
Abstract
Background:
Continuing professional development (CPD) is essential for maintaining competency and quality in healthcare practice, yet low- and middle-income countries (LMICs) often lack practical guidance to design, implement, and sustain CPD programs. While implementation science frameworks provide theoretical structure, accessible tools to operationalize these frameworks for rehabilitation workforce development remain limited. This study describes the development and pilot testing of the Clinical Skills Training Tool (CSTT); a theory-informed, planning and evaluation tool to support contextually relevant CPD development for rehabilitation professionals.
Methods:
The CSTT was developed using implementation science frameworks, including the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework and the Consolidated Framework for Implementation Research (CFIR), and incorporated the Kirkpatrick model to guide CPD evaluation. The tool was piloted between 2021 and 2024 with multidisciplinary rehabilitation stakeholders in Myanmar, Ukraine, Uganda, and Pakistan. Data were collected through stakeholder workshops, structured planning activities, guided reflections, and evaluation of CPD programs developed using the tool. Qualitative framework-informed analysis was used to assess usability, feasibility, contextual adaptation, and implementation factors influencing tool use.
Results:
A total of 191 stakeholders participated in CSTT pilot implementation across 4 countries. The tool supported systematic identification of workforce training priorities, structured CPD program design, and development of evaluation strategies. CSTT-supported programs demonstrated improvements in stakeholder knowledge, clinical confidence, and adoption of structured evaluation practices. Stakeholders successfully adapted the tool across diverse health system contexts while maintaining fidelity to core planning processes. Iterative refinement improved usability, clarity, and sustainability guidance.
Conclusions:
The CSTT operationalizes implementation science frameworks into a practical, adaptable tool to support CPD planning and evaluation in LMIC rehabilitation settings. By bridging the gap between implementation theory and workforce development practice, the CSTT provides a scalable approach to strengthening rehabilitation workforce capacity and supporting sustainable CPD systems across diverse global contexts.
Keywords
Introduction
Rehabilitation encompasses interventions that aim to improve functioning and minimize disability for individuals experiencing health conditions within the context of their daily environments. 1 It is recognized as a fundamental component of universal health coverage and plays a critical role in supporting individuals’ ability to participate fully in society across the lifespan. 2 The global demand for rehabilitation services is increasing rapidly, driven by population aging, the growing prevalence of noncommunicable diseases, traumatic injuries, and disability associated with conflict and humanitarian crises.3,4 Despite this increasing need, rehabilitation systems in many low- and middle-income countries (LMICs) remain insufficiently developed and inadequately resourced, with limited integration into national health systems. 5 Workforce shortages are a major contributing factor, including insufficient numbers of physiotherapists, occupational therapists, speech and language therapists, and prosthetists and orthotists to meet population needs. 2 Even where rehabilitation professionals are present, access to structured opportunities for ongoing professional development is often limited, contributing to variability in clinical practice and constrained service capacity.
Continuing professional development (CPD) is essential to maintaining competency, supporting workforce development, and improving healthcare quality. 6 CPD enables rehabilitation professionals to integrate evolving evidence into practice, strengthen clinical reasoning, and respond to emerging population health needs.6,7 In LMICs, however, CPD opportunities are often inconsistent, fragmented, or unavailable due to resource constraints, limited institutional infrastructure, and lack of structured planning frameworks. CPD is not routinely mandated, and participation remains low due to multiple access barriers.6,8,9 The development and implementation of comprehensive CPD systems in these contexts are often hindered by limited financial, infrastructural, and human resources. 6 As a result, healthcare systems in LMICs may struggle to keep pace with changing care demands, resulting in gaps in provider competencies and service quality.
While numerous reviews have explored CPD systems in high income countries offering insights into system design, governance, and sustainability, their applicability to LMICs is often limited.10 -12 The socio-economic, cultural, and political conditions in these settings differ significantly from those in wealthier countries, necessitating context-specific strategies for CPD system development. More recently, a growing body of literature has begun to focus specifically on CPD systems within LMICs.13 -20 For instance, Magwenya et al offered a global overview of CPD frameworks. 17 It was discovered that legislative frameworks for encouraging participation in CPD were not universally present in all countries. Expert and mentor availability was a barrier in resource limited countries. Furthermore, there are few theoretical frameworks for evaluating quality of CPD offered. Other studies explored access to CPD including digital platforms and international collaborations.15,18 Despite these valuable contributions, most studies highlight the lack of detailed guidance on the processes involved in CPD system development and sustainability in LMICs. 21
Strengthening CPD infrastructure is therefore essential to support workforce capacity, improve service quality, and expand equitable access to rehabilitation. Stakeholders often face uncertainty regarding where to begin, how to structure effective CPD programs, and what factors are critical to long-term success. To date, no comprehensive resource exists that consolidates this information into a user-friendly, actionable tool designed specifically for LMIC settings. This manuscript describes the development of a novel tool, the Clinical Skills Training Tool (CSTT), intended to support stakeholders in LMICs, such as government bodies, health professional councils, educational institutions, and implementing partners, in the planning, development, and strengthening of CPD systems for healthcare professionals. We hypothesized that CSTT use would be feasible and acceptable across diverse LMIC rehabilitation contexts and would support stakeholders to systematically design and evaluate CPD aligned with local needs.
