
Abstract
Introduction
In 1994, the first Australasian paramedicine tertiary program commenced as an off-campus offering not required as an entry-to-practice qualification A quarter of a century later, university programs have proliferated with tertiary qualifications becoming mandatory to acquire Australian Health Practitioner Regulation Agency registration. Despite this progression, concerns have been voiced regarding student enrolment volume and sustainability of the paramedicine academic workforce. To date, a census of the sector and the workforce has not been conducted, limiting capacity for data-informed strategic planning. The aim of this study was to profile the Australasian paramedicine tertiary sector and describe the academic workforce working in it.
Methods
A cross-sectional study was conducted in May 2022 using an online survey designed specifically for this research. The participants were discipline leaders from 19 universities or polytechnics offering entry-to-practice courses in Australia and New Zealand. Participants were asked to provide data on their course structure, organisational position, student enrolment loads and academic and non-academic staffing profiles. Simple descriptive statistics were generated to describe these data.
Results
Of the 19 eligible programs, 18 participated (response rate 90%). All but one course was at the undergraduate level; of the undergraduate courses, all but one were 3 years in duration. The academic workforce comprised 161 full-time or fractional and 727 casual paramedicine academics. Of the full-time academics, 131/161 were registered, with 45% of those holding ‘non-practicing’ status. Twenty-nine paramedicine academics (18%) had PhDs. There was 1 Professor and 10 Associate Professors, whilst 65% overall were Lecturers or Associate Lecturers.
Conclusion
This analysis represents the first description of the Australasian paramedicine tertiary sector. It reveals a diverse sector with large student enrolments and diverse course structures. The seniority of the academic workforce is skewed substantially towards lower academic levels; this shortfall in senior academics creates risk for the sector and may be symptomatic of a workforce sustainability issue.
Introduction
As with paramedicine models of care, there is considerable heterogeneity in models of paramedicine education throughout the international community, due to local regulation and accreditation by bodies. Countries, such as New Zealand, South Africa, the United Kingdom (UK) and Australia, and regions such as Scandinavia, have embedded tertiary-based education as an entry-to-practice requirement, whereas regions such as North America and Central Europe continue with predominantly community college, sub-degree or internal industry education.1–7 Other countries are contemplating transition, for example, Canada, which is currently engaged in ongoing consideration regarding the transition to degree-based entry-to-practice education as a vision to be achieved by 2025. This progression is also further recognition of the meaningful contribution paramedics make within contemporary healthcare systems and the increasingly complex and autonomous nature of their practice.8,9
In Australia and New Zealand, referred to hereafter in this paper as Australasia, tertiary-level entry-to-practice education has been established for more than a quarter of a century. 10 The first Australasian tertiary programs emerged in 1994 as non-mandatory courses, taught largely as off-campus distance education hybrid offerings delivered in partnership with jurisdictional ambulance services, and staffed predominantly by ambulance industry educators in the absence of a paramedicine academic workforce. 11 Over the ensuing decade, the majority of Australasian ambulance jurisdictions moved to a paramedicine Bachelor degree qualification as an employment and practice requirement. Concurrently, the paramedicine tertiary sector experienced substantial expansion, with the number of universities offering entry-to-practice degree courses growing rapidly between 2005 and 2015. 11 In 2010, the need for oversight and regulation of the expanding tertiary sector was recognised, resulting in the emergence of the Paramedic Education Program Accreditation Scheme. 11 In 2018, national registration was implemented in Australia under the Australian Health Practitioner Regulation Agency, governed by the Paramedicine Board of Australia, and to which paramedicine tertiary education accreditation responsibilities were transferred under the Paramedicine Accreditation Committee. 12 In New Zealand, following the establishment of the Te Kaunihera Manapou Paramedic Council in 2020, the same transfer of responsibility occurred for programs in that country.
