causes. Participants indicated frustration related to these decisions, which often added several complications in CR processes as clinicians had to find ways to incorporate these but still maintain a good face for the patient, collaborative partners, and their own moral beliefs. Furthermore, ORs recounted often having to defend the EMS to the overall hospital organization to maintain resources and staff for daily operations. A lack of understanding for the work and care provided in EMS seemed to be present which in turn lead to increased workload. OR: Healthcare today is run on a skeleton crew. I constantly debate with hospital management to keep my clinicians in the ambulances and its effects on patient safety and clinicians’ work environment. (Individual interview 2)
A permissive yet restrictive workplace culture
Clinicians seemed fearful of making mistakes, which sometimes led them to perform certain assessments or documentation to protect themselves from repercussions rather than to benefit patient care. Ambulance missions were viewed as having different values depending on their content. Participants identified a climate for open debate as important to CR.
The widespread fear of doing wrong
ORs emphasized having a high level of confidence in the clinicians’ CR and ability to solve all tasks in a professional and suitable manner. However, clinicians still described feeling a constant fear of making mistakes, although there seemed to be no real consequences for it. Indeed, no evidence was found to indicate if the threat the clinicians felt was real, perceived or where it originated from. Even so, clinicians described producing a more thorough patient journal in cases of referrals or non-conveyance for the sole purpose of protecting themselves. C3: You probably write more because you feel an increased burden of responsibility if there were to be any [bad] consequences, since the increased writing does not benefit the patient – Group interview
An uncaring attitude towards low prioritized patients
Even though participants asserted that the patient and the mission were important and highly prioritized, apparently, it could be influenced by the prioritization of the assignment. During missions with a lower priority, clinicians would stop to get some food or to discuss non-pressing matters with their colleagues at the station. Furthermore, certain communications regarding low prioritized patients who were retrieved at local healthcare facilities or elderly homes demonstrated an uncaring attitude.
This sentiment was also reflected in the linked patient journals, which were sparsely informative and sometimes empty. The patient journals seemed to be given a lower priority than other tasks, but clinicians also could be provided with a new mission before handover was finished and, thus, failed to complete their documentation. As the only possibility opportunity for documenting the patient journal was at the emergency department or at the EMS stations it caused delays in completing documentation, ranging from hours to days. This risked influencing the clinician's remembrance of their CR of the patient encounter which in turn could lead to a poorer description in the patient journal. This in turn could influence the sharing of CR with the following care units.
So called ‘frequent fliers’, are discussed among clinicians but also with ORs; however, finding appropriate solutions and long-term care plans for these patients seems to be difficult, subsequently influencing CR.
Collective development through the sharing of experiences and mistakes with colleagues
Participants expressed the need for an organizational atmosphere in which everyone was encouraged to share their mistakes. This as collective learning and reflection were considered as crucial for CR development. However, finding opportunities for this kind of sharing in terms of days of education or time for collective reflection was challenging. Difficulties primarily stemmed from economic limitations. C1: I believe that additional time for group reflection would help improve CR [C2 and C3 nod approvingly]. As it is now, we only do this at shift changes. These reflections are unstructured, and we often stay after hours on our own accord. (Group interview)
A working environment in constant need of development
Having to conduct CR in highly demanding environments that are not optimally tailored for the work can present both a challenge and an opportunity. The organization appears to do what it can to provide clinicians with different aids and solutions, but the reality warrants additional efforts.
Manageability of workload burden
Clinicians perceived they had sufficient time to conduct proper CR for each patient, but the high workload seemed to influence the process. Clinicians worked a great amount of overtime, leading them to adapt their driving time to finish their shift in the desired vicinity. This was done in an attempt to manage activities in daily life, but clinicians explained that they always had back up plans or various solutions for this. High demand often prevents clinicians from having lunch or a short break, which can influence CR performance. Moreover, it leads to failure to present a patient journal during the work shift; instead, they may be left unwritten for several days, thus influencing the continuation of consistent CR into the next unit of care. However, a high workload can have a positive influence on clinicians and CR. During observations of night shifts, teams that had continual patient encounters communicated more effectively and were less repetitive in their questioning than the teams who could take a short resting period with the possibility to sleep. Finally, some clinicians had additional administrative responsibilities during their shifts (i.e. staffing), which influenced the CR and teamwork during patient encounters.
The ambulance vehicle as a source of risky behaviour
The ambulance vehicle is the only care environment that remains unchanged no matter what. This is the one space and work environment where clinicians should be able to work safely and properly. However, the design of the caring space within the ambulance was not perceived as optimal as clinicians often had to unbuckle their safety harness to get hold of equipment, placing themselves and their patient at risk. In addition, various aspects related to being situated in a traffic environment posed additional risk which needs to be accounted for with CR, for example trying to predict where weather conditions influence the road surface, or anticipating the movement of other individuals in the traffic environment.