Methods
Theoretical Frameworks
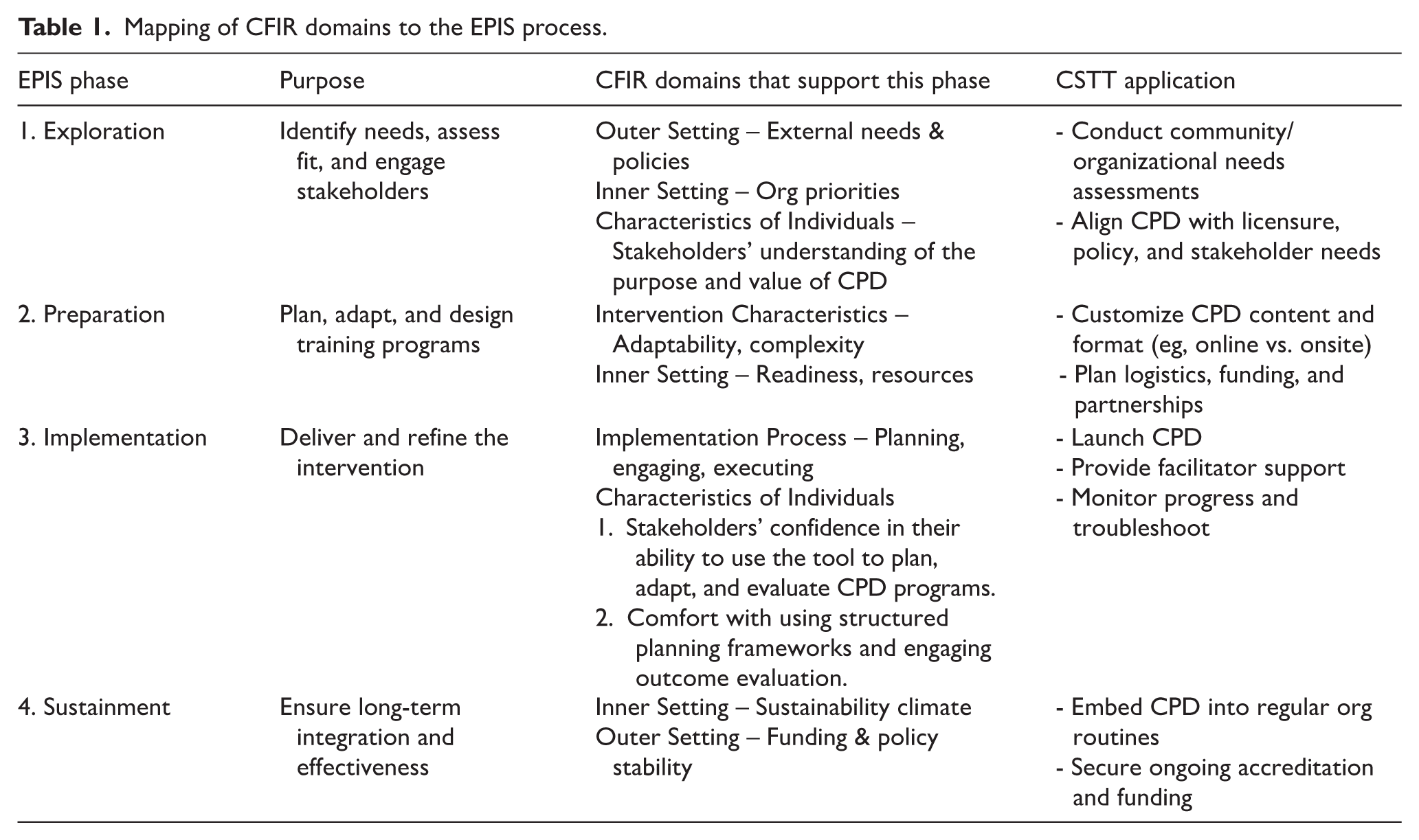
The tool integrates 2 complementary frameworks from implementation science: the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework and the Consolidated Framework for Implementation Research (CFIR).22,23 EPIS provides a phased structure to support systematic planning and integration of CPD within health systems. 22 CFIR offers a comprehensive lens to assess contextual factors, such as organizational readiness, policy environment, and stakeholder engagement, that influence implementation success. 23 To enhance contextual relevance and scalability, CFIR domains were mapped onto each phase of the EPIS process (see Table 1), enabling users to systematically consider implementation facilitators and barriers at the system, organizational, and individual levels. Additionally, the Kirkpatrick evaluation model was embedded within the tool to support outcome evaluation across 4 levels: participant satisfaction, learning, behavior change, and system-level results. 24
Mapping of CFIR domains to the EPIS process.
EPIS Framework
Each phase of the EPIS framework is functionally outlined within the tool to support sustainable, long-term professional development integrated into the organizational system. After identifying key stakeholders, the tool guides participants in completing a community needs assessment to ensure CPD developed supports practice. The preparation phase includes ensuring the education is culturally and contextually relevant, planning logistics such as identifying the venue and drafting a schedule. Identification of local and/or international expertise for providing the education is also within this phase. During the implementation phase, the CPD offering is provided with guidance on how to monitor progress and address barriers in real time as well as use feedback to improve delivery. Finally, the sustainment phase addresses integrating CPD into a consistent schedule and ensuring continued funding, leadership support, and engagement.
CFIR Framework
The CFIR assisted development of the tool to ensure guidance aligned with real-world contexts by accounting for barriers and facilitators at multiple levels: individual, organizational, and systemic. The tool guides participants to consider not only that the CPD delivered is contextually relevant but also cost-effective and easy to assess. The tool outlines the considerations in the outer setting, such as policy, accreditation requirements, or funding opportunities. Inner setting considerations include leadership support and readiness for change. Individual characteristics are also included including stakeholder motivation, skill level, and perceived value of CPD. The implementation process domain overlaps with the EPIS framework for planning, executing, and reflecting on the CPD provided.
Kirkpatrick Model
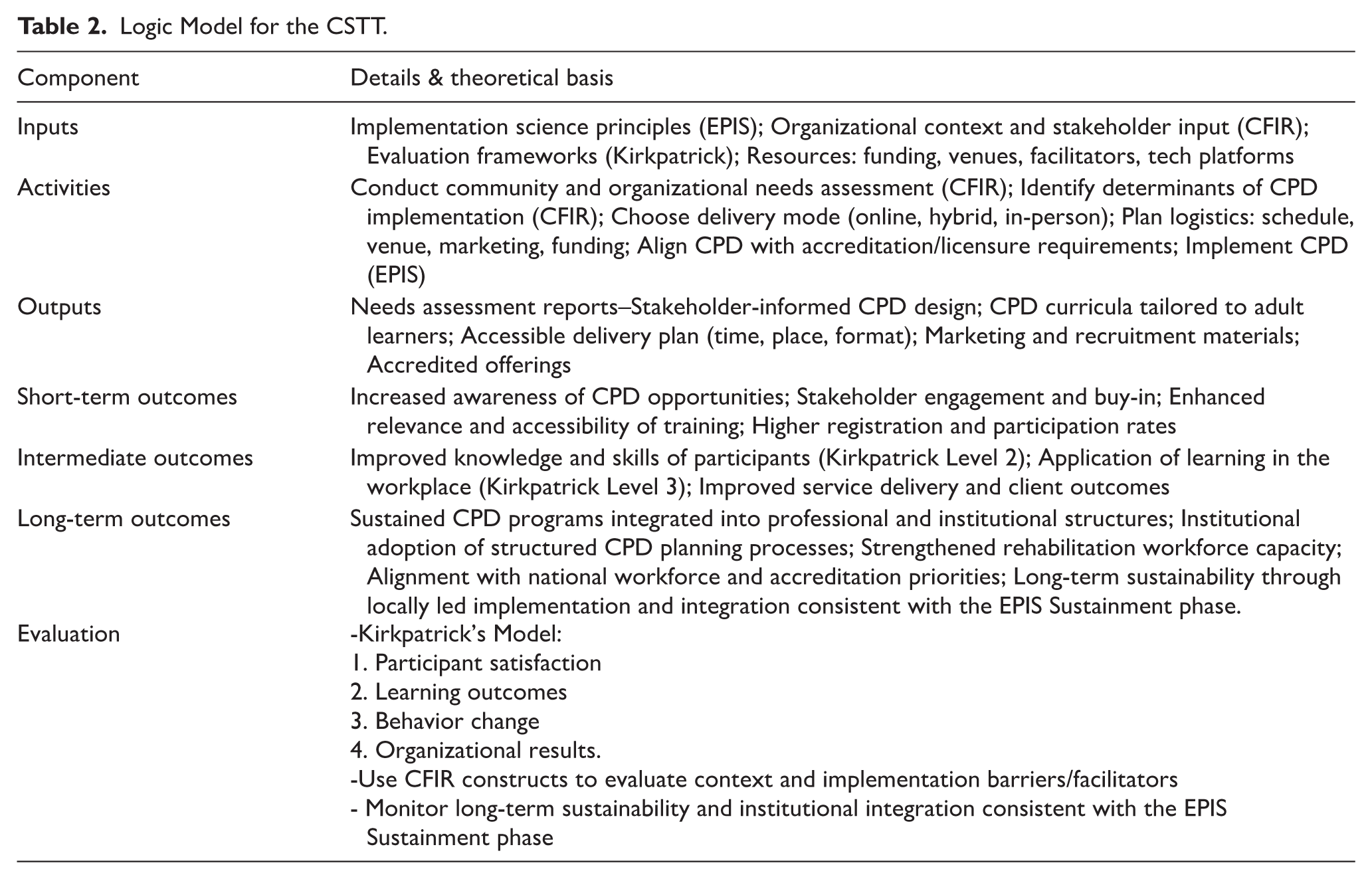
To support meaningful evaluation of CPD efforts, the tool incorporates the Kirkpatrick model, a widely used framework for assessing the effectiveness of training and professional development programs. 24 The model guides stakeholders in evaluating outcomes at 4 progressive levels: Reaction, Learning, Behavior and Results. 24 Within the tool, each level is paired with example indicators and data collection strategies to guide stakeholders in conducting structured evaluations. This helps ensure that CPD initiatives move beyond participation metrics to assess meaningful change. When used alongside the EPIS and CFIR frameworks, the Kirkpatrick model provides a comprehensive structure for stakeholders to assess both what was achieved and how contextual factors influenced CPD implementation and outcomes. Insights gathered through this model during pilot testing informed subsequent revisions of the tool to strengthen its utility and relevance across LMIC contexts. The logic model for the CSTT can be found in Table 2.
Logic Model for the CSTT.
Study Design
This study used an implementation-informed, iterative development and pilot testing approach to design and refine the CSTT. Tool development and pilot testing were conducted between 2021 and 2024 in collaboration with rehabilitation stakeholders in Myanmar, Ukraine, Uganda, and Pakistan. The study was guided by implementation science frameworks, including EPIS and CFIR, which informed both tool design and evaluation.
Participants and Stakeholder Engagement
Development of the tool was informed by iterative consultation with multidisciplinary stakeholders from 4 LMICs: Myanmar, Ukraine, Uganda, and Pakistan. Stakeholders were purposively selected based on their roles in rehabilitation workforce development and included rehabilitation clinicians, professional association representatives, educators, program implementers, and health system leaders. Stakeholders participated in workshops, tool application activities, and structured feedback sessions to inform tool refinement. Input was used to shape key components, including needs assessment templates, logistical planning guides, customizable content strategies, delivery modalities, and evaluation mechanisms.
