
Abstract
Purpose:
The COVID-19 pandemic disrupted in-person healthcare and accelerated the adoption of telemedicine, for which most low- and middle-income countries were unprepared. This study describes the population, service delivery, and therapeutic outcomes of telerehabilitation in Cali, Colombia, during the pandemic, and identifies factors influencing its feasibility to guide future implementation in similar low-resource settings.
Methods:
We conducted a retrospective cohort study using medical records from 2 rehabilitation centers in Cali, Colombia, including patients who received synchronous telerehabilitation between January 2020 and December 2021. Data on demographics, diagnoses (grouped as mental health, neurological, chronic, post-traumatic, or unspecified), and outcomes (recovery, dropout, continued care) were collected using a structured form and analyzed with descriptive statistics and non-parametric tests (Wilcoxon, Kruskal-Wallis, chi-square, or Fisher’s exact), with significance set at p < .05.
Results:
We analyzed 1572 patients receiving telerehabilitation. Most were women (65.4%), aged 36 to 64 (46.5%), with trauma sequelae (32.8%) and mental health conditions (26.3%) as common diagnoses. Main services were physiatry (32%), psychosocial therapy (29%), and physiotherapy (27%). Most sessions were by phone (67.5%) and completed successfully (90%). Recovery was reported in 6.4% of cases; 13.3% completed treatment, 72.3% required ongoing care, and 3% dropped out. Completion was more common in older patients (p < .05).
Conclusions:
The COVID-19 pandemic underscored telerehabilitation’s vital role in Latin America, revealing access gaps and the need for further research to address socioeconomic, educational, and digital barriers affecting vulnerable populations. The patterns of telerehabilitation utilization varied notably by age, sex, and diagnosis, highlighting the necessity of strengthening and adapting these services to improve health outcomes and ensure equitable access. Gaps remain in areas of telerehabilitation such as, mental health, cardiovascular diseases and ophthalmology, underscoring the need for broader implementation and integration across specialties.
Introduction
The outbreak of the COVID-19 pandemic in 2020 led to precautionary measures in Latin America and the world, including enforced lockdowns, to mitigate the spread of the virus and prioritize healthcare resources for critical cases. 1 Instead of in-person care, the countries were compelled to adopt and scale emergency measures to meet the population’s growing healthcare and rehabilitation needs. One of those measures was telemedicine, which already existed but had limited distribution. 2
Telerehabilitation, a branch of telemedicine within the field of physical medicine and rehabilitation, refers to the remote delivery of rehabilitation services. It encompasses a broad range of tools and protocols aimed at managing, intervening, monitoring, supervising, educating, and guiding individuals throughout the therapeutic process, all facilitated through information and communication technologies (ICTs). 3 Such services experienced substantial expansion across Latin America during the pandemic. Nations like Brazil, Chile, Perú, and Colombia have endeavored to boost telehealth utilization and ease regulatory constraints to meet population demands, directly toward supporting the healthcare requirements of both COVID-19 patients and those seeking routine primary care. 4
Colombia implemented several governmental measures, including the suspension of elective procedures and surgeries, the cancellation of non-essential healthcare services, and the development of virtual healthcare consultation pathways to ensure continued access to care while minimizing infection risks. 1 However, one of the most adversely affected services was rehabilitation, impacting individuals with disabilities or those requiring ongoing therapeutic interventions.5,6 People with disabilities are particularly vulnerable to health and socioeconomic disparities, 7 which further heightened their susceptibility to the negative consequences of the pandemic. 8
Challenges in implementing telerehabilitation include regulatory barriers, infrastructural deficiencies, workforce limitations, sustainability issues, and cultural factors.9 -11 Despite these obstacles, the COVID-19 pandemic accelerated its adoption and highlighted the urgent need for the formal integration of telemedicine-based healthcare services.5,6,12 However, comprehensive knowledge regarding telerehabilitation practices during lockdowns and public health emergencies remains limited, and evidence on the utilization and outcomes of such services is still scarce. 13
Given the limited research on telerehabilitation in low- and middle-income countries (LMICs) during the COVID-19 pandemic, 14 this study aims to address this gap by analyzing the implementation of telerehabilitation services in Cali, Colombia; a major urban center in a middle-income Latin American country. Through this investigation, the aim of this study is to establish the outcomes of the telerehabilitation programs and evaluate their limitations, strengths, and potential areas for improvement, with a view to informing future implementation in similar settings and among comparable populations in LMIC.
