
Abstract
Objective:
To report practice based evidence built on clinical findings where an intensive therapeutic approach called ACQUIRE Therapy was used as a rehabilitation/habilitation tool for children diagnosed with CASK mutations. ACQUIRE Therapy delivery is based on principles of learning and guided by a therapeutic framework often used in the delivery of intensive therapy.
Design:
Clinical Cohort.
Setting:
Natural environments (eg, home-like environment).
Participants:
A total of 20 females, 12 to 128 months, mean age = 44.75 (SD = 31.64).
Intervention:
Trained Occupational therapists delivered high-dosage rehabilitation for an average of 64.06 hours (SD = 12.91) across 4 weeks. ACQUIRE Therapy targeted cross-domain intervention targets often associated with executive control and praxis.
Main outcome measures:
Clinical data was examined from the following sources; therapist daily treatment documentation (eg, therapy goals, video recordings, daily therapy logs, and discharge documentation).
Results:
Receptive communication improved in all children. The most common motor skill improvements occurred in trunk control occurring in 33% of children; followed by, gross reaching abilities in 21% of children; fine-motor skills in 19%; head control in 15%; and mobility in 12%. Documentation of cognitive-motor pairing of skills was documented in all children.
Conclusions:
Diagnosis specific intervention targets (eg, attention and cognitive-pairing skills) need to be considered when providing therapeutic services to children with CASK-gene mutations and other forms of Global Developmental Delay.
Clinicaltrials.gov registration number is NCT03325946. Date of registration: 1 May 2013. Trial Dates: December 2014 and October 2023. https://clinicaltrials.gov/study/NCT03325946?locStr=Roanoke,%20VA&country=United%20States&state=Virginia&city=Roanoke&cond=Cerebral%20Palsy&intr=Intensive%20therapy&rank=2
Keywords
Introduction
CASK-related disability (calcium/calmodulinactivated serine kinase) is an X-linked disorder 1 of brain development that stems from a mutation in the CASK gene and results in disabilities that affect cognition, motor skills, sensory impairments, and functional abilities.2,3 This diagnosis is associated with a wide phenotypic spectrum ranging from mild-to-severe intellectual disability and impairment across multiple developmental areas 4 dependent upon the place and amount of mutation. 5 The exact prevalence of CASK related disability is unknown. 6 The disorder is more commonly reported in females than males and the exact mechanisms for impairment on brain pathology are not well understood.7,8 Movement disorders specifically can include; hypo- or hypertonia, with hyperkinetic movements that range from chorea to dystonia.3,4 The discovery of the CASK gene is relatively recent, thus there is a paucity of understanding of the diagnosis, its developmental progression, and or its responsiveness to varied rehabilitation efforts.
One form of intensive neurorehabilitation that has been reported in the treatment of children with CASK mutation is ACQUIRE therapy. This approach is an evidenced based form of high-dosage therapy guided by a therapeutic framework (shown in Figure 1), and it has been used in multiple RCTs with children with other developmental disorders such as Cerebral Palsy. 9 The ACQUIRE framework describes the reciprocal exchange between a child participating in therapy and a therapist guiding the therapeutic process to promote learning. The framework provides a model of therapy where therapists use operant conditioning to systematically scaffold therapy activities towards targeted goals. Historically, the framework has been implemented for children with Cerebral Palsy and the treatment focus has been on motor and functional skill development.

The ACQUIRE framework.