The dualistic nature of aids, equipment and routines
The process of clarifying what the clinicians need to do at the start of their work shifts to be updated on current situations and ongoing processes within the organization involved active work. This work called for a good solution for information sharing, something that seemingly needed to improve.
The organization procured equipment and developed guidelines which should aid and support the clinicians. Apparently, these items were not always ideal for clinical work. For example, guidelines should be evidenced based and assist in the quality assurance of clinicians’ assessments by reducing individual variations. ORs reported that guidelines were created based on an expectation of what a clinician minimally needs to know, and that there can be a variation in background experience of clinicians. However, the clinicians perceived the guidelines as too rigid and often had to adapt these to fit the real-world situation. ORs recognized this problem but stated that creating a guideline for every possible situation was impossible, and therefore the guidelines were of a more general nature. Clinicians are expected to apply their experience to contextualize the guidelines, which places a demand on them to actually have sufficient clinical experience and competence. Sufficient support was provided to clinicians who chose to deviate from guidelines and routines if they supported their deviations’ reasoning and accounted for these in the patient journal. OR: Each clinician has the responsibility to be aware of what they can and cannot do…//…there is also freedom in the situation to make adaptations in relation to the guidelines, but these need to be properly accounted for as to why it was deemed necessary to adjust in this specific situation. (Individual OR interview 2)
Technical equipment can also be a cause of concern for clinicians during the implementation phase. Clinicians expressed difficulties in using the new equipment properly, even after receiving a short education on it. The long learning curve influences clinician's confidence in managing it and solving problems arising, which puts an extra load on CR.
ORs were searching for appropriate IT systems that could provide a digital solution for organizational documents, which could ease updating these but also to reduce the amount of information clinicians need to keep in their working memory. Being able to electronically access the patient journal has been considered as a strengthening for CR, as it allows the clinician to provide themselves with a follow-up on patient encounters.
Discussion
The results present several factors present in the EMS organization that can influence CR. Clinicians and ORs seemingly were aware and sometimes agreed on specific factors and had an ongoing discussion for solving issues. Some factors were of a more objective origin, while others were perceived but not spoken, which may relate to a workplace culture. One of the major findings relates to the autonomy placed on clinicians’ CR in their work performance. This reflects a great deal of trust and responsibility for making suitable decisions that must consider multiple perspectives and varied demands. This can be referred to as ‘room for action’ (RFA), meaning the authority to make autonomous decisions.
The RFA comprises three key concepts: organizational context (i.e. EMS guidelines and policies), official laws and regulations and clinicians’ professional competence.14,23 These provide the structures and boundaries to which clinicians need to relate, and thereby influence actions. Clinicians are expected to make decisions and proceed at their own discretion, but these decisions should be within the organizational regulations to be supported and sanctioned otherwise clinicians need to provide valid justification for working outside of these boundaries and guidelines argumentation. 23 This is not an easy task when demands and expectations differ between various stakeholders involved in the care situation. In this study, this is exemplified by clinicians’ need to weigh the patients’ needs with their right to autonomy, the desires of the patients’ loved ones or operators and the sometimes-conflicting organizational guidelines, laws and regulations. Evetts 32 observed that an increase in standardization of work processes can lead to compromised professional discretion. This needs to be weighed against the fact that standardization, to a certain extent, increases an adherence to care protocols and assessment structures, 33 which also eases the cognitive load on clinicians and reduces the risk of biased decisions. The problem with the guidelines could also be viewed from the concept of work-as-imagined as to work-as-done from resilience engineering. 34 The guidelines portray the optimal world without confounding factors, the imagined work. Clinicians need to translate these guidelines into the real-world context and transform it into work-as-done. Difficulties might also stem from that EMS work is constantly changing in provision of care and not clearly defined in terms of responsibilities, mandates which makes updating guidelines a hard task. This also means that EMS clinicians need to be prepared for the unprepared.34,35
RFA can also be viewed in the context of collaboration between clinicians and other actors at the scene. They all operate on different RFAs, having to relate to different boundaries stated by their own organizations, professional regulations, and applicable laws. Previous research on collaboration in the EMS in general, has often focused on time-sensitive emergencies, 36 or work with hospitals 37 but has paid less attention to low-priority missions. This study indicates that clinicians and ORs believe that EMS positioning in relation to possible collaborators needs strengthening to enable clinicians to act based on their CR. However, instead of strengthening EMS position, an increased understanding among collaborators may be needed. Hjörne, Juhila and van Nijnatten 38 expressed the need for clear communication between collaborators, internal as well as external. This allows for an organizational climate in which discussions and critiques can take place. An open climate can contribute to developing a sustainable work environment and collaborations, which, in turn, can improve organizational influences for CR and is considered as a psychological safety aspect in the work environment. 39 Familiarity within the group is important for feeling psychologically safe in emergency department, and that team huddles at the beginning of shifts could have a positive influence. 40 These huddles are like the video-meetings conducted in this case, where shift-teams know who is working in which ambulance and they can get an update on status of equipment and facilities.