Methods
Study Design
This is a retrospective non-concurrent cohort study to investigate the utilization and outcomes of telerehabilitation services at 2 centers in southwestern Colombia, Fundación Ideal and Cosmitet, based on patients seen from January 1st, 2020 to December 31, 2021. Historical data were extracted from electronic medical records using a structured Qualtrics™ form. The study evaluated patient characteristics, intervention effectiveness, and satisfaction with synchronous telemedicine-based rehabilitation across a diverse population.
Setting
This study was carried out at 2 healthcare institutions in southwestern Colombia—Fundación Ideal® and Cosmitet—both of which operate established telemedicine and telerehabilitation programs. These centers connect rehabilitation professionals with individuals with disabilities and their families through digital platforms such as Zoom™, google meet™, and WhatsApp ™, video calls and communication technologies through mail and chat. Fundación Ideal® and Cosmitet provide rehabilitation services to approximately 37 000 and 78 000 patients annually, respectively.15,16
Participants
The cohort consisted of patients who received telerehabilitation services from January 1, 2020, to December 31, 2021. Eligibility criteria were broad, with no restrictions based on age, sex, or diagnosis. All patients whose consultations or therapeutic sessions were conducted via remote communication technologies during the study period were included. These sessions adhered to synchronous telemedicine principles, enabling real-time interactions between patients and healthcare providers. 17 Eligible communication modalities encompassed various digital platforms, such as video conferencing, telephone calls, live chat, and virtual call systems. Through these channels, a range of therapeutic services was delivered, including physical therapy, speech therapy, psychotherapy, supervised exercise sessions, and occupational therapy, depending on the individual patient’s condition and clinical needs. Patient records were excluded if labeled as teleconsultations solely for scheduling purposes without any associated therapeutic intervention.
Data Collection/Measurement
Data were extracted retrospectively using a predesigned Qualtrics™ form that incorporated quality control features—such as validation rules, value limits, and predefined multiple-choice options—to minimize entry errors and ensure data accuracy. Trained personnel were responsible for data collection under the supervision of one of the researchers (SGP). The data search focused on patients with conditions requiring rehabilitation, grouped into key clinical categories. Musculoskeletal and trauma-related disorders included polytrauma, traumatic brain injury, fractures, amputations, chronic pain, and rheumatic diseases. Neurological disorders encompassed cerebral palsy, stroke, Parkinson’s disease, epilepsy, and conditions of genetic, infectious, or toxic origin. Mental health conditions such as depression, anxiety, schizophrenia, PTSD, and developmental disorders with behavioral impact were also included. Additionally, the search covered patients with cancer-related impairments—particularly those undergoing or recovering from treatment—and individuals with respiratory conditions like COPD, post-COVID-19 sequelae, and pulmonary fibrosis. This broad inclusion reflects the diversity and complexity of patients served by the telerehabilitation programs. Only patients who were receiving services offered by the participating clinics and who remained actively enrolled in follow-up during the study period were included in the analysis. Data were accessed for research between August 15, 2021 and December 31, 2021. Authors had access only to information relevant to the study that could not identify individual participants.
Variables
Sociodemographic, clinical, and implementation-related variables were collected. Diagnoses were grouped into non-communicable chronic diseases (coronary heart disease, stroke, cancer, diabetes, and chronic pulmonary diseases), neurological diseases (primary and secondary of genetic, infectious, or toxic origin, resulting in sequelae in the central and peripheral nervous system), posttraumatic conditions (associated with externally caused injuries such as traumatic brain injury and spinal cord injury, and musculoskeletal conditions), mental health disorders, and unspecified diagnoses in the medical records.
