
Abstract
Introduction
British Columbia Emergency Health Service trialled the use of intranasal (IN) ketamine given by Primary Care Paramedics (PCPs). Prior to this practice change, the PCPs had not performed weight-based drug calculations, given medications intranasally, nor been responsible for controlled and targeted substances. This study aimed to use the Capability, Opportunity, Motivation and Behaviour (COM-B) model and Theoretical Domain Framework (TDF) to identify enablers and barriers to implementing IN paramedic administered ketamine analgesia (iPAKA) for PCPs.
Methods
This was a parallel convergent mixed methods study with two phases. The quantitative phase consisted of longitudinal staff surveys to assess PCP knowledge and perceptions of ketamine and controlled and targeted substances policies. The qualitative phase involved staff focus groups on programme implementation. Descriptive statistics of survey results were integrated with coded focus group data and analysed using the COM-B model and TDF. Evidence-based behavioural change techniques were mapped to each TDF domain.
Findings
Our analysis revealed barriers and enablers across several TDF domains. Implementing ketamine was enabled by quality education, strong organisational support and the availability of cognitive aides. Trial success was attributed in part to participant's feelings of optimism and their increased job satisfaction. Key barriers included a knowledge gap involving drug dosage calculations, negative emotions associated with performance anxiety and a lack of field education and supervision to monitor paramedic practice.
Conclusion
The use of theoretical frameworks and models like COM-B/TDF serves to improve the sustainable implementation of behaviour and clinical practice change in paramedicine. When project teams use theory to guide design and implementation, they can systematically identify and target individual and organisational enablers and barriers to adopting routine practices. The iPAKA study reveals key barriers and facilitators in several TDF domains and presents theory-linked targeted behavioural techniques to support on-going implementation of PCP-administered IN ketamine for analgesia.
Introduction
Paramedic practice across Canada continues to evolve with regards to patient needs and health service demands. Such evolution can be observed in the implementation of novel service designs such as community paramedicine, 1 the continued integration of paramedicine into healthcare systems through programmes including palliative care 2 and advances in clinical practice (e.g., prehospital thrombolysis 3 ). In response to an identified patient need, a recent innovation in British Columbia Emergency Health Services (BCEHS) saw ketamine introduced and administered by Advanced Care Paramedics (ACPs) for analgesia and cases of excited delirium. 4
Between 2017 and 2018 BCEHS received over 40 patient safety submissions from Primary Care Paramedics (PCPs) 5 related to nitrous oxide being inadequate to treat pain. This was further compounded by a lack of ACP support to provide appropriate analgesia in some regions. To address these concerns, BCEHS initiated a proof-of-concept trial for PCP-administered intranasal (IN) ketamine. This followed the 2019 Prehospital Analgesia with Intranasal Ketamine (PAIN-K) study that demonstrated PCP-administered IN ketamine was safe and more effective at reducing pain when compared to nitrous oxide. 6
Implementing PCP-administered ketamine at BCEHS involved significant behaviour and practice change. During the PAIN-K trial, a small number of PCPs could administer ketamine to trauma patients who were experiencing severe pain. PCPs accustomed to giving patient-controlled inhaled nitrous oxide now assumed responsibility for providing patients with a weight-based IN dose of a controlled substance. This new practice involved adhering to Federal legislation and BCEHS policies for controlled and targeted substances (CTS). Despite the success of the PAIN-K trial, the implementation of such a significant change to paramedic practice remains poorly understood.
Implementing change in healthcare, in particular to clinical practice, presents challenges 7 and is more likely to succeed when implementation strategies are informed by theory and evidence.8–10 Despite this, little is known about knowledge translation for many health professions outside of medicine and nursing. Implementation and behavioural theories are commonly used to evaluate change in healthcare organisations and provide a lens through which we can view influences on behaviours. 11 Using theory to guide design and implementation offers generalisable, structured, replicable frameworks to inform interventions and guide evaluation. 12 By following such approaches, we can systematically identify and target individual and organisational enablers and barriers to adopting new practices.13,14 In doing so, we can facilitate knowledge translation to close the gap between theory and practice. 15 Implementing best practice is essential to improve health outcomes 16 and theoretically informed approaches can reduce the burden on staff and improve the delivery of patient care. 9 We therefore elected to adopt an Implementation Science perspective to identify the enablers and barriers to implementing this clinical practice change in paramedicine.
Theoretical approaches
The ‘Capability, Opportunity, Motivation and Behaviour’ (COM-B) model is a theoretical model often employed in Implementation Science. 17 The three components of COM-B provide structural context for key factors that produce change and are used to help identify reasons why a change is or is not being implemented (Figure 1).
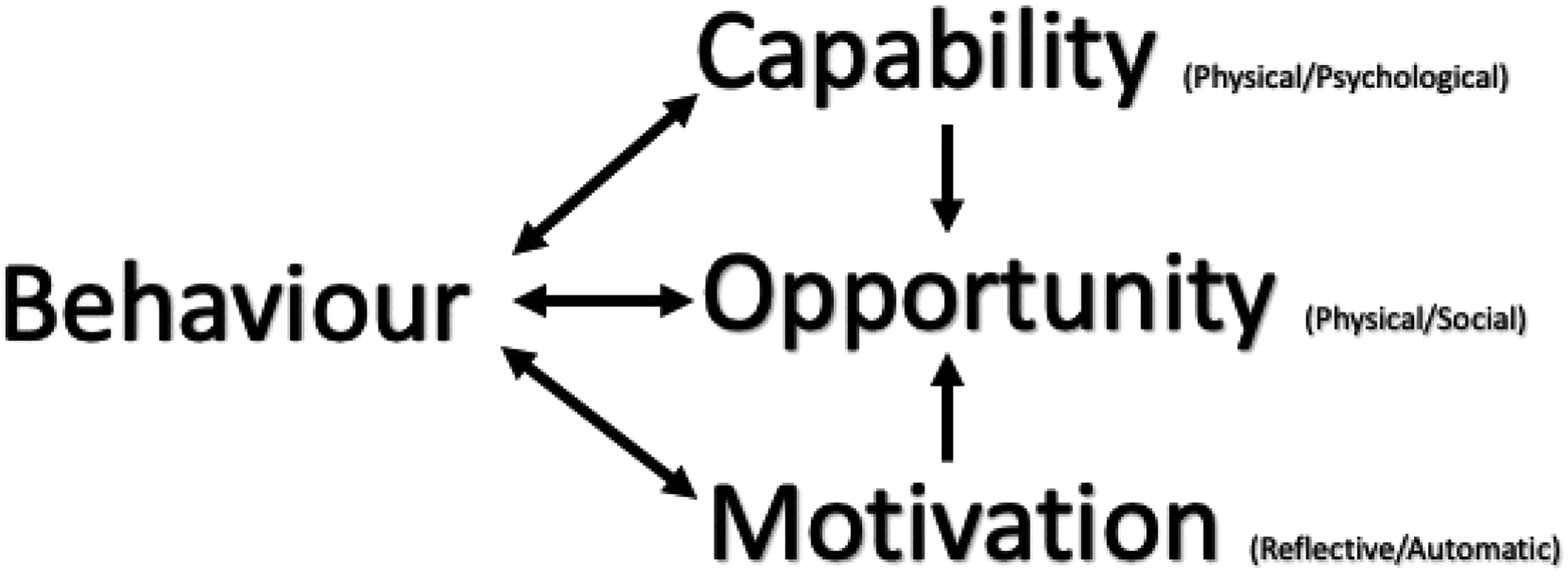
Capability, Opportunity, Motivation and Behaviour model and subcomponents adapted from Michie et al. 17
Building on the COM-B system, the Theoretical Domains Framework (TDF) is used extensively in health research to further understand barriers to change. 18 Researchers synthesised over 100 theories of implementation and behavioural change to develop the TDF which is comprised of 14 domains 18 (Appendix A Table 1).
When mapped and combined, the COM-B model can assist to determine which of the theoretical domains either enable or represent barriers to adopting the desired change (Table 1). Once barriers are identified, behavioural change techniques (BCTs) can then be used to influence individual behaviours that prevent change. BCTs are active components of interventions aimed at changing specific behaviours in the COM-B model. 19 A taxonomy of 93 theory-linked BCTs has been mapped to the TDF. 19
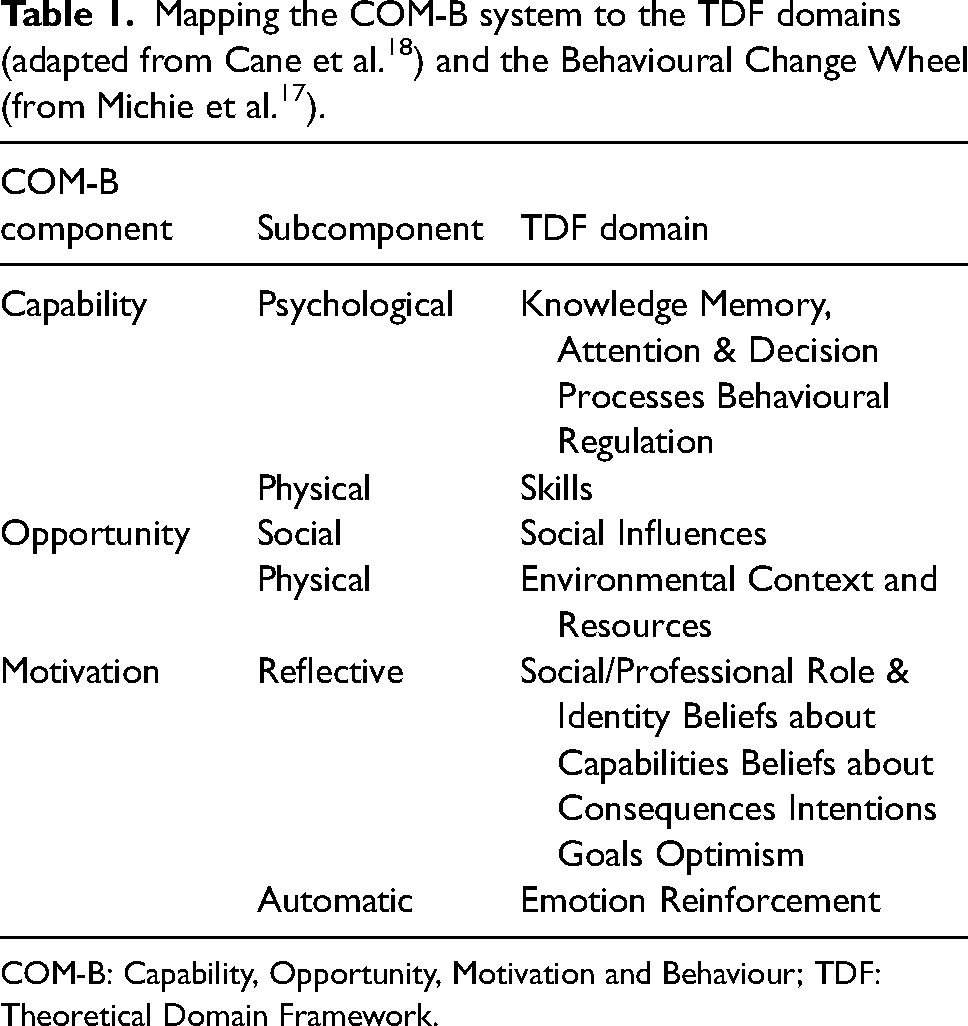
COM-B: Capability, Opportunity, Motivation and Behaviour; TDF: Theoretical Domain Framework.
