
Abstract
Introduction:
Amblyopia is the medical term for a “lazy eye.” It occurs when vision in one or both eyes does not develop properly during childhood even though there is no structural abnormality of the eye. It consists of an interocular difference of two lines or more in a visual acuity table (without specifying any), or visual acuity worse than or equal to 20/30 Snellen Feet equivalent to 0.2 LogMAR, with the best optical correction. (American Academy of Ophthalmology) Patching is the international gold standard amblyopia treatment, based on a monocular stimulation of the eye with lower vision. It needs high compliance and a long period of treatment during plastic age. The purpose of our work is to evaluate the efficiency of a different and faster method for amblyopia rehabilitation, useful even for patients out of the plastic age: specifically homebased binocular rehabilitation therapy through specific smartphone/tablet games combined with anagliphyc glasses. This method, due to its ease of use, high compliance and cheap cost, could reach a great number of patients that until now have the risk of being abandoned if they are not able, for different reason, to follow the others common therapies.
Methods:
Fifty-five patients: mean age 8.98 ± 5.38, underwent ophthalmologic and orthoptic evaluations for amblyopia: BVCA with ETDRS logMAR, stereoacuity with Lang Stereotest I, ocular motility examination, fundus oculi and cycloplegic refraction examination. Eligible children had ⩾0.2 (as applicable) logMAR interocular difference, or BVCA worse or equal to 0.2 LogMAR. Patients were rehabilitated with specific dichoptic treatment by digital videogames for 1 hour/day for 2 months. Children wore red–blue anaglyphic glasses to play the games (with low-contrast components visible to 1 eye and high-contrast components visible to the other eye) for 7 hours per week (1 hour per day) for 8 weeks, with 2 outcome examinations programmed by protocol at 4 and 8 weeks from baseline.
Results:
After 8 weeks of treatment, amblyopic eye BCVA improved from 0.28 ± 0.13 logMAR at baseline to 0.10 ± 0.09 (P < .05) logMAR, with an improvement of 0.18 ± 0.09 logMAR.
Conclusion:
Achieved results relating to visual acuity improvements using binocular rehabilitation by digital videogames were statistically significant and encouraging. It is important that research and experimentation does not cease at this stage. Larger sample sizes, extended rehabilitation treatment periods and longer follow-up must be undertaken, in order to obtain objective data relating to visual acuity maintenance and also to obtained visual acuity results linked to age.
Keywords
Introduction
In recent years new technologies and new physiological research development have shifted attention to a different therapeutic approach for amblyopia with binocular treatment.1 -5 Patching is the international gold standard treatment, based on a monocular stimulation of the eye with lower vision. Suppression and reduction in cortical excitatory binocular neurons in V1 during critical period, commonly lead to amblyopia.6 -8 Binocular neurons’ loss could be prevented due to a prompt. . . surgical and/or optical correction.6,7,9 The loss of binocular responsiveness of V1 neurons in strabismic animals is reversible when interocular suppression is removed by using a GABA antagonist to block GABAergic inhibition. 10 This suggests that the loss of binocular summation is a result of active suppression. This hypothesis received support from a report that adults with amblyopia can experience binocular vision when fellow eye contrast is reduced, revealing the presence of an intact binocular cortical mechanisms.11 -14 Taken together, these results suggest that it is active suppression that renders a structurally intact binocular visual system functionally monocular in amblyopia. Therefore, the structurally intact binocular pathways may be responsive to rehabilitation using binocular treatments. 15
On the basis of several international studies relating to these considerations, binocular rehabilitative treatment has been considered proficient.4,5,8,13,16 -18
The purpose of this work is to evaluate efficacy of binocular rehabilitation treatment in amblyopia, with an alternative therapeutic method: homebased therapy through specific smartphone/tablet games combined with anagliphyc glasses to assess the improvements in amblyopic eye visual acuity.