The therapeutic outcome variable was categorized into several groups: treatment abandonment (reported by the therapist after 3 or more missed sessions or inability to re-establish contact with the patients or their caregivers/family), treatment completion (full completion of the prescribed treatment regimen), recovery (reported by the therapist when the therapeutic goals of the ongoing intervention are met), and requiring further treatment (patients who are undergoing ongoing or have upcoming authorized sessions for continued care, mainly in the chronical conditions). Variables such as consultation duration and pain-related reasons were not uniformly recorded in the electronic records and were only available for a subset of patients. This variability was due to non-mandatory fields in the clinical documentation systems used at the participating institutions.
Study Size and Sampling
Initially, billing codes for telerehabilitation services were identified to generate a list of patients who received care from 2020 to 2021. We estimated a sample size of 1345 based on a hypothetical telerehabilitation usage proportion of 46%, 18 a 5% margin of error, and a 95% confidence level (z = 1.96). From a total of 9161 eligible cases, 1911 records were randomly selected balanced by sex and type of service—namely physiatry, speech therapy, physiotherapy, occupational therapy, and psychosocial therapy—from 2 participating centers. After applying the inclusion criteria, 339 records were excluded, resulting in a final sample of 1572 patients. The final sample exceeded our estimate and allowed for adequate characterization of users and services provided. Supplementary Figure S1 shows the Participant Flow Diagram.
Bias
Selection and information biases were minimized through the random selection of participants and cross-validation of medical record data by 2 independent investigators (SGP and DSC) who reviewed the data separately and then compared their findings to identify and resolve any discrepancies or errors. Furthermore, data collection personnel received specific training, and a random verification of 10% of the extracted data was performed to ensure accuracy and consistency.
Analysis
The data were exported from Qualtrics™ to Stata 16 (STATA Corp., TX, US)® for analysis. Initial exploratory analysis was conducted to assess missing and extreme values and we double checked these outcomes.
A bivariate analysis was performed using measures of central tendency and dispersion. Categorical variables were analyzed using frequency distributions and percentages, and chi-square or Fisher’s exact tests were used to test for hypotheses. For continuous variables, the distribution’s normality was assessed using the Shapiro-Wilk test. As the variables were found to be not normally distributed, we used Wilcoxon and Kruskal-Wallis tests for hypotheses testing. Statistically significant differences were defined as a p-value < .05.
Ethical Aspects
The study obtained ethical approval from the ethics committees of the participating centers and the Institutional Review Board of the Universidad del Valle, under the declaration of Helsinki with approval document No. 014-021 on 13 August 2021. Written consent was obtained prior to the first session of each consult.
Results
Population Characteristics
A total of 1572 patients who received telerehabilitation services during the study period were included in the analysis. Participants were drawn from 2 institutions, with 822 (52.29%) and 750 (47.71%) patients sampled from each center, respectively. An increase in teleconsultations was observed during periods of mandatory lockdown. The first period occurred between late March and August 2020, and the second occurred between October 2020 and February 2021 (Figure 1). Additionally, there was an increase in teleconsultations from April to July 2021 during confinement due to civil unrest and social protests. Patients utilizing telerehabilitation services were predominantly women (1028; 65.40%), with a female-to-male ratio of approximately 2:1. The mean age of the cohort was 50 ± 20 years. Women were slightly older than men, with a median age of 54 years (IQR: 37.5-67) compared to 51 years for men (IQR: 30-65), a difference that was statistically significant (p < .001) (Table 1).

Telerehabilitation consultation trends during 2020-2021 in Cali, Colombia.
Social and clinical characteristics of patients using telerehabilitation services during the COVID-19 pandemic in 2020-2021, Cali, Colombia.

Abbreviations: IQR, interquartile range p25-p75; NCD: non-communicable diseases.
Chi-square test.
Wilcoxon test.
Most patients were between 36 and 64 years of age (46.50%), followed by those aged over 65 years (27.54%). In the 0 to 17 years group, the majority of patients were male, whereas in the 36 to 64 years group, consultations were predominantly from female patients (11.40% vs 3.50%; 49% vs 40.91%, respectively; p < .001).