Applying the combined COM-B/TDF to the factors associated with implementing PCP-administered ketamine at BCEHS may help us to better understand enablers and barriers, informing broader pan-Canadian implementation discussions.
Aim
This study aims to use the COM-B/TDF to identify enablers and barriers to implementing IN paramedic-administered ketamine analgesia (iPAKA) for PCPs.
Programme design and implementation
Building on the PAIN-K study, a team was assembled to represent input from across BCEHS. The iPAKA study involved preparing the project, developing and delivering education, ketamine supply and storage and readying PCPs to safely administer ketamine. It took approximately nine months from conception to start the project. The trial initially commenced in December 2020 in one ambulance station then extended to two others in 2021. In total, there were 64 PCPs assigned to these stations at the time of the pilot study. Key activities related to the iPAKA project implementation are described in Appendix B Table 2.
Methods
Positionality of research team
TJ, a Caucasian female and ACP, is a researcher, educator and research lead for iPAKA who is not employed by BCEHS. RB, a Caucasian female, is an emergency physician who assisted with project implementation while undertaking an Emergency Medicine fellowship at BCEHS. JA, a Caucasian male and Critical Care Paramedic (CCP), was the Director of Clinical and Professional Practice for BCEHS and project sponsor who conceived and designed the trial. AB, a Caucasian male and a CCP, is a researcher and educator who developed the education for the iPAKA study as a contractor for BCEHS. He has methodological expertise with focus groups and mixed methods (MM) studies.
Methodology
We approached our study from a pragmatic epistemological perspective. Pragmatism acknowledges that reality is created as individuals act in the world and it is thus ever changing, based on human experience and oriented towards solving practical problems. 20 Our choice of a MM approach was informed by our pragmatic perspective, in that one method would be inadequate to develop a complete understanding of a given issue 21 and we aimed to examine processes and experiences along with outcomes. 22 Informed by the model of disciplined inquiry, 23 we elected to adopt Implementation Science approaches, which aim to explore processes, in particular enablers and barriers to change. Our use of the COM-B and TDF models ensured that we remained aware of contextual sensitivities, individual behaviours and organisational resources.
Reflexivity
Being methodologically reflexive entailed the research team discussing the use of MM and whether quantitative results would inform the qualitative data collection. We were contextually reflexive when interpreting our study findings, relying on the research team's combined knowledge and understanding of the history of PCP education and practice in BCEHS. We explicitly reflected on our close relationships with the organisation and made every effort to account for these when interpreting results.
Study design
This parallel convergent MM study had two phases. The quantitative phase consisted of staff surveys to assess PCP knowledge and perceptions of ketamine and CTS policies. The qualitative phase involved staff focus groups on programme implementation. Contemporary literature on programme evaluation guided our choice in using an MM approach, acknowledging the complexity of implementing programmes in healthcare settings.24–26
Setting
BCEHS is the largest ambulance service in Canada and responds to over 750,000 ambulance calls each year. The service employs approximately 4200 paramedics across 183 ambulance stations. 23 Of these, there were 2950 PCPs, 252 ACPs, 63 CCPs and 607 Emergency Medical Responders (EMRs) in 2018. The remainder of the staff members were dispatchers and drivers with first-aid training.
The 911 resource response system in British Columbia is two tiered with ACPs available to support PCPs in larger cities including Victoria and Vancouver. The PCPs are primarily paired together or with an EMR and typically do not have access to ACP backup in smaller communities. Paramedics at both levels have 24 h access to clinical support for advice from a Paramedic Specialist or Emergency Physician. 5 Refer to Appendix C for a more detailed explanation of PCP and ACP education and licensed scope of practice.
As part of the implementation strategy, BCEHS chose to pilot the use of IN ketamine with a small group of PCPs before expanding its use across the province. Three smaller rural stations were identified for the study. These were selected due to their proximity to ski resorts and major highways where historically there was a relatively high incidence of trauma presentations. In addition, ACPs are not usually assigned to these ambulance stations.
Study phases
Phase 1: Quantitative data collection
Phase 1 of the study involved quantitative data collection using a longitudinal survey design. A series of three surveys were developed by the research team with input from staff in Clinical and Medical Programs. They were piloted by four ACPs and two PCPs and edited to incorporate suggested changes. The surveys were substantially similar in design with between 10 and 13 questions including the invitation to participate, consent form and demographic questions. The second section employed 5-point Likert scale questions for participants to rate their knowledge of ketamine, IN administration, the CTS legislation and regulations and assessing and documenting pain. Participants were asked a series of questions specific to administering ketamine and given a free-text option. The surveys are available in Appendix D.
Participants were a convenience sample of all 64 PCPs assigned to permanent positions at the three stations included in the study. The PCPs were invited via a participant information letter and web link for survey 1 sent to their work email addresses. Participants were informed that by completing the consent form and submitting their survey, they were consenting to be part of the study but could withdraw at any time. Their survey responses could not be withdrawn as no identifying data were collected. They were also advised that only PCPs enrolled in the trial could administer ketamine. PCPs not enrolled in the trial would continue to follow the standard clinical practice guidelines for pain management. Upon completing the electronic consent form, the PCPs were given access to the survey. After submitting survey 1 they could access and complete an online ketamine education package. The PCPs subsequently participated in a 4 h practical training session delivered by an ACP paramedic educator. The educator invited participants to complete survey 2 immediately after they had finished the education. The surveys were administered using SurveyMonkeyTM and could be completed in less than 10 min. All participants then received an invite to survey 3 at the end of the trial period. Participation was optional and one reminder to complete surveys 2 and 3 was sent two weeks after the initial invitations. The surveys remained open for the duration of the trial period. All responses in SurveyMonkeyTM had individual IP addresses recorded but it would not be possible to determine if participants had responded more than once from a work computer. Data were anonymised and stored on a secure, password-protected university server.
Quantitative data analysis
The Statistical Packages for the Social Sciences (SPSS) version 26.0 was used to analyse the quantitative survey data. Descriptive statistics were calculated using the frequencies dialogue. Medians and modes were calculated for the ordinal data.
Phase 2: Qualitative data collection
Qualitative data were collected using focus groups. Focus groups were selected as they can provide valuable insight into participant behaviours, experiences, feelings and attitudes. They can also assist participants to identify and explain their individual viewpoints to generate deeper insights. 27 Two facilitators (one male ACP and one female PCP) facilitated a series of focus groups at the end of the trial. Both facilitators work outside of the study area and are practising paramedics known to the participants. All participants were invited to the focus groups. The invitation was included in the final survey and again in an email sent to all participants in the trial. Participants were reminded of their consent to participate and their ability to withdraw at any time.
The research team developed a focus group question guide (Appendix E) to ensure consistency between the groups, and it was iteratively adjusted in response to feedback.
Participants were asked to provide insights on various aspects of the iPAKA trial. The semi-structured questions explored education and training, CTS procedures and ketamine administration. All focus groups were recorded, transcribed verbatim using software (www.otter.ai.com), checked by members of the research team for accuracy and stored on a secure online server. There were no personal identifiers in the recordings and the transcripts were not returned to the participants.
Qualitative data analysis
The anonymised transcripts were imported into NVivo (Version 12, QRS International, Australia) for data management, coding and analysis. Two authors (TJ and RB) familiarised themselves with the data by reading the transcripts and listening to the recordings to clarify comments. The two authors developed a coding guide based on the constructs of the TDF 28 informed by existing studies. 29 Where data could be assigned to more than one domain, the authors came to an agreement on a dominant domain. To ensure fidelity of the coding, the authors coded two transcripts together then completed the remaining coding independently. A third author (JA) assisted to resolve any differences in opinion. Quotes used in this manuscript have been edited only for brevity and conciseness (e.g., removing pauses in speaking).
Lastly, two authors (TJ and RB) reviewed the coded data to identify comments representing barriers and enablers across the COM-B model and TDF. These were presented to the entire research team to gain consensus. The Theory and Techniques Tool 30 was used to identify the BCTs associated with each of the TDF domains. The authors then used APEASE criteria (Affordability, Practicability, Effectiveness and cost effectiveness, Acceptability, Side-effects and safety, Equity) 17 to evaluate each BCT to determine if it was feasible to implement at BCEHS. Participant feedback was also used in this final step.
Ethical approvals
The BCEHS Clinical and Medical Programs Research Committee approved the project proposal, and ethics approval was provided by the Justice Institute of British Columbia Research Ethics Board (JIBCER2020-07-PAKA).
Integration of data
We used the conceptual depth criteria 31 to ensure we were integrating data to an appropriate level to inform our concepts – range (multiple instances of the concept were in the data sets), complexity (concepts were part of a rich network), subtlety (concepts could be differentiated or combined), resonance (concepts resonated with existing literature) and validity (concepts were credible). Focus group questions were written prior to survey results being available. Interviewers were, however, aware of the results from surveys 1 and 2 prior to facilitating the focus groups. During analysis, we followed threads from the survey data through to focus group data and back again, seeking multiple instances, convergence or divergence and emerging concepts informed by the TDF.