The expansion of tertiary paramedicine education has however created complex issues that continue to challenge the Australasian, and most likely, the international sector. Prominent amongst those are educational infrastructure and resourcing, program funding, work-integrated learning capacity, research capacity and sustainability of the paramedicine academic workforce. 13
A sustainable paramedicine academic workforce sits at the core of a successful tertiary paramedicine sector. The larger the paramedicine tertiary sector, the more paramedicine academics will be needed to service it, and hence a need for more clinicians to consider the transition to academia. However, despite the long history of the Australasian paramedicine tertiary sector, significant concern exists regarding the stability and sustainability of the academic workforce within it. These concerns were first expressed by O’Meara in 2006, 14 well before the acceleration in the emergence of new programs, then again in 2018 by O’Meara and Maguire. 15
However, despite these cautionary commentaries, the Australasian paramedicine industry appears to have not been proactive in terms of gaining a greater understanding of the profile of the paramedicine tertiary sector nor the academic workforce within it. This is fundamental to informing debate and developing a forward-thinking strategy designed to create a sustainable paramedicine academic workforce. What is known is entirely Australasian in context and focuses on the transition of paramedics from clinical roles to academia. 16 In 2013, Munro et al. conducted a suite of research retrospectively exploring that transition using an online survey and focus groups to engage paramedicine academics in Australia and New Zealand.17,18 From participants in that research the authors estimated a workforce of 66 paramedicine academics, a number that has most likely grown enormously over the ensuing decade. In a 2014 cross-sectional study consisting of 33 respondents by Munro et al., participants described many challenges experienced during their transition, including lack of preparedness for transition, lack of a transferrable professional skillset, lack of research capacity and funding and academic workload issues. 17 A key finding from the qualitative component of the research was an identity crisis, with participants feeling to be in what the authors described as a ‘professional no-man's land’; stuck between being a paramedic and an academic, and not feeling a sense of true belonging to either. 18 Clearly, these issues impact not only attraction of paramedicine academics but retention in academia in the early- and mid-academic career.
Against this background, there is a demonstrable need to gain a greater understanding of paramedicine academia in order to identify existing, emerging and future challenges and inform the development of strategy aimed at securing a successful and sustainable sector.
The aim of this research was to conduct a cross-sectional study to create a profile of the Australasian paramedicine academic sector and the workforce within it.
Methods
Study design and theoretical paradigm
This study utilised a cross-sectional design to conduct a national survey of Australian and New Zealand paramedicine entry-to-practice programs. The epistemological stance adopted was one of objectivism, and a positivist theoretical lens was applied: these acknowledge there is a single observable truth that can be quantified using scientific methods. The study was reported in adherence to the STROBE reporting standard extension for cross-sectional studies. 19
Setting
The setting was the Australasian paramedicine university sector; for the purposes of this study, Australasian referred to Australia and New Zealand. Australasia boasts university-level entry-to-practice education as the minimum educational requirement for paramedic practitioner registration under the Paramedicine Board of Australia or in New Zealand, the Te Kaunihera Manapou Paramedic Council, with the exception of NSW in which a Diploma may be recognised in one jurisdiction. At the time of data collection, 19 institutions provided entry-to-practice tertiary programs.
Participants and eligibility
The participants were the academic leads of the entry-to-practice paramedicine programs in Australia and New Zealand, participating on behalf of their respective university. Programs were eligible if they were a member of the Australasian Council of Paramedicine Deans. The Australasian Council of Paramedicine Deans is the peak national body representing the interests of the Australasian paramedicine university sector and has 100% membership across institutions providing entry-to-practice paramedicine education.
Recruitment and consent
Recruitment was conducted through the Australasian Council of Paramedicine Deans (referred to hereafter as ‘the Council’). Following ethical approval being granted, the research team sought the support of the Council in disseminating the participation invitation to its membership. As all program leaders of the targeted programs are members of the Council, this was deemed the most appropriate approach for effective recruitment rather than contacting individual program leaders separately. The recruitment invitation and participant information sheet were emailed to Council membership by the Council's executive.
