
Abstract
Background:
Traumatic spinal cord injury impacts physical functioning, independence, and quality of life. The high incidence rate of 75.6 per million in South Africa indicate the crucial role of successful community reintegration. Despite South African’s policy emphasizing comprehensive rehabilitation of persons with disabilities, community reintegration following spinal cord injury remains inadequate.
Objective:
To develop a multidimensional model to improve community reintegration for individuals with traumatic spinal cord injuries in South Africa.
Methods:
A 4-phase mixed methods study was employed. Phase 1 used a cross-sectional survey of 108 individuals with spinal cord injuries to investigate levels and factors influencing psychosocial and community reintegration. Phase 2 involved 28 qualitative interviews with different content experts, including individuals with spinal cord injuries, caregivers, rehabilitation professionals, and persons representing people with disabilities in the communities. Phase 3 reviewed existing community reintegration programs, while Phase 4 used a Delphi technique with 10 experts to design and refine program components and strategies.
Results:
The study revealed low levels of psychosocial and community reintegration, influenced by employment and housing factors. Content experts highlighted barriers such as inaccessible environments, transportation challenges, and negative societal attitudes. Program components included technological support, employment assistance, mentorship, and recreational activities. The first 3 phases informed a development of a 3-level model addressing client, community, and legislative domains. In the fourth phase, experts reached consensus on components and strategies to achieve this multi-level community reintegration model.
Conclusion:
The evidence-based community reintegration model offers a structured, multi-level framework to address reintegration challenges in South Africa. It emphasizes coordinated interventions at individual, community, and policy levels to improve outcomes for individuals with traumatic spinal cord injuries.
Keywords
Introduction
Traumatic spinal cord injury (TSCI) represents a catastrophic event that fundamentally alters an individual’s life trajectory, resulting in varying degrees of permanent physical impairment, activity limitations, and participation restrictions. 1 Beyond the immediate physical consequences, TSCI profoundly impacts independence and quality of life (QoL). 2 Individuals with TSCI frequently encounter substantial challenges in maintaining employment, pursuing educational opportunities, and engaging in social activities, subsequently elevating their risk of social isolation and economic instability. 3
These multifaceted challenges emphasize the paramount importance of successful community reintegration (CR), defined as “the process of becoming part of the mainstream of family and community life, participating in normal roles and responsibilities, and being an active and contributing member of one’s social groups and society as a whole.”4,5 Dijkers 6 conceptualizes CR as an individual’s capacity to resume societal positions and activities commensurate with their demographic characteristics, particularly within community-based social networks. This conceptualization aligns with the International Classification of Functioning, Disability and Health’ (ICF) framework, which emphasizes how personal and environmental factors can either facilitate or impede community participation for individuals with disabilities. 7
Evidence suggests that comprehensive CR programs incorporating self-management strategies, psychosocial support, and enhanced functional independence are crucial for optimizing long-term outcomes and QoL. 8 These programs focus on facilitating meaningful societal participation, encompassing aspects such as securing appropriate housing, achieving independent community mobility, engaging in chosen professional and educational pursuits, and developing fulfilling interpersonal relationships. Additionally, addressing environmental barriers and advocating for inclusive policies are essential elements in promoting full participation and successful CR for individuals with TSCI. 9
South Africa faces a particularly challenging situation, with a reported TSCI incidence rate of 75.6 per million population. 10 This high incidence rate presents a significant public health challenge within the context of the country’s resource-constrained healthcare system. While rehabilitation services are delivered through a combination of public healthcare facilities, non-governmental organizations, and private practitioners, with coordination by the National Department of Health, the system faces substantial limitations in resources and distribution of services.
Despite South Africa’s national rehabilitation policy emphasizing CR and productive activity, a substantial implementation gap persists in rehabilitation services, particularly for individuals with TSCI. Current rehabilitation practices often terminate at basic functional outcomes such as mobility and self-care, failing to progress to comprehensive CR outcomes.11,12 This limitation is especially problematic within South Africa’s distinct socioeconomic context, characterized by inadequate accessibility infrastructure, elevated unemployment rates, and pronounced disparities in healthcare access between urban and rural regions.
The development of culturally appropriate and contextually relevant CR programs has been impeded by the scarcity of multidimensional research approaches to TSCI rehabilitation in South Africa. While few studies have investigated barriers to CR following various disabilities in the South African context,13-17 none have specifically addressed the design of a CR program tailored for individuals with TSCI. To bridge this critical knowledge gap, this study employed a multidimensional methodology comprising 4 distinct phases to develop a CR program specifically designed for individuals with TSCI in South Africa.