Rigour and trustworthiness
We aimed to ensure trustworthiness in our data and findings. For the quantitative data collection, the survey was reviewed by members of the research and implementation teams. Data were downloaded directly from the survey tool, reducing the chance of transcription errors. We reported the findings of this section in accordance with the CHERRIES reporting guideline. 32 For the qualitative data, we aimed to ensure credibility and confirmability by gathering multiple sources of data and integrating them during analysis and using MM to ensure a complete representation of the data. We also employed a theoretical approach to guide our data analysis and interpretation and achieved agreement among the team on themes and categories. We aimed to ensure transferability by exploring programme and system level enablers and barriers which may be similar in other contexts. Dependability was ensured through accurate documentation, a clear audit trail, checking transcripts and reflexively reviewing data throughout the study. We reported the qualitative methods in accordance with the SQUIRES reporting guideline. 33
Results and findings
Quantitative survey results
Demographics
A total of 64 (100%) PCPs completed survey 1; 47 (73.4%) completed survey 2; and 39 completed survey 3 (60.9%). Respondents were predominately from the larger Vernon station and 56% (n = 34) had a minimum of 11 years of PCP experience. Demographic results are available in Appendix F Table 3.
Knowledge and ability
Respondents reported increased knowledge levels after the online and face-to-face education (Table 2). This continued for those who completed survey 3 at the end of the trial. When asked to rate their knowledge of ketamine, intranasal drug administration, CTS and BCEHS policies and procedures for CTS, the most common (or mode) response for participants increased from moderate in survey 1 to high in surveys 2 and 3.
PCP survey responses related to their knowledge and ability to administer ketamine.
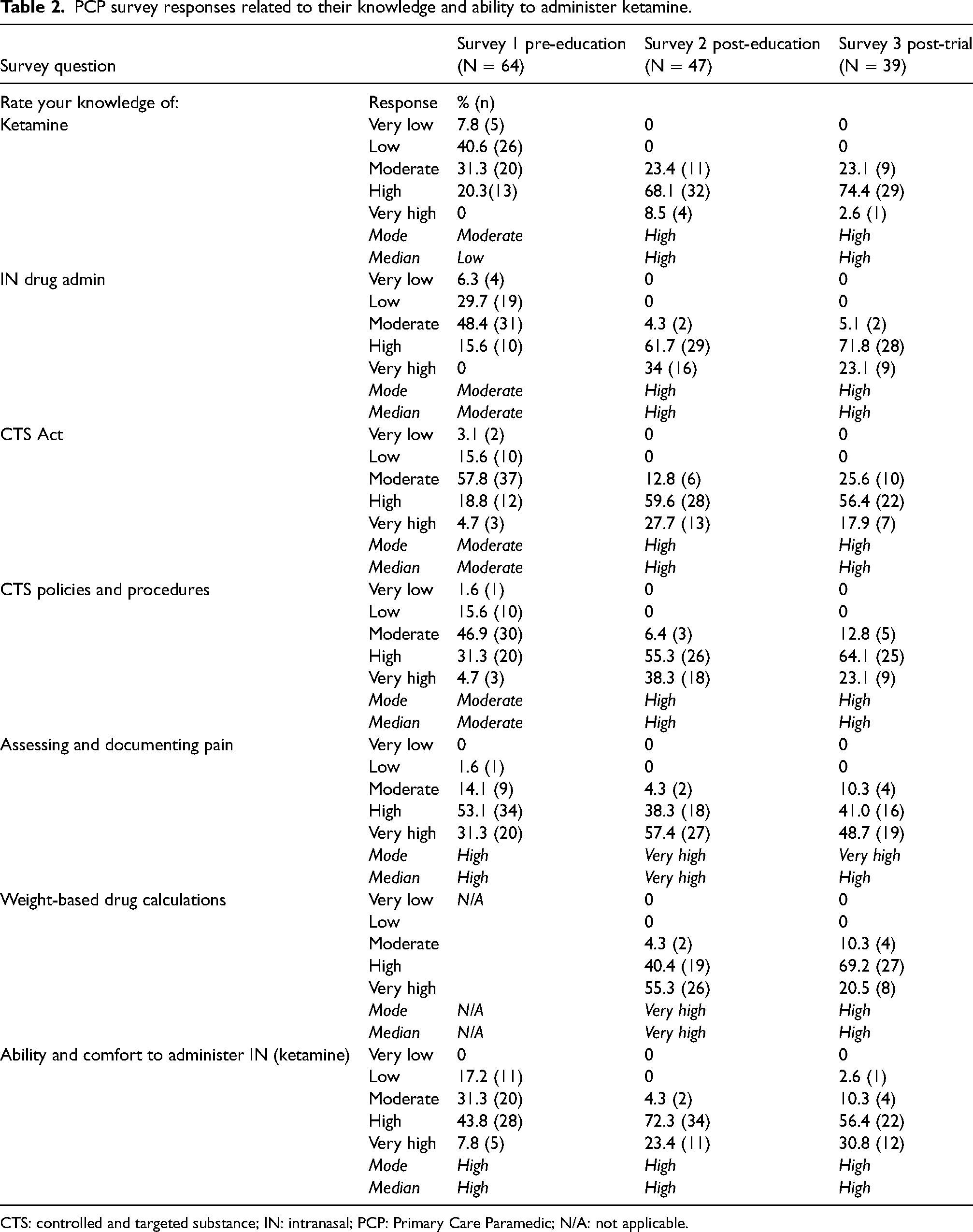
CTS: controlled and targeted substance; IN: intranasal; PCP: Primary Care Paramedic; N/A: not applicable.
The mode response for knowledge related to assessing and documenting pain scores also increased from high in survey 1 to very high in the subsequent surveys. When asked to rate their knowledge of weight-based drug calculations in survey 2, post-education, both the mode and median responses were reported as very high. This then decreased to high in survey 3 at the end of the trial period. Respondents reported their comfort level and ability to administer IN drugs to be high at all points in the study (median and mode = high).
Overall, respondents who completed survey 2 reported that they were satisfied with the CTS education (median and mode = high) and very satisfied with the ketamine education (median and mode = very high).
Analgesia and organisational support
When asked to rate their satisfaction with nitrous oxide as an analgesic for their patients, respondents most often selected moderate as their response in survey 1 (mode and median = moderate) and low in survey 3, signalling a reduced opinion of nitrous oxide. By contrast, respondents rated ketamine as an analgesic option as very high (mode and median). Respondents indicated that they felt supported by BCEHS to administer CTS drugs with 70.5% (n = 45) and 87.2% (n = 34) selecting strongly or very strongly responses (mode and median = strongly) (Table 3).
PCP survey responses related to their views on analgesia and organisational support to administer ketamine.
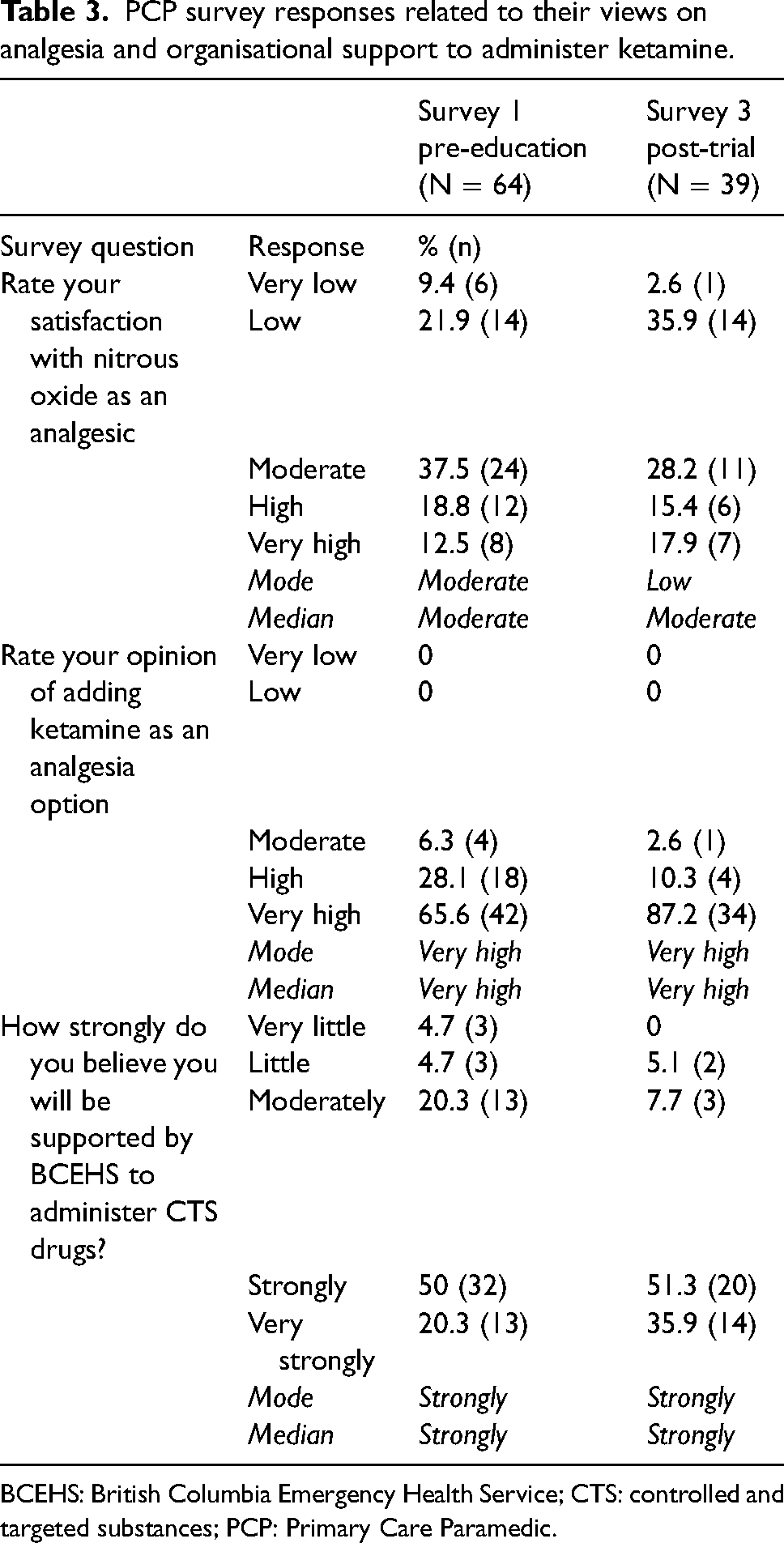
BCEHS: British Columbia Emergency Health Service; CTS: controlled and targeted substances; PCP: Primary Care Paramedic.
Qualitative focus group findings
Participant characteristics
Nine out of a possible 64 participants (14%) participated in focus groups at the end of the trial. Two in-person focus groups lasting approximately 45 min were held at the stations at times convenient to participants when they were off duty. Two participants had scheduling conflicts. The facilitators used the same series of focus group questions to collect their responses individually. Participants were primarily male (n = 6, 66.6%) with clinical experience ranging from 5 years to more than 16 years.