The participant information sheet contained information pertinent to the study, upon which the individual program leaders could base their decision to participate or not. Participation was anonymous, thus protecting the identity of each university. The information sheet contained a link to the anonymous survey; accessing and completing the survey was deemed implied consent. To ensure the robustness of the consent process, the first question of the survey asked participants to confirm they had read the information sheet and their consent to participate.
Instrumentation
An informal electronic search of MEDLINE, Education Resources Information Centre and Google Scholar was conducted to identify existing validated survey instruments that might be suitable to meet the needs of the present study. No such instruments were identified, resulting in a new instrument being developed. The research team first met to discuss the data variables required to answer the research questions. A survey was then constructed, consisting of 21 questions. To ensure face and content validity the survey was piloted amongst 10 paramedicine academics, whose feedback was incorporated into the refinement of the instrument. To promote consistency across participants during data collection, definitions and guidance statements were provided with each question. The full instrument is available in Appendix 1.
Data variables
The instrument focused on collecting the following key data variables:
- Situation of the program within the organisational administrative structure - Number and Australian Qualification Framework (AQF) education level of courses offered within a program https://www.teqsa.gov.au/how-we-regulate/acts-and-standards/australian-qualifications-framework - Paramedicine full-time and fractional academic staffing numbers (headcount). These data include only academics with a paramedic qualification, who are working in balanced teaching/research roles in a program providing appointments, honorary positions and those in pure-research roles not engaged in teaching. -Paramedicine casual academic numbers (headcount). These data include only academics with a paramedic qualification teaching into a program providing entry-to-practice education (undergraduate or post-graduate) and exclude adjunct or honorary positions - Academic level of paramedicine academics (Associate Lecturer (‘Level A’), Lecturer (‘Level B’), Senior Lecturer (‘Level C’), Associate Professor (‘Level D’) and Professor (‘Level E’). - Paramedicine academic educational qualifications (AQF framework qualifications) - Paramedicine academic registration status (registered or not registered) - Paramedicine academic patient-facing clinical practice engagement status (engaged in patient-facing clinical practice or not)
The program lead (the ‘participant’) reported these data via the instrument on a program level on behalf of their institution; that is, it was not completed by each individual staff member within an eligible program.
Data collection
Data were collected electronically using the Qualtrics online survey platform (Qualtrics, Provo, UT). The survey was available for four weeks from May 1–31, 2022. Weekly reminders were provided via email to the eligible participant group by the Australasian Council of Paramedicine Deans on behalf of the research team.
Data analysis
Data were downloaded from Qualtrics into Excel, via which all data analyses were conducted. Data were subjected to descriptive analysis, in line with the stated aim of the study. Continuous variables were examined for normality of distribution and reported as mean with standard deviation or median with interquartile range for normal and non-normally distributed data, respectively. Categorical data were presented as proportions, with 95% confidence intervals where appropriate.
Ethics approvals
Approval from the Western Sydney University Human Research Ethics Committee was sought and secured in March 2022 (Approval number H14677).
Results
Of the 19 eligible institutions at the time of data collection, 18 responses were received constituting a response rate of 95%.
Paramedicine tertiary sector structure, scope and leadership
At the time of data collection, the Australasian paramedicine sector consisted of 19 institutions (18 universities and 1 polytechnic college), of which 18 participated and provided data. All but one provides undergraduate entry-to-practice education, the other offering only a post-graduate course. All institutions offered a pure paramedicine qualification, with two also offering a dual paramedicine/nursing qualification. Eight offered post-graduate qualifications in specialist areas beyond the entry-to-practice level. Twelve offered generic Doctor of Philosophy (PhD) degrees, two reported paramedicine-specific PhD courses and four offered no PhD courses.
All but two institutions providing pure paramedicine qualifications at the undergraduate level offered 3-year Bachelor's degrees. One offered a 4-year pure paramedicine degree, whilst two offered a 1-year post-graduate diploma. One provided an ‘accelerated’ course, compressing a 3-year course into two. Combined, these 18 participating institutions collectively accommodate a population of 8500 paramedicine students.