Male patients were predominantly treated for neurological conditions and traumatic injuries or their sequelae (17.69% and 36.92%, respectively). In contrast, teleconsultations for mental health conditions were more prevalent among female patients (30.32% vs 18.46%; p < .001). The mean age varied by clinical condition, being higher among patients with chronic diseases and lower among those treated for mental health conditions and neurological disorders (chronic diseases: n = 171, mean = 60 ± 20 years; neurological disorders: n = 181, mean = 38 ± 28 years; traumatic injury sequelae: n = 497, mean = 54 ± 16 years; mental health: n = 398, mean = 43 ± 18 years; Kruskal-Wallis test; p < .001; Figure 2). The primary reason for consultation was the continuation of ongoing treatment (62.73%).
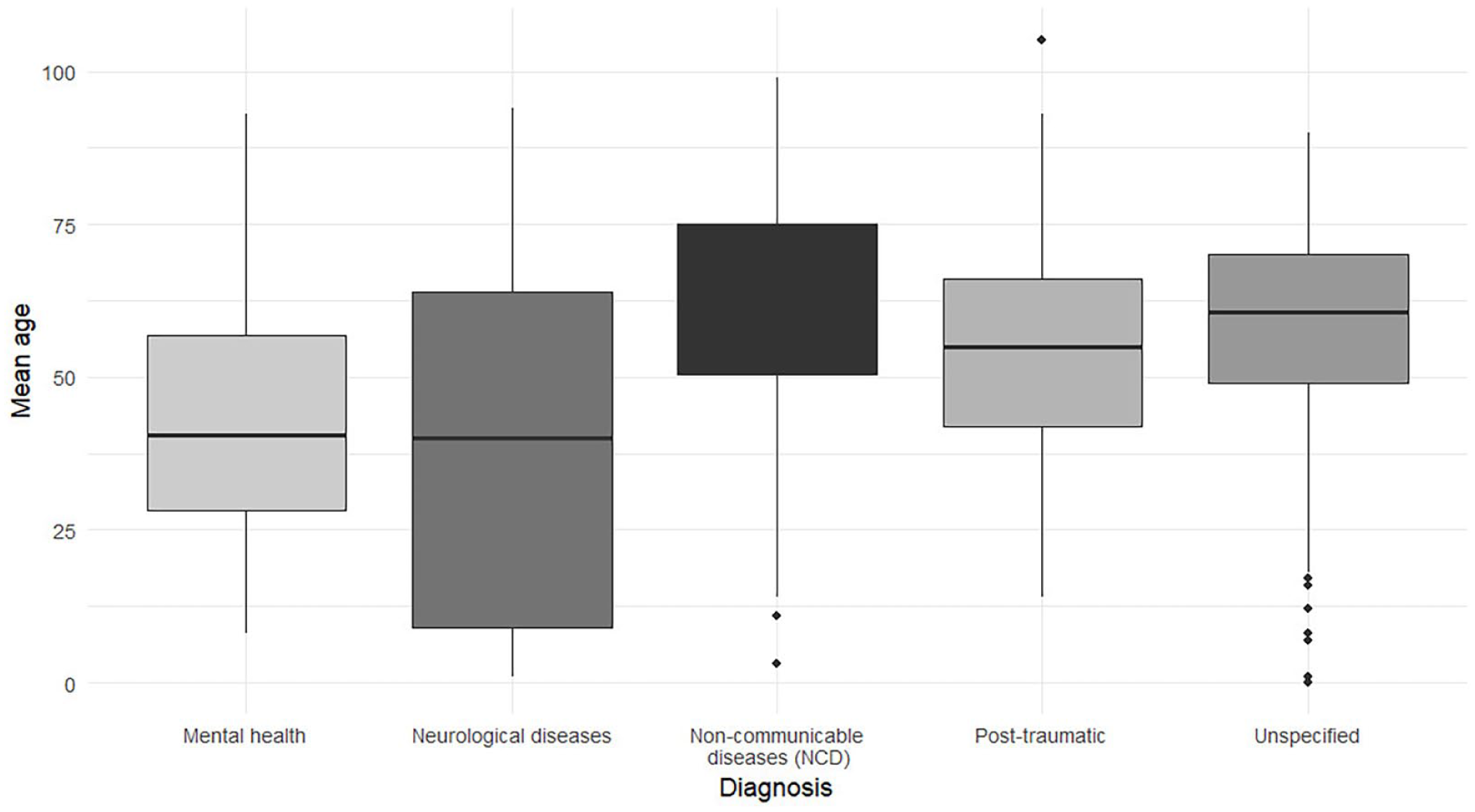
Boxplot of age by telemedicine participant diagnosis.