Barriers and enablers to implementation
Focus group data codes representing barriers and enablers to iPAKA were mapped to 10 of the 14 domains in the TDF: knowledge, memory, attention and decision processes, behavioural regulation, skills, environmental context and resources, beliefs about capabilities, beliefs about consequences, optimism, emotion and reinforcement (Table 4).
Focus group coding against domains of the TDF.
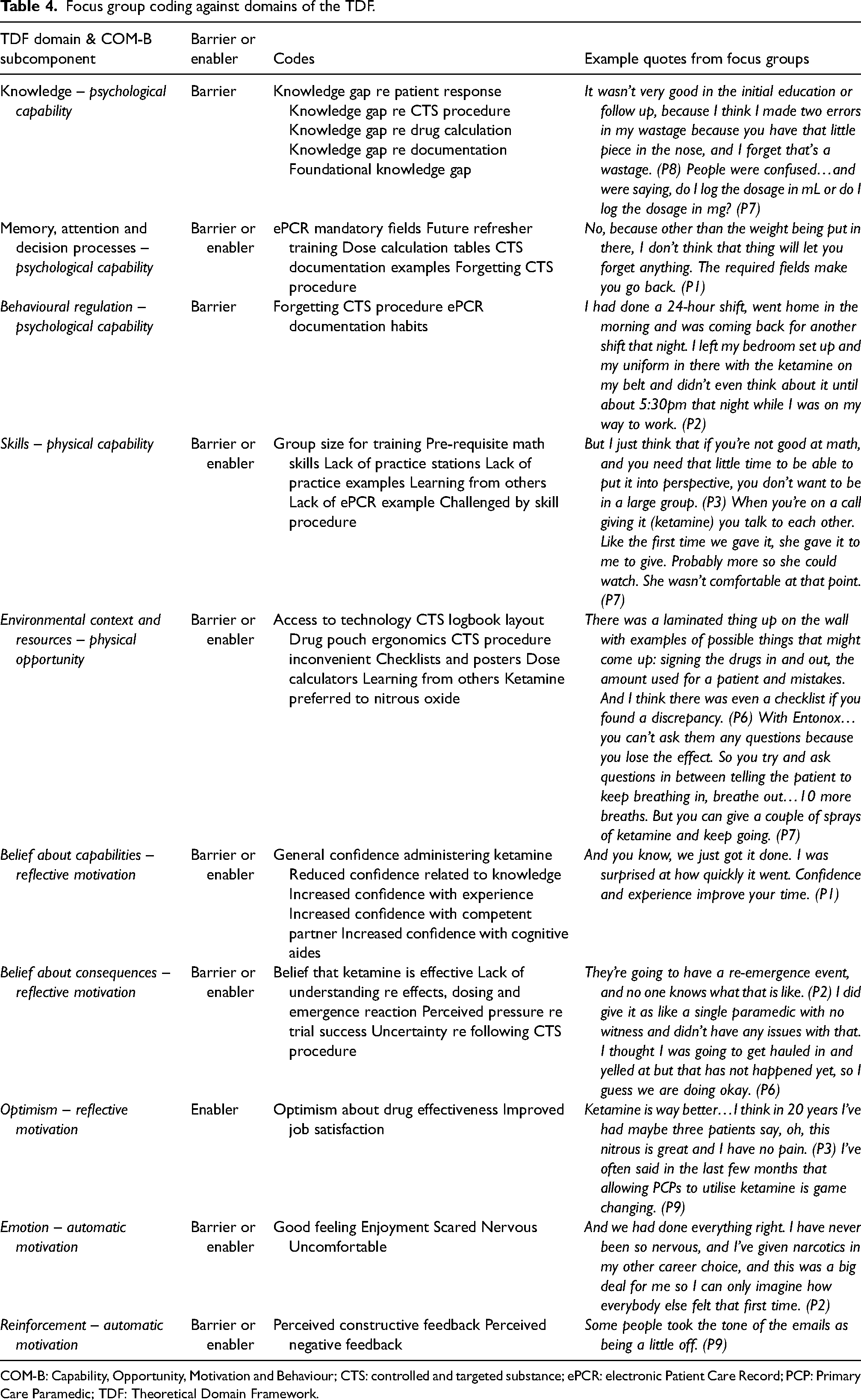
COM-B: Capability, Opportunity, Motivation and Behaviour; CTS: controlled and targeted substance; ePCR: electronic Patient Care Record; PCP: Primary Care Paramedic; TDF: Theoretical Domain Framework.
Integrated findings and analysis
The authors reviewed predominant findings from the surveys and focus groups to identify common themes using codes based on the COM-B and TDF. Data were integrated and assessed for convergent validity, complementarity and dissonance. 34 Seven theoretical domains of interest with relevant findings are presented below.
Knowledge
A person's capability is an attribute that makes a behaviour possible if they are given the opportunity. A psychological element of capability is knowledge or the awareness that something exists. 18 Findings in this study revealed how vital it is for PCPs to have the foundational knowledge required to administer ketamine and perform CTS procedures.
Consistent with survey findings where respondents reported high satisfaction with ketamine and CTS education, most participants spoke favourably of the education. However, participants also revealed gaps in the education. For example, the training did not adequately prepare them to explain to patients how ketamine would make them feel. This gap was further exacerbated by the PCPs' prior understanding of ketamine being used as a recreational drug. The other analgesia we’ve had experience with is easy to explain. (P2)
Especially ketamine which has a large recreational stigma around it … what most people know about ketamine use is like, oh, you get K-holed… but we had no idea what a patient was going to experience. (P1)
One participant highlighted that PCPs had not previously been expected to know how to document CTS drug administration. They recounted having to learn to use aspects of the electronic Patient Care Record that they admitted to ignoring in the past. These included specifying the paramedic that administered a medication, populating the ‘wastage’ and ‘patient weight’ fields and documenting pain scores in the ‘pain’ fields rather than the free text or not at all.
Participants also commented on initial difficulties learning to use the CTS logbook, performing drug counts and accounting for drug waste associated with dead space in the medication mucosal atomiser device. It's been explained to me umpteen dozen times about the dead space and the 0.1 mL, but I cannot for the life of me wrap my head around that. I just I don’t know why, I just I don’t get it. That's just the way my brain works. (P3)
Memory, attention and decision processes
Memory, attention and decision processes, another psychological subcomponent of capability, are described as one's ability to retain knowledge, select between multiple options and focus on features in the environment.
18
The study findings revealed that while participants generally rated their knowledge levels high, some PCPs struggled to recall or apply the knowledge. Despite survey respondents reporting an increase in CTS-related knowledge from moderate to high throughout the trial, focus group findings highlighted being able to retain and recall specific knowledge as a barrier. For example, one participant explained how they struggled to remember to replace a used drug vial. Or forgetting at the end of the day that you’ve used one and forgetting that you have to actually pull one out and return it. That was as hard for the first call…because it just took a minute to get your mind wrapped around that. Okay, I need to refill so I’m taking one out, but I need to put two back. (P8)
Some PCPs also could not recall how to perform drug calculations in real time and emphasised the usefulness of pre-calculated weight/dosage charts. The survey results supported these findings where knowledge of weight-based drug calculations was lower at the end of the trial period (mode/median = high) compared to just after the education (mode/median = very high).
Other participants found it hard to recollect the process to complete the CTS logbook when starting a new page and suggested that an example be made available on each page. Just a simplified book would be helpful… or even an example on each page…because the worst was always ..oh, no, I’m the last person and I’m going to flip it over to the next page. (P4)
Environmental context and resources
Combined with capability, people require the opportunity to perform a given behaviour. The physical subcomponent of opportunity involves the environmental context and resources, referring to elements or characteristics of the workplace that either assist or hinder one's ability to perform the behaviour. 18 The study participants identified numerous physical aspects of their environment that influenced their ability to administer ketamine, both positively and negatively.
The CTS logbook and sign-out procedure presented barriers in that they were reportedly confusing. For on-call staff who reported to the station multiple times in a shift, they did not always elect to sign ketamine out from the safe as it was deemed too time consuming. When working on-call…we might sign it in and out three or four times in a shift. We’re in a busier station…and I know some people just opted not to sign it out because of that. (P6)
Introducing a belt drug pouch was seen as a facilitator in that ketamine was readily available to administer compared to nitrous oxide which is more cumbersome. In contrast, the pouch posed a barrier for one participant who found it uncomfortable to wear while sitting or driving and described keeping it in his pocket instead of on his belt, a violation of the CTS policy. I hate the pouch. If there is an easier way to carry it that's not so bulky. I find it hits the seat belt or that it gives me bad posture when sitting down for too long in certain seats… I ended up putting it in my pocket because it was so uncomfortable. (P4)
To a small extent, technical issues were also reported as a barrier. For example, two participants described an instance when they did not have a mobile phone or laptop to access dosing charts. I don’t carry my own cell phone on a call and the car cell phone hadn’t been updated and it didn’t let me turn it on. She (my partner) didn’t have the handbook and couldn’t find the chart. And there was the two of us…writing all this down, doing the math until we finally got onto the laptop and the handbook that we could double check. (P3)
Participants mentioned a variety of additional useful references including dosage charts in the medical control guideline phone app, checklists and posters at the station and phone numbers for educators, station officers and Paramedic Specialists to call for assistance. Most staff members had access to a ‘locally made’ reference chart stored in the drug pouch, although this reportedly went missing when some PCPs either misplaced it or kept it for personal use.
Participants also identified the drug administration procedure as an enabler when compared to nitrous oxide. PCPs could administer a single dose of ketamine intranasally, while by contrast, the patient must keep the nitrous oxide mouthpiece in their mouth, making it difficult to communicate. The nitrous oxide set up is also large and relatively cumbersome. We are in the middle of the field so now I’m carrying the oxygen bottle and lugging the Entonox, whereas this one here (the ketamine), it was right there on my belt. I could give it to him before we even moved him. It was good. I mean, it's busy. Comparatively, it makes the call busy, especially when you’re by yourself. (P7)
Survey results complemented focus group descriptions of preferring to give ketamine over nitrous oxide. Rating their opinion of ketamine as very high, respondent satisfaction with nitrous oxide as an analgesic was moderate in survey 1 and rated lower by survey 3 (mode = low, median = moderate).