Data Collection and Pilot Testing
Data were collected during pilot testing through structured workshops, guided discussions, mentor-facilitated planning sessions, and stakeholder reflections. Feedback focused on tool usability, clarity, feasibility, contextual relevance, and implementation challenges. Observational notes and structured feedback were documented by facilitators during each pilot phase. The tool was piloted by multidisciplinary stakeholder teams in the 4 participating countries with stakeholder teams applying it to the design of CPD initiatives. In each country, users were guided by a mentor to apply the tool to design CPD programs tailored to national rehabilitation workforce priorities. These pilot experiences generated practical feedback on usability, relevance, and clarity. Based on these findings, the tool underwent iterative revisions to improve clarity, adaptability, and real-world applicability across diverse LMIC settings.
Data Analysis
Qualitative feedback was analyzed using an iterative, framework-informed approach guided by CFIR and EPIS Frameworks. This approach is consistent with framework analysis, which allows structured examination of implementation processes using predefined theoretical constructs while remaining responsive to emergent contextual factors. Feedback from workshops, guided reflections, mentor-facilitated planning sessions, and stakeholder discussions was documented through facilitator notes and structured feedback summaries. These data were reviewed iteratively to identify key implementation facilitators, barriers, and usability considerations. Observations were categorized according to relevant CFIR domains, including intervention characteristics (eg, usability and clarity), inner setting (eg, organizational readiness), outer setting (eg, professional infrastructure), characteristics of individuals (eg, stakeholder confidence and experience), and implementation process (eg, stakeholder engagement and leadership support). Findings from this analysis informed iterative refinement of the CSTT. Refinements were implemented following each pilot phase to ensure the tool was responsive to stakeholder needs and adaptable across diverse health system contexts.
Training Needs Assessment Findings
Training needs assessments conducted in each pilot country identified specific rehabilitation priorities that informed the development and adaptation of CPD programs using the CSTT. These assessments were conducted through stakeholder consultations, workshops, and structured planning activities, and were informed by prior mixed-methods research examining CPD needs among rehabilitation professionals in low- and middle-income countries. 25 These country-specific priorities were consistent with prior findings identifying neurological rehabilitation and workforce development as key CPD priorities while reflecting contextual clinical demands in each implementation setting.
In Myanmar, stakeholders identified neurological rehabilitation as a critical priority, particularly for individuals with stroke and pediatric neurological conditions associated with long-term functional impairments. 25 Participants emphasized the need for training in comprehensive neurological assessment, treatment planning, and gait rehabilitation to address complex rehabilitation needs across the lifespan. These priorities informed the development of CSTT-supported CPD programs focused on improving competency in neurological rehabilitation assessment and intervention. In Ukraine, stakeholders identified rehabilitation related to burns, trauma, and complex injuries as a priority, reflecting the increased demand for rehabilitation services associated with war-related injuries. 25 Participants emphasized the need for training in rehabilitation assessment, functional recovery planning, and management of patients with complex wounds and associated impairments. These priorities informed CSTT-supported CPD programs focused on burns rehabilitation and management of complex injuries. In Pakistan, stakeholders identified neurological rehabilitation as a key priority, including rehabilitation for individuals with spinal cord injury and stroke. In addition to condition-specific training needs, participants emphasized the importance of interprofessional education to strengthen collaboration among rehabilitation disciplines and improve coordinated patient care. 25 These findings informed CSTT-supported CPD planning efforts focused on neurological rehabilitation and interprofessional workforce development. In Uganda, stakeholders, including professional association leaders, emphasized the need to strengthen internal capacity for CPD development. Rather than focusing solely on condition-specific clinical skills, stakeholders prioritized development of sustainable systems to support profession-specific CPD programs. This included building capacity among professional leaders to design, implement, and sustain CPD initiatives aligned with national workforce needs.