Materials and Methods
This study employed a multi-phased mixed methods approach 18 to investigate CR among individuals with TSCI. The research comprised 4 interconnected phases designed to examine CR levels, identify influencing factors, review CR programs, and develop a CR model.
The initial phase established baseline data through quantitative analysis of psychosocial reintegration, perceived CR, and their associations with self-efficacy and quality of life. Subsequently, qualitative research was conducted to explore perspectives from multiple content experts, including TSCI individuals, caregivers, rehabilitation professionals, and disability organization representatives. A scoping review systematically examined existing CR programs, while a Delphi study facilitated consensus-building for CR model development.
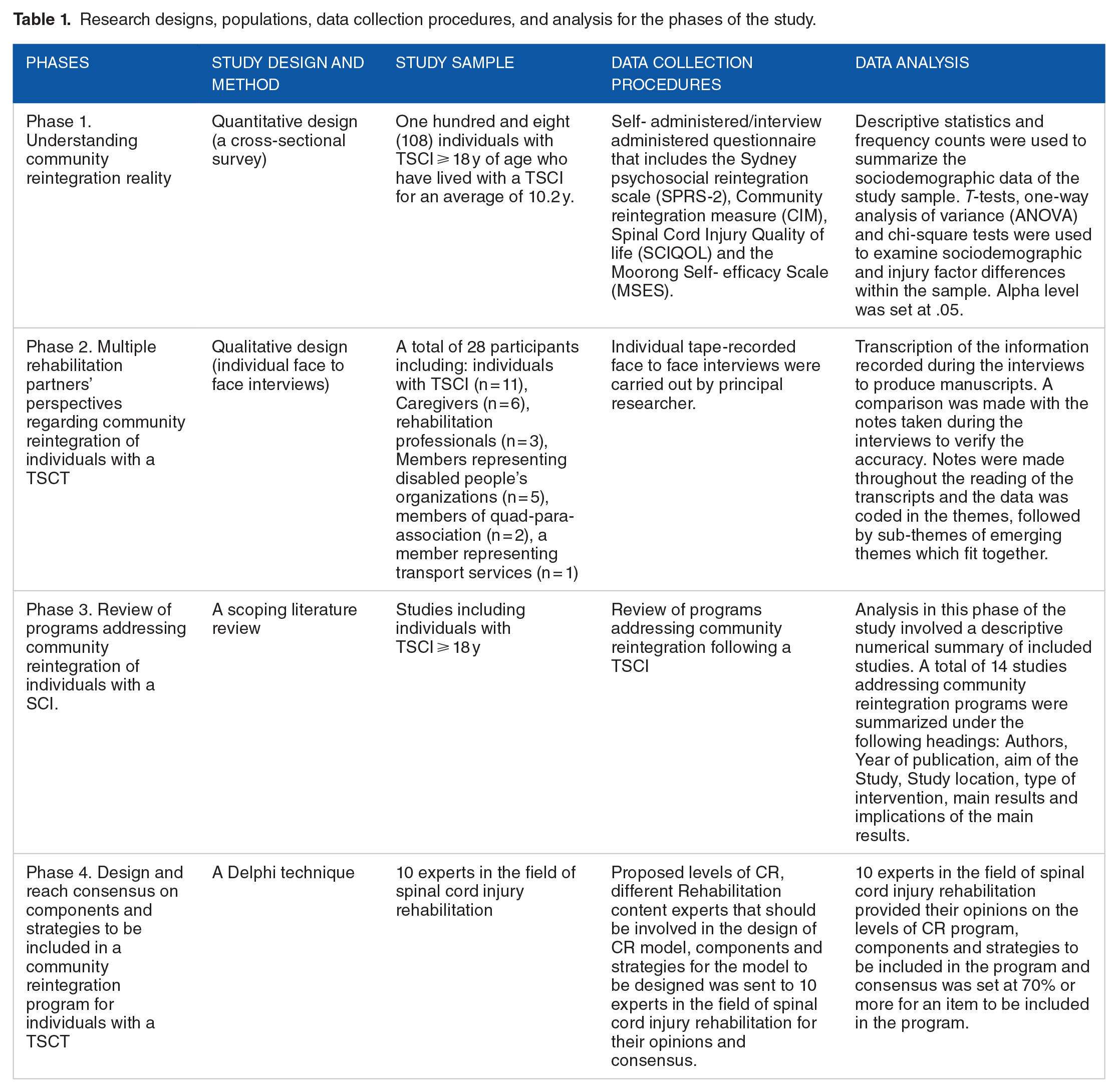
The methodological framework was structured to ensure each phase informed subsequent stages, creating an integrated research approach. This design enabled strategic data integration and triangulation across phases, enhancing the validity of the resulting CR model. The involvement of diverse content experts throughout the process strengthened the study’s potential for policy-directed guidance. Table 1 summarizes the methods, study design, sample characteristics, and analytical approaches employed in each phase, demonstrating the systematic progression of the research protocol.