Telerehabilitation Service
The primary specialty involved in the provision of telerehabilitation services was physiatry (32%), followed by psychosocial services (psychology or social work) (29%) and physiotherapy (26.59%). Female patients predominantly sought psychosocial services (33%) and physiotherapy (28%), with statistically significant differences compared to males (p < .001) (Table 2).
Characteristics of the telerehabilitation services by sex during the COVID-19 pandemic in 2020-2021, Cali, Colombia.

Chi-square. bPhonoaudiology, Occupational Therapy and Physiotherapy. cFisher’s exact test.
Patients receiving speech (Phonoaudiology) and occupational therapy services had a mean age of ⩽30 years, whereas consultations for physiatry and physiotherapy were predominantly among older individuals (physiatry: n = 497, mean = 57 ± 19; physiotherapy: n = 418, mean = 57 ± 16; phono-audiology: n = 69, mean = 30 ± 29; psychosocial therapy: n = 458, mean = 44 ± 18; occupational therapy: n = 69, mean = 26 ± 26; mixed services: n = 61, mean = 48 ± 15; Kruskal-Wallis test, p = .001) (Figure 3).

Boxplot of age of telemedicine participants by type of teleconsultation.
Most patients successfully completed their teleconsultations without difficulties (n = 1423; 90.52%). Consultations that were not conducted (n = 149; 9.48%) were primarily due to the inability to contact the patient (81.63%) or the patient’s unavailability at the scheduled time (16.33%). Telephone calls were the most frequently utilized communication modality (62.70%), followed by video calls (37%). The average duration of the teleconsultations was 55 ± 37 minutes.
Approximately 29% of patients sought consultation for pain management, with this subgroup being significantly older (mean age: 58 ± 16 years) compared to those consulting for other reasons (mean age: 47 ± 20 years) (p < .001). More than half of the participants had at least 1 follow-up appointment (54.41%).
Further treatment was required in 72% of the cases, while 13% of patients successfully completed their rehabilitation process. A satisfactory recovery was documented in 6.42% of patients. The treatment dropout rate was 3%. Among patients who completed treatment, women were proportionally more represented than men (15% vs 11%), although this difference did not reach statistical significance (p = .051). The mean age of patients who completed treatment was 56 ± 16 years, compared to 52 ± 23 years for those who abandoned treatment and 47 ± 17 years for those who achieved recovery (p < .05).
Discussion
The telerehabilitation landscape in Colombia and Latin America has evolved in response to the COVID-19 pandemic, with a focus on improving healthcare access and timeliness.4,10 The implementation of telemedicine services, particularly in rehabilitation and virtual therapy, has been a crucial aspect of this evolution.4,10 To our knowledge, this is the first study in Colombia to examine both the existing literature on telerehabilitation and the practical outcomes from 2 rehabilitation centers. The findings provide insight into existing barriers, associated challenges, and future opportunities for the development of telerehabilitation services.
The literature on telemedicine and telerehabilitation in Latin America, and particularly in Colombia, remains limited and reflects diverse perspectives and healthcare contexts. While several studies have examined the implementation of telemedicine in Colombia—including telerehabilitation in gynecology, pediatrics, speech-language therapy, and occupational therapy, as well as regulatory challenges during the COVID-19 pandemic.19 -23 There is a notable gap in research focused on the evaluation and characterization of telerehabilitation services and patient populations. None of the reviewed studies have comprehensively addressed this aspect.