In 2017, we reported a clinical case series of 3 females with microcephaly with pontine cerebellar hypoplasia (MICPCH) that were responsive to the ACQUIRE therapy model. 4 The primary focus of the initial case series was in understanding if ACQUIRE therapy impacted change in these young girls’ motor abilities, and in fact, results from the Peabody Developmental Motor Scales - Second Edition (PDMS-2) did show 2 areas of consistent change across children within the Stationary and Visual-Motor subscales. Other subscales of the PDMS-2 were less responsive to change. As we began to work with more children with CASK-related disability, we recognized that the areas of change might be related to overarching functional control mechanisms, and we began to try to identify explicit intervention targets. The ACQUIRE framework indicates attention and awareness as they jointly occur between a therapist and a child as a major factor for successful therapy. In children with static lesions of the brain (eg, cerebral palsy and stroke), this represents variables for effective therapy engagement. However, in most therapy processes if a child and therapist are jointly attending to a task, then awareness of the task and the constructs associated with the task (eg, cause and effect) are thought to be almost automatic. We began to realize that perhaps these constructs might need to be thought of as distinct intervention goals for children with CASK diagnosis in a manner that allowed for the therapist to actually target tying attention and awareness together. Actually targeting and expanding the child’s abilities in attention or their ability to have an “attentional awareness” became a critical intervention target for learning new skills. In essence, it was clear that children could sometimes “attend,” or at least appear to attend to an event or task, and still have no functional awareness of the surrounding constructs of the task. There seems to be limited ability of children with a CASK diagnosis to pair cognitive abilities and or sensory information with functional outcomes. For example, some children diagnosed with CASK who can walk do not avoid objects in their path, despite being able to see the object. We also began to realize attentional awareness could be disrupted in multiple areas of the learning process. As such, Figure 2 shows therapy targets that we theorize can be systematically shaped to promote learning in children with CASK-related disability. There are many motor planning theories that demonstrate a child must have an intention to act and successfully pair that intention to act with age-appropriate output action for function to occur. 10 We theorize that attentional awareness of the intention to act, the actioned output, and or even the pairing of those things can all be disrupted in children with CASK-related disabilities, and that these points can also be specific intervention targets, as shown in the figure 2.

Rehabilitation targets for children with cask-related disability.
An advantage of the ACQUIRE framework is that it encourages the pairing of skills across multiple domains of development that can be simultaneously targeted to promote learning during the therapeutic process (eg, attention and interaction, attention and motor skill development, motor skills and functional use, and communication and interaction). However, in traditional rehabilitation, pairing of attention and function are often measured synonymously. There is recognition that attention is required for a function to occur, but rarely is the construct of attention the target of rehabilitation. It is somewhat assumed that ‘attention’ is automatically related to an actionable intention whether that intention is for an outward functional action or an internal cognitive function. In addition, there are few childhood measures of function or stage of development that allow for distinguishing between a functional output, the intention to create the output, and or the attention needed at both of these junctions.
The following clinical cohort reports the ACQUIRE Therapy process on 20 female children with MICPCH associated with CASK mutation(s). This expanded population has allowed us to consider additional therapeutic targets and potential mechanisms that may be change agents important to consider when working with children with CASK-related disability. We also recognize that our presentation has many recognized limitations because of these somewhat ‘novel’ intervention topics. Those limitations are represented in our data presentation, where we found no satisfactory standardized measures of change. Rather, we present clinical interpretations that call for a need to develop standardized measures of the proposed intervention targets with appropriate sensitivity to children who have complex disabilities. While not the specific target of this paper, we believe that such measures would have broad applications across pediatric rehabilitation because while the proposed intervention targets have been defined based on the limitations we have seen expressed across children with CASK-related disability, the intervention targets themselves likely have implications across many diagnoses.
Methods
Study design
This clinical cohort includes a convenience sample of 20 females diagnosed with CASK gene mutations. Inclusion criteria included the diagnosis of CASK gene mutation, medical stability, and no documented uncontrolled seizures. Participants included families whose caregivers independently sought out clinical services from the Fralin Biomedical Research Institute’s Neuromotor Research Clinic (FBRINMC). The University’s Institutional Review Board approved the collection and use of clinical data. Informed consent was obtained from each family prior to participation.