The Clinical Skills Training Tool
The tool is organized into sequential domains. It begins with stakeholder analysis and needs assessment to identify key actors, define expectations, and determine training priorities based on system and workforce needs. Subsequent sections guide users through defining learning outcomes, selecting training approaches, and developing a design that aligns with available resources, accreditation requirements, and adult learning principles. The implementation planning component assists in constructing feasible schedules, coordinating the recruitment of trainers and participants, and preparing logistical elements for both virtual and in-person training (Figure 1).
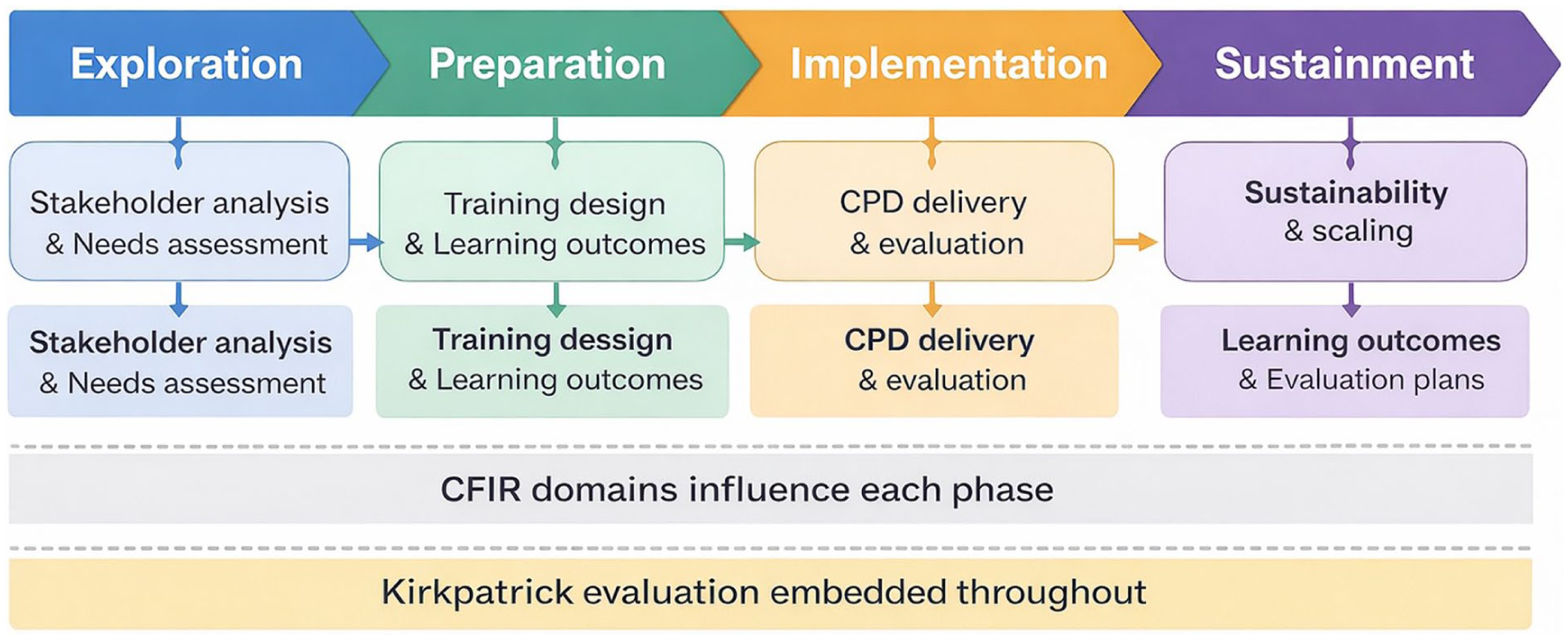
Stepwise implementation process of the Clinical Skills Training Tool (CSTT). The CSTT guides stakeholders through sequential phases of continuing professional development planning and implementation aligned with the EPIS framework. Key activities include stakeholder engagement, needs assessment, training design, implementation, evaluation using the Kirkpatrick model, and sustainability planning. Contextual factors influencing implementation are assessed using the CFIR. This structured process supports sustainable CPD development across diverse health system contexts.
Assessment and evaluation processes are guided by the Kirkpatrick model, ensuring that the outcomes identified align with both learning objectives and broader system goals. The tool includes guidance to help stakeholders identify appropriate rehabilitation-specific outcome indicators, such as functional outcome measures, clinical practice adherence, complication rates, and service delivery indicators, to support long-term evaluation of CPD impact. The final section emphasizes sustainability and accreditation, encouraging users to embed CPD programs within existing systems and to seek long-term institutional and policy support. The CSTT was designed to support both facilitated and independent use through structured worksheets, sequential planning steps, and embedded guidance, enabling scalability across settings with varying levels of CPD planning experience. Table 3 presents the final structure of the CSTT and alignment with implementation.
Structure of the CSTT and Alignment With Implementation Frameworks.