We encounter an increase expected in consultations under telerehabilitation during the pandemic and social crisis in Colombia. While telerehabilitation services existed before the pandemic, it was underutilized in Latin America and its implementation ensured healthcare by adapting with the tools that the patients and healthcare providers had (cell phones, home computers).18,24,25 Furthermore, telerehabilitation services have been adopted in situations of isolation due to social unrest, become relevant to ensure the continuity of interventions, and reducing attention time without affecting the cost.26 -29
Most of the telerehabilitation users were adults in their productive years (18-35 years) and older adults (⩾65 years). Observational studies have described how advanced age, being Latino or from an ethnic minority, adverse socioeconomic conditions, low digital literacy, and residing in rural areas are associated with lower utilization of telemedicine and tools such as video or video conferencing.30,31 This highlights the importance of addressing disparities and providing adequate support and resources to ensure equitable access regardless of age or socio-economic background. 32
A superior educational background can enhance the utilization of virtual healthcare tools, thereby fostering more efficient correspondence between healthcare providers and patients concerning the prescribed therapeutic directives. 33 Within our study population, most patients had university-level educational attainment. Nevertheless, it is crucial to acknowledge that age and proficiency in digital literacy emerge as significant variables that may some individuals able to use these tools in higher proportions.
Mental health was the second most addressed condition in telerehabilitation, primarily among women, followed by traumatic injury and sequels. The global impact of the COVID-19 pandemic on mental health has been reported in Colombia and worldwide.34,35 A recovery rate of 6.4% in the context of telerehabilitation may initially appear low; however, this figure must be interpreted in light of several key factors. The study population included individuals with chronic, post-traumatic, or neurological conditions, which typically require long-term or continuous therapy rather than short-term resolution.36,37 The fact that 72.3% of patients required ongoing care reflects the complexity of the cases, where full recovery is often delayed or not feasible.36,37 Additionally, “recovery” in this study was defined as the achievement of therapeutic goals, rather than a complete return to baseline health. In chronic or neurodegenerative conditions, this type of recovery is often unattainable, and lower rates are expected.36,37 Comparable telerehabilitation studies, particularly in resource-limited or post-disaster settings, frequently report recovery rates below 10%, with most patients transitioning to maintenance care.11,36,37 Lastly, external factors such as the COVID-19 pandemic, social unrest, and digital barriers likely disrupted the continuity and intensity of care, further impacting outcomes. When considering social determinants of health, one of the most affected population were low-income young females 38 , and among specific populations such a pregnant women during the pandemic revealed prevalence rates of 2.77% for PTSD, 27.88% for anxiety, 14.7% for depression, and 16.5% for insomnia symptoms, coinciding with the “third wave” COVID-19 peak in Colombia. 39
Furthermore, there is a greater likelihood and inclination among women to seek psychosocial services compared to men. 40 All above support the idea that a differential approach and intersectional perspective, based on the unique health requirements of distinct population groups, such as gender, ethnicity, and other demographic attributes ensures the incorporation of personalized strategies and pathways, programs, and disciplines, ultimately leading to improved care and attention. 41 This could be applied in future telerehabilitation services for better outcomes.
Men seek telerehabilitation services, related to traumatic injury and its sequelae. This can be attributed to the overall levels of violence and high rates of externally caused injuries in both the city and the country.42,43 Despite being considered preventable events, these continue to pose a challenge for rehabilitation services in Colombia and particularly in Cali.44,45 Therefore, the main teleconsultations are expected to relate to physiatry and physiotherapy 46 ; In our study, about 30% of consultations were related to pain. This aligns with the significant role of telerehabilitation in addressing the aftermath of traumatic injuries and chronic pain patients, 47 emphasizing its relevance for the population served.
The pandemic significantly impacted health and well-being in Latin America. Data from 2015 to 2021 across Brazil, Ecuador, Mexico, and Peru, regarding hospital discharges and mortality rates for conditions amenable to healthcare, indicates that hospitalizations for these conditions decreased by 28%, while mortality rates rose by 15% compared to pre-pandemic levels. Noncommunicable diseases contributed to 89% of the increased mortality, with poorer states experiencing more significant rises. These findings highlight the importance of maintaining healthcare services during emergencies, particularly for noncommunicable diseases, and expanding telemedicine and nonphysician healthcare worker roles. The use of telemedicine was instrumental in addressing the challenges posed by the pandemic, particularly in rural communities, where it amplified the identification and management of chronic conditions such as cognitive decline and cardiovascular issues. 48
Less than 2% of teleconsultations were not conducted due to internet access issues, which a common barrier that has become a social determinant of health along with technological device ownership in other to access telerehabilitation for the most underserved.13,49 Additionally, it is essential to consider that the retrospective data may underestimate the therapeutic outcomes. These factors underscore the need for further attention and research into the specific needs of each patient, which can either hinder or enhance the utilization of telerehabilitation and the achievement of therapeutic goals. 50
Colombia’s legislation on telemedicine is still in early stages, approval for using the services is not specified in terms of instances or by whom it is determined, whether by provider criteria or patient willingness to accept it. Additionally, there is no regulatory association overseeing the development of these practices, with regulatory gaps that difficult the progress of e-Health, requiring reforms to align with the needs of the population, not only in response to the challenges posed by COVID-19 but also to extend the reach of telemedicine and telerehabilitation to populations unable to relocate, such as inmates.51,52 This underscores the pivotal role of public health interventions and the decision-making of national leaders in enhancing healthcare outcomes.