Emotion
Motivation, the third component of the COM-B model, is a combination of the automatic and reflective mental processes that stimulate and direct behaviours. The automatic emotion domain is defined as ‘a complex reaction pattern, involving experiential, behavioural and physiological elements by which the individual attempts to deal with a personally significant matter or event’. 18
The PCPs in this study described a range of emotions that were potential barriers to implementing ketamine. These related to the procedures and to perceived pressure to do things correctly. The first time I gave it, it was really scary because I was on with an EMR (Emergency Medical Responder) who had sat in on the training just for her own information. So that was really good…it was a bit nerve wracking for sure. It's a big deal. It was drilled into us during the training that you don’t mess this up. (P1)
One participant explained the discomfort some PCPs felt the first time they signed out ketamine, not having been responsible for controlled and targeted substances previously. You go to do the count…and the first time I went in there to do it, I’m (thinking) what do I do, because like I said it was brand new. I had never seen a book like that ever…everything was brand new and well it was drilled into us, do not screw this up…so yeah, I think everybody was a little on edge. (P2)
The survey results presented dissonant findings to the above statements. Though they were not specifically asked to rate their emotions, respondents did indicate at the start and completion of the trial that they ‘strongly’ believed they would be supported by their employer to administer CTS drugs (mode and median = strongly).
Participants also relayed positive emotions associated with giving ketamine. They expressed a strong sense of job satisfaction and were happy to provide what they perceived to be effective pain management to their patients. I’ve given it (ketamine) twice with the same partner and both times we got called the Dream Team and told “yeah this is the chill-est place and you guys are the best”. With his busted pelvis and his fractured collar bone, he was tickled pink. What a great feeling as a paramedic. It really was especially good after all these years of always bouncing down these mountain roads. (P3)
Ketamine was just instant, and it was obvious that it was working… I felt good knowing that I actually had a really good analgesic I could administer. I felt like a real paramedic…It worked really well, and I remember with some partners being super- jacked that we just did it, and it worked, and they (the patient) felt better…we did something good. (P4)
Belief about capabilities
Reflective TDF domains influencing motivation include belief about capabilities and consequences. Belief about capabilities is defined as ‘acceptance of the truth, reality or validity about an ability, talent or facility that a person can put to constructive use’. 18
In addition to rating their knowledge levels highly in the three surveys, respondents indicated a high level of comfort with their ability to administer IN ketamine (median and mode = high). Convergently, focus group participants described how confidence in their ability to administer ketamine continued to grow with experience. One PCP reflected that he initially struggled with the IN administration device but readily adapted his practice once he had some real-life experience using it. I don’t know that I did it right the first time because the lady said, ‘that's dripping down my throat’, so it might not have aerosolized. The next one I pushed a lot harder and had no complaints there. (P6)
Being partnered with a paramedic who had received the same training was also identified as a facilitator during the study. Had she (my partner) not been there, I would have probably opted not to have used it. And it worked out brilliantly for that lady, so it would have been a shame if I was uncomfortable. (P8)
Participants also described how electronic and paper-based reference tools and drug dosing charts were used as cognitive aides. If you are in a high stress situation and are starting to do complicated math, we have the little cheat sheets that went along with it …It makes it a lot safer…those calculations are not the easiest for a lot of people. (P9)
Belief about consequences
A second domain correlated to motivation is belief in consequences or how people perceive and accept possible outcomes related to performing a behaviour. 18 Participants provided mixed feedback related to the potential and real consequences of administering ketamine. Some focus group participants reported feeling ill-prepared to manage a ketamine overdose and emergence events, both barriers to administration. One participant highlighted that some patients had already been given opioids at the scene by ski patrol medics, causing unanticipated consequences and creating uncertainty.
Personal experience giving ketamine became a facilitator. For example, PCPs described how the medication did not necessarily reduce a patient's pain score but enabled them to successfully cope with their pain, which was a good outcome. The patients that I gave the ketamine to, it didn’t reduce their pain (score) to a 2 or 3. It more made them forget about the pain. I don’t know if it's that's what it's supposed to do. If they were sitting at an 8, 9 or 10, it brought them down to a 6 or a 7 but maybe that's just what they were thinking because they were high. (P5)
Optimism
Another domain associated with motivation is optimism. The TDF describes optimism as ‘the confidence that things will happen for the best or that desired goals will be attained’.
18
Participants’ experiences administering ketamine proved to be enablers to adopting the medication as part of their practice. All focus group participants relayed positive feedback on ketamine as an effective analgesic. It definitely adds to your job satisfaction when you see results like that. Thank you for allowing us to have it. It has been a long time coming as they have been talking about that since I started and its better pain control for us to use. (P4)
There were instances described during the focus groups in which the PCPs had decided to administer ketamine as a first-line analgesic rather than strictly adhering to the clinical practice guideline that required them to use it for severe pain intractable to nitrous oxide. There was one time where I did give it (ketamine) before the nitrous, but that's because this lady had broken her pelvis. I was thinking this is going to work, I know it. (P6)
If you walk up and someone is in excruciating pain and their right leg is bent up behind their left ear, and you think let's go to something that we know is going to be very effective. (P9)
This optimism was also evident in the survey results. Complementarity findings include respondents reporting very high opinions of adding ketamine as an analgesic option and decreasing satisfaction with nitrous oxide by the end of the trial period.
Identifying BCTs to address identified implementation barriers
Informed by evidence, Michie et al.'s 19 taxonomy of BCTs is arranged into 16 hierarchical groups. Examples of these groups include (1) goals and planning, (2) feedback and monitoring, (3) social support, (4) shaping knowledge and (5) natural consequences. The TDF domains representing identified barriers and enablers map to the BCTs to generate potential strategies to support successful implementation. 19 In this study, there were 38 BCTs that mapped to the 10 TDF domains identified in the focus group data. The researchers evaluated each BCT against the APEASE criteria 17 to determine its feasibility. Nine were selected as both theory-linked and feasible at BCEHS (Table 5).
Mapping TDF domains, barriers and enablers onto behavioural change techniques to help PCPs implement behavioural change in practice.
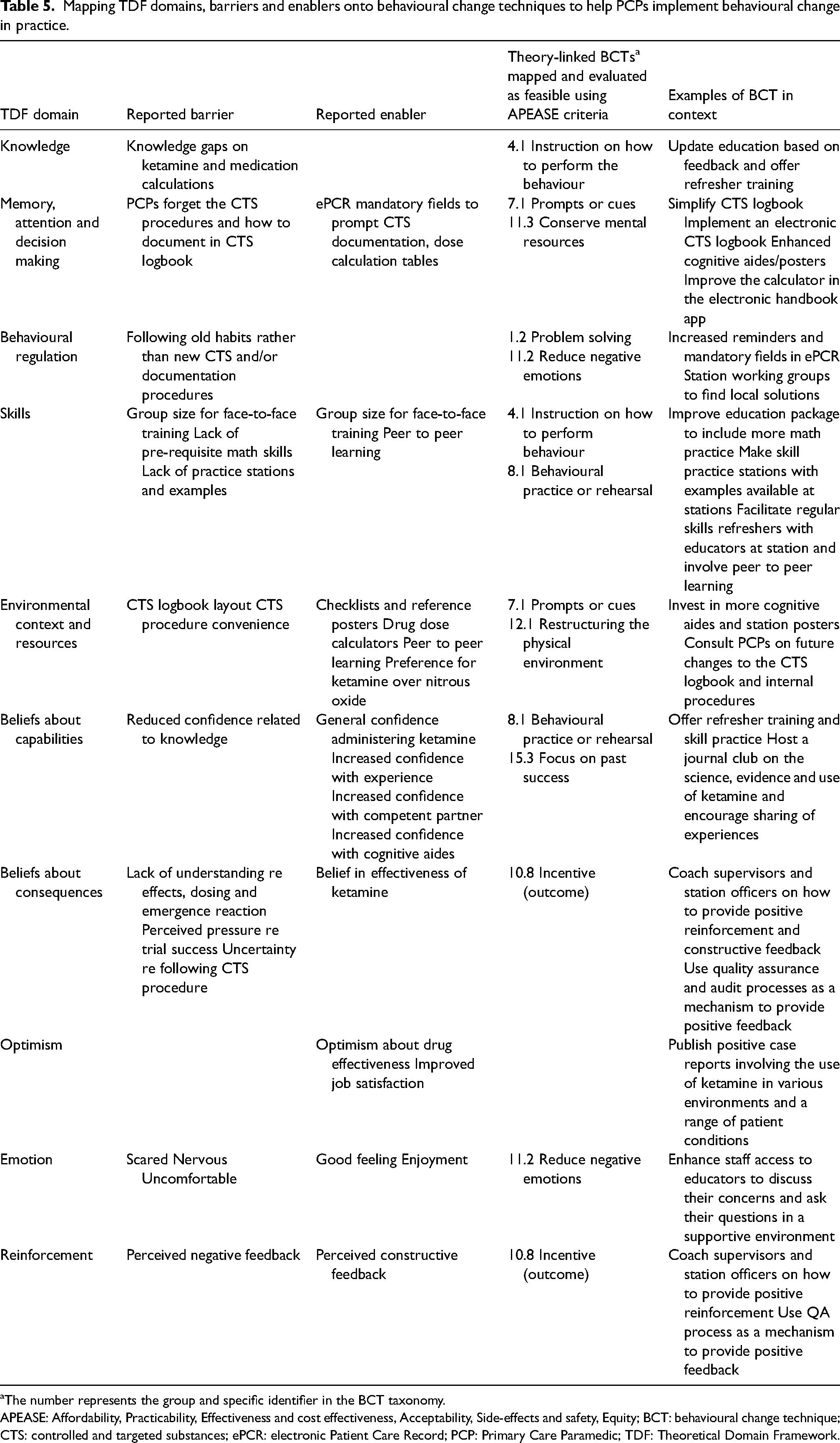
The number represents the group and specific identifier in the BCT taxonomy.
APEASE: Affordability, Practicability, Effectiveness and cost effectiveness, Acceptability, Side-effects and safety, Equity; BCT: behavioural change technique; CTS: controlled and targeted substances; ePCR: electronic Patient Care Record; PCP: Primary Care Paramedic; TDF: Theoretical Domain Framework.
Discussion
This study sought to explore the barriers and enablers to implementing a transformation of PCP practice, namely PCP-administered IN ketamine for analgesia. This was achieved through a parallel convergent mixed methods approach using survey data and focus groups. Implementing ketamine for PCPs was enabled by quality education, strong organisational support and the availability of cognitive aides such as dosage charts. The trial was also successful largely in part to the PCPs’ feelings of optimism around the change and the increase in job satisfaction they experienced when giving ketamine. Key barriers identified during the study included a significant knowledge gap involving drug dosage calculations, negative emotions associated with performance anxiety and a lack of field education and supervision to monitor paramedic practice.