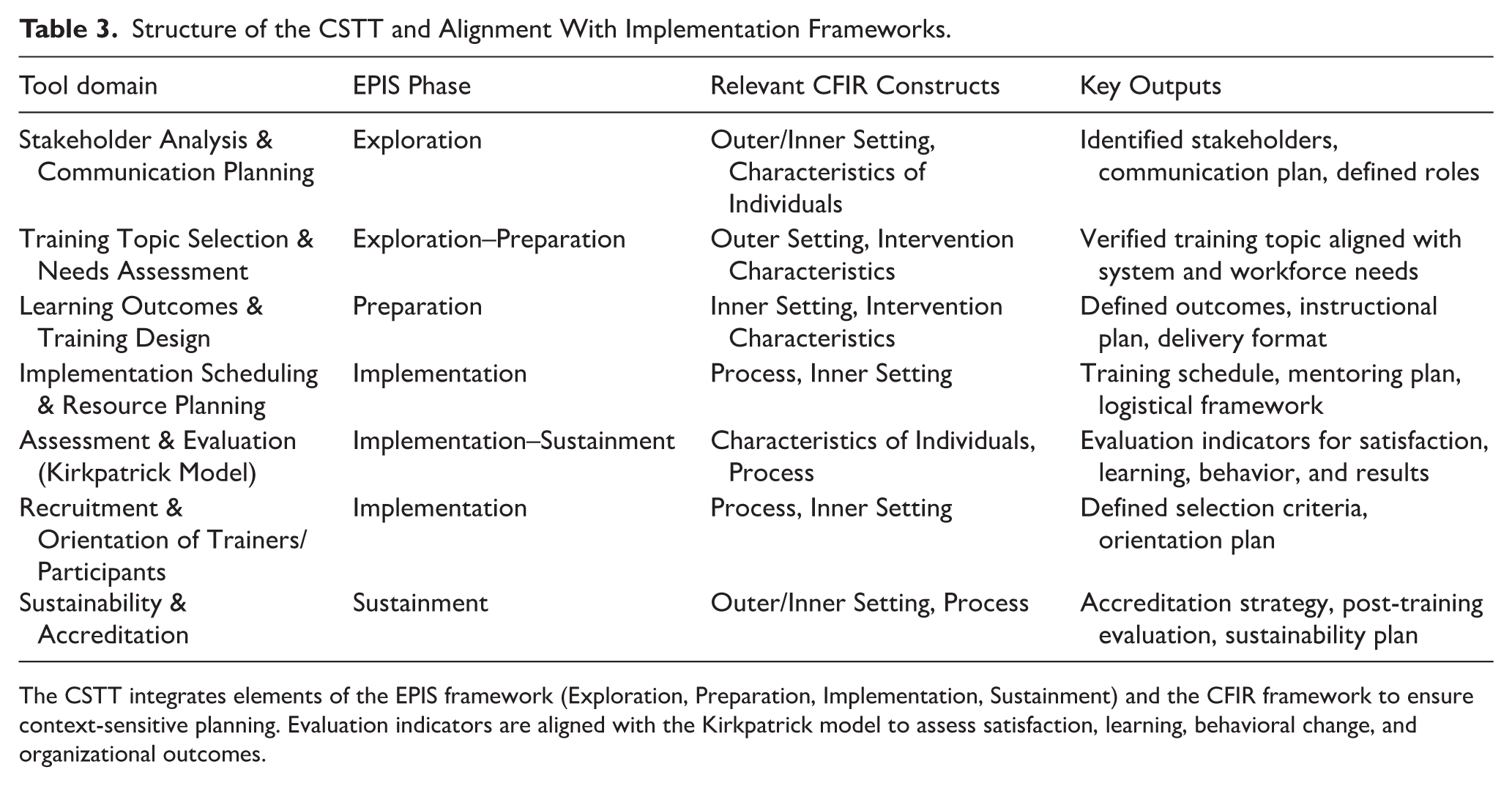
The CSTT integrates elements of the EPIS framework (Exploration, Preparation, Implementation, Sustainment) and the CFIR framework to ensure context-sensitive planning. Evaluation indicators are aligned with the Kirkpatrick model to assess satisfaction, learning, behavioral change, and organizational outcomes.
Results
Pilot Implementation Overview
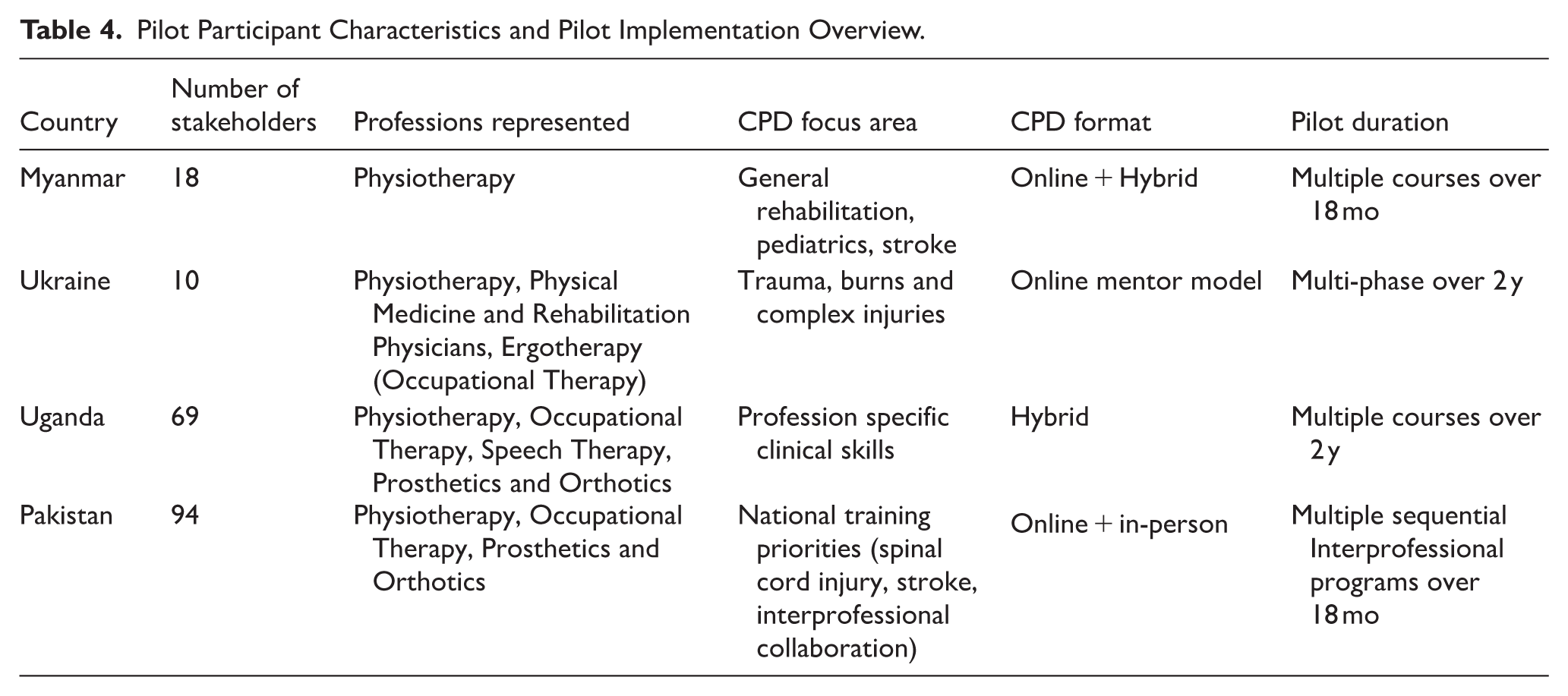
The piloting of the tool across diverse contexts provided key insights into how varying national and infrastructural conditions influenced the design and delivery of CPD programs. These experiences informed iterative refinements to enhance the tool’s flexibility, applicability, and contextual relevance. Table 4 summarizes key characteristics of pilot implementation across participating countries. Stakeholders noted that the tool’s templates, planning prompts, and clear stepwise approach facilitated ease of use and localization, making it adaptable to a variety of local contexts. This flexibility allowed stakeholders to tailor the tool to meet specific needs within their countries, ensuring relevance to national rehabilitation priorities and local conditions.
Pilot Participant Characteristics and Pilot Implementation Overview.