Despite the establishment of definitions for telemedicine and technical requirements to ensure communication, security, infrastructure conditions, data storage, and other aspects described in Colombian normativity,3,53 budgetary decisions, along with the lack of interinstitutional networks and public policies, continue to limit the scope and development of telerehabilitation in the country. 54 In high-income countries, telemedicine has proven to be a convenient way to continue providing care and closely monitor patients, thereby improving adherence and clinical outcomes. 55
Limitations
In Colombia as in Latin America, there are limitations such as infrastructure, political, and technological capabilities to facilitate effective virtual healthcare processes. This is exemplified by notable service gaps in the assessed referral centers: While synchronous physiatry, physiotherapy, phonoaudiology, psychosocial therapy, and limited occupational therapy were delivered via telephone/video, pivotal domains like low-vision rehabilitation, cardiopulmonary rehabilitation, structured cognitive training, virtual assistive-technology training, and vocational rehabilitation were absent. In Colombia’s resource-constrained environment, these omissions reflect multifactorial feasibility barriers: Limited broadband access beyond metropolitan areas, overreliance on telephone-only modalities, and uneven digital literacy hinder bandwidth-intensive services (e.g., virtual reality or vision-based retraining). 56 National regulations prioritize general teleconsultation but exclude specialized rehabilitation requiring equipment or coordination, complicating scalability of services like visual or cardiac/respiratory telerehabilitation.9,57 In addition visual rehabilitation services in Colombia have historically operated under significant resource constraints, even prior to the pandemic. Predominantly centralized within tertiary facilities, with particularly fragmented infrastructure for low-vision care restricted. This underdevelopment fundamentally impedes remote service delivery models and contributes to the systematic underrepresentation of visual rehabilitation in empirical investigations such as ours. 58
In high-income countries such as USA, the American Telemedicine Association, dictates the principles of delivering telerehabilitation services and regulations, before the COVID-19 pandemic. 59 Furthermore, Europe has several well-established programs focused on telerehabilitation, particularly in cardiology.60,61 A comparative study in 2022 explored telerehabilitation services across South America (Brazil, Chile, and Colombia) and Australia, identified significant barriers in LMICs (limited resources, infrastructure, and technological networks). Also highlights promising opportunities for healthcare advancements in telerehabilitation, indicating its potential to facilitate healthcare improvements. 9 This creates barriers and inequity for vulnerable population, making it challenging to implement telerehabilitation properly during periods of confinement. 53 Despite this, we describe the outcomes of telerehabilitation in 2 specialized centers, responding to a high demand in southwestern Colombia, with acceptable adherence expressed in a 3% treatment dropout rate. This observation could be explained because most of consultations were ongoing treatments (62.73%) for chronic conditions.
This observational study has potential inaccuracies in estimating therapeutic outcomes due to the absence of explanatory models. The sample, limited to 2 specialized telerehabilitation centers, may not fully reflect the Colombian population, thus limiting the generalizability of the results. Another limitation was the incomplete availability of certain variables, such as consultation duration and pain-related reasons, which were inconsistently recorded across the institutions’ medical record systems. This led to reduced denominators in the corresponding analyses and may limit the interpretation of these specific findings. Despite this, the centers comply with regulatory standards. Service stratification provides insights into the specific conditions treated and aids in identifying rehabilitation needs. However, the study indicates unclear technological barriers, highlighting the necessity for further qualitative research to enhance understanding.
Strengths
This pioneering study uniquely explores Colombia’s telerehabilitation landscape, utilizing a robust observational method with a broad patient base from the southwestern region. It contributes novel insights into digital medicine, with data from 2 specialized centers ensuring high-quality, representative findings. The diverse sample enriches our understanding of telerehabilitation’s impact across demographics. Conducted during the pandemic, it underscores telerehabilitation’s role in maintaining healthcare continuity, filling a critical gap in Latin American telemedicine literature. The results can guide policy and practice development in telerehabilitation, enhancing healthcare access in resource-constrained settings and supporting global health equity objectives.
Future Directions
Telemedicine and telerehabilitation offer the potential for enhancing healthcare access in Latin America. Overcoming barriers across various levels, particularly among underserved demographics like educational status, and enhancing infrastructure and telecommunication services in remote areas through regulatory measures are crucial. Adopting models from high-income countries and customizing them to local population characteristics can significantly improve healthcare coverage. National leaders and stakeholders play a crucial role in promoting these endeavors by establishing well-coordinated healthcare policies for telerehabilitation.
Longitudinal studies assessing the long-term outcomes of telerehabilitation, comparative feasibility research, and investigations into the implementation of specific technological solutions, combined with qualitative analyses on telerehabilitation and e-health, could improve the services in this field.
Conclusions
The COVID-19 pandemic has highlighted the importance of telerehabilitation in Colombia and Latin America, underscoring the need for improved healthcare accessibility and efficiency. Despite its crucial role in providing services to those unable to access traditional care, research on telehealth remains limited. Factors such as age, education, economic status, and digital literacy affect the effectiveness of telerehabilitation, especially among vulnerable populations facing technological and social challenges. Further longitudinal, qualitative, and prospective research is essential to understand these barriers and to promote initiatives in the area.
Supplemental Material
sj-jpg-1-rpo-10.1177_27536351251375637 – Supplemental material for Telemedicine Challenges in Latin-America: Outcomes from Telerehabilitation Services During the COVID-19 Pandemic in Cali, Colombia—A Retrospective Cohort Study
Supplemental material, sj-jpg-1-rpo-10.1177_27536351251375637 for Telemedicine Challenges in Latin-America: Outcomes from Telerehabilitation Services During the COVID-19 Pandemic in Cali, Colombia—A Retrospective Cohort Study by Sara Gabriela Pacichana-Quinayaz, Lina María Rodríguez Vélez, Daniel Sánchez Cano, Olga Marina Hernández Orobio, María Ana Tovar Sánchez, Gloria Isabel Toro Córdoba and Francisco Javier Bonilla-Escobar in Advances in Rehabilitation Science and Practice
Supplemental Material
sj-pdf-1-rpo-10.1177_27536351251375637 – Supplemental material for Telemedicine Challenges in Latin-America: Outcomes from Telerehabilitation Services During the COVID-19 Pandemic in Cali, Colombia—A Retrospective Cohort Study
Supplemental material, sj-pdf-1-rpo-10.1177_27536351251375637 for Telemedicine Challenges in Latin-America: Outcomes from Telerehabilitation Services During the COVID-19 Pandemic in Cali, Colombia—A Retrospective Cohort Study by Sara Gabriela Pacichana-Quinayaz, Lina María Rodríguez Vélez, Daniel Sánchez Cano, Olga Marina Hernández Orobio, María Ana Tovar Sánchez, Gloria Isabel Toro Córdoba and Francisco Javier Bonilla-Escobar in Advances in Rehabilitation Science and Practice
Footnotes
Acknowledgements
The authors thank Fundación IDEAL para la Rehabilitación Integral “Julio H. Calonje” and Cosmitet LTDA for their collaboration in this study.
ORCID iDs
Ethical Considerations
The study was approved by the ethics committees of participating centers and the Universidad del Valle Institutional Review Board (Approval No. 014-021, August 13, 2021) in accordance with the Declaration of Helsinki.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universidad del Valle, Internal Call, 2020—Project Research CI-1904. Cali, Colombia (≈USD $15,000).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data are included in the manuscript and supporting information files. Due to the presence of medical records and clinical data, the full dataset cannot be shared publicly. Data are available upon request from the ethics committees of Fundación Ideal (
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.