Workplace cultures are difficult to gain full insight into, but this study managed to capture a few. One is difficulty in implementing new work structures among clinicians. Difficulties in implementation may be referred to various subgroups among the personnel in the specific organization. 41 Acceptance for change can be influenced by the origin of the decision being either ‘top down’ or ‘ground up’.41–43 This apparently becomes more of an issue if the change challenges the professionalism norms in relation to work and caring ethics, and values shared within the group. 23 Problems with the implementation can also be linked to difficulties in sharing information within the organization and the heavy workload described in this case. Factors such as uncertain environments,3,4 workload, 44 problematic guidelines3,44 and ethical dilemmas 45 as to whose wishes the clinicians should comply with have previously been reported.3,4 Furthermore, financial structures and political agendas are influential in the administration of EMS care, 46 and informs CR.
Conforming to policies that one does not agree with, or that might put the clinicians at risk of litigation or repercussions can be perceived as an uncertainty in the workplace. 4 The financial factors might put an additional drive on the development of new work processes, but there is a risk that these are rushed to implementation and not properly evaluated in terms of patient or clinician safety. Finally, we draw the conclusion that this case does not stand out from an overall EMS context3,4 or presented in public debate, 46 which adds to the possible generalization of the findings.
There are limitations to this study. First, the relatively large amount of research data, which is common in the case study methodology. It needs to be well-structured and managed. 47 This is believed to be accounted for using the computerized analysis software program which allowed for structuring and easy tracing of the data. The time variance between data collections could influence the results as the EMS organization develops continuously. The naturalistic setting limited the possibility to control variables, however, it instead adds to the realistic and descriptive perspectives of the setting.24,47,48 All authors have experience from the EMS context and related research, which could influence the interpretation of the data. The demographics of participants could have influenced the findings as they all were ALS experienced clinicians with long periods in service. It would be beneficial to investigate BLS clinicians and those with a shorter work experience to understand if their experience of organizational factors differs from the findings in this study. Finally, due to the qualitative nature of this research it is not automatically transferable to other organizations or EMS contexts.
Implications
Based on the current study, the following implications are suggested:
- ORs need to strengthen or illuminate the EMS position as a care provider against the hospital organization and collaborative partners. - Clinicians and ORs need to jointly investigate, develop and implement proper methods for sharing information and updating routine documents. - Hospital organizations (or others responsible) must ensure sufficient room for clinicians and ORs in EMS to manage aspects other than purely operational demands, allowing for collective development.
Conclusion
Organizational influences for EMS clinicians’ CR are difficult to fully grasp. But to enable clinicians to feel secure and confident in which mandates they have in relation to other collaborators seems important. There is also a need for additional support in how to balance various requirements, rules and regulation with the wishes and expectations from patients as well as professional and ethical values. Adhering to the rules and regulations of the organization can keep clinicians from experiencing negative consequences resulting from committing a violation. However, the risk exists for the violation of professional and ethical values, or of losing the trust of the patient. Collaboration in EMS needs to be regulated for contexts beyond emergencies, increasing understanding of each other's RFA can be a way forward. Possibilities for sharing and implementation of information need to be improved. A secure line of information sharing could reduce uncertainty and increase confidence in clinicians’ CR. Additional research could focus on RFA for clinicians and ORs, but also addressing ORs’ possibilities for addressing influential factors for CR.
Supplemental Material
sj-docx-1-pam-10.1177_27536386231189011 - Supplemental material for Organizational factors influencing clinical reasoning in a Swedish emergency medical service organization: An explorative qualitative case study
Supplemental material, sj-docx-1-pam-10.1177_27536386231189011 for Organizational factors influencing clinical reasoning in a Swedish emergency medical service organization: An explorative qualitative case study by Ulf Andersson, Hanna Maurin Söderholm, Henrik Andersson, Birgitta Wireklint Sundström, Magnus Andersson Hagiwara and Goran Puaca in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386231189011 - Supplemental material for Organizational factors influencing clinical reasoning in a Swedish emergency medical service organization: An explorative qualitative case study
Supplemental material, sj-docx-2-pam-10.1177_27536386231189011 for Organizational factors influencing clinical reasoning in a Swedish emergency medical service organization: An explorative qualitative case study by Ulf Andersson, Hanna Maurin Söderholm, Henrik Andersson, Birgitta Wireklint Sundström, Magnus Andersson Hagiwara and Goran Puaca in Paramedicine
Footnotes
Acknowledgments
The authors would like to thank the participants of this study. It was a privilege to take part in their experiences and hear their thoughts on the research topic.
Author contributions
UA was the main author and conducted the majority of data collection, analysis and writing of the manuscript. BWS and HA contributed in the data collection process, analysis and provided feedback on manuscript drafts. MAH and HMS took part in the analysis process and provided feedback on manuscript drafts. GP took part in data collection, analysis and discussion of the results.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.