Capability
It was evident that the participant's capability, including self-reported knowledge and skill level influenced the implementation of ketamine. The education proved an enabler with participants reporting increased knowledge in all aspects of the drug and associated procedures. Education and training are primary mechanisms to facilitate knowledge translation for allied health professionals and a proven strategy to introduce new initiatives.12,15,35 The PCPs also rated the education they received highly. High levels of satisfaction with staff training have been linked to increased participant self-confidence, further supporting learning and skill development. 36 A note of caution – while participants may report increased knowledge levels, this does not necessarily translate to successful implementation of a training initiative nor improve patient care. 8
While the survey results were overwhelmingly positive, the focus group data revealed important gaps in the initial education. For example, some participants stated that they were unsure how patients would respond to ketamine and what to expect or do during an emergence reaction. Others admitted to feeling uncertain about specific CTS procedures and documentation practices. In addition, the PCPs in this study rated their knowledge of weight-based drug calculations lower at the conclusion of the trial as compared to post-education. These findings are consistent with other implementation research that identifies how knowledge gaps 15 can significantly impede initiatives to improve clinical practice.13,37 To improve knowledge transfer in health professions, researchers advocate for staff consultation and for the end user to be involved in development of the education curriculum.8,38 Although feedback as an enabler was not reported in this study, this is highlighted elsewhere as an important activity for successful knowledge transfer.36,39 In addition, post-training support provided by experts is required to maintain clinical knowledge and skills over time. 40 As BCEHS considers a wider rollout of PCP-administered ketamine, they can integrate study findings with evidence informed behavioural techniques to support paramedic capability aspects of the practice change. These could include involving PCP feedback to update and enhance the theoretical and practical education curriculum and improving access to quality cognitive memory aides. They might also increase staff access to field educators who would provide feedback and offer skill practice sessions with regular refresher training.
Opportunity
The opportunity to perform a behaviour cannot be underestimated, especially in the paramedic context. Participants revealed how the CTS procedures created barriers. In one poignant example, when the sign-out process proved too cumbersome, some PCPs simply elected not to carry ketamine. One participant described storing the drug in their pocket instead of the assigned belt pouch that was uncomfortable to wear. Administrative issues are a known barrier for healthcare workers expected to adapt to new forms or processes. 41 Compliance presents a significant challenge to monitor in the paramedic setting. Paramedics work relatively independently with little direct clinical oversight or supervision. 42 Thus, the success of an implementation strategy in paramedicine is largely reliant on the individual practitioner's decision to follow new processes. Our study revealed instances in which paramedics elected to not follow their guidelines. They gave ketamine as a first-line analgesic contrary to the CPG that allows for ketamine after nitrous oxide proves ineffective. Paramedic non-adherence to practice guidelines is a known phenomenon,43,44 likely due to the perceived inflexible nature of CPGs and the reality of the dynamic environment and complex setting where paramedics make clinical decisions. 45 It is important that practitioners be included in early consultation of policies, procedures, clinical practice guidelines and processes to ensure they will work as intended and will be adhered to in the real-world setting.
The decision to use weight-based doses instead of a fixed dose had significant ramifications in the study. Participants identified challenges associated with math calculations, something underestimated by the implementation team. Participants provided examples wherein they struggled to calculate the correct dose. This finding is consistent with a recent review that revealed how the uncontrolled nature of the pre-hospital setting negatively impacts cognition and increases the risk of medication errors. The often-stressful nature of paramedicine can lead to drug calculation errors, emphasising the importance of medication dosing aides. 46 Indeed, our findings illustrated that paramedics relied heavily on cognitive aides such as the phone handbook app, drug reference charts and reference cards, and could benefit from additional resources.
Our study also highlighted how participants viewed ketamine as much simpler to administer than nitrous oxide once the dose was calculated. This is especially useful for PCPs who may be responding alone. There is evidence that paramedics will adjust their practice in response to environmental factors such as whether items are stored in a convenient location. 44 It is a reminder of how different the physical setting is for paramedics compared to healthcare workers who practice where others are typically available to assist them. Working independently in an uncontrolled environment with little oversight and assistance places an increased level of responsibility on paramedics. 47 To facilitate a successful wider implementation of ketamine, BCEHS can use these findings and associated BCTs involving restructuring the physical environment in consultation with PCPs.
Motivation
Impacted by their capability and opportunity, our study revealed the complex nature of participant motivation as evidenced by belief in their capabilities, their optimism and emotions. Self-efficacy is the belief and judgement of one's capability to perform specific tasks or behaviours. 48 As Bandura 48 contends, ‘there is a marked difference between possessing knowledge and skills and being able to use them well under taxing conditions’. While higher levels of self-efficacy are known to enable a higher number of skill attempts and success rates, a lack of professional efficacy and self-confidence are commonly reported barriers to optimal clinical practice.13,39 Our study demonstrated how participant confidence increased after they gained experience giving ketamine, especially if they had a competent partner. One participant raised the issue of low call volumes in remote stations. Low exposure to skills in these settings is known to erode self-confidence and highlights the importance of re-training to increase self-efficacy. 49 Despite reporting several procedural issues and missteps related to dosing, preparing and administering the medication, our study participants rated themselves as ‘highly confident’ to administer ketamine at all points in the trial. This raises important questions about the relationship between PCPs' belief in their capabilities and skill performance and their true competence. While our study did not directly measure how the PCPs performed, the literature highlights dissonance between paramedic self-efficacy ratings and skill performance in airway management for example.35,49 Similar discordance is presented elsewhere between medical residents’ confidence levels to perform paediatric skills and their assessed abilities. 50 This has implications for BCEHS who could provide additional skill practice sessions with feedback mechanisms to support current and future PCP skill performance that more closely aligns with their confidence levels.
This study also revealed important findings related to PCP optimism and emotions. Participants had highly positive opinions about ketamine and low to moderate views about the use of nitrous oxide for analgesia. All PCPs shared examples of how administering ketamine increased their professional satisfaction including how one ‘felt like a real paramedic’ and another described it as ‘game changing’. Health care professionals’ attitudes to new treatments or therapies are known to play a role in how widely they are adopted. 41 Clinicians are more likely to embrace a change that addresses what they perceive to be an important gap 51 and are more optimistic when they feel engaged and clearly understand the reason for the change. 52 However, participants also reported experiencing negative emotions during the trial. For example, despite survey results suggesting that they felt supported, participants revealed emotional stress related to assuming personal and professional responsibility for enhanced practice. Some participants commented on the pressure they felt to succeed and not to ‘mess up’ or ‘screw this up’ during the trial. The PCPs also described their feelings during the trial using terms such as ‘scary’, ‘nerve wracking’ and ‘on edge’. Fear of making a mistake, high staff expectations and general feelings of stress can erode confidence and clinical performance.39,53 Factors that cause negative emotions can hinder self-confidence and create barriers. The BCTs that address motivation are aimed at improving self-confidence, building on past success and fostering positive emotions. Accordingly, it is important that implementation teams at BCEHS provide constructive and supportive feedback through QA processes, create opportunities for two-way communication and provide resources to support PCPs struggling with change. They might also offer managers and educators contemporary training on coaching and mentoring and the implementation of a just culture approach.
Limitations
There are several limitations associated with this study. First, the TDF is detailed and resource intensive to use. There is no guidance on how to code data that represents multiple domains while the BCTs target individual domains. Next, the sampling method and size is a limitation. While the organisation purposely limited participation to a small number of PCPs in three rural stations, this reduces the generalisability of the findings across the province and outside of BC. There was initially a 100% participation rate from the 64 eligible PCPs who could give ketamine only if they consented to the study, completed the survey and received the education. Despite being sent a reminder, subsequent survey participation declined to 73.4% and 60.9% when the PCPs had the option to complete the surveys. The results could be biased by more positive responses from participants more inclined to complete the surveys. Future studies could expand upon initial findings to include participation from a larger, more representative group of PCPs across the province. The sample size limitation is also present in the focus group findings. Unfortunately, the focus groups were hosted during a particularly challenging time when the PCPs were facing multiple professional demands on their time, including BCEHS’ response to the COVID-19 pandemic, record breaking heat waves and wildfires. This likely impacted participation rates and reduces generalisability of the qualitative findings. In the future, researchers should be mindful of how wider organisational and societal factors can impact study findings and schedule accordingly.
Conclusion
The use of theoretical frameworks and models like COM-B/TDF serves to improve the sustainable implementation of behaviour and clinical practice change in paramedicine. When project teams use theory to guide design and implementation, they can systematically identify and target individual and organisational enablers and barriers to adopting routine practices. The iPAKA study reveals key barriers and facilitators in several domains of the TDF and presents evidenced based targeted behavioural techniques that BCEHS can use to support on-going implementation of PCP-administered IN ketamine for analgesia.
Footnotes
Acknowledgements
The authors would like to acknowledge the staff members at BCEHS who contributed to this study including Chad Dietz, Trevor Campbell, Karly Jones, Duane Leslie, Lee Roberts, Kevin Lambert, Toby Mcleod, Kirk Pitaoulis, Scott Lequesne, Brian Silvester, Alex Shanny, Leon Baranowski, Randy Hansen, Alison Garrett, Jennifer Molhoj, Ryan Ackerman, Mike Sugimoto, Loyd Ondang, Dr Anders Ganstal and the Primary Care Paramedics at Vernon, Armstrong and Revelstoke stations.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AB is Deputy Editor of Paramedicine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix A
The 14 domains of the TDF and exemplar construct examples (adapted from Cane et al.