The paramedicine courses were organisationally situated in a diverse range of schools or faculties (noting the variation in nomenclature and structure across institutions, not all of which have faculties). Four were co-located with nursing, four within medicine, and the remainder within health or allied health.
Regarding paramedic academic leadership, 78% (14/18) had a dedicated paramedicine discipline lead or equivalent overseeing the course, and slightly more than half of course leaders (55%) were reported to be registered paramedics. Fifty percent of courses (9/18) reported having paramedicine academic as part of the higher-level school or faculty executive.
Paramedicine academic workforce
The total number (headcount) of paramedicine academics in full-time or fractional roles across the sector was reported as 161 persons. These were supported by a casual academic workforce numbering 727, adjunct or honorary staff numbering 42 and 136 non-paramedicine academics.
Of the 161 full-time or fractional paramedicine academics, 131 (81%) were in undergraduate blended roles (teaching and research components), 16% in post-graduate blended roles and 4 (2%) in research-only positions within an undergraduate program. No teaching-only academic roles were reported.
The highest completed academic qualification of full-time or fractional paramedicine academics is described in Figure 1. Twenty-nine (17%) possessed a PhD, whilst 35% held a Bachelor degree or lower.
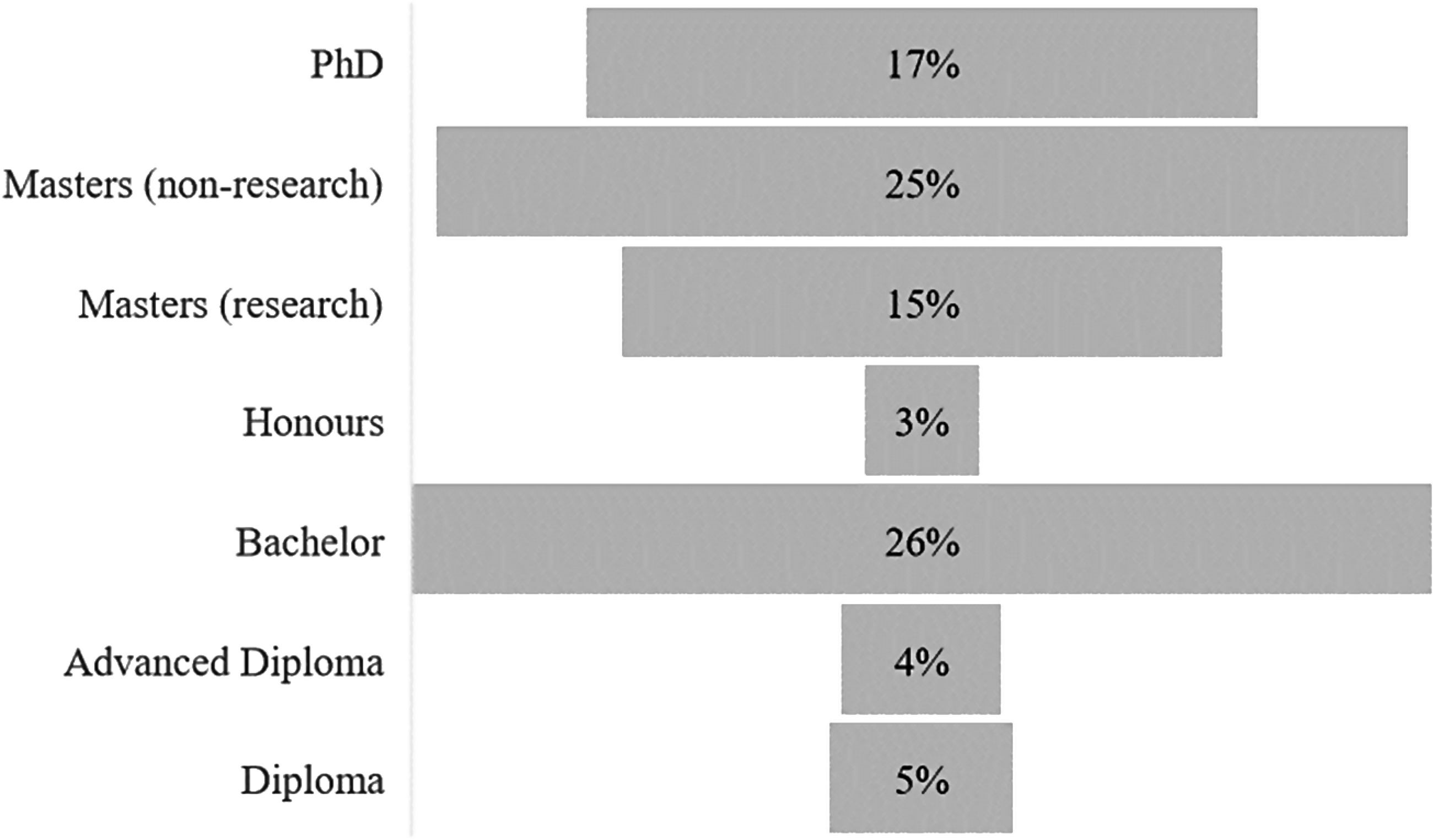
Distribution of paramedicine academics by highest educational qualification (n = 161).
The distribution by academic level for full-time or fractional paramedicine academics is described in Figure 2. The professoriate numbered 11 (7%), with one full Professor (Level E) and 10 Associate Professors (Level D). Lecturers and Associate Lecturers (Level B and A, respectively) accounted for two-thirds of the academic workforce (66%).