Research designs, populations, data collection procedures, and analysis for the phases of the study.
Ethical approval to conduct this study was obtained from the Senate Research Committee of the University of the Western Cape (No. 15/4/51).
For phase 1 and 2, the detailed methodologies are described in our previous papers published elsewhere.19-22 In phase 3, A scoping review was conducted to map existing literature on community reintegration programs for individuals with TSCI. The review followed Arksey and O’Malley’s 23 framework and Pham et al’s 24 recommendations. Multiple databases were searched including Science Direct, EBSCOHOST (Academic search complete, CINAHL, ERIC, Health sources (Nursing/academic edition, Master file premier), MEDLINE, SocINDEX, Africa online platforms. In addition, Hand-searching and reference list checking supplemented the database searches. Keywords included terms related to spinal cord injury, rehabilitation, community integration and program/s. Studies were included if they were published in English between 2010 and 2023, addressed community reintegration programs, and focused on adults (⩾18 years) with spinal cord injury.
A standardized form was used to capture key study characteristics including participant demographics, program components, intervention details, outcomes, and implementation factors. Thematic analysis was used to identify patterns across programs, while descriptive statistics summarized study characteristics.
In Phase 4, a 2-round Delphi study 25 was conducted to develop a standardized CR program for spinal cord injury patients. Expert participants were nominated through prominent organizations including the World Health Organization (WHO), International Spinal Cord Society (ISCoS), American Spinal Injury Association (ASIA), and international academic institutions.
Initially, 20 potential experts were identified and invited to participate. Of these, 15 experts consented to engage in the study, with 12 completing and returning the first-round questionnaire. The initial questionnaire comprised demographic data collection and 3 open-ended questions exploring critical aspects of CR: The 3 open-ended questions in this phase included: (1) In your opinion what does community reintegration following spinal cord injury mean?, (2) In your opinion, what components should be included in a community reintegration program following spinal cord injury?, and (3) In your opinion, who are the role player/content experts that should be involved when designing a community reintegration programme following spinal cord injury?.
Qualitative data from the first round was analyzed using Atlas.ti version 22, 26 employing thematic analysis to generate emergent themes. The resulting insights informed the development of proposed CR levels, content experts, program components, and strategies. The results from the first round informed the development of the questionnaire for the second round.
The second round utilized a Likert-scale questionnaire containing proposed levels of CR, a list of content experts that should be involved in the development of CR program, components that should be included and strategies. The response options ranged from strongly agree to strongly disagree. Following McKenna and Hasson’s guidelines, 27 consensus was set at 70% or higher for including levels, components, and strategies in the CR program. Ten experts completed the second-round questionnaire within a 3- week period, successfully achieving consensus and concluding the final study phase. This systematic approach ensured a comprehensive, expert-validated framework for CR program for individuals with TSCI.
Results
This section presents the results of each phase used to design a CR program for individuals with TSCI. The study took a comprehensive approach, examining the reality of CR, content experts’ perspectives, existing programs, and ultimately proposing a holistic CR model targeting individual, community, and government levels.
Phase 1: Understanding community reintegration reality
The initial phase used a quantitative methods to established baseline data on CR among individuals with TSCI, examining psychosocial reintegration, perceived CR, and their relationship with self-efficacy and quality of life. The detailed findings of this phase are described in details in our previous papers published elsewhere.19-21 In general, the findings revealed low levels of psychosocial and perceived CR, with employment emerging as a significant factor. Employed participants demonstrated higher scores in psychosocial reintegration, perceived CR, self-efficacy, and quality of life.19-21 and individuals with higher self-efficacy demonstrated better quality of life. 21 However, only 38% of participants were employed. This employment challenge was reflected in the Community Integration Measure (CIM), particularly in Item 10: “I have useful/productive things to do in this community,” which received the lowest scores. 20
In addition to employment, housing conditions also significantly impacted CR perceptions, with informal dwelling residents reporting poorer reintegration.20,22 Limited employment opportunities likely forced individuals to live in affordable but less desirable communities, as evidenced by low scores on CIM Item 1: “I feel like part of this community that I belong here.” 20 In addition to employment and living situation, self-efficacy also emerged as a critical factor influencing perceived CR, and psychosocial reintegration, particularly in social functioning rather than daily activities. 21
The findings from Phase 1 provided a crucial foundation for the subsequent phases of the study. The low levels of psychosocial and perceived CR observed and the influence of employment, living conditions and self-efficacy on reintegration and QoL emphasized the need for a deeper understanding of the contributing factors leading to phase 2 of this study that aimed to explore multiple content experts’ perspectives about CR following a TSCI.
Phase 2: Multiple content experts’ perspectives regarding community reintegration of individuals with a traumatic spinal cord injury
Moving beyond the quantitative data obtained in Phase 1, phase 2 employed qualitative methods to explore perspectives from multiple content experts, including individuals with TSCI, caregivers, rehabilitation professionals, and persons representing people with disabilities in the community.
Thematic analysis identified 6 major themes and 16 sub-themes from multiple content experts. All themes and sub-themes identified fall under the contextual factors classified within the ICF. Individuals with a TSCI expressed their experiences in form of barriers and facilitators to reintegration. These were confirmed by other content experts in their views for what is needed for an optimal CR. Figure 1 outlines the themes and sub-themes that emerged during analysis. Few selected verbatim quotes are highlighted and readers are referred to our paper 22 published elsewhere for the detailed findings of this phase.

Themes and categories identified by multiple content experts.
In general, inaccessible physical environment significantly impacted reintegration, with participants highlighting challenges in both home and outdoor spaces in some cases leading to confinement and isolation as persons with spinal cord indicated:
“When I returned home, the lack of space made it challenging to move around with a wheelchair” (Tom, Person with TSCI), “The side roads is not suitable, and I struggle to move around, that is why I often prefer not to go out” (James, Person with TSCI).
Other content experts emphasized the importance of accessible design. A disability organization representative stated: “For me, full reintegration means modifying toilets, bathrooms, and kitchens to fit the needs of people with TSCI and ensure full participation” (PRDPO1, Person representing disabled people’s organization). A rehabilitation professional added: “Public toilet seats are often too low or inaccessible, ATMs are too high and difficult to access, and banks should have dedicated help desks” (RP3, Rehabilitation professional). Both of these highlight the need for adequate materials and goods to enhance physical capacity and performance for CR.
Employment transitions often proved difficult after the injury. One participant with TSCI stated: “Before I got into this accident, I was working with this company as a driver, after my rehabilitation I could not go back to work because I was in the wheelchair. I called them to find out if they could give me an alternative job. They said that they would call me back, but I never heard from them again” (John, Person with TSCI).
Employer attitudes presented another significant barrier. A rehabilitation professional noted: “The employers do not want to employ people with disabilities. Especially people with physical disabilities because they do not want to adjust the work environment to meet the needs of disabled people. So, I think there should not be any discrimination towards employment opportunities based on any condition including people with disabilities” (RP3, Rehabilitation professional).
Lack of transport also emerged as a critical barrier to employment, creating a paradoxical situation as 1 participant with TSCI explained: “I would like to get a job, but transport is a problem. Actually, I got a job at the day hospital, but I could not take it because I could not get there. I need a hired vehicle to take me there because it is uphill from where I am staying, and I cannot get there with a wheelchair” (Ana, person with TSCI).
Support systems and relationships proved crucial for successful reintegration. One participant with TSCI shared: “If I want to go to the clinic my brother always pushes me there . . . and if my brother is not available my sister in-law pushes me” (Monica, Person with TSCI).
This was confirmed by a rehabilitation professional who stated: “Support from family members and close friends is important and it can play a valuable role in facilitating individuals with SCIs to reintegrate back into communities” (RP2, Rehabilitation professional).
However, societal attitudes and stigma remained significant challenges. One participant with TSCI expressed: “Their attitudes make me sick . . . They need to be educated; they need to know that we are human beings like them” (Nick, Person with TSCI).
Besides environmental factors, personal factors, including self-efficacy and confidence, also significantly influenced reintegration success for individuals with TSCI. One participant noted: “There are many places which are not comfortable, but you can make it comfortable for you. You can make life easier even if it seems very difficult. If you choose to be negative, then everything will be difficult for you” (Tim, Person with TSCI).
However, many struggled with confidence and relationships post-injury: “I used to do part time event planning before the accident. But because my job requires me to speak in front of big crowds, I noticed that after the accident I do not have the same ability and confidence to walk up to people and speak over the mic again” (Mary, Person with TSCI).
Another participant shared: “I used to have a girlfriend before, but she left me immediately after the accident. Now I do not have one and I am scared to approach any girl when I am still in this wheelchair . . . What about if I approach someone and she rejects me because I am in the wheelchair? I am really scared” (Tom, Person with TSCI).
The insights gained from Phase 2 provided valuable context to the quantitative findings of Phase 1 and highlighted the multifaceted nature of CR. Based on results of this phase, it was clear that the issues of CR for individuals with a TSCI highlighted by various content experts during the discussion were closely linked to participation domain of the ICF including environmental and personal factors. The qualitative insights from Phase 2 revealed multiple interconnected challenges affecting CR for individuals with TSCI, including transportation barriers, employment difficulties, physical environment limitations, societal attitudes, and personal factors like self-confidence. These content experts’ perspectives, ranging from TSCI individuals to rehabilitation professionals and disability representatives, highlighted the need for comprehensive programs addressing both environmental and personal barriers to successful reintegration. Given these multifaceted challenges identified through content experts experiences, Phase 3 aimed to review existing programs addressing community reintegration of individuals with SCI.
Phase 3: Review of programs addressing community reintegration of individuals with a TSCI
The results of the first and second phase pointed to the need to identify existing programs addressing CR following SCI through a scoping review for potential adoption, adaptation, or contextualization. The search yielded 272 articles (269 from databases, 3 from manual search). After screening, 252 were excluded for irrelevance, 5 for duplication, 2 for including brain injuries only, and 2 for including participants under 18. The final review included 14 full-text articles. Figure 2 presents the flow chart of included studies.

Flow chart of included studies.
The analysis of programs described in the included papers revealed distinct yet interconnected domains of intervention, each addressing specific aspects of the reintegration journey. These evidence-based programs can be systematically categorized into the following key therapeutic domains:
Technological Integration and Communication Support Programs
Advanced technology-aided program focusing on enabling the participants to activate songs, videos, requests, text messages, and telephone calls was designed. These options were presented on computer screen and activated through a small pressure microswitch by man with SCI and special touch screen by the post-coma man. The program demonstrated significant efficacy in enhancing communication and leisure activities for SCI patients. Implementation of pressure microswitches and touch screens enabled independent management of entertainment systems, telecommunication, and request submission, showing promising outcomes for daily independence for post-coma man. 28
Employment Support Programs
Ottomanelli et al29,30 reported that participants who participated in their supported employment (SE) programs were 2.5 to 11.4 times more likely to achieve competitive employment compared to traditional treatment groups, with a 30.8% employment success rate versus 10.5% in controls. Bangladesh’s vocational training program achieved 60% employment rates, with 74% reporting enhanced family economic status. 31 These findings were corroborated by Singaporean research demonstrating improved community integration and functional independence through vocational rehabilitation program. 32
Mentorship and Educational Programs
The “Back on Track” mentoring program, requiring quarterly mentor-mentee interactions over 2 years, achieved a 24% return-to-education rate and 6.9% employment rate, emphasizing the significance of support systems in community reintegration. 33
Therapeutic Recreation and Sports Integration Programs
Adaptive sports programs for veterans demonstrated significant improvements in psychological health and quality of life. 34 Therapeutic recreation cottage programs increased positive affect and self-efficacy, 35 while, outdoor recreational programs, including skiing, rafting, and climbing, facilitated enhanced social, recreational, and vocational engagement, effectively supporting community reintegration. 36
Empowering Community-Based Reintegration Programs
A 12 week therapeutic education program co-facilitated by occupational therapy and social work professionals, demonstrated marked improvements in self-efficacy and quality of life, 37 whereas the “Reinventing Yourself After SCI” program, focusing on 8 specific skills for personal development, achieved notable improvements in SCI-specific self-efficacy within 6 months post-discharge. 38
Health Promotion Programs
Project Shake-It-Up, comprising 10 full-day bimonthly sessions, integrated structured learning with physical activities. The program incorporated indoor activities (strength training, aerobic conditioning) and outdoor experiences (sailing, kayaking), resulting in significant improvements in independent-living skills and self-confidence across multiple life domains. 39
Sex Education Programs
A multidisciplinary sexuality program for male SCI patients, emphasizing safe sexual practices and adaptive equipment, demonstrated high participant satisfaction. The program’s success highlighted the effectiveness of interdisciplinary approaches in addressing both functional and emotional aspects of sexual health. 40
The collective evidence suggests that successful CR following SCI requires an integrated approach combining multiple elements including: Sustained employment support, technological adaptation, recreational engagement, comprehensive health services, psychological support, and social integration strategies. The findings from Phases 1 to 3 provide a critical foundation for Phase 4’s program design. Phase 1’s quantitative data revealed low reintegration levels and key barriers, while Phase 2’s content experts’ insights identified interconnected challenges to community reintegration. Phase 3’s review mapped effective evidence-based programs, creating a comprehensive understanding of needs, perspectives, and successful interventions that provides the empirical basis for developing targeted reintegration strategies in Phase 4.
Phase 4: design and reach consensus on levels, components and strategies to be included in a community reintegration program for individuals with a TSCT
The integration of results from the first 3 phases revealed that a successful CR program should target 3 distinct levels: client, community/society, and government/legislative levels. This multi-level approach emerged from the analysis showing that factors influencing CR following TSCI were closely aligned with the ICF domain of participation, while accounting for contextual factors including both environmental and personal elements.
Based on these findings, the first round of the Delphi study was designed to explore rehabilitation experts’ perspectives on 2 key aspects: The meaning of community reintegration, the identification of components that should be included and critical contents experts who should be involved in program design.
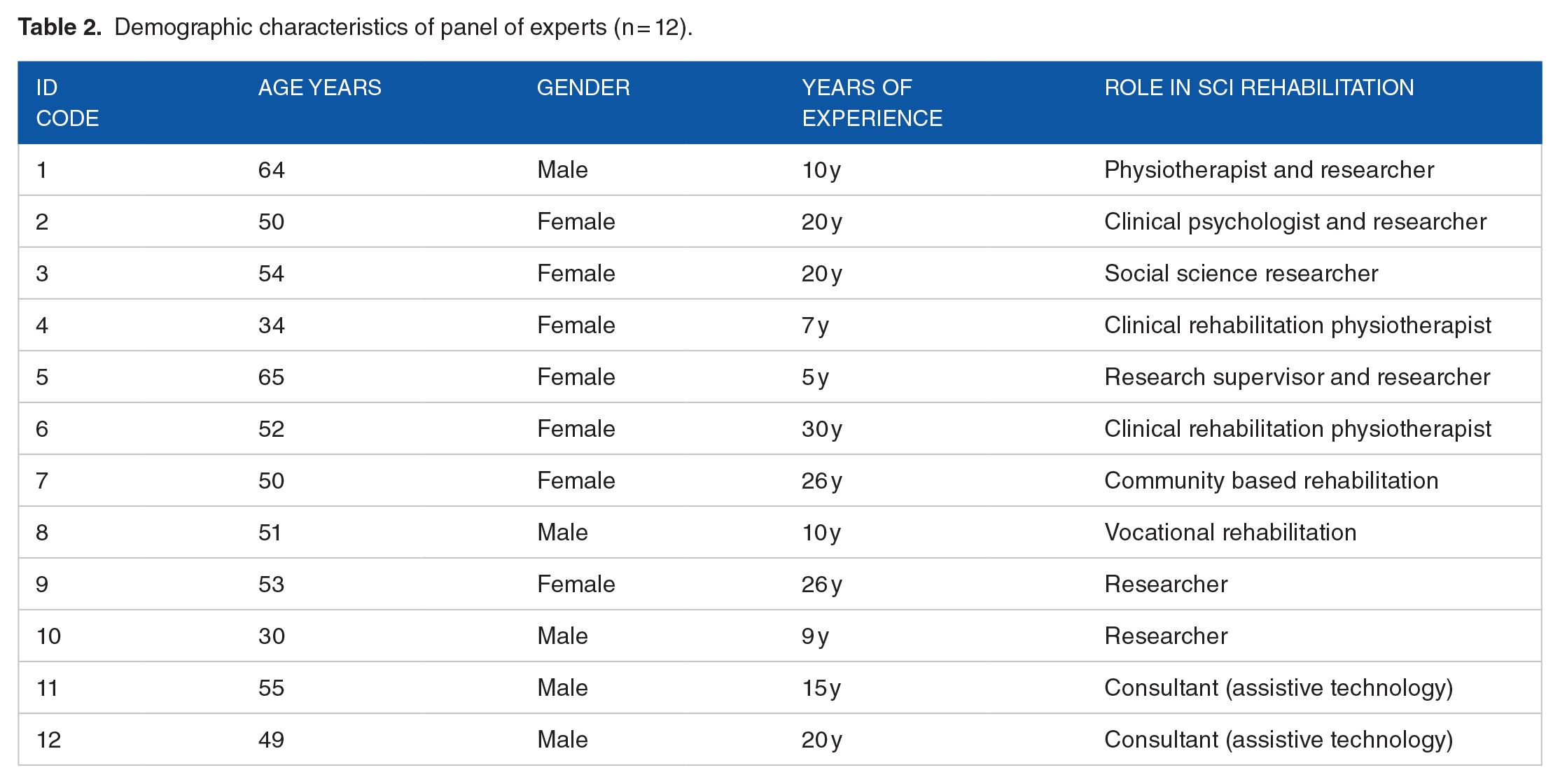
Twelve experts completed and returned the questionnaire in phase 1. These included: 8 females and 4 males, aged 30 to 65 years, representing various disciplines: physiotherapy (6), occupational therapy (2), orthotics (2), clinical psychology (1), and social science research (1). Participants were recruited from 6 countries: South Africa (4), USA (2), New Zealand (2), Sweden (2), Australia (1), and UK (1), with professional experience ranging from 5 to 30 years. Table 2 presents demographic characteristics of the experts in the first round of the study.
Demographic characteristics of panel of experts (n = 12).
The experts described the meaning of community reintegration following TSCI as being able to live independently in the community, full participation in social role, able to gain employment, having access to education and having family, friends, and societal support. The content experts that should be involved included, individuals with traumatic spinal cord injuries, their families and caregivers, multidisciplinary rehabilitation team, policy makers, employers, community leaders, religious leaders, peer support/mentors, leisure, and recreational workers, school leaders and business people. The proposed main components were: Self-management, access to education and employment, Accessible homes, outdoor communities, and work place environment. Availability of transport, assistive devices/technology, recreational facilities, peer support systems, and counselling services. These components formed the foundation for developing specific program strategies (detailed in the Supplemental File). The second round of the Delphi study achieved consensus on levels of CR, content experts that should be involved, components that should included and strategies, successfully concluding the final phase of the research.
Community Reintegration Model
The CR model (Figure 3), developed through 4 rigorous research phases, presents an integrated approach targeting client, community, and governmental levels.

Proposed community reintegration model for individuals with TSCI.
The model strategically addresses barriers identified in earlier phases through interconnected components including self-management, environmental access, including sports and recreation facilities, education, attitudinal change, vocation, and employment, as well as inclusive policies addressing issues of persons with TSCI. This multi-level framework, validated through a Delphi consensus, provides a structured pathway for successful CR of individuals with TSCI in South Africa.
Discussion
The developed CR model presents a comprehensive 3-tiered approach that could significantly impact rehabilitation outcomes for individuals with TSCI. The framework’s strength lies in its recognition that successful reintegration requires simultaneous intervention at individual, community, and policy levels.
At the individual level, the focus on self-management and psychological support is particularly crucial in the South African context, where limited resources often necessitate greater self-reliance. The emphasis on developing self-advocacy skills and coping strategies could be especially powerful in communities where disability awareness is still evolving. 41 Implementation could involve establishing peer support networks and skills training programs, potentially leveraging mobile technology, providing reliable fast broadband internet connection to reach rural areas which may introduce possibility of some working from home overcoming the barriers of the inaccessible work place environment which can help reduce social isolation.
The community-level implementation requires careful coordination among diverse rehabilitation partners. In the South African context, this could be achieved through the establishment of local disability forums that bring together healthcare providers, community leaders, religious institutions, and disability advocates. These forums could focus on practical initiatives such as: Creating awareness campaigns that address cultural stigmas around disability, implementing accessibility audits of public spaces and businesses, developing community-based rehabilitation programs that utilize local resources, establishing vocational training partnerships with local businesses.
The policy-level component is perhaps the most generalizable aspect of the framework, as many countries face similar challenges in implementing disability legislation. South Africa’s progressive constitution and existing disability rights framework, 42 provide a strong foundation, though implementation remains challenging. Success at this level requires: strengthening enforcement mechanisms for existing accessibility regulations, creating financial incentives for businesses to improve accessibility, developing public-private partnerships for infrastructure development, establishing monitoring systems to track progress and outcomes.
The framework’s emphasis on rehabilitation partners’ collaboration is particularly relevant to resource-limited settings such as South Africa. By involving diverse content experts from the outset, programs can leverage existing resources and infrastructure more effectively. This collaborative approach could be enhanced by: creating formal coordination mechanisms between healthcare facilities and community organizations, establishing regular content experts’ forums to share resources and best practices, developing standardized assessment tools to measure reintegration outcomes, implementing continuous feedback loops to refine interventions.