18
). TDF: Theoretical Domains Framework.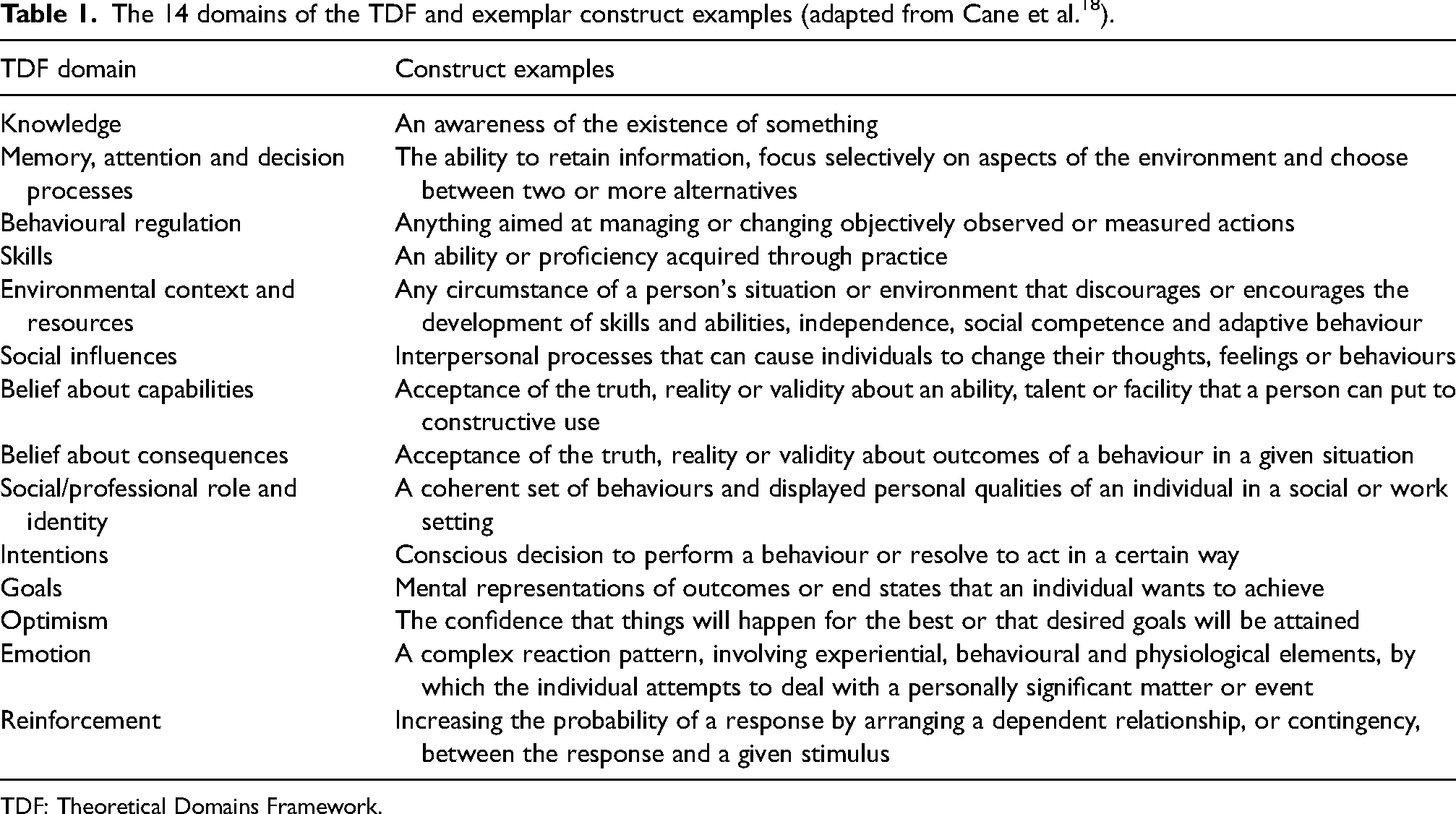
TDF domain
Construct examples
Knowledge
An awareness of the existence of something
Memory, attention and decision processes
The ability to retain information, focus selectively on aspects of the environment and choose between two or more alternatives
Behavioural regulation
Anything aimed at managing or changing objectively observed or measured actions
Skills
An ability or proficiency acquired through practice
Environmental context and resources
Any circumstance of a person's situation or environment that discourages or encourages the development of skills and abilities, independence, social competence and adaptive behaviour
Social influences
Interpersonal processes that can cause individuals to change their thoughts, feelings or behaviours
Belief about capabilities
Acceptance of the truth, reality or validity about an ability, talent or facility that a person can put to constructive use
Belief about consequences
Acceptance of the truth, reality or validity about outcomes of a behaviour in a given situation
Social/professional role and identity
A coherent set of behaviours and displayed personal qualities of an individual in a social or work setting
Intentions
Conscious decision to perform a behaviour or resolve to act in a certain way
Goals
Mental representations of outcomes or end states that an individual wants to achieve
Optimism
The confidence that things will happen for the best or that desired goals will be attained
Emotion
A complex reaction pattern, involving experiential, behavioural and physiological elements, by which the individual attempts to deal with a personally significant matter or event
Reinforcement
Increasing the probability of a response by arranging a dependent relationship, or contingency, between the response and a given stimulus
Appendix B
Key activities performed to prepare for and initiate the iPAKA trial at three ambulance stations. CMP: Clinical and Medical Programmes; CTS: controlled and targeted substances; ePCR: electronic Patient Care Report; IN: intranasal; iPAKA: intranasal paramedic administered ketamine analgesia, PCP: Primary Care Paramedic; PPL: paramedic practice leader.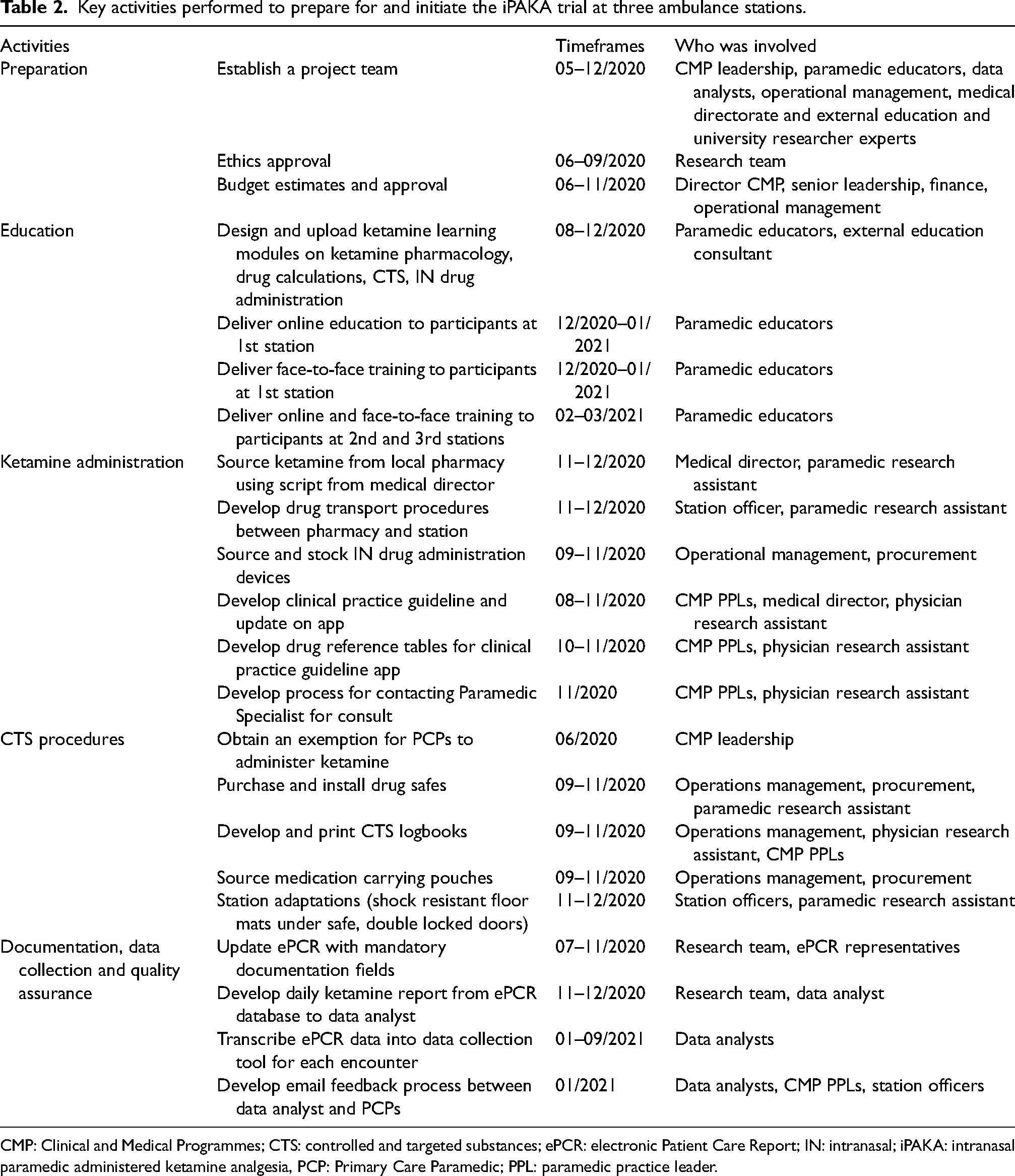
Activities
Timeframes
Who was involved
Preparation
Establish a project team
05–12/2020
CMP leadership, paramedic educators, data analysts, operational management, medical directorate and external education and university researcher experts
Ethics approval
06–09/2020
Research team
Budget estimates and approval
06–11/2020
Director CMP, senior leadership, finance, operational management
Education
Design and upload ketamine learning modules on ketamine pharmacology, drug calculations, CTS, IN drug administration
08–12/2020
Paramedic educators, external education consultant
Deliver online education to participants at 1st station
12/2020–01/2021
Paramedic educators
Deliver face-to-face training to participants at 1st station
12/2020–01/2021
Paramedic educators
Deliver online and face-to-face training to participants at 2nd and 3rd stations
02–03/2021
Paramedic educators
Ketamine administration
Source ketamine from local pharmacy using script from medical director
11–12/2020
Medical director, paramedic research assistant
Develop drug transport procedures between pharmacy and station
11–12/2020
Station officer, paramedic research assistant
Source and stock IN drug administration devices
09–11/2020
Operational management, procurement
Develop clinical practice guideline and update on app
08–11/2020
CMP PPLs, medical director, physician research assistant
Develop drug reference tables for clinical practice guideline app
10–11/2020
CMP PPLs, physician research assistant
Develop process for contacting Paramedic Specialist for consult
11/2020
CMP PPLs, physician research assistant
CTS procedures
Obtain an exemption for PCPs to administer ketamine
06/2020
CMP leadership
Purchase and install drug safes
09–11/2020
Operations management, procurement, paramedic research assistant
Develop and print CTS logbooks
09–11/2020
Operations management, physician research assistant, CMP PPLs
Source medication carrying pouches
09–11/2020
Operations management, procurement
Station adaptations (shock resistant floor mats under safe, double locked doors)
11–12/2020
Station officers, paramedic research assistant
Documentation, data collection and quality assurance
Update ePCR with mandatory documentation fields
07–11/2020
Research team, ePCR representatives
Develop daily ketamine report from ePCR database to data analyst
11–12/2020
Research team, data analyst
Transcribe ePCR data into data collection tool for each encounter
01–09/2021
Data analysts
Develop email feedback process between data analyst and PCPs
01/2021
Data analysts, CMP PPLs, station officers
Appendix C
Paramedic Education and Scope of Practice in British Columbia (BC).