Pilot Outputs and Learning Outcomes
Pilot implementation of the CSTT supported the development and delivery of multiple CPD programs across participating countries, incorporating structured evaluation approaches aligned with the Kirkpatrick model. These programs included training initiatives addressing identified through stakeholder needs assessments. Evaluation methods varied by program and context but commonly included pre- and post-training surveys, competency assessments, satisfaction surveys, and follow-up evaluations to assess knowledge acquisition and clinical application. Examples of CSTT-supported CPD programs illustrate the tool’s capacity to facilitate structured evaluation of learning outcomes. In Myanmar, rehabilitation professionals participating in a stroke rehabilitation training program demonstrated statistically significant improvements in self-reported knowledge, clinical skills, and confidence following completion of the training. Structured surveys assessed domains including stroke assessment, use of standardized outcome measures such as the Functional Independence Measure (FIM), and application of evidence-based therapeutic interventions. Six-month follow-up evaluations demonstrated continued application of learned skills in clinical practice and dissemination of knowledge to colleagues.
Influence of CFIR Domains Across Implementation Phases
Analysis of pilot implementation across countries identified key CFIR domains that influenced CPD planning and tool application during each EPIS phase. During the Exploration phase, Outer Setting factors played a critical role in determining CPD priorities. National rehabilitation priorities, workforce needs, and health system demands directly influenced training topic selection. For example, in Ukraine, urgent workforce needs related to conflict-related trauma drove the selection of training topics focused on burns and complex injuries. In Pakistan, national-level training needs assessments conducted through professional associations guided CPD planning. During the Preparation phase, Inner Setting factors, including organizational readiness, leadership engagement, and professional association infrastructure, influenced the extent to which stakeholders were able to systematically plan CPD initiatives. Countries with established professional associations, such as Uganda and Pakistan, demonstrated more structured planning processes compared to settings with less formal institutional infrastructure.
During the Implementation phase, Characteristics of Individuals were particularly influential. Stakeholder confidence, prior experience with CPD planning, and the presence of local champions strongly influenced implementation success. In Myanmar, motivated clinicians and local champions played a key role in facilitating implementation despite limited formal institutional support. During the Sustainment phase, Process factors, including stakeholder engagement, mentorship, and train-the-trainer strategies, supported ongoing CPD activities. In Ukraine, training regional supervisors enabled local dissemination of knowledge and expanded workforce reach, supporting long-term sustainability.
Contextual Adaptation and Tool Flexibility
Organizational readiness for tool implementation varied significantly across countries. In settings where strong institutional support was present, such as backing from ministries of health, academic institutions, or well-established professional associations, the tool was applied more comprehensively and sustained over time. These environments facilitated the integration of the tool into ongoing CPD efforts. Differences in clinical priorities, workforce structure, institutional readiness, and available resources influenced how stakeholders applied the CSTT. For example, in Pakistan, CPD priorities were identified through a national training needs assessment survey and coordinated through professional associations. In contrast, in settings with limited leadership engagement or resources, the tool was implemented within a motivated group of rehabilitation clinicians. In Myanmar, where formal professional infrastructure was limited, CPD planning was initiated by motivated clinicians and local champions, demonstrating the tool’s applicability in both structured and emerging professional environments. Although the tool was designed to support CPD on a national scale, the CSTT was able to be implemented by a community-driven group of motivated clinicians, whose enthusiasm and engagement played a pivotal role in the success of the CPD program, despite limited external resources.
Stakeholder Engagement and Implementation Experience
The individual characteristics of stakeholders, including their confidence and prior experience with structured planning tools, influenced the depth of their engagement with the CSTT. Stakeholders with greater familiarity with structured planning processes were more likely to assume leadership roles in implementing the tool, driving forward CPD initiatives within their organizations. In countries with strong institutional support, such as Uganda and Pakistan, the CSTT was integrated into existing professional development structures, facilitating systematic CPD planning and implementation. Conversely, stakeholders with less experience or confidence in using such tools benefited from mentorship and guidance throughout the process. In Myanmar, these individuals were supported by local champions or facilitators who helped them navigate the tool’s various phases and encouraged active participation. This support enabled participants to navigate tool components, apply structured planning processes, and develop CPD programs aligned with local needs.
Tool Refinement and Usability Improvements
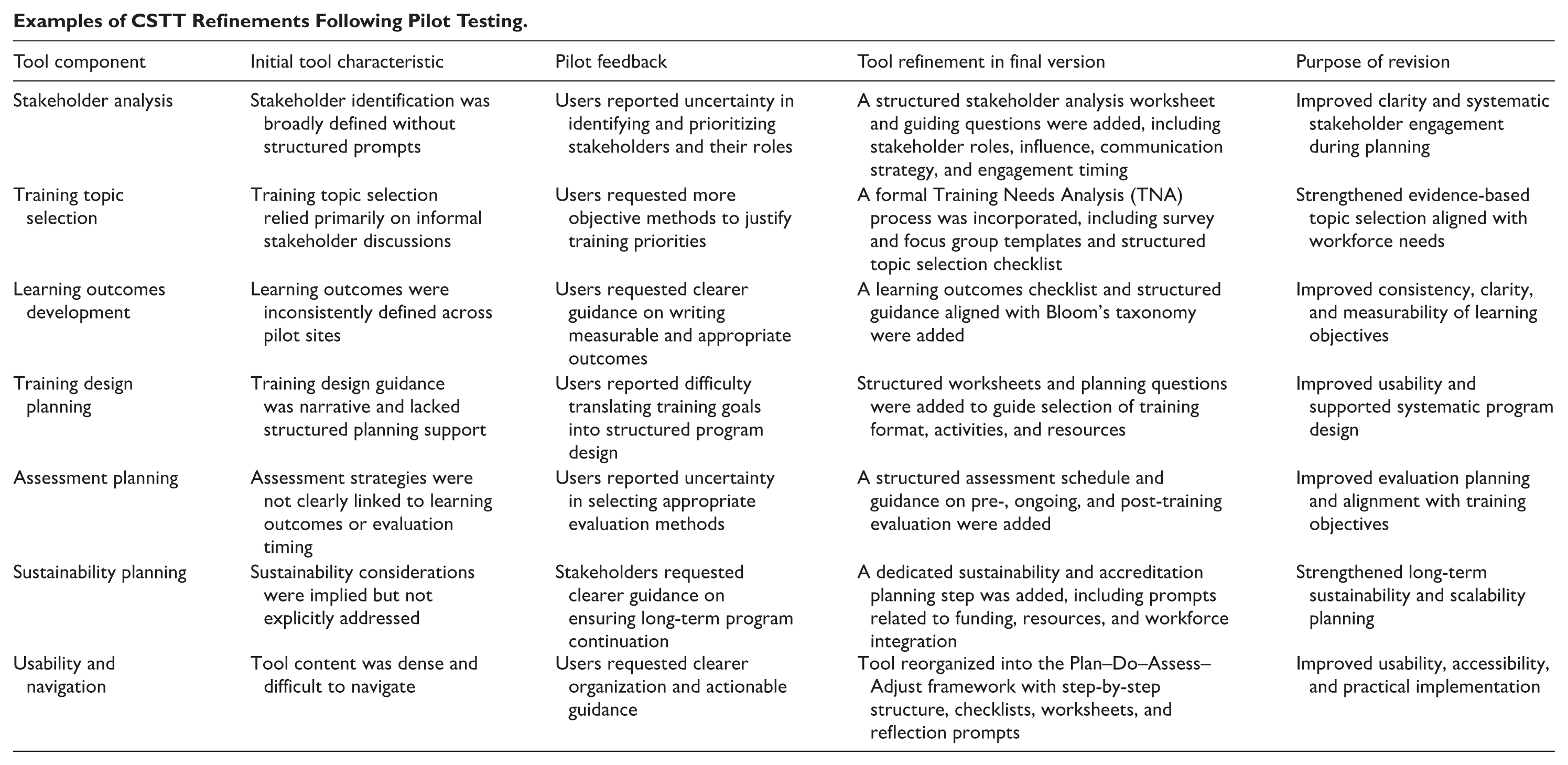
Pilot testing provided critical insights into tool usability and contextual relevance. Stakeholders reported that the CSTT’s structured, stepwise format improved clarity and facilitated systematic CPD planning. Feedback led to several refinements, including simplification of language, improved sequencing of planning steps, and enhanced guidance on sustainability planning. Stakeholders emphasized the importance of the tool’s flexibility, which allowed adaptation across diverse health system contexts, professional structures, and training delivery models. Table 5 lists CSTT refinements based on the pilot feedback. Examples of CSTT refinements following pilot testing can be found in Appendix A.