Participants
Participants ranged in age from 12 to 128 months (Mean age = 44.75 months; SD = 31.64). Data regarding race was gathered post hoc identifying 16 White participants, 1 Black participant, 2 Asian participants, and 1 Multi-Race participant. All children presented with delays in multiple areas of development associated with CASK mutations and microcephaly with pontine cerebellar hypoplasia. All participants had noticeably decreased attention (eg, visual attention, duration, and/or impulsivity), all were observed to have inconsistent and or ineffective receptive and or expressive communication, as well as varying levels of delayed gross and or fine motor development.
Treatment protocol
All 20 participants received an intensive therapy treatment protocol where the ACQUIRE Framework was used to guide therapy activities. The first 3 of 20 participants received 40 hours of treatment, 5 days a week, within a 2 weeks period. The therapeutic dosage was then increased for the remaining 17 children following study reports in neurorehabilitive efforts recommending higher dosage for maximum learning. 9 The FBRINMC typically provides a dosage of 4 hours of therapy a day, 5 days a week, across 4 weeks. Variations in dosage sometimes occur due to illness and scheduling conflicts. Of the remaining 17 participants, the minimum dosage delivered was a total of 46 hours and the maximum dosage delivered was 78.75 hours. Exact dosage for each participant is reported in Table 1. Across all children the average dosage was 64.06 hours (SD = 12.91) with a range between 40 and 78.75 hours. Therapy was implemented by trained ACQUIRE Occupational therapists in the child’s home-like environment. All intervention components were supervised by an Occupational Therapist who is part of the team who developed the ACQUIRE framework and participated in multiple clinical trials of the ACQUIRE therapy model. Most children did not live in the local area of the FBRINMC, so they relocated and made temporary living arrangements that allowed for in-home therapy delivery.
Individual changes across motor abilities, other developmental domains and total number skills changed across motor and developmental domains combined.

✓, present at pre-treatment; no entry, Not present; ↑, positive change.
Outcome measures
Clinical data was collected and examined from the following sources; therapist daily treatment documentation (eg, therapy goals, video recordings, daily therapy logs, and discharge documentation). For reporting purposes baseline data consisted of data obtained from the first 3 days of clinical documentation and post data or gain data was developed via examination of the last 3 days of clinical documentation data. Systematic examination of data occurred for all 20 children. Examinations were considered for 4 common domains of change that included; attention, communication, motor (gross or fine), and motor-cognitive pairing. All domains were scored as present, absent, or change from the first week to the last week of treatment. The attention domain included visual attention, duration of attention, and or ability to control behaviors. Communication was broken down into 2 components, effectively receiving a message (receptive communication), and expressive communication (effectively sending a message). Receptive communication was demonstrated by the child appearing to understand messages from conversational partners by appropriately acting or with purposeful looking at activity targets. Expressive communication included all forms of expression (eg, pointing, manual signs, sounds, words, and sentences). Due to the wide spectrum of motor abilities at baseline, the motor domain was broken down into 6 categories of abilities: head control, trunk/sitting posture, crawling/transitions, walking, targeted reaching, and fine motor. Categories were intentionally broad to allow for individual incremental changes to be captured since the goal was to create a documentation of clinical changes that were not addressable via traditional developmental metrics that would allow for cross children comparison in domain categories. For example, improvements in sitting posture for 1 child might be to maintain an upright positon with back support, another child might be propped sitting, while another child might be dynamic sitting. Finally, motor-cognitive pairing was scored for changes in ability to pair a motor skill with a cognitive demand to create a functional outcome (eg, following single or multi step directions and completing single or multi step demands within play activities, activities of daily living, or within social interactions).
Data analysis
The data presented is primarily subjective and qualitative as described in our assessment section above. First, we present frequencies of changes in various domains of development for each individual child. Finally, the percentage of change by motor skills domains across the group of children. Analysis was completed for age-related effects via a correlation between the number of motor-skill domain changes and age in months.