Aligned with the Paramedic Association of Canada's National Occupational Competency Profile (NOCP), 54 multiple levels of Emergency Medical Assistants (EMA) in BC are defined as ‘paramedics’ and regulated under the Emergency Health Service Act administered by the Emergency Medical Assistants Licensing Board (EMALB). 55 These include Emergency Medical Responders (EMRs), Primary Care Paramedics (PCPs), Advanced Care Paramedics (ACPs) and Critical Care Parmedics (CCPs).
The Justice Institute of British Columbia (JIBC) is the only accredited post-secondary educational institution in BC offering training for PCPs and ACPs. To study the PCP certificate at JIBC, prospective students must either have a high school certificate or be a mature age student and have completed a 15-day EMR course. The current PCP certificate involves 8 months full time study including 600 h of classroom training and 3 months practical ambulance placement with BCEHS. 56 PCPs working with BCEHS are licensed by the Emergency Medical Assistants Licensing Board (EMALB). Their license outlines a specific scope of practice including all EMR basic assessment and resuscitation skills. PCPs are also licensed to perform intermediate airway management with supraglottic airway devices, administer several medications via varied routes and initiate intravenous access and electrocardiograph monitoring. The complete scope of practice is available in the EMA Regulation Schedule 1. 57 As the employer, BCEHS determines the scope of practice that PCPs can utilise by following Clinical Practice Guidelines (CPGs) outlined in the BCEHS Handbook. 58 At the time of the intranasal paramedic administered ketamine analgesia (iPAKA) study, the PCPs at BCEHS could only administer nitrous oxide to manage pain.
PCPs can further their studies at JIBC to become an ACP. The advanced diploma in ACP consists of 20 months full time study and includes 3 practical ambulance placements. Consistent with the NOCP, ACP education is focused on using advanced technology, clinical decision making and leadership, additional emergency treatments and advanced pharmacology. 56 A select number of experienced ACPs can apply to study a purpose-built vocational CCP programme offered in partnership between BCEHS and JIBC. The course is approximately 24 months in length and prepares CCPs to work in the air ambulance environment. 5
In 2017, BCEHS credentialed a cohort of experienced ACPs and CCPs as Paramedic Specialists. The Paramedic Specialists received additional training in patient resuscitation and clinical leadership, high-risk situations, complex patient events and telephone consultation. 59 The Paramedic Specialists support their PCP and ACP colleagues both in the field as a backup resource in metro areas and through the coordination centre by providing phone advice.
Appendix D
Survey questions
Survey 1 – pre-ketamine education
Invitation to participate
Are you a Primary Care Paramedic (PCP)?
Indicate your primary station.
How many years of PCP experience do you have?
Likert scale: very high, high, moderate, low, very low
Rate your current knowledge regarding the drug ketamine.
Rate your current knowledge regarding intranasal drug administration.
Rate your current knowledge of the Controlled and Targeted Substances Act.
Rate your current knowledge of the Controlled and Targeted Substances policies and procedures at BCEHS.
Rate your current knowledge of assessing and documenting patient pain scores.
Rate your current ability and comfort level to administer medications via the intranasal route.
Rate your satisfaction level with PCPs using inhaled nitrous oxide as analgesia to manage patient pain.
Rate your opinion of the value of adding ketamine as an alternate analgesia option for PCPs to manage patient pain.
How strongly do you believe you will be supported by BCEHS to administer controlled substances as regulated under National Law?
Is there anything else you would like to comment on regarding PCP analgesia?
Survey 2 – post-ketamine education
Same as survey 1 with the addition of:
Rate your current knowledge of performing weight-based drug calculations.
Rate your satisfaction with the education you were provided on ketamine.
Rate your satisfaction with the education you were provided on the Federal Controlled and Targeted Substances (CTS) Act and related BCEHS policies and procedures.
Is there anything else you would like to comment on regarding the online or face to face education for PCP analgesia?
Survey 3 – at the end of trial
Same as survey 1 with the addition of:
Did you have the opportunity to give ketamine (or assist to give it) during the trial period?
Rate your current knowledge of performing weight-based drug calculations.
Appendix E
Focus group question guide
Education and training
Do you feel that the education and training provided enabled you to use intranasal (IN) ketamine safely and effectively? Why or why not?
Probing question: Was the type and duration of training sufficient? Probing question: What could have been done better to improve the quality of the training? Was the training delivery method used, including blended learning with both online and face-to-face components effective? Why or why not?
Probing question: What education delivery method would you prefer? Probing question: Has BCEHS provided you with training in the past that used an approach you think would have been suitable here? Documentation and Controlled and Targeted Substance (CTS) procedures Did you have any challenges following the CTS procedures? If so, what challenges did you have?
Probing question: Do you feel that the CTS procedures provided enough security for the CTS medication? If not, what could be done better? Probing question: Did you feel well prepared to follow the CTS procedure and was enough support available? Probing question: What could be done to improve the paramedic experience with using CTS medications? Did you have any challenges completing the required medication sections in the patient care report for the use of ketamine? If so, what challenges did you have?
Probing question: What could be done to improve the paramedic experience with documenting the use of medications and wastage of CTS medications? Experience using IN ketamine as an analgesic agent Please share your thoughts about ketamine as an analgesic agent as compared to nitrous oxide?
Probing question: In your experience, is ketamine more effective, less effective, or about the same as nitrous oxide? Probing question: In your experience, is ketamine easier to use, more difficult to use, or about the same as nitrous oxide? Probing question: In your experience, did ketamine produce more or less side effects as compared to nitrous oxide? Recommendations for further implementation of IN ketamine What advice do you have for us if we plan to expand the use of ketamine to other parts of British Columbia? Do you see any barriers to implementation?
Probing question: Could the training be improved? Probing question: Could the clinical practice guidelines be improved? Probing question: Could the CTS procedures be improved?
Appendix F
PCP survey demographic results. PCP: Primary Care Paramedic.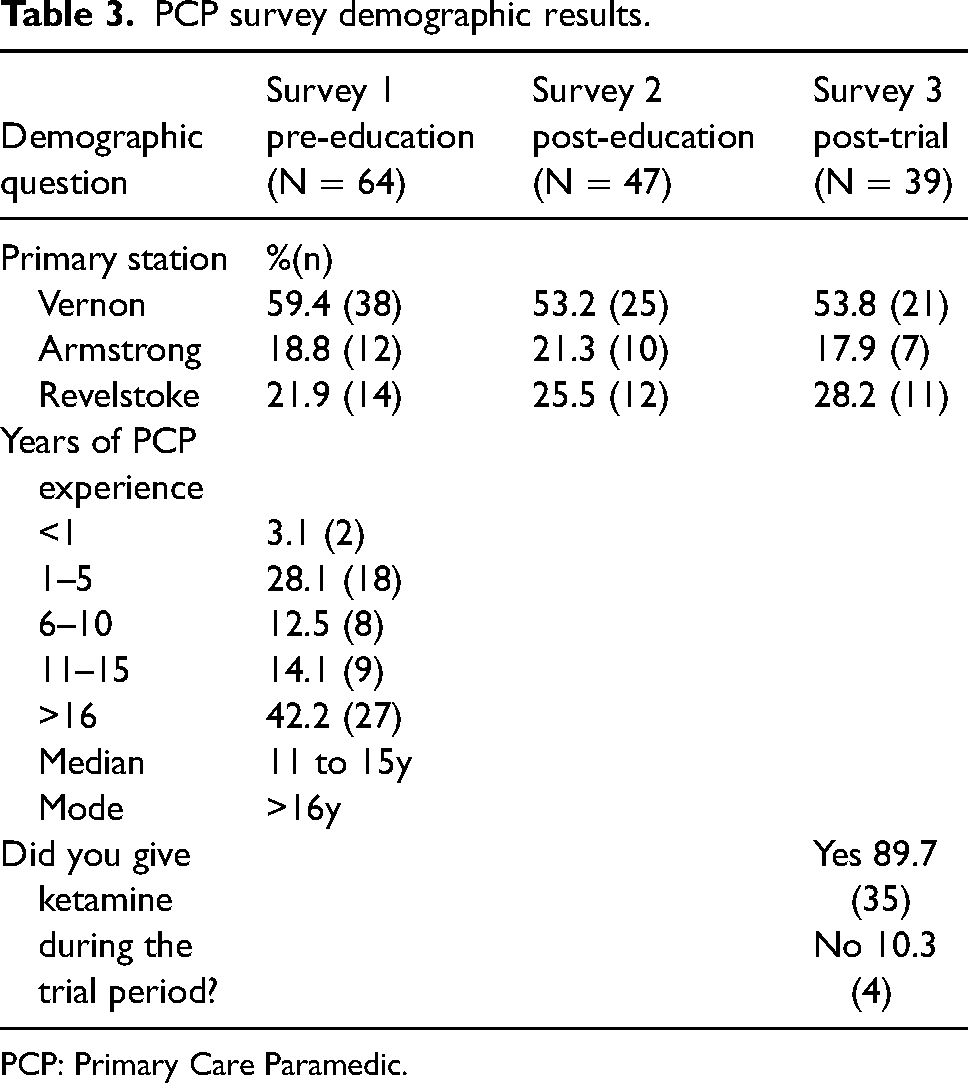
Demographic question
Survey 1 pre-education (N = 64)
Survey 2 post-education (N = 47)
Survey 3 post-trial (N = 39)
Primary station
%(n)
Vernon
59.4 (38)
53.2 (25)
53.8 (21)
Armstrong
18.8 (12)
21.3 (10)
17.9 (7)
Revelstoke
21.9 (14)
25.5 (12)
28.2 (11)
Years of PCP experience
<1
3.1 (2)
1–5
28.1 (18)
6–10
12.5 (8)
11–15
14.1 (9)
>16
42.2 (27)
Median
11 to 15y
Mode
>16y
Did you give ketamine during the trial period?
Yes 89.7 (35)
No 10.3 (4)