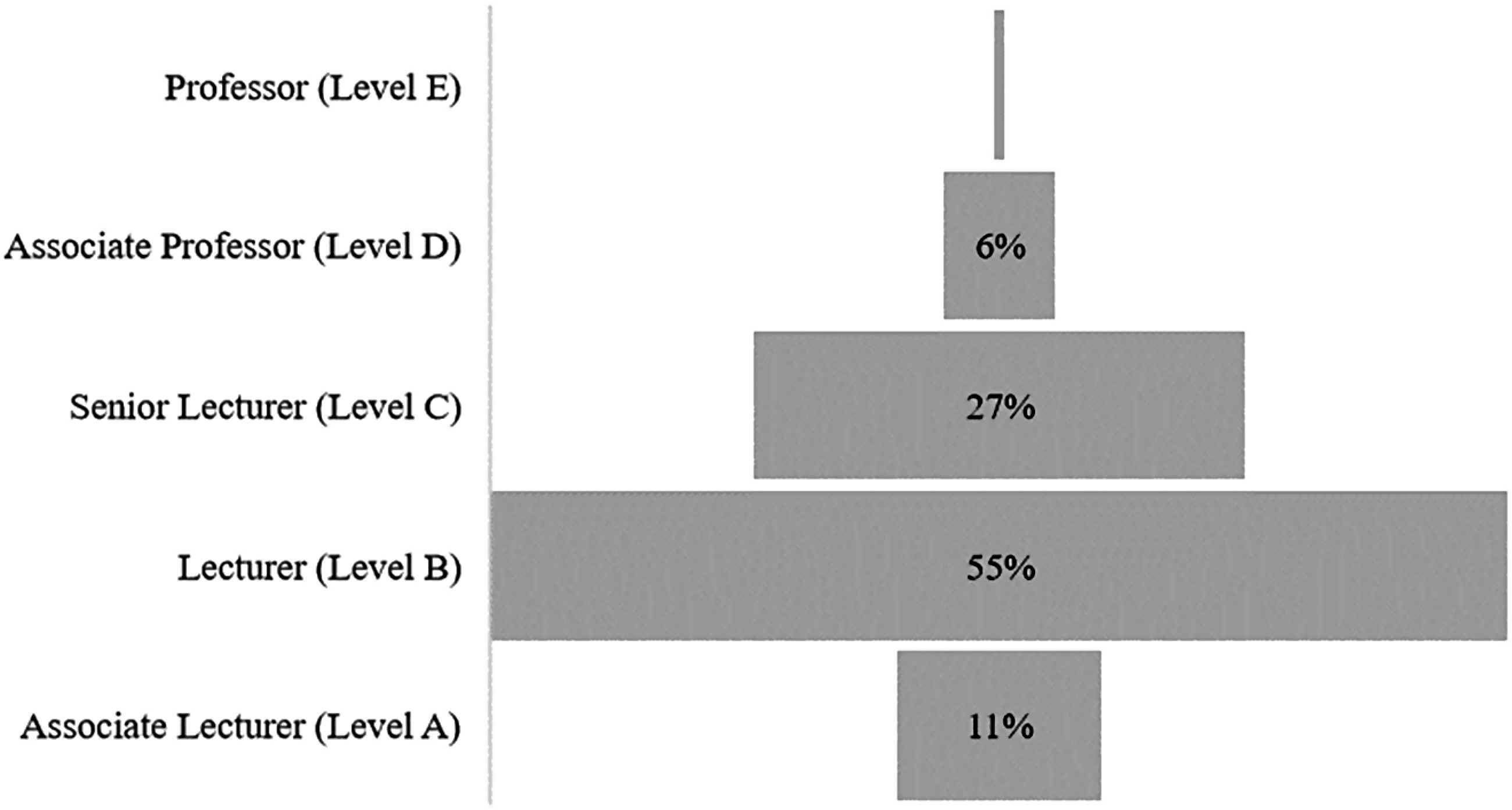
Distribution of paramedic academics by academic level (n = 161).
Ninety percent of full-time or fractional paramedicine academics held registration with the relevant national regulatory board. Of those who were registered, 45% held ‘non-practicing’ registration. Forty-five percent of programs required staff wishing to engage in patient-facing practice to do so in their own time, external to their university role. Overall, 47% of paramedicine academics had engaged in patient-facing clinical practice in the preceding 12 months.
Discussion
This cross-sectional study sought to provide a program-level description of the Australasian paramedicine tertiary academic sector and the academic workforce within it. It represents the first census-level description of a paramedicine academic workforce and provides insights into opportunities and barriers present in a sector approaching thirty years in existence. The data illustrate an expansive sector that at the time of data collection spanned 19 institutions staffed by 161 full-time or fractional paramedicine academics, suggesting the workforce has more than doubled based on a previous estimate of 66 arising from a 2013 survey. 17
The study identified that three-quarters of programs sat within health-focussed schools or faculties, emerging from the predominantly nursing-based organisational units in which the early programs were situated. Only two were reported to be located in a nursing-centric organisational location. This shift represents significant growth in the identity and prominence of paramedicine programs within the broader health, medicine, allied healthcare and nursing tertiary sectors. It is unclear where the optimal positioning of a paramedicine program should be within a university faculty structure, but clear establishment as a discipline of its own rather than a subset of another is an important step in the recognition of paramedicine as a legitimate university-based healthcare profession. There is evidence of movement towards this ideal, with at least two institutions flagging imminent restructures that would include specific Schools of Paramedicine. 20
Leadership of paramedicine university programs appears to be an area for growth, with just over half (55%) of programs reporting a registered paramedic as the discipline lead. This may indicate a lack of senior paramedicine academics or academic leadership capacity or might reflect an organisation's cultural view of paramedicine as not being sufficiently mature to lead itself. This situation would most likely be anomalous with other health disciplines, in which an academic leader from outside a given discipline would be extremely rare. Currently, there appear to be few levers that if pulled would stimulate growth in the number of programs with paramedic leaders. One driver of change could be program accreditation standards, which currently do not stipulate having a paramedic in the key leadership role. 12 By comparison, the Australian Nursing and Midwifery Council accreditation standards for approved programs stipulate programs must have ‘a governance structure that ensures the head of discipline is a registered nurse with the NMBA, with no conditions or undertakings on their registration relating to performance or conduct and holds a relevant post-graduate qualification’. 21 This does present a ‘double-edged sword’ though; in a younger discipline with less leadership capacity, mandating a paramedic as program leader could result in the inappropriate appointment of more junior paramedicine academics to senior roles they are not mature enough to fulfill. Conversely not doing so takes the onus away from universities and the profession to ensure opportunities for career progression through leadership roles, or to strategically grow paramedicine academic leadership capacity.