While the framework’s core principles are broadly applicable, successful implementation requires careful adaptation to local contexts. In South Africa, this might mean addressing unique challenges such as rural accessibility, diverse cultural perspectives on disability, and varying levels of infrastructure development across provinces. The model’s flexibility allows for such customization while maintaining its fundamental focus on comprehensive support across all levels of intervention. Moving forward, pilot programs in different South African communities could help refine implementation strategies and identify key success factors. These insights could then inform adaptation of the framework to other settings, particularly in countries with similar socioeconomic challenges.
A comprehensive financing framework for community rehabilitation initiatives encompasses multiple funding streams. Primary funding sources include government social development grants, international development assistance, and private sector partnerships through corporate social responsibility programs. Religious institutions and NGOs can facilitate resource pooling for peer support and educational programs. the implementation of this model requires strategic partnerships: the Department of Social Development coordinates with corporate sponsors, while international partners support environmental modifications. Disabled persons’ organizations maintain oversight to ensure program effectiveness. The Department of Health allocates resources for peer support, while sports federations facilitate recreational activities through corporate investment. This multi-sectorial approach promotes sustainable community ownership and program longevity.
Strengths
This study demonstrates notable strengths through its comprehensive mixed-methods approach and systematic 4-phase design. The methodology allowed for robust data collection and triangulation of findings, with each phase informing subsequent ones to create a cohesive research framework. A key strength lies in the study’s inclusive content experts engagement, incorporating perspectives from individuals with TSCI, caregivers, rehabilitation professionals, and disability organization representatives. The evidence-based nature of the study, combining empirical data with existing literature and expert opinions through the Delphi technique, provided a strong foundation for the model’s development. The resulting model’s comprehensive approach addresses interventions at individual, community, and government levels while maintaining specific focus on the South African context.
Limitations
The sample size of 108 participants may not fully represent South Africa’s diverse geographic and socioeconomic contexts. The cross-sectional design provides only a snapshot view, limiting understanding of how community reintegration changes over time. Additionally, the study focuses on model development without testing implementation or evaluating effectiveness in practice. The lack of cost-benefit analysis and limited discussion of resource requirements could affect practical implementation. While the South African focus ensures relevance locally, it may limit generalizability to other contexts. Finally, our survey focused solely on traumatic SCI patients, though our rehabilitation model would serve all paraplegic individuals regardless of etiology. Future studies should include non-traumatic cases.
Conclusion
The development of a comprehensive CR model for individuals with TSCI in South Africa represents a significant advancement in rehabilitation science and practice. This rigorous 4-phase mixed-methods study created an evidence-based framework addressing the complex challenges of CR within the South African context. Key insights emerged, including the crucial role of employment status, housing conditions, transportation accessibility, and personal factors like self-efficacy in shaping reintegration outcomes. Integrating diverse content experts’ perspectives ensures the model addresses real-world challenges and practical implementation considerations. The systematic approach to identifying program components through multiple research phases provides stronger empirical support compared to many existing models. The model’s strength lies in its multi-level approach, targeting interventions at client, community/society, and government/legislative levels. This comprehensive CR framework acknowledges that successful reintegration requires coordinated efforts across multiple domains, from individual self-management to broader community engagement and policy initiatives, representing a significant advancement in rehabilitation science and practice.
Supplemental Material
sj-docx-1-rpo-10.1177_27536351251326797 – Supplemental material for A Community Reintegration Model for Persons With Traumatic Spinal Cord Injury in South Africa: Process and Outcomes
Supplemental material, sj-docx-1-rpo-10.1177_27536351251326797 for A Community Reintegration Model for Persons With Traumatic Spinal Cord Injury in South Africa: Process and Outcomes by Eugene Nizeyimana, Quinette Louw and Conran Joseph in Advances in Rehabilitation Science and Practice
Footnotes
Acknowledgements
We thank all persons with spinal cord injury and other content experts who voluntarily participated in this study. We also thank our colleague Thandi Conradie for her contribution on the design of the model.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Research Foundation of South Africa (NRF; Award no 98727).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
EN: Involved in conceptualization of the study, processing and analysis of data, drafted the first version on the manuscript, submitted the paper and acted as a corresponding author. QL and CJ assisted in data analysis, contributed to the first draft and approved the final version of the article.
Data Availability
The dataset generated and analyzed during the current study is available from the corresponding author on reasonable request.
Statement and Declaration
Not applicable.
Ethical Approval
Ethical approval to conduct this study was obtained from the Senate Research Committee of the University of the Western Cape (No. 15/4/51).
Consent to Participate
Informed consent was obtained from all subjects involved in the study.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.