Results
Table 1 lists each child in chronological order based on age and dosage received. This table also reports changes in motor abilities across 6 categories, changes in other developmental domains including: communication(s) (receptive and expressive), attention, and cognitive-motor pairing, and provides a total number of changes observed across all 10 categories. Figure 3 shows percentage change of motor skills across all 20 children. The most common areas of change were in trunk control and reaching. Age in months and levels of measurable motor change were negatively correlated with high significance (r = .72, P < .001). This correlation was of moderate strength (r2 = .52).
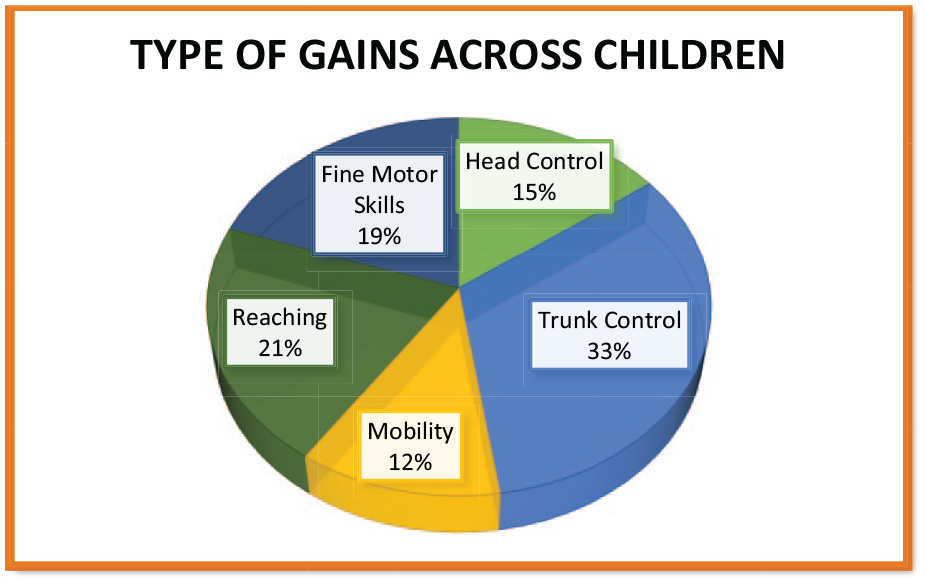
Percent change by motor categories in 20 females with CASK-related disabilities.
Discussion
All children demonstrated positive changes in at least 2 traditional domains of development following an intensive burst of ACQUIRE therapy. In addition, we could clinically score changes where motor skills were paired with another functional process that matched a therapeutic request in all children, often across many tasks. A few examples include independent adjustments of posture following verbal request, grasping items and placing them in a requested location, or completing a multistep puzzle. However, it is notable that the data we report is categorizations of change based on expert observation, not objective standardized measures. As stated in the introduction, we did so because we believed that standardized assessments had limited ability to inform our understanding of the children’s responsiveness to therapy efforts. While this is a limitation it could also be argued to be a strength of reporting practice-based efforts. Practice-based evidence should be routinely gathered in rehabilitation for many reasons. We report our findings to help inform other clinicians who might have children with microcephaly on their case-load and to encourage increased attention to the need for therapy research efforts for children with rare disorders such as CASK mutation. Also, we believe this work represents and reports on novel constructs that many rehabilitationists in both the clinical and research communities should consider.
In our rehabilitation attempts across all 20 children we consistently targeted and saw positive responses to our efforts when intervention targets crossed developmental domains. Our intervention targets were aimed at aiding the children to construct an understanding of an event (creating an intention) and or creating appropriate actions (output) to requested events.
While we have put forward a model that represents areas of potential impairments, we also recognize that the learning children demonstrated likely occurred in many ways, but our model is designed to suggest areas to consider. Changes in processing, organizing, and sequencing events related across many cognitive processing areas that are needed for purposeful functional actions (ie, intention to use information coming into a system and or acting on information to create a singular or multiple actions as appropriate output). Children with CASK-related disability have global developmental delays associated broadly with executive functioning and praxis. Collectively, planning, organizing, and sequencing a series of steps to create a motor output or action is defined as praxis.10,11 Many areas of rehabilitation focus on apraxic disabilities. 11 While praxis is thought to be heavily related to executive functioning, 12 praxis typically can be thought of in terms of specifics of an action; whereas, executive functioning is often thought of as more encompassing representing control, exchanges of information, and interactions with considerations across time for learning and memory.13 -17 While these definitions are none-the-less true for children with CASK-related disabilities or other types of developmental delay, we are suggesting there needs to be more specification in constructs within these definitions (eg, attention) that may serve as rehabilitation targets of interest for interventions.
Understanding this is complicated, however, and our work with 20 children is only a start. Children with CASK-related disability likely have limitations across many areas of processing, organizing, and sequencing information to create functional actions. For example, many children with CASK mutations who do learn to speak often start with echolalic speech patterns. They do not always pair word production with object identification or communication. Is this a representation of multiple intervention targets in our model or is the disruption more at a specific area? Is this child and mutation dependent? Similarly, a child with CASK-related disability may have the motor ability/action to grasp and release and object, but lack the cognitive representation to pair with the functional ability of grasping a utensil and utilizing it for feeding. These system disruptions likely occur at differing rates across development and in relation to types and levels of mutations as suggested above, and it is likely that future clinical efforts and future research will require refinements in our proposed model and definitely in how interventions are used to targets these areas. Interventions will need to promote greater levels of organizing and sequencing of combinatory inputs to allow and encourage children to meet the cognitive demands associated with motor and functional requests in order to be effective ‘rehabilitation/habilitation’ for children with CASK-related disability. Finally, we wish to reiterate that clinicians and researchers must consider the measures available for documenting change. We made clinical observations of changes that are not easily measured via traditional outcome measures given the distinct characteristics of children with CASK-related impairments. Perhaps child and diagnosis-friendly measures of executive functioning and praxis need to be developed.
Conclusions
This clinical cohort is one of the largest known to be reported for children diagnosed with CASK-related disability. The findings suggest that each child responded positively to the ACQUIRE intensive therapy approach. We observed that changes in motor skills, often a target of rehabilitation efforts, were more likely to occur or at least be seen with younger children, but the relationship was only of moderate strength. This might indicate that other variables related to cognitive processes or the intervention targets are impacting this relationship across all ages. It is important these findings be replicated and that studies investigate the efficacy of differing therapy efforts in this population. Long term follow-up data also needs to be collected regarding therapy efforts, but also on the natural history of children with CASK-diagnoses. Ultimately, therapeutic targets for rehabilitation for children with CASK-related disabilities need to be defined and measurable to improve outcomes for children with CASK-related disabilities to elucidate rehabilitation efforts.
Footnotes
Acknowledgements
The authors wish to acknowledge and thank first and foremost the families and children who have allowed us to learn from them. We would also like thank the Fralin Biomedical Research Institute and the Neuromotor Research Clinic team of therapist Kelsey Burke, Megan Price, and Rachel Mitchell, as well as Sharon Landesman Ramey and Craig Ramey who contributed to the development of the ACQUIRE therapy model of services.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was internally funded by the Fralin Biomedical Research Institute Neuromotor Research Clinic (FBRINMRC).
Availability of Data and Materials
Datasets analyzed for this study are not publicly available and cannot be shared opening to protect study participant privacy. Data collected were collected for clinical purposes and therefore individual data are not available for distribution or public use.
Ethical Approval and Consent to Participate
Virginia Tech University’s Institutional Review Board approved the collection and use of clinical data (IRB # 13-196). Parental permissions were obtained for each participant prior to participation.
Consent for Publication
All data is de-identified therefore no personal health information is presented. And consent for publication and use of this data is a subheading in the parental permissions that all participants’ parents signed.