CSTT Refinements Based on Pilot Feedback.

Discussion
Principal Findings
This study describes the development and pilot testing of a theory-informed tool designed to support stakeholders in LMICs in the planning, contextualization, and evaluation of CPD for rehabilitation providers. Pilot implementation across Myanmar, Ukraine, Uganda, and Pakistan demonstrated that the CSTT provided a structured, adaptable framework that facilitated systematic CPD planning across diverse health system contexts. Stakeholders were able to apply the tool to identify workforce needs, design contextually appropriate training programs, and plan for sustainability. These findings address a previously identified gap in CPD system development in LMICs, where stakeholders often lack structured guidance for designing and sustaining professional development programs.19,21 While prior research has highlighted the importance of CPD for improving healthcare workforce capacity, practical tools to operationalize CPD planning in resource-limited settings have been limited.
Role of Implementation Science Frameworks
The integration of EPIS and CFIR provided a structured foundation that supported tool adaptability and contextual relevance. These frameworks enabled stakeholders to systematically assess implementation barriers and facilitators, including organizational readiness, leadership engagement, and workforce capacity. The EPIS framework helped users conceptualize CPD as a multi-phase process requiring sustained engagement, while CFIR provided a structured lens to assess contextual readiness and adapt plans accordingly. These features were important in settings where rehabilitation systems are still emerging and may lack standardized CPD requirements or infrastructure. Previous studies have emphasized the importance of implementation science approaches in strengthening health workforce interventions, particularly in LMICs where contextual variability significantly influences program success.22,23 The CSTT operationalizes these frameworks into a practical, stepwise tool, bridging the gap between theoretical implementation models and applied workforce development strategies. The inclusion of the Kirkpatrick model further supported a shift in thinking, from focusing solely on CPD participation rates to evaluating the quality, application, and impact of learning. However, many teams reported limited initial capacity to measure Level 3 (behavior change) and Level 4 (system-level outcomes), underscoring the need for further investment in monitoring and evaluation skills within the rehabilitation workforce.
Importance of Contextual Adaptation and Local Ownership
Pilot findings demonstrated that contextual adaptation and stakeholder engagement were critical to successful implementation. Differences in professional infrastructure, institutional support, and workforce organization influenced how the tool was applied across countries. For example, strong leadership support and existing intersectoral collaboration enabled more effective use of the tool in some countries, while in others, limited resources or lack of institutional commitment constrained implementation. Variability in stakeholders’ self-efficacy and familiarity with planning tools also influenced the depth of engagement, pointing to the need for targeted facilitation and capacity-building during initial tool deployment. These findings align with prior research showing that CPD interventions in LMICs are most effective when locally driven and adapted to national and organizational contexts.17,18 The CSTT’s modular structure, embedded prompts, and planning templates helped mitigate some of the variability in readiness, but active support from local champions and ongoing technical assistance emerged as critical success factors in all 4 countries. The presence of local champions and stakeholder ownership facilitated engagement and sustainability, reinforcing the importance of participatory approaches in implementation efforts.
Implications for Rehabilitation Workforce Development
Rehabilitation workforce shortages remain a significant barrier to achieving equitable access to rehabilitation services globally. 2 Strengthening CPD systems is essential to ensure that rehabilitation professionals maintain competency and can respond to evolving healthcare needs. The CSTT provides a structured mechanism to support rehabilitation workforce development by enabling stakeholders to design CPD programs aligned with local workforce needs and health system priorities. A well-trained, continually developing rehabilitation workforce is essential for expanding service coverage, improving quality, and addressing disparities in access to care, particularly in resource-limited settings. This approach supports global rehabilitation strengthening efforts, including WHO’s Rehabilitation 2030 initiative, which emphasizes workforce development as a key strategy for expanding rehabilitation access. 2
Supporting Structured, Sustainable CPD
Sustainability is a critical challenge in workforce development initiatives, particularly in resource-limited settings. Findings from pilot applications in Myanmar, Ukraine, Uganda, and Pakistan demonstrate that stakeholders found the tool useful for organizing CPD planning processes, aligning training with national priorities, and identifying implementation facilitators and barriers. The CSTT’s emphasis on train-the-trainer models, stakeholder ownership, alignment of national workforce strategies, and integration into existing professional associations supports long-term sustainability. These strategies are consistent with prior evidence demonstrating that locally led CPD programs are more likely to be sustained beyond initial implementation phases. 21
While evaluation of Level 3 (behavior change) and Level 4 (system-level outcomes) was beyond the scope of early pilot implementation, the CSTT incorporates structured evaluation planning to support long-term outcome measurement. In rehabilitation settings, meaningful indicators of CPD impact may include improvements in functional outcomes, such as Functional Independence Measure (FIM) scores, increased adherence to evidence-based clinical protocols, reductions in preventable complications such as pressure injuries or contractures, and improvements in service delivery metrics, including increased rehabilitation service utilization or reduced length of stay. 26 Additional indicators may include improvements in clinical documentation quality, adoption of standardized assessment tools, and expanded service availability. By encouraging stakeholders to define outcome measures during the planning phase, the CSTT supports systematic evaluation of CPD effectiveness beyond immediate training outcomes. These measures provide a mechanism to assess how professional development contributes to improvements in rehabilitation service quality and patient outcomes over time.
Implementation Fidelity and Role of Mentorship
Stakeholders with previous experience in professional education and program planning were generally able to follow the CSTT’s sequential domains independently, using the structured checklists and planning worksheets to guide CPD development. In contrast, stakeholders with less experience in CPD planning required additional clarification and benefited from mentorship and facilitated discussions to interpret tool components and align planning decisions with local contexts. Importantly, pilot implementation demonstrated that mentorship served as a capacity-building mechanism rather than a requirement for tool use. As stakeholders gained familiarity with structured CPD planning, reliance on external guidance decreased, supporting progression toward independent tool use.
Implementation science research highlights that early implementation phases often benefit from facilitation and mentorship, particularly when introducing new planning approaches or frameworks. 23 However, as users gain familiarity with implementation processes, structured tools can support sustained independent use. Pilot findings suggest that the CSTT provides sufficient structure to guide CPD planning across varying levels of stakeholder experience and organizational readiness. Furthermore, integration of the CSTT into professional associations, academic programs, and institutional training systems supports scalability without ongoing external mentorship. By embedding structured planning processes within local systems and promoting train-the-trainer approaches, the CSTT supports progressive transfer of ownership to local stakeholders and reduces long-term dependence on external support.
Implementation in Resource-Constrained and Low-Readiness Settings
While pilot implementation benefited from engaged stakeholders and local champions, variability in institutional readiness and leadership support is common in real-world settings, particularly in LMIC contexts. Implementation science research consistently identifies leadership engagement, organizational readiness, and stakeholder motivation as key determinants of successful implementation.22,23 However, the CSTT was intentionally designed to support implementation across a range of readiness levels. The structured, stepwise format of the CSTT provides guidance that can help stakeholders initiate CPD planning even in the absence of strong institutional leadership. By incorporating structured needs assessments, stakeholder mapping, and sustainability planning, the tool enables individual clinicians, professional associations, or small working groups to initiate CPD activities and build momentum for broader institutional adoption. In several pilot settings, motivated clinicians were able to use the tool to initiate CPD planning despite limited formal institutional infrastructure, demonstrating its applicability in early-stage or resource-constrained environments.
Furthermore, the CSTT’s emphasis on stakeholder engagement and train-the-trainer approaches supports gradual expansion of leadership capacity over time. This approach aligns with implementation science evidence showing that implementation efforts often begin with early adopters and expand as organizational readiness increases.22,27 By providing structured guidance and emphasizing local ownership, the CSTT supports implementation even in settings where leadership engagement is initially limited, enhancing its robustness and scalability.
Limitations and Future Directions
This study focused on tool development and early-stage application. While pilot testing provided valuable insights, further implementation and research are necessary to assess the long-term impact of the tool on the quality, consistency, and structure of CPD, as well as its influence on provider performance and client outcomes. Additionally, further adaptation may be required. Building communities of practice around the tool and expanding its use through global partnerships may further enhance its utility and scalability.
Footnotes
Appendix 1
Examples of CSTT Refinements Following Pilot Testing.
| Tool component | Initial tool characteristic | Pilot feedback | Tool refinement in final version | Purpose of revision |
|---|---|---|---|---|
| Stakeholder analysis | Stakeholder identification was broadly defined without structured prompts | Users reported uncertainty in identifying and prioritizing stakeholders and their roles | A structured stakeholder analysis worksheet and guiding questions were added, including stakeholder roles, influence, communication strategy, and engagement timing | Improved clarity and systematic stakeholder engagement during planning |
| Training topic selection | Training topic selection relied primarily on informal stakeholder discussions | Users requested more objective methods to justify training priorities | A formal Training Needs Analysis (TNA) process was incorporated, including survey and focus group templates and structured topic selection checklist | Strengthened evidence-based topic selection aligned with workforce needs |
| Learning outcomes development | Learning outcomes were inconsistently defined across pilot sites | Users requested clearer guidance on writing measurable and appropriate outcomes | A learning outcomes checklist and structured guidance aligned with Bloom’s taxonomy were added | Improved consistency, clarity, and measurability of learning objectives |
| Training design planning | Training design guidance was narrative and lacked structured planning support | Users reported difficulty translating training goals into structured program design | Structured worksheets and planning questions were added to guide selection of training format, activities, and resources | Improved usability and supported systematic program design |
| Assessment planning | Assessment strategies were not clearly linked to learning outcomes or evaluation timing | Users reported uncertainty in selecting appropriate evaluation methods | A structured assessment schedule and guidance on pre-, ongoing, and post-training evaluation were added | Improved evaluation planning and alignment with training objectives |
| Sustainability planning | Sustainability considerations were implied but not explicitly addressed | Stakeholders requested clearer guidance on ensuring long-term program continuation | A dedicated sustainability and accreditation planning step was added, including prompts related to funding, resources, and workforce integration | Strengthened long-term sustainability and scalability planning |
| Usability and navigation | Tool content was dense and difficult to navigate | Users requested clearer organization and actionable guidance | Tool reorganized into the Plan–Do–Assess–Adjust framework with step-by-step structure, checklists, worksheets, and reflection prompts | Improved usability, accessibility, and practical implementation |
Acknowledgements
We wish to thank all our colleagues for their valuable input, insightful discussions, and collaborative effort throughout the tool development. The development team included Rachael Lowe, Cheryl Footer, Larisa Hoffman, Angela Patterson, Martina Lukin, Shala Cunningham, Olha Kovalchuk, Herbert Omoding, Neelum Zehra, and Hsu Wai Mon Oo.
Ethical Considerations
This study (IRB No. 21399) was reviewed by the Johns Hopkins School of Public Health (JHSPH) Institutional review board and determined to be exempt. Informed consent and confidentiality practices were followed.
Author Contributions
ML: Conception or design of the work, Implementation of Tool, Critical revision of the article, Final approval of the version to be submitted. SC: Data collection, Data analysis and interpretation, Drafting the article, Critical revision of the article, Final approval of the version to be submitted. AP: Conception or design of the work, Implementation of Tool, Critical revision of the article, Final approval of the version to be submitted. RL: Conception or design of the work, Critical revision of the article, Final approval of the version to be submitted; Acquisition of funding
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was made possible by the support of the American people through the United States Agency for International Development (USAID) through the Learning Acting Building for Rehabilitation in Health Systems (ReLAB-HS) project (7200AA20CA00033). The contents are the sole responsibility of ReLAB-HS and do not necessarily reflect the views of USAID or the United States Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.