Leadership capacity within paramedicine academia has not been previously described in published literature, but the academic level distribution data presented herein constitutes a useful surrogate measure. Academic leadership sits within the professoriate, that being Professors and Associate Professors (Level E and D); this study identified a small professoriate consisting of one Professor and 10 Associate Professors spanning the 18 universities that participated in the study. Whilst this current study did not collect data on the number of Professors or Associate Professors in formal program leader roles, data from the Australasian Council of Paramedicine Deans indicates that only 6 of the current 20 programs have Level D or E academics in those roles (two of whom are from non-paramedicine disciplines). 22
Further, two-thirds of the workforce were at the junior academic levels of Lecturer and Associate Lecturer (Level B and A, respectively). The small professoriate may be indicative of paramedicine academics encountering barriers preventing progression to senior levels, or of a sector unable to retain its post-doctoral staff. These present data identified 27 post-doctoral full-time or fractional staff, a number that by international standards are exceptional in the paramedicine context. However, it was estimated that internationallly there were 30 PhD-qualified paramedics in 2016, and a further 60 undergoing Higher Degree by Research (HDR) training. 15 Those data were for PhD paramedics regardless of if they were in academia, whereas the present data are limited to those currently full-time or fractional in universities providing entry-to-practice education, suggesting little net growth in post-doctoral paramedics and indicating a retention issue for senior academics.
Similarly, the large junior academic group could be the result of the inability of newer staff to progress their academic career through being research active and successful in application for promotion. It could also constitute retention issues, characterised by junior academic staff leaving academia before being able to, or because they cannot, progress, resulting in a ‘revolving-door’ of new academic staff unable to gain a foothold in their academic career. Multiple barriers to paramedicine academic career progression and sustainability have been proposed including lack of research capacity and funding; high teaching and marking workload allocations; the requirement to pursue a PhD; inability to move past the transitional phase from clinician to academic; difficulty in managing complex workplace issues such a contra-power; and junior academic salaries being below what can be earned in a clinical role.15,18,23,24 The transition is further complicated by transitional identify issues, conflict in trying to maintain clinical recency, mismatched expectations of what academia actually is and a lack of well-developed professional skillset on entry to academia.11,18,23,25
The requirement to pursue a PhD represents a daunting hurdle for new paramedic academics but is a phenomenon not unique to paramedicine. 26 New academics have reported not realising the realities of an academic role, many suggesting they expected the role to be more an educator than a true academic. 23 Achieving this requirement is made all the more difficult amongst new paramedicine academics. The present study identified 35% of paramedicine academics with the highest completed qualification of Bachelor's and 25% with a completed non-research Master's degree. These data are consistent with that Munro's 2013 data that found 36% of paramedicine academics had entered with a Bachelor's or less, though the small sample size (n = 30) limits the usefulness of that finding. Value could be found in the development of transition to academia initiatives or pathways that enable the development of a professional skillset and completion of an HDR qualification before entering academia. Central to such a strategy is greater engagement with and stewardship of the large casual academic workforce, identified in this research as numbering 727. 27 Opportunities exist amongst such a large group already engaged in academia to promote and support the transition to a full-time role, one of which may be having this group more strongly identify as a ‘casual academic’ rather than a ‘tutor’ or ‘clinical facilitator’ and making sure such roles entrain broader academic responsibly rather than simply transient and intermittent delivery of practical classes or tutorial sessions.16,18 Another strategy may be a stronger embracement of the ‘clinical-academic’ role commonly seen in other disciplines, particularly medicine. The inability to continue with clinical work has been identified as a key issue in the attraction of an academic role and retention once engaged.15,18,28 However, despite the need for these and the benefits they would bring, clinical-academic roles or similar shared models are most likely not the panacea to the academic workforce issue. Whilst they could promote the transition to the sector, it could be argued that clinical academics are less likely to completely immerse in the full scope of academic responsibility and engagement; the fraction of such roles devoted to academic pursuits would tend in most instances to be unidimensional, focussing on teaching or research. It is possible that over-reliance on clinical-academic roles might be at the expense of career paramedicine academics keen to engage in the scholarship of academia and broader academic citizenship, thus serving as a barrier to the development of academic and professional leadership within the paramedicine tertiary sector.