Poor compliance, poor recovery and maintenance of visual acuity relating to current therapies inspired our approach: adherence to occlusion is less than optimal8,19 and patching can improve visual acuity for 73% to 90% of children with amblyopia, but 15% to 50% may never achieve normal visual acuity after a lengthy course of treatment20 -22 and 25% of successfully treated suffer recurrence within 1 year off treatment 8 ; atropine penalization can have local and systemic side effects, 8 as the optical penalization that can be used only in moderate anisometropic amblyopia because of the potential effect on the fellow eye and alignment. 8 Inadequate adherence to the patching regimen is a major factor in treatment failure and can be poor due to the social and psychological effects of having to wear a patch, alongside the impaired vision experienced by the child on occlusion of their nonamblyopic eye. 1 Less frequent clinic visits and prolonged treatment duration are also associated with lower compliance. 23
Methods
Inclusion and exclusion criteria
Amblyopic children aged 4 to 12 years, (only 2 patients out of range) with strabismus, anisometropia, or both were recruited from “Azienda ospedaliero-univeritaria consorziale Policlinico di Bari” between May 2017 and September 2017 and “IRCCS—Casa Sollievo della Sofferenza” in San Giovanni Rotondo between December 2018 and April 2019. A further group of patients was recruited through our Private Medical Office. For this group we did not foresee age limits. Eligible children had ⩾0.2 (as applicable) logMAR interocular difference, or BVCA worse or equal to 0.2 LogMAR. Exclusion criteria were prematurity ⩾8 weeks, developmental delay, coexisting ocular, or systemic diseases.
Protocol
Recruited children underwent a complete orthoptic and ophthalmological examination. Following data was recorded:
- Medical history: Informations about prior strabismic surgery and other prior or co-existing anti- amblyopic therapies, such as patching and/or optic penalization. If in use patching was not stopped.
- BCVA with ETDRS logMAR chart.
- Ocular motility examination.
- Binocular cooperation examination with Lang Stereotest I (Lang-Stereotest AG; Küsnacht, Switzerland), Stereo Butterfly Test (Stereo Optical Co., Inc).
- Anterior segment and lens examination.
- Fundus oculi examination.
- Cycloplegic refraction examination was assessed previously, at least 6 weeks before the beginning of the treatment, with cyclopentolate hydrochloride 1%—1 drop every ten minutes, repeated 3 times. In this case, children wore glasses during the treatment if provided.
According to the Declaration of Helsinki, written consent was collected at the same time as the eye examination, and a compliance calendar was delivered in which information about the total hours of games played per day and the types of the games played would been entered from parents.
Methods
Children and parents have been encouraged to familiarise with binocular games and anaglyphic glasses (provided by us) under supervisors. The proper treatment procedures, such as saturation and contrast settings, were shown to parents and three type of games were available: Tetris (Stereopsis) (Figure 1), Letter Hunt (Minian Software Ltd.) (Figure 1) and Snake (Minian Software Ltd.). Children wore red–blue anaglyphic glasses to play the games for 7 hours per week (1 hour per day) for 8 weeks, with 2 outcome examinations programmed by protocol at 4 and 8 weeks from baseline. Further follow-up was not expected in this study.

Rehabilitation with binocular game.
All games used were available for free from the various online stores. The features we researched for, such as the increase of visual-spatial skills with increasing speed of the proposed stimulus, were included in the game’s software. In this study there was no commercial company involved. The common features in the proposed games have been ascertained by the supervisors, comparing the games’ settings. Three types of games were available, and we recommended an alternate use to offer an interchange in the choice to improve compliance.
Binocular games
Each game was dichoptic (Figure 2), with low-contrast components visible to 1 eye and high-contrast components visible to the other eye. For binocular games, fellow-eye contrast was set to 15% to 20% with amblyopic eye contrast 100% to allow the child to experience binocular vision.14,24 -26 As the child demonstrated that they did experience binocular vision (by achieving a criterion game score and with incremented VA), the lower contrast was gradually (5%-10%) incremented by the supervisors. The Tetris game, which was used in previous amblyopic treatment pilot studies,14,24 -26 had high-contrast falling blocks and low-contrast stationary base blocks that had to be fit together to form continuous rows of blocks. In the Letter Hunt game, a grid with randomize letters were presented and half divided in high-contrast and low-contrast. The aim of the game was to find and tap the letters to spell each word presented in a box. In the classic Snake game, high-contrast snake must be swiped to change direction and to catch as much low-contrast food as possible. Anaglyphic red lens was always placed on the amblyopic eye, to stimulate the foveal area, more sensitive to red wavelength.

Binocular game example.
Compliance
Compliance evaluation was carried out by a calendar compiled by parents where information about the total hours of the game played per day and the types of games played were entered. We have established 3 compliance levels: low, with less than 50% of prescribed hours of game play; medium, with a percentage between 50% and 70% of prescribed hours of game play; high, with more than 70% of prescribed hours of game play.
Data analysis
Data were elaborated and submitted by criterion with the Friedman test, a non-parametric statistical test well-stuited for repeated measurements on a single sample. Here, we will test if there are statistically significant differences among the 3 time points: “Income” (time zero), “1st outcome,” and “2nd outcome.”
Each patient was identified with a progressive number to be able to analyze the data anonymously.
Results
A total of 55 patients were enrolled into the study (mean age 8.98 ± 5.38). There were 17 children with strabismic amblyopia (31%), 23 children with anisometropic amblyopia (42%), 14 children have both, strabismus and anisometropia (25%) and 1 patient have deprivation amblyopia due to congenital cataract (2%).
At baseline, mean (+SD) amblyopic eye BCVA was 0.28 ± 0.13 logMAR. Overall, 31% had patching or optical treatment for amblyopia during the experimentation, with an average patching treatment of 3.82 ± 1.59 hours per day and 69% of patients received only binocular rehabilitation. Individual participants and their baseline characteristics are provided in Table 1.
Baseline data.

Abbreviations: A, anisometropic; B, both; D, deprivation.; S, strabismic
After considering data analysis, BCVA mean (+SD) of amblyopic eyes improved from baseline value 0.28 ± 0.13 logMAR to 0.14 ± 0.09 logMAR, at 4 weeks outcome, with an improvement of 0.14 ± 0.09 logMAR. According to the 8th weeks outcome, amblyopic eyes BCVA improved from 0.28 ± 0.13 logMAR, baseline value, to 0.10 ± 0.09 logMAR, with an improvement of 0.18 ± 0.09 logMAR (Chart 1).
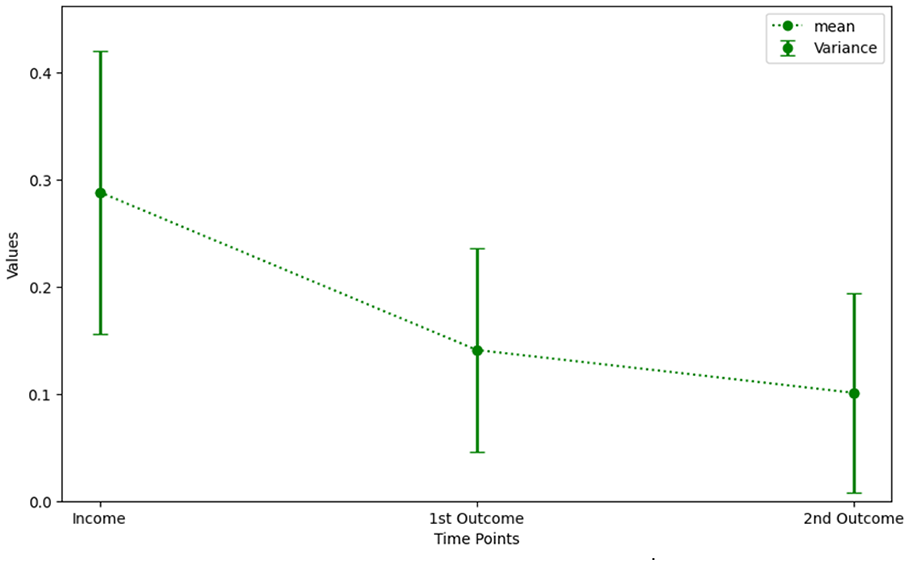
Values of the BCVA of the amblyopic eyes tend toward 0 logMAR.
The improvements recording with this method results is statistically significant with a P < .05.
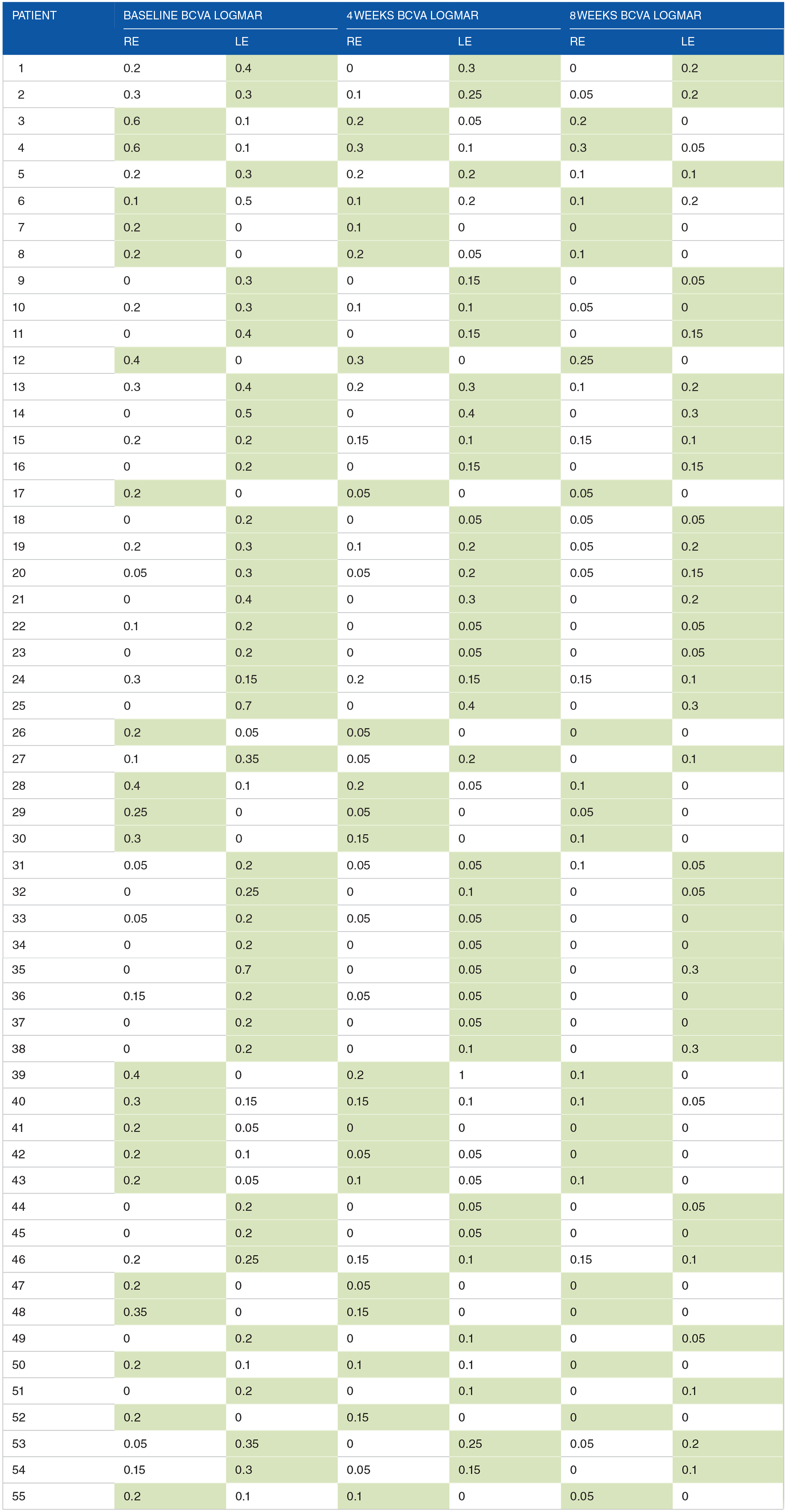
In the following table (Table 2) are shown baseline, 4 and 8 weeks BCVA logMAR outcomes. Amblyopic eyes in green.
Baseline, 4 and 8 weeks results (amblyopic eyes in green).

Analysing records regarding the fellow eye, an improvement, though modest, has also been found. Mean (+SD) BCVA concerning the fellow eye was 0.08 ± 0.1 logMAR at baseline, 0.04 ± 0.06 logMAR at the 4 weeks outcome and 0.02 ± 0.04 logMAR at the 8 weeks outcome. For some patients this result was more evident because they had bilateral amblyopia.
Based on the available sample, we are unable to estimate a reliable correlation between achieved improvements and the depth of amblyopia in each patient. For the same reason we can’t describe any correlations linked to age. The distribution of improvements is fairly homogeneous. The only consideration is that the greater the gap in visual acuity between the 2 eyes, the greater recovery was recorded. Furthermore, another correlation we cannot express with statistical data is a correlation between obtained improvements and type of amblyopia; however, the trend of our sample shows better response to binocular stimulation from patients with anisometropic amblyopia.
There is no doubt that the comparison of results between amblyopic eyes and fellow eyes shows a different outcome due to the different stimulation received. This is confirmed by the data: an average improvement in BCVA amblyopic eye from baseline to 8 weeks outcome of 0.18 ± 0.09 logMAR against an average improvement in BCVA fellow eye from baseline to 8 weeks outcome of 0.05 ± 0.07 logMAR.
Patients who received binocular rehabilitation in combination with patching were enrolled at least 6 months after the last visual acuity measurement without recorded improvements. We therefore decided to extend the check-up period to 6 months to verify that there were no improvements before combining the new therapy. During these 6 months, checks were made every 2 months to check for any improvements related to patching, which would have led to the exclusion of the patient from the study. That being so, BCVA enhancement seems too fast to be connected only with occlusion; Wallace et al 23 support that 120 hours of occlusion resulting in, on average, a 1 line (0.1 logMAR) improvement in visual acuity at 6 years of age. Moreover, Repka et al 27 compared the effectiveness of patching therapy versus atropine therapy, they found out that at the age of 10 years the improvement of the amblyopic eye is maintained, although residual amblyopia is common following treatment initiated at 3 to <7 years of age and that the outcome is similar regardless of initial treatment with atropine or patching. Similarly, Bangerter filters were found to be a reasonable treatment option for moderate amblyopia due to a lower burden of treatment and similar improvement in VA (less than half a line difference) compared to patching. 28
Cases of patients number 2 and 15 presented a bilateral amblyopia. We have alternately selected in green, as amblyopic eye, for patient number 2 the eye that has shown a minor improvement and for patient number 15 the eye that has shown greater improvement. This is to ensure that the results were not altered by subjective choices, because of the difficulty in detecting in bilateral amblyopia, which is the eye more involved.
Referring to patients older than 9 years, binocular rehabilitation has been tested individually, without additional patching therapy. The average age of the participants was 8.98 ± 5.38, most of them had had previous occlusion therapy. What we found, analysing data of our study, is an average improvement in visual acuity of 1 line (0.1 logMAR) after 1 month of rehabilitation (7 hours per weeks, a total of 28 hours per month) in patients, on average, out of “critical period.”
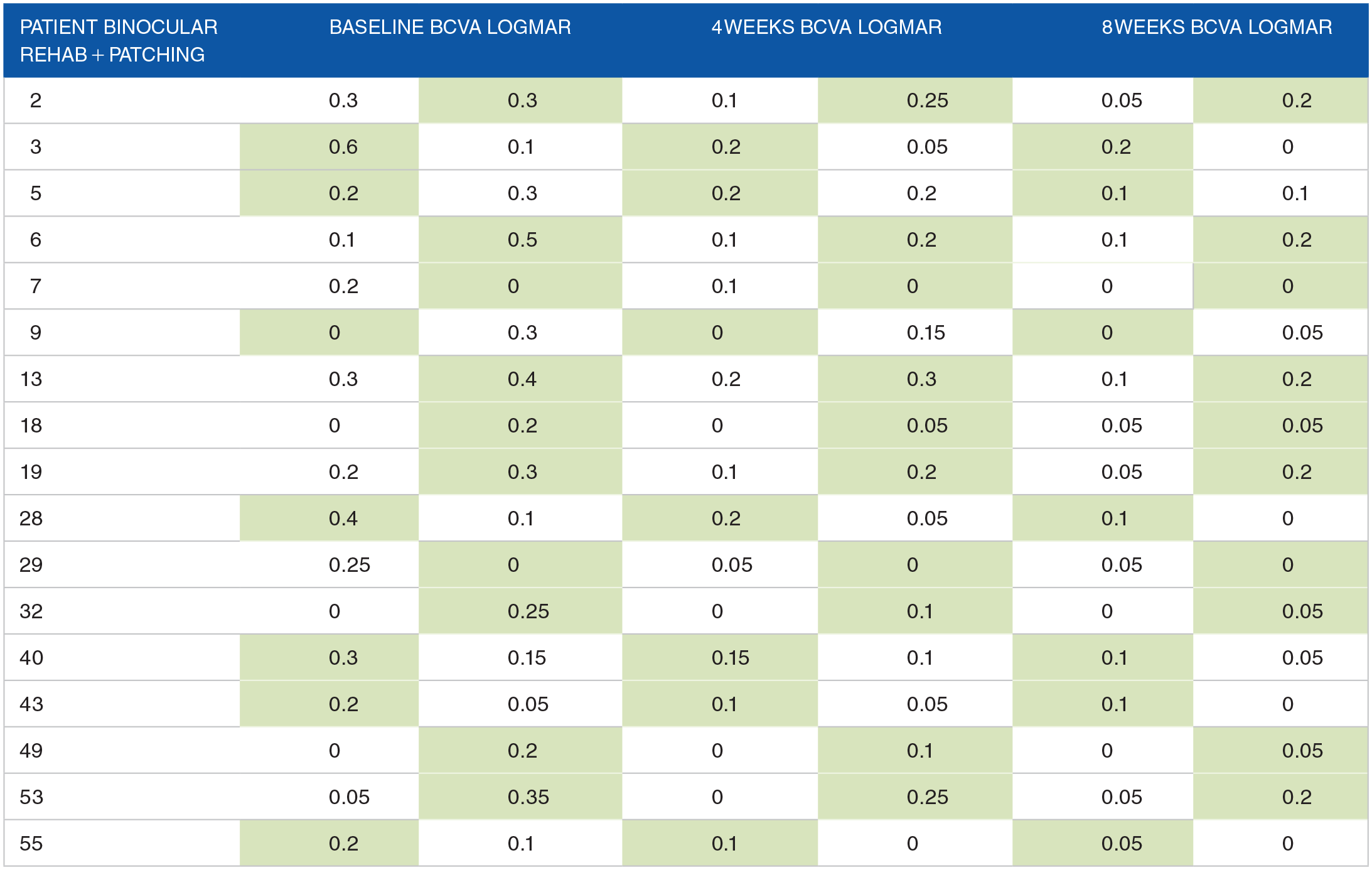
The following tables (Tables 3 and 4) presents data about 2 subgroups. The first one contains patients treated only with dichoptic games, the second one contains patients treated with dichoptic games and patching at the same time. Mean (+SD) BCVA of the amblyopic eyes concerning patients treated only with binocular rehabilitation was 0.28 ± 0.13 logMAR at baseline, 0.13 ± 0.10 logMAR at the 4 weeks outcome and 0.09 ± 0.10 logMAR at the 8 weeks. The mean (+SD) BCVA of the amblyopic eyes concerning patients treated with binocular rehabilitation combined with patching was 0.28 ± 0.11 logMAR at baseline, 0.15 ± 0.07 logMAR at the 4 weeks and 0.10 ± 0.06 logMAR at the 8 weeks.
Baseline, 4 and 8 weeks results, patients with only binocular rehabilitation.

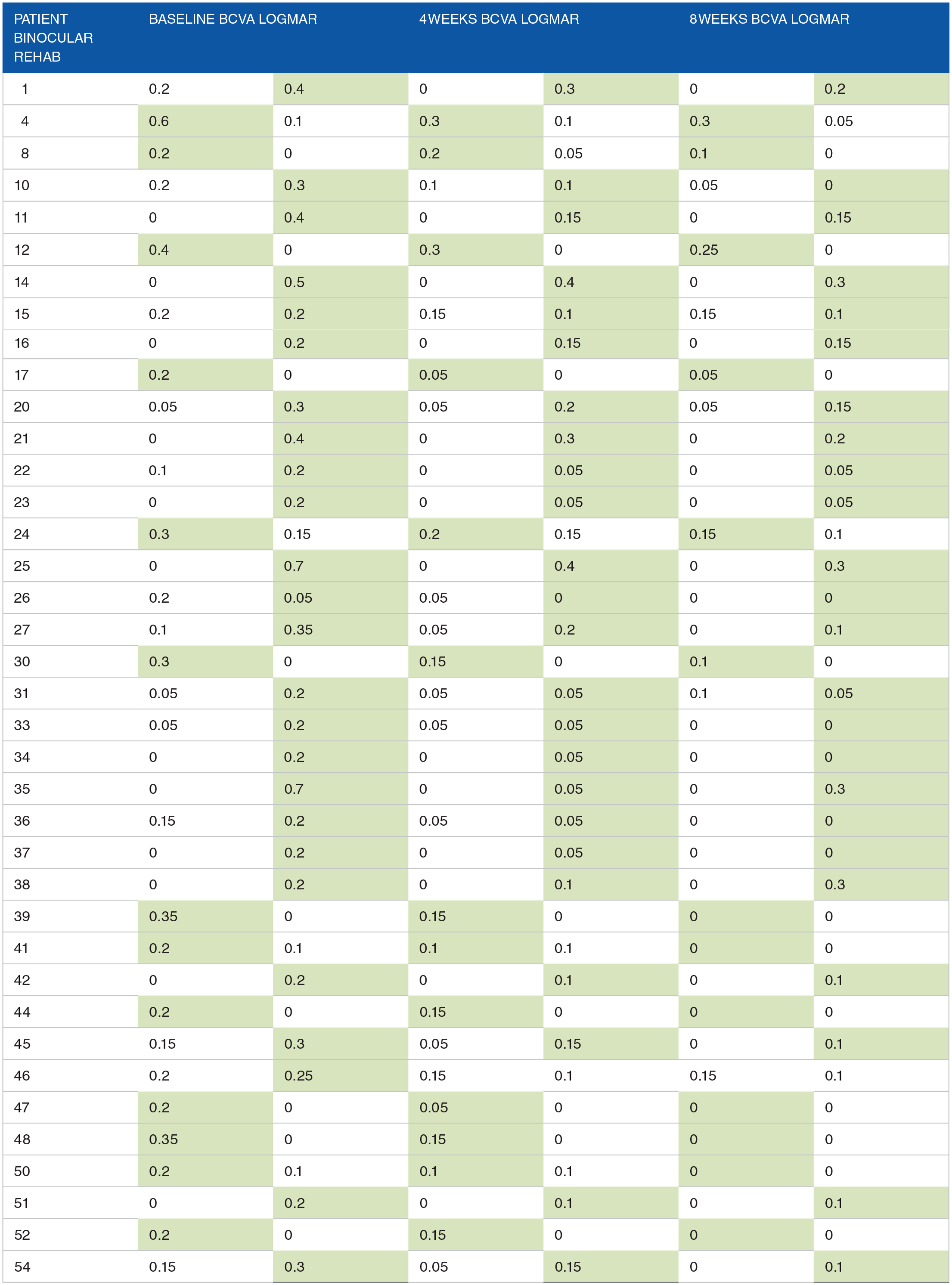
Amblyopic eyes in green.
Baseline, 4 and 8 weeks results, patients with combined binocular rehabilitation and patching (amblyopic eyes in green).

It is evident that an improvement was reached in both groups.
In our view this is an interesting result that gives us a clue of the potential of this rehabilitation approach. The usefulness of this method does not stop at its exclusive use but can also be considered within a combined treatment with classic therapies.
The results data, obtained from the calendar compiled by parents, also showed good compliance. At 4 weeks outcome, 75% of patients (41 children) had a high level of compliance, and 25% (14 children) had a medium level. At 8 weeks outcome, 70% (38 children) of patients had a high level of compliance, 25% (14 children) had a medium level and only 5 % (3 children) showed a low level.
The correlation between compliance level and achieved results, is in favor of patients with higher adherence to rehabilitative therapy. As well as in patching therapy, even in binocular therapy the greater the compliance the greater the results.
Discussion
Revaluing a therapy that has been in use for a 100 years presents many challenges. However, the evolution of science and innovation inevitably supersedes previous discoveries and assumptions. Recent, scientific research relating to the electrophysiological process, paved the way for our chosen approach.6,7,10 Specifically, the approach was based on the presence in amblyopic patients, of a structurally binocular system, that works like a monocular system.
It is well known that binocular cooperation is compromised in amblyopic patients. Nevertheless, actual accepted therapies expect that monocular rehabilitation can be achieved through visual input reduction in the healthy eye. Traditionally, amblyopia is linked to “critical period,” a period in which vision system plasticity should guarantee functