
Abstract
Background:
As populations age, rehabilitation needs are increasing sharply. Older people experience declining intrinsic capacity, multimorbidity, and environmental barriers, which intensify their reliance on rehabilitation to optimize and maintain functional ability. Despite its critical role in healthy ageing, access to rehabilitation remains limited across the WHO European Region (WHO EURO).
Aim:
To examine the availability, implementation, and challenges of rehabilitation service delivery for older people in WHO EURO from the perspectives of rehabilitation stakeholders.
Design and Methods:
We conducted a secondary mixed-methods analysis of a 2023/2024 global online survey called “Rehabilitation Service Delivery to Foster Healthy Ageing,” initially designed to identify and validate global rehabilitation delivery models, focusing on WHO EURO data. The survey, offered in 8 languages, targeted health and care workers providing rehabilitation for people aged 60 and above. Quantitative and qualitative data were analysed descriptively, thematically, and integrated using the Health System Dynamics Framework. Reporting followed CROSS and MMR-RHS guidelines.
Results:
706 responses from 45 countries were analysed. Six validated rehabilitation delivery models were confirmed: outpatient, inpatient, home, telerehabilitation, community, and residential long-term care. Findings revealed disparities in the availability of these models and in the responsiveness – assessed through a self-designed responsiveness index – of rehabilitation services to ageing populations, varying by country and income level. Strengthening outpatient, home, and residential long-term rehabilitation was considered most urgently needed. Barriers and facilitators to strengthening rehabilitation were identified across all domains of the Health System Dynamics Framework and synthesized into 8 themes and 19 subthemes.
Discussion:
Rehabilitation models remain unevenly implemented across Europe, and inequities in provision persist. Systemic barriers span governance, financing, human resources, and service delivery, underlining the importance of integrated approaches that reflect older people’s realities and priorities.
Conclusion:
Rehabilitation plays a key role not only after illness or injury but also in maintaining functional ability during age-related declines in intrinsic capacity. Strengthening rehabilitation for older people is essential for Healthy Ageing and requires investment, intersectoral collaboration, and implementation science to overcome systemic barriers.
Keywords
Introduction
Rehabilitation needs in the World Health Organization European Region (WHO EURO) are increasing rapidly as the population ages. In 2021, an estimated 394 million people, equivalent to 2 in 5 individuals, in WHO EURO had a health condition requiring rehabilitation, highlighting the need for strong and responsive rehabilitation services. 1 Globally, these rehabilitation needs have increased by almost 80% since 1990, mainly due to population growth and ageing. 2 In Europe, demographic trends indicate that by 2050, over 30% of the population in many countries will be aged 60 or older. 3 As a result, this shift is already putting significant pressure on health systems and is expected to greatly increase the demand for rehabilitation services tailored to older peoples’ needs 4 and capable of supporting healthy ageing for all.
Understanding the multifaceted rehabilitation needs of ageing populations is essential. The WHO and the United Nations (UN) define healthy ageing as the process of developing and maintaining functional ability, which depends on intrinsic capacity, the environments in which people live, and how individuals interact with those environments. 5 The ageing process is associated with a gradual decline in intrinsic capacity, often accompanied by the emergence of complex health states that typically appear later in life and do not fit neatly into specific disease categories, such as geriatric syndromes. 6 Older people are also more likely to experience multiple, often chronic, health conditions simultaneously, commonly referred to as multimorbidity.7 -10 In Europe, this trend is especially pronounced, with more than 60% of individuals aged 65 and over living with 2 or more chronic conditions. 11 These health challenges are further compounded by environmental barriers, such as inaccessible housing, inadequate transport systems, and societal ageism, which can significantly limit functional ability and increase reliance on care. Indeed, older people are particularly vulnerable to such hindering environments,5,12 and the WHO Baseline Report for the Decade of Healthy Ageing highlights how these environmental factors contribute to persistent inequalities in ageing outcomes across the region. 5 When combined with increased susceptibility to severe infectious diseases like COVID-19, 13 increased risk of injury, especially falls,14 -16 and a higher incidence of mental disorders, especially depression and anxiety, 17 these overlapping vulnerabilities underscore the essential role of rehabilitation in preserving independence and functional ability in later life.
Rehabilitation is a key health strategy for achieving healthy ageing. Rehabilitation plays a vital role in achieving healthy ageing and has been widely recognized as a key person-centred health strategy,18 -20 rehabilitation supports the process of healthy ageing as defined by the Decade 5 by optimizing functioning and reducing disability in people with health conditions in interaction with their environment. 21 This directly contributes to improving or stabilizing both intrinsic capacity and functional ability. Building and strengthening intrinsic capacity and, in turn, functional ability, is a cornerstone of rehabilitation. While rehabilitation has often been viewed primarily as a remedial service delivered after injury, illness, or the onset of chronic conditions, it has an equally vital role as a health strategy that supports preventive measures, such as “prehabilitation” to maintain health, slow functional decline, and support healthy ageing. Recognizing and investing in this health strategy could help reduce the future burden on health and care systems. The WHO World Report on Ageing and Health emphasizes that rehabilitation can reduce disability and dependency, prevent avoidable hospitalizations, and improve ageing trajectories. 6 Its recent inclusion in the updated WHO Integrated Care for Older People (ICOPE) guidelines further underlines the growing recognition of rehabilitation as an important element of ageing-related care. 22
However, gaps in accessing rehabilitation in the WHO European Region persist. Despite its benefits, access to rehabilitation remains limited across many parts of WHO EURO. 1 Inadequate access increases the risk of social exclusion, poverty, and greater dependence on long-term care, while also leading to avoidable complications and functional decline. 23 Insufficient access is driven by factors such as service underprovision, workforce limitations, and unequal geographic distribution24,25 and, in some cases, ageism that results in older persons being deprioritized or excluded from needed health and care services. 26 To address these challenges, the World Health Assembly (WHA) adopted a landmark resolution on strengthening rehabilitation in health systems, urging countries to integrate rehabilitation at all levels of care, particularly in response to the growing needs of ageing populations. 27 Improving the availability, accessibility, and responsiveness of rehabilitation services is therefore not only a clinical priority but also a social and policy imperative for individuals, families, and societies at large.
Recent studies have identified and described service delivery models for the rehabilitation of older people, including Outpatient, Inpatient, Telerehabilitation, as well as rehabilitation delivered at Home, in Residential Long-term Care (previously referred to as “Eldercare”), and at the Community. These models have been initially defined in scoping reviews, including mostly studies conducted in high-income countries (HICs)18,19,28 and subsequently validated from the perspective of rehabilitation professionals with hands-on experience working in countries of all income levels, through an international stakeholder consultation. 29 This consultation highlighted differences in the availability and implementation status of the rehabilitation models, revealing that all of them, regardless of the world region or income level, still require either implementation or further strengthening. 29 However, this global study neither reported on region-specific barriers and facilitators for implementing or further strengthening rehabilitation models nor provided details about the current state of rehabilitation provision for older people in WHO EURO. Therefore, this secondary mixed-methods study of the international stakeholder consultation 29 has the objectives of (a) expanding knowledge about rehabilitation service delivery models for the ageing population in the countries belonging to WHO EURO and (b) identifying barriers and facilitators to their implementation or further strengthening in WHO EURO. These findings aim to support rehabilitation stakeholders and policymakers in (re)designing services that promote healthy ageing in WHO EURO.
Material and Methods
This work was carried out as part of the work plan of the WHO Collaborating Center for Rehabilitation in Global Health Systems hosted by the University of Lucerne in Switzerland.
Study Design
This is a secondary mixed-methods analysis of the 2023/2024 global cross-sectional survey “Rehabilitation Service Delivery to Foster Healthy Ageing”, originally designed to identify and validate global rehabilitation delivery models. 29 The present analysis focuses on WHO EURO responses and adds region-specific quantitative and qualitative analyses. The quantitative part gathered data on the characteristics of rehabilitation models, availability, and implementation status. Given the lack of prior evidence to inform a predefined list of potential determinants, the qualitative strand included open-ended questions, inviting respondents to describe perceived barriers and facilitators for implementing rehabilitation models. Both datasets were analysed independently, and integration occurred during the interpretation phase. The protocol was registered on the OSF platform prior to data generation (https://doi.org/10.17605/OSF.IO/Z4EKD). We adhered to the Consensus-based Checklist for Reporting of Survey Studies (CROSS) 30 and the Mixed Methods Reporting in Rehabilitation & Health Sciences (MMR-RHS) to guide the reporting, 31 see Supplemental File I.
Participants
Participant eligibility criteria were the same as in the global survey, with analysis focused on WHO EURO member states and related languages. Participants were eligible if they: (a) were healthcare workers currently involved in the provision of rehabilitation services or working with older people at various levels, including the individual (eg, rehabilitation worker) and the organizational level (eg, manager, coordinator) in countries that are member states of WHO EURO, which includes central Asia and Israel, (b) had at least 2 years of experience, or indicated a value of at least 30 in the self-rated expertise question from 0 to 100, in their respective fields, ensuring adequate knowledge and understanding of rehabilitation services provided to older people, (c) were proficient in at least one of the WHO EURO official languages (English, French, Russian) and other languages (Spanish, Portuguese, German), d) were willing and able to give informed consent, and (e) were older than 18 years. Participants who only viewed the first page (less than 4% progress) were automatically excluded. Participants who answered only demographic and professional background questions progressing less than 40% of the survey were also excluded from the analysis. In a previous publication, we showed there was no selection bias related to this issue. 29
Questionnaire Development, Content and Structure
The survey, originally developed as part of a global study on rehabilitation service delivery, 29 was structured using information on rehabilitation service delivery models identified was structured using information on rehabilitation service delivery models identified.18,19 It included an introductory module, covering demographic information and professional background, along with 2 content modules. The first one assessed the characteristics of rehabilitation service delivery models. The second addressed the availability of models in different regions of the world, implementation needs, and barriers and facilitators to implementation. Availability refers to the current presence of a rehabilitation service model within a country, whereas implementation status captures respondents’ perception of the population coverage and the need for new implementation or further strengthening of that model beyond current availability. In total, the survey consisted of 33 questions, including multiple-choice questions with Likert scales, sliding metric scales from 0 to 100, and open-ended questions. Further details on the survey development process can be found elsewhere, 29 the complete survey is available as Supplemental File II.
Sample and Data Collection
Relevant stakeholders were identified using a combined purposive and snowball sampling and a 2-layer strategy. The first layer focuses on the roles involved in rehabilitation provision, including direct (eg, rehabilitation workers delivering interventions) and indirect (eg, managers, coordinators of services) roles. The second layer examines various professional groups, including traditional rehabilitation workers (eg, physical therapists – PTs), generalist healthcare providers (eg, general practitioners – GPs), professionals serving the ageing population (eg, geriatricians), and other professionals (eg, social workers). A rule of thumb was utilized to determine the number of participants per group or category of interest, as suggested by Sim et al. 32 Based on previous findings, we allocated a higher number of representatives to the healthcare workers most frequently involved in the rehabilitation of older people. The a priori calculated sample size for WHO EURO was 44 respondents. The survey was distributed via email after stakeholders mapping and the social media platform LinkedIn® as an “open survey” (ie, open to any visitor to a website). Data were collected from August 10, 2023, to February 20, 2024. The survey was administered using Qualtrics and no incentives were offered for participation. Further details are available elsewhere. 29
Data Analysis
Quantitative Analysis
Results were summarized using descriptive statistics: median and quartiles (Q1, Q3) for metrical variables (sliders), due to skewed response distributions, and absolute numbers and proportions for categorical variables. Countries were classified by income level according to their gross national income (GNI) as reported by the World Bank in 2022 33 and grouped into 2 categories: High-Income countries (HICs), and Middle-Income countries (MICs). Missing responses were possible for all questions except informed consent. Questionnaires with missing responses were included in the analysis, and the number of missing values reported for all questions. A summary rehabilitation responsiveness index was calculated to assess the extent to which rehabilitation services were responsive to the needs of older people. The index was computed by averaging responses to key rehabilitation characteristics: person-centeredness, use of multidisciplinary teams, goal-oriented planning, provision of assistive technologies (AT), environmental adaptations, psychological interventions, and service integration. All questions ranged from 0 to 100, except for the item on prescription of environmental adaptations, which was standardized to a 0 to 100 scale before averaging. See questionnaire in Supplemental File II.
Qualitative Analysis
Responses provided on the barriers and facilitators to implementing or strengthening rehabilitation were analysed through an inductive thematic analysis, utilizing MAXQDA Analytics Pro software and following methods. 34 Two researchers (VS and JY) independently coded a subset of 80 responses to ensure consistency and reliability. After this calibration phase, one researcher (JY) continued coding the remaining responses. Any coding discrepancies were resolved through discussion until a consensus was reached. Initial codes were generated inductively from the data and later refined through iterative team discussions as new patterns and meanings emerged. Codes were then organized into higher-order themes, which were mapped onto the domains of the Health System Dynamics Framework (HSDF). 35 In comparison to the WHO Health System Building Blocks, the HSDF comprises 10 components (eg, Service Delivery, Human Resources) and their interactions, providing a more comprehensive analytical view of a health system by highlighting interconnections between health system components, the influence of values, and multi-level interactions, 36 facilitating understanding of community, societal, and policy macro-dynamics. The first-level codes aligned with the HSDF components (eg, service delivery, governance, financing), while second-level codes were defined either from existing literature or, when unavailable, developed de novo by the research team. Reflexivity and the maintenance of an audit trail were employed to enhance analytical rigour. 34
Data Integration and Triangulation
We used the HSDF as the guiding integrative framework for triangulation. For each HSDF component, we compared the relevant descriptive statistics with the corresponding qualitative themes. The aim was to identify points of convergence, where both data types mutually confirmed a finding, and complementarity, where the qualitative data provided context or explanation for the quantitative results. This integrated analysis formed the basis for the overall assessment of the health system dynamics influencing rehabilitation provision for older people in the WHO EURO.
Ethical Considerations
We received formal confirmation from the Ethics Committee of Northwestern and Central Switzerland (EKNZ) that ethical approval was not necessary because no personal data were collected from participants beyond general demographic information. Additionally, as the consultation aimed solely to elicit expert opinions and feedback, without involving any intervention or evaluation of a specific approach, ethical oversight was deemed unwarranted. The survey was anonymous, and data were stored securely on password-protected servers to prevent unauthorized access.
Data Availability
The analysed data is available from the corresponding author on reasonable request.
Results
Of the 1302 valid responses included in the original global survey, 706 (54%) were from WHO EURO, with 81% (n = 578) from HICs and 19% (n = 128) from MICs (see Figure 1 for flowchart). Among all participants, 329 (47%) answered at least 1 question about barriers and facilitators. Respondents came from 45 countries: 44 WHO EURO member states and 1 additional response from Kosovo. The highest number of responses came from Portugal (n = 180, 25%), followed by Kyrgyzstan (n = 74, 10%), Switzerland and Spain (each with n = 60, 8.5%), Germany (n = 46, 6.5%), and the United Kingdom (n = 41, 5.8%) (Supplemental Figure S3). We exceeded the planned sample size and met the a priori quotas (Supplemental Table S4). Most participants were female (n = 493, 70%), nurses (n = 254, 36%), physical and rehabilitation medicine (PRM) doctors (n = 153, 22%), and physical therapists (PTs) (n = 108, 15%), with a clinical role (n = 598, 85%) and more than 10 years of experience (n = 498, 71%). No large differences were observed between HICs and MICs, except for self-rated expertise (0 “no experience” to 100 “expert”) in delivering rehabilitation, with a median of 77 (IQR = 61, 88) in HICs versus a median of 38 (IQR = 15, 71) in MICs (Table 1).
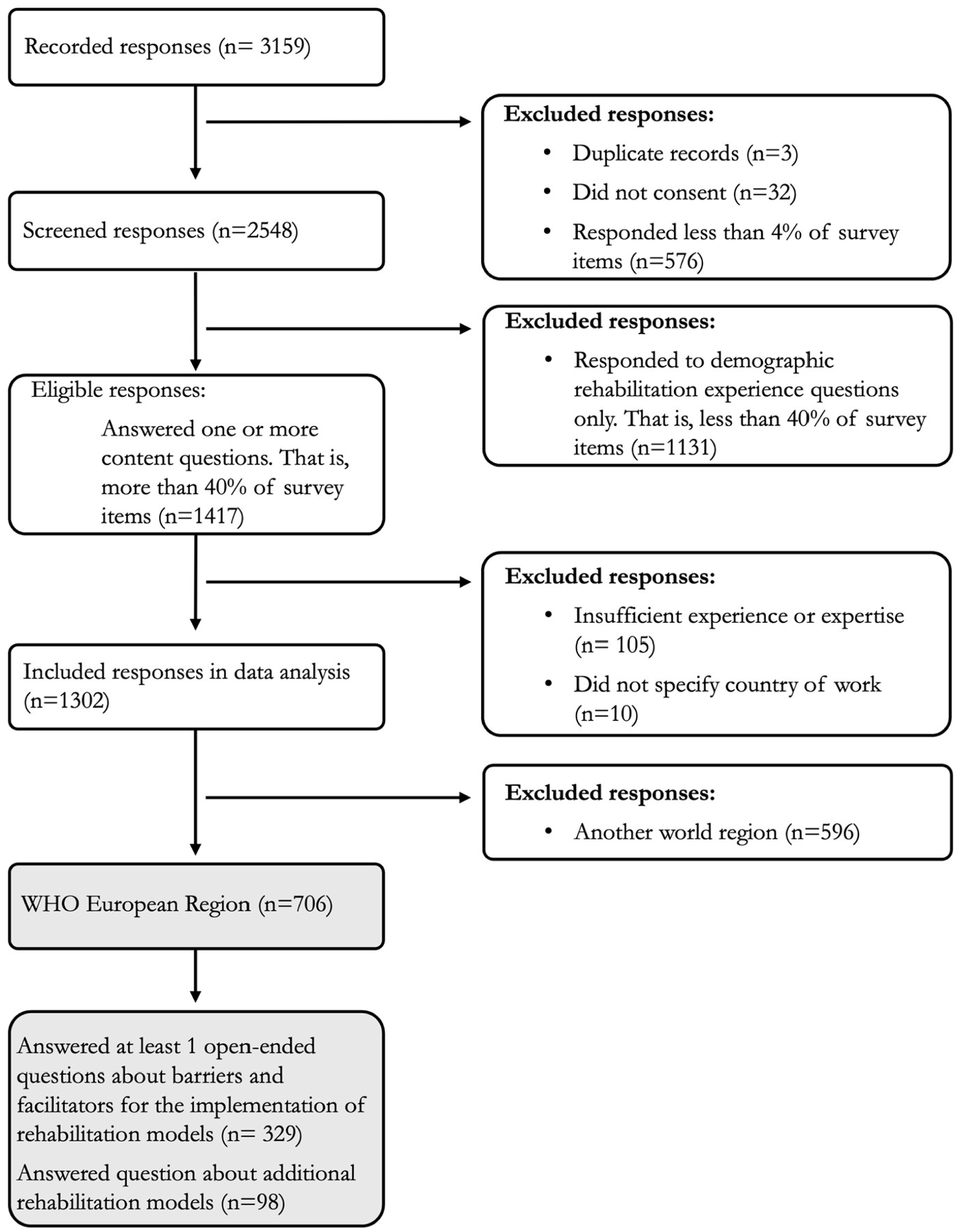
Study participant flowchart.
Participant Characteristics Overall and by Income Group.

Abbreviations: HICs, high income countries; MICs, lower middle and upper middle-income countries; PRM, physical and rehabilitation medicine doctors.
Rehabilitation Delivery Models in WHO European Region
When asked about additional rehabilitation delivery models to those identified in previous scoping research (Outpatient, Inpatient, Home, Telerehabilitation, Community, and Residential Long-term Care),18,19 15% of participants suggested other models. Responses referred to additional characteristics of the already identified models, such as the timing of rehabilitation (eg, prehabilitation, acute rehabilitation, long-term rehabilitation) or the source of rehabilitation (eg, family, volunteers, peers, self-provision), but no new models were brought up. Furthermore, additional settings for rehabilitation provision, including the workplace, correctional institutions, palliative care hospitals, spas, and AT service providers, were reported.
Table 2 presents the characteristics of rehabilitation models by country income group. Differences are observed in the use of multidisciplinary teams, with 88 (IQR 70, 100) in HICs compared to 55 (IQR 25, 75) in MICs in inpatient settings. Moreover, the assessment of person-centred goals, which considers not only health needs, but also the values and preferences of the individual, a key task of rehabilitation, 37 is more prevalent in all models in HICs than in MICs. Figure 2 and Supplemental Figure S5 illustrate the current responsiveness of rehabilitation services to the needs of older people by country using the rehabilitation responsiveness index. Switzerland, Germany, and the Netherlands achieved the highest scores in the responsiveness index, and Uzbekistan, Kyrgyzstan, and Greece the lowest. Table 3 outlines the most common health and care workers and target conditions associated with each rehabilitation model. PTs were the most common providers across all models, except for the Home model, where nurses were more frequently involved. Rehabilitation for musculoskeletal conditions is most often addressed within the Outpatient, Community, and Residential Long-term Care models, whereas neurological conditions are mostly addressed in the Inpatient and Home models. Most participants indicated either that they were unaware of the conditions targeted in the Telerehabilitation model or that the model was not yet available in their country.
Rehabilitation Characteristics by Model of Service Delivery and Income Level.
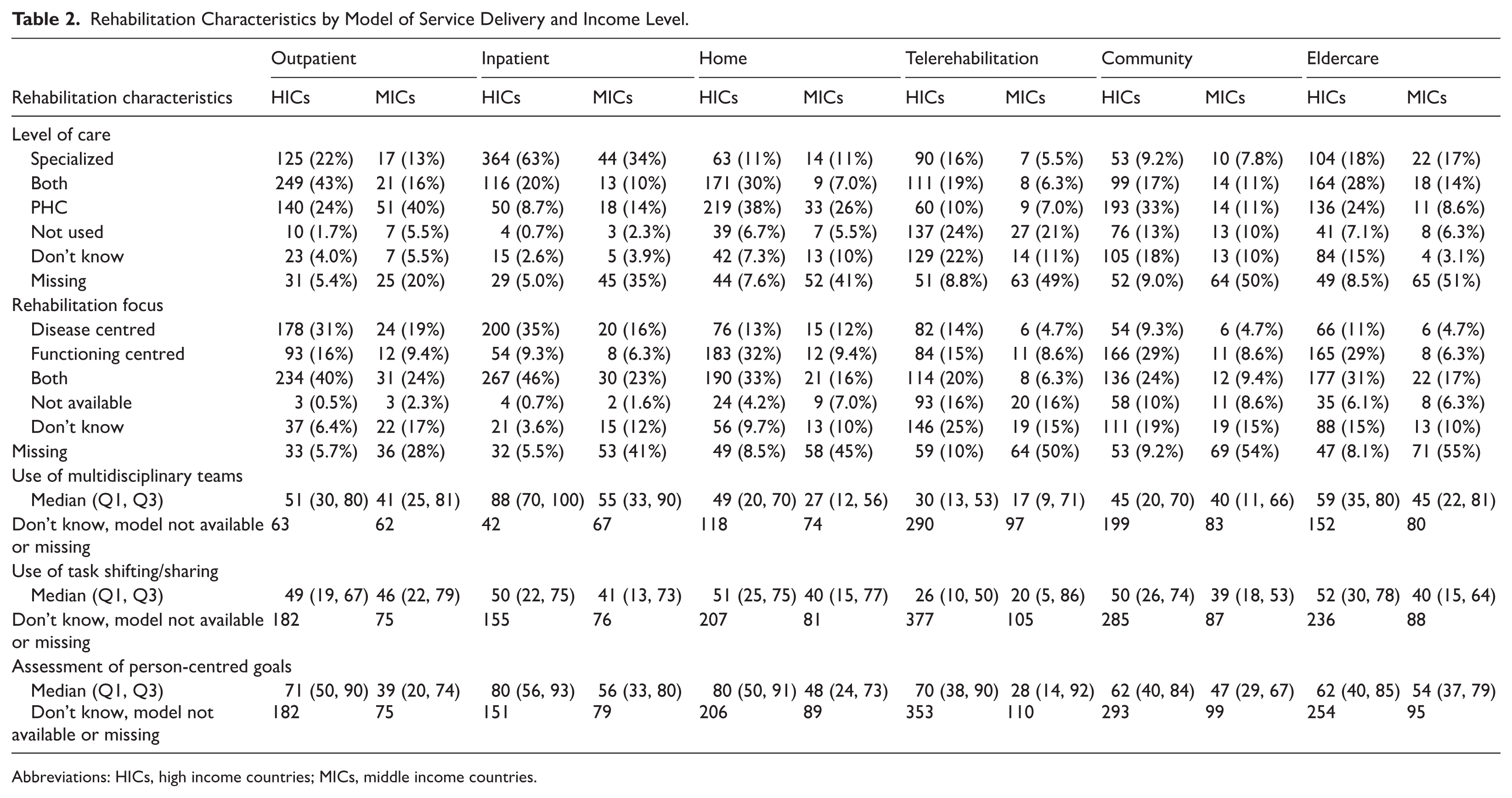
Abbreviations: HICs, high income countries; MICs, middle income countries.

Responsiveness of rehabilitation services to the needs of older people by country (responses/participants). Countries with less than 10 participants are not shown.
Rehabilitation Providers and Target Health Condition by Rehabilitation Services Delivery Models.

Abbreviations: HICs, high income countries; MICs, lower middle and upper middle-income countries; PRMs, physical and rehabilitation medicine doctors.
The 6 most often selected health workers and conditions are reported and ordered according to their overall frequency.
Availability of Rehabilitation Delivery Models and Implementation Needs in the WHO European Region
Figure 3 displays a heat map of availability and Figure 4 illustrates the implementation status of rehabilitation models by country. Telerehabilitation and Community models are the least available models. In Uzbekistan, all models, including Outpatient and Inpatient, have been reported to have low availability. All models were reported as requiring implementation or strengthening, but the lowest priorities appear to be Inpatient and Telerehabilitation, while the greatest need surrounds the Outpatient, Residential Long-Term Care, and Home models. Supplemental Table S6 presents the availability and implementation status of models by country income category.

Availability of rehabilitation models to people over the age of 60 by country.

Implementation status by country.
Barriers and Facilitators to Implementing or Strengthening Rehabilitation Models in the WHO European Region
Among the 329 responses to the barriers and facilitators questions, most came from Portugal (n = 95, 29%), the United Kingdom (n = 29, 9%), Switzerland (n = 26, 8%), Spain (n = 25, 8%), and Germany (n = 23, 7%). We identified 8 themes and 19 subthemes within the HSDF domains (Table 4). Barriers were identified across all domains of the health system. Within Context, participants described adverse social determinants of health, including financial insecurity, low pensions, and poor living conditions, as factors that limit individuals’ ability to access rehabilitation services. A broader lack of societal interest in financing or prioritizing rehabilitation for older people also emerged. In terms of Goals and Outcomes, age-based discrimination in accessing rehabilitation services was reported. Under Population, caregivers were reported as lacking the resources and support to provide sustained care, and low health literacy among both older persons and families was reported as a reason for reduced service uptake. At the Leadership and Governance level, weak health system design, outdated care models, and limited accountability mechanisms were highlighted, along with insufficient stakeholder involvement and restrictive occupational regulations that limit task-sharing. Barriers in Financing included systemic underfunding and rigid or fragmented financing mechanisms, such as separate health and social care budgets. In Human Resources, the workforce was described as insufficient, poorly retained, and undervalued, with gaps in training and limited awareness or understanding of rehabilitation among professionals. In Service Delivery, fragmentation, poor coordination, and a lack of integrated, person-centred models were recurrent, alongside poor service quality due to limited time and capacity. Finally, geographical inaccessibility and a lack of adapted infrastructure, technologies, and supplies, especially in rural areas, limit effective rehabilitation provision.
Facilitators were likewise identified across all HSDF domains. Under Context, some participants observed growing societal awareness of older persons’ needs and the role of rehabilitation. In terms of Goals and Outcomes, countries where access to rehabilitation was not restricted by age were viewed positively. Under Population, the presence of knowledgeable caregivers and increased health literacy among families were enablers of continuity of care. In Leadership and Governance, facilitators included health policy reforms, improved planning tools, strong professional networks, advocacy, and co-creation with key stakeholders. Effective accountability mechanisms and the expansion of occupational roles also supported implementation. Facilitators in Financing included the availability of national health insurance, investment in human resources, and policy willingness to support service development despite constraints. Within Human Resources, training programmes, continued professional development, and efforts to improve recognition and retention were emphasized. Respondents also noted a cultural shift towards valuing rehabilitation as a key health service to improve functioning in older age. In Service Delivery, emerging models of integrated and person-centred rehabilitation, shared decision-making, and team-based care were described. Lastly, facilitators related to Infrastructure and Supplies included investments in telerehabilitation, adapted equipment, and the implementation of Community models.
Thematic Analysis of the Barriers and Facilitators to Implementing or Strengthening Rehabilitation Delivery Models to Foster Healthy Ageing in the WHO European Region.
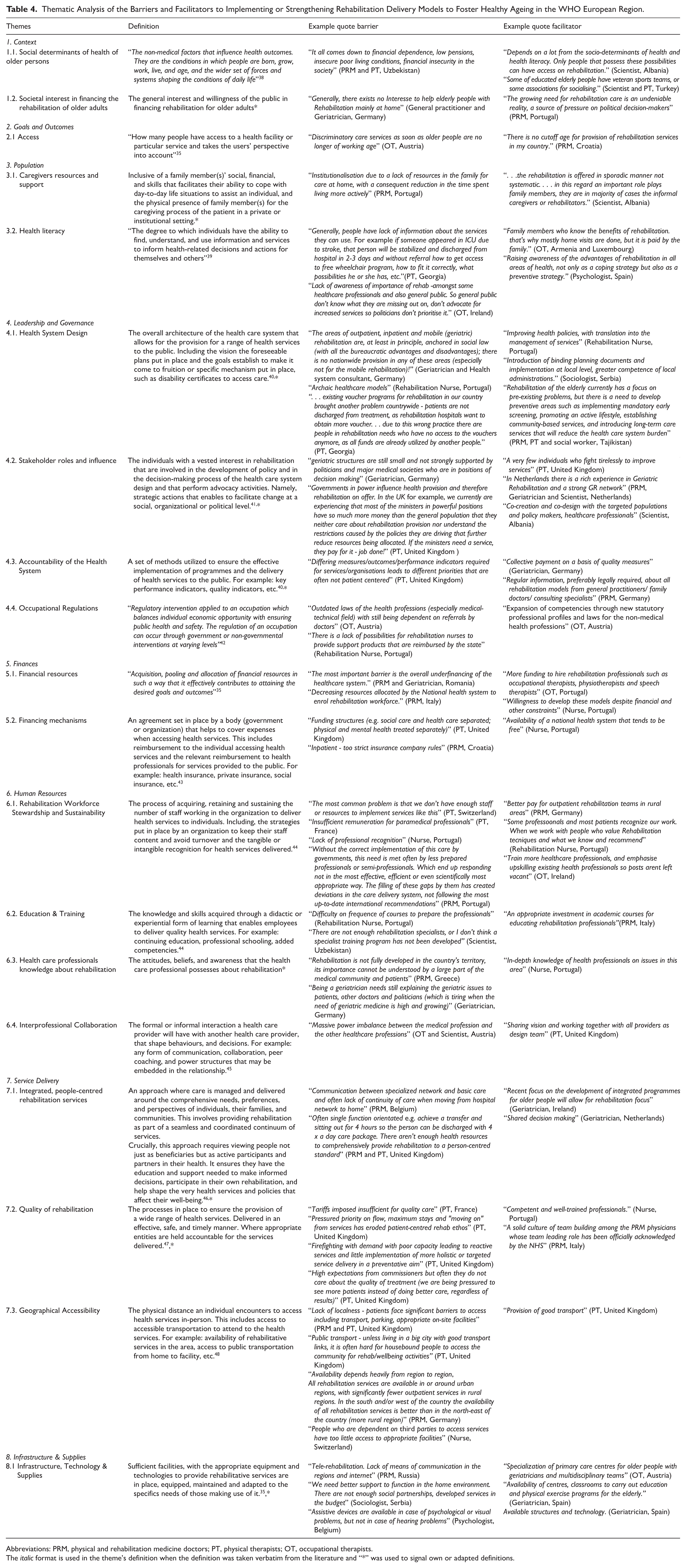
Abbreviations: PRM, physical and rehabilitation medicine doctors; PT, physical therapists; OT, occupational therapists.
The italic format is used in the theme’s definition when the definition was taken verbatim from the literature and “*” was used to signal own or adapted definitions.
Health System Dynamics for Rehabilitation in the WHO European Region
Figure 5 condenses the gathered evidence about health system barriers influencing rehabilitation for older people in WHO EURO using the HSDF framework. The summary highlights that within a Context of demographic ageing, which creates pressures like increased service utilization, higher dependency levels, and financial insecurity and varying societal interest in financing rehabilitation for older people, rehabilitation-related Outcomes and Goals for older persons are still suboptimal. Interconnected systemic barriers drive these outcomes and goals. Primarily, structural issues in Leadership and Governance, such as service fragmentation and restrictive occupational regulations, combined with significant constraints in mainly financial and Human Resources, hinder the provision of appropriate, comprehensive, and integrated rehabilitation Service Delivery. This cycle is further perpetuated by factors at the Population level, including inadequate health literacy about rehabilitation and limited patient and caregiver resources, which reinforce the challenges within the system.

Health system dynamics for rehabilitation provision to older adults in the WHO European Region.
Discussion
This study provides one of the most comprehensive overviews to date of the state of rehabilitation services for older people in WHO EURO. Based on responses from 706 healthcare professionals across 47 countries, we confirmed that previously identified models of rehabilitation service delivery (Outpatient, Inpatient, Home, Telerehabilitation, Community, and Residential Long-term Care) 18 can be used to describe the state of rehabilitation services in WHO EURO. Our findings reveal significant differences in the availability, implementation, and response of rehabilitation services to meet the changing needs of ageing populations across countries. These findings reflect healthcare professionals’ perceptions of service availability and implementation rather than audit-based or population-level data, and should be interpreted accordingly. Telerehabilitation and Community models were the least available, but all models require some level of implementation or strengthening, with the greatest needs in Outpatient, Residential Long-term Care, and Home models. In WHO EURO, rehabilitation for musculoskeletal conditions mainly occurs within the Outpatient, Community, and Residential Long-term Care models, while neurological conditions are primarily managed through Inpatient and Home models. PTs were the most common providers of rehabilitation across all models except for the Home model, where nurses were predominant. Switzerland, Germany, and the Netherlands scored highest in the responsiveness index of rehabilitation services to the needs of ageing populations, whereas Uzbekistan, Kyrgyzstan, and Greece scored the lowest. Additionally, barriers and facilitators to strengthening rehabilitation models were identified and described across all domains of the HSDF in 8 themes and 19 subthemes. We found that, within a Context of demographic ageing and varying societal interest in funding rehabilitation for older people, the Outcomes and Goals of ageing populations remain suboptimal. Systemic barriers are interconnected and influence these outcomes and goals. Key structural issues in Leadership and Governance, such as service fragmentation and restrictive occupational regulations, along with major limitations in Financial and Human Resources, hinder the delivery of appropriate, comprehensive, and integrated rehabilitation services. Our results highlight both the urgency and opportunity to invest in and innovate within rehabilitation systems for ageing populations across WHO, emphasizing potential targets for evidence-informed public health measures and policy reforms.
Rehabilitation models are unevenly implemented in the WHO European Region and leave the ageing population frequently underserved. Our study reveals persistent inequities in the delivery of rehabilitation. Respondents from MICs reported the lowest implementation rates for nearly all models, confirming prior findings on the weak integration of rehabilitation in these contexts.49,50 This aligns with the rationale behind the recent WHA Resolution on Strengthening Rehabilitation in Health Systems 27 and the UN Decade of Healthy Ageing Plan of Action. 51 However, our findings also show that significant gaps persist in HICs. This is in line, for instance, with a recent national survey in Switzerland reporting concerning unmet rehabilitation needs among older people. 52 Outpatient and inpatient rehabilitation were the most widely available models, consistent with earlier evidence. 49 In contrast, telerehabilitation and community delivered rehabilitation, despite their potential to enhance access and continuity of care of older people, particularly in primary health care (PHC) settings, remain the least implemented. This echoes findings from WHO on access to rehabilitation in PHC and the WHA Resolution, 23 and is corroborated by recent qualitative research on the drivers of rehabilitation implementation.49,53
Key characteristics of rehabilitation services must be met to deliver services that adequately respond to the needs of the ageing population. We therefore condensed 6 core characteristics of rehabilitation services, person-centredness, the use of multidisciplinary teams, goal-oriented planning, the provision of AT, environmental adaptations and psychological interventions as well as service integration – into a rehabilitation responsiveness index to enable cross-country comparison. This study specific index revealed marked differences in service response across the region. Higher scores were observed in HICs such as Switzerland, the Netherlands, and Germany, where services were reported to integrate person-centred approaches and multidisciplinary teams. In contrast, MICs such as Uzbekistan or Kyrgyzstan scored lower, often lacking person-centred goal setting. These disparities are consistent with evidence suggesting that AT are frequently siloed from rehabilitation services, 54 that person-centred care is less common in disease-oriented models, 55 and that workforce development in geriatrics remains insufficient in many settings. 56 To our knowledge, this is the first study to propose and apply such an index. As a pragmatic measure, it offers policymakers a tool to assess and track the extent to which rehabilitation systems respond to older people’s needs changes over time, and to identify targets for interventions. Importantly, rehabilitation is not only beneficial when a health condition like stroke or chronic pulmonary disease is present or after injuries like falls but also plays a key role when older individuals experience health-related declines in their intrinsic capacity, even in the absence of a specific disease. In such cases, rehabilitation takes on a preventive character, helping to restore and maintain optimal levels of intrinsic capacity and functional ability, and thereby preventing or delaying the onset of health conditions, an aspect that remains widely underestimated.
The reporting of system-level barriers provides insights into why rehabilitation is still weakly integrated in most health systems of the WHO European Region. Our health systems analysis uncovered common and interrelated barriers across governance, financing, service delivery, and workforce domains, aligning with previously reported global challenges.29,53 Fragmentation of services limited public funding, and insufficient training of rehabilitation professionals in geriatric care were among the most frequently mentioned obstacles, collectively hindering the integration of rehabilitation into European health systems. Health systems are composed of 6 interdependent building blocks – governance, financing, workforce, health information, service delivery, and access to medicines and AT – and increasingly understood as complex adaptive systems. 57 This means that health systems tend to self-organize, adapt, and evolve over time, and that any changes introduced may trigger both intended and unintended changes. The complexity of the integration of rehabilitation in health systems was mirrored in the interwoven barriers reported by study participants, so that the introduction of isolated changes, for instance, increasing workforce capacity without addressing financing or governance, are unlikely to yield sustainable improvements. Instead, system-level interventions grounded in a “systems thinking” perspective are needed to create meaningful and lasting change in European health systems. Our results also indicate that older people may face age-based discrimination in accessing rehabilitation, with some respondents reporting they were deprioritized for services. Low health literacy among older persons and families, along with limited caregiver resources, further reduced service uptake. Tackling these inequities will require removing age-based barriers, integrating equity goals into rehabilitation policies, and strengthening outreach and caregiver support. Furthermore, country-specific strategies are essential. Tailored approaches can address context-sensitive barriers and build on existing strengths. The WHO Rehabilitation in Health Systems: Guide for Action 58 provides a structured and evidence-informed process for developing such national rehabilitation strategies, and several countries in our sample indicated that they have already begun using this tool to formulate national rehabilitation plans. In addition, countries can leverage platforms such as the WHO European Healthy Cities Network and the Global Network for Age-friendly Cities and Communities to support the development and implementation of context-sensitive rehabilitation strategies.
In line with current efforts to promote healthy ageing, strengthening the provision of rehabilitation through PHC is key to improve the intrinsic capacity and functional ability of the ageing population. One of the most prominent frameworks for improving the health of the ageing population is the ICOPE approach. 22 ICOPE is WHO’s approach to provide a continuum of integrated care that helps to reorient health and social services towards more person-centred and coordinated care for older people. While the first edition of ICOPE, 59 released in 2017, did not include rehabilitation, its recently published revised edition 22 broadly acknowledges its importance for healthy ageing and devotes an entire chapter to rehabilitation. This highlights rehabilitation’s relevance but leaves open the question of how best to deliver it in PHC settings for older people. A currently prominent WHO product is the “Basic Package of Interventions for Rehabilitation” (Basic PIR), a toolkit developed specifically for integrating rehabilitation in PHC settings 60 but not specifically developed for the older population. Our study contributes to the discussion on how to deliver rehabilitation through PHC by showing, for instance, that telerehabilitation remains a rarely available delivery mode, ranked lowest in implementation priority, despite demonstrated effectiveness. 61 Barriers identified, such as inadequate digital infrastructure,62 -64 limited provider training,65 -67 and unclear reimbursement mechanisms65,68 confirm existing evidence and illustrate persistent challenges. Complementing ICOPE, WHO EURO has also initiated the regional strategy “Ageing is living: promoting a lifetime of health and well-being (2026–2030),” 69 which seeks to build more inclusive societies and health systems for older people across the European Region. Together, these frameworks emphasize the central role of integrated, person-centred rehabilitation to support intrinsic capacity and functional ability throughout later life. Our findings point to a significant gap between effective rehabilitation models, their translation into policy and practice, and the linkage of rehabilitation and healthy ageing agendas. This underscores the need for implementation science approaches in rehabilitation, such as Learning Health Systems (LHS), 70 which can support the uptake of effective interventions through evidence-informed, adaptive policy development. Indeed, a current capacity building project is ongoing in Armenia with the aim to enable the use of the LHS approach to foster evidence-based rehabilitation for healthy ageing (see project 1947 in Ref. 71 ).
Limitations and Strengths
The use of self-reported survey data may introduce bias, including social desirability and subjective interpretation of questions. Although responses were received from 45 countries, some countries were underrepresented, which may limit the generalizability of the findings. All findings on service availability, implementation, and response are based on expert self-report rather than audited facility or population-level data and therefore reflect perceived service characteristics. Furthermore, the perspectives captured were limited to healthcare professionals. Views from other relevant stakeholders, such as patients and policy makers, were not included. Nonetheless, the study also presents notable strengths. It constitutes one of the most comprehensive regional assessments of rehabilitation service provision for older people within the WHO EURO to date. The large, diverse sample exceeded recruitment quotas defined a priori and included respondents in representative numbers from both HICs and MICs. The use of a rigorous mixed-methods design and the HSDF framework facilitated a comprehensive, system-level analysis, enhancing the validity and relevance of the findings for informing policy and service design.
Conclusion
Rehabilitation is already being delivered to older people across the WHO European Region and holds strong potential to advance the goals of the UN Decade of Healthy Ageing. Its role goes beyond recovery after illness or injury: rehabilitation can also help prevent or slow age-related declines in intrinsic capacity, supporting older people to maintain optimal functional ability and independence.
Yet, rehabilitation services remain fragmented, with major disparities in access and responsiveness to the complex needs of ageing populations. To address these gaps, rehabilitation must receive greater priority in the Healthy Ageing agenda and in national and regional policy frameworks. Recognizing its preventive value is key to building systems that not only respond to current needs but also slow down future declines in intrinsic capacity and functional ability.
Strategic investment and health system strengthening are urgently needed. Implementation science can help develop context-sensitive implementation strategies that facilitate the uptake of evidence into practice and support the development of integrated, person-centred, and age-inclusive models of care. Ensuring access to responsive rehabilitation services across Europe is essential to achieving health equity and enabling older people to maintain optimal levels of functional ability and independence throughout later life.
Supplemental Material
sj-docx-3-rpo-10.1177_27536351261419007 – Supplemental material for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries
Supplemental material, sj-docx-3-rpo-10.1177_27536351261419007 for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries by Vanessa Seijas, Roxanne Maritz, Julia Yee, Beatriz Moreira, Clara Lussi, Andreas Limacher, Yongjie Yon, Shirin Kiani, Tomas Zapata and Carla Sabariego in Advances in Rehabilitation Science and Practice
Supplemental Material
sj-docx-4-rpo-10.1177_27536351261419007 – Supplemental material for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries
Supplemental material, sj-docx-4-rpo-10.1177_27536351261419007 for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries by Vanessa Seijas, Roxanne Maritz, Julia Yee, Beatriz Moreira, Clara Lussi, Andreas Limacher, Yongjie Yon, Shirin Kiani, Tomas Zapata and Carla Sabariego in Advances in Rehabilitation Science and Practice
Supplemental Material
sj-docx-5-rpo-10.1177_27536351261419007 – Supplemental material for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries
Supplemental material, sj-docx-5-rpo-10.1177_27536351261419007 for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries by Vanessa Seijas, Roxanne Maritz, Julia Yee, Beatriz Moreira, Clara Lussi, Andreas Limacher, Yongjie Yon, Shirin Kiani, Tomas Zapata and Carla Sabariego in Advances in Rehabilitation Science and Practice
Supplemental Material
sj-docx-6-rpo-10.1177_27536351261419007 – Supplemental material for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries
Supplemental material, sj-docx-6-rpo-10.1177_27536351261419007 for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries by Vanessa Seijas, Roxanne Maritz, Julia Yee, Beatriz Moreira, Clara Lussi, Andreas Limacher, Yongjie Yon, Shirin Kiani, Tomas Zapata and Carla Sabariego in Advances in Rehabilitation Science and Practice
Supplemental Material
sj-pdf-1-rpo-10.1177_27536351261419007 – Supplemental material for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries
Supplemental material, sj-pdf-1-rpo-10.1177_27536351261419007 for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries by Vanessa Seijas, Roxanne Maritz, Julia Yee, Beatriz Moreira, Clara Lussi, Andreas Limacher, Yongjie Yon, Shirin Kiani, Tomas Zapata and Carla Sabariego in Advances in Rehabilitation Science and Practice
Supplemental Material
sj-pdf-2-rpo-10.1177_27536351261419007 – Supplemental material for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries
Supplemental material, sj-pdf-2-rpo-10.1177_27536351261419007 for Rehabilitation Service Delivery Models to Foster Healthy Ageing in the WHO European Region: Results From a Cross-Sectional Stakeholder Consultation Involving 45 Countries by Vanessa Seijas, Roxanne Maritz, Julia Yee, Beatriz Moreira, Clara Lussi, Andreas Limacher, Yongjie Yon, Shirin Kiani, Tomas Zapata and Carla Sabariego in Advances in Rehabilitation Science and Practice
Footnotes
Acknowledgements
The authors are grateful to Barbara Machado for her assistance in preparing the research protocol and implementing the survey in Qualtrics, and to Nasya Patiyasevi for support in disseminating the survey. Special thanks go to Denis Zelko (Russian) and Shamyr Castro (Portuguese) for translating the questionnaire, and to Anna Romanova (Russian) for translating the responses.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this work was received from the Velux Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.