Our data identified that of those academics who maintained registration, 45% held ‘non-practicing’ status, and only 47% had engaged in patient care in the past 12 months. Demonstrative of the challenges associated with maintaining a clinical identity in academia, just under half of universities made staff wishing to engage in clinical practice do so in their own time on top of normal academic workloads. Possible also is that some paramedicine academics may misunderstand the regulatory definition of practice, which states ‘…practice is not restricted to the provision of direct clinical care. It also includes using professional knowledge in a direct non-clinical relationship with clients, working in management, administration, education, research, advisory, regulatory or policy development roles and any other roles that impact on safe, effective delivery of services in the profession.’ 29 p.01
The results presented herein, whilst simply descriptive in nature, provide the first overview of a paramedicine academic sector and the workforce within it. The significance of this research lies not only in its ability to inform existing well-developed sectors such as Australia, the UK and New Zealand as to their current situation but also in that it informs regions contemplating transition to tertiary education, or where that transition is underway, as to the importance of ensuring that ongoing sustainability and viability is considered strategically at the outset in longitudinal planning.
Limitations
There are several limitations that should be considered when examining these data. First, the data were collected on a program-level and gathered by the program lead (the participant) on behalf of their institution and team. Therefore, the data may have some inaccuracy inherent to that approach. However, the collected data were high level and it would be expected that the program lead completing the survey did so with appropriate diligence. Second, the study reported on 18 of what are now 20 programs in the sector. One program did not participate, and one additional program has been established since the time of data collection; the data herein, therefore, represent the minimum for the tertiary sector given those missing data. However, the high participation rate does confirm the data set to be largely complete whilst acknowledging the non-inclusion of recent developments since the data collection period. Finally, the instrument used to collect data was not one previously validated, resulting in the creation of one specifically for the study. The instrument was not subjected to rigorous validation analysis; however, piloting in a population similar to the intended participants was undertaken to optimise face and content validity.
Conclusion
The Australasian paramedicine academic sector is large, now spanning 20 institutions. The paramedicine academic workforce within it consists of 161 full time or fractional staff and 747 casual academics, an increase in full-time staff of more than 50% in the past decade.
The paramedicine academic workforce appears to lack post-doctoral senior academic leadership and has a demonstrably junior academic base. The data suggest issues in attracting academics to academia and retaining them in the longer term. The sector may be well served by collaborating with industry to promote the development of transitional pathways to and with academia and academic leadership.
Supplemental Material
sj-pdf-1-pam-10.1177_27536386231185602 - Supplemental material for Profiling the Australasian paramedicine tertiary academic sector and workforce: A cross-sectional study
Supplemental material, sj-pdf-1-pam-10.1177_27536386231185602 for Profiling the Australasian paramedicine tertiary academic sector and workforce: A cross-sectional study by Paul Simpson, Nigel Barr, David Reid, Malcolm Boyle and Brett Williams in Paramedicine
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Paul Simpson is the Editor-in-Chief of Paramedicine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Correction (September 2023):
This article has been updated to disclose the Declaration of conflicting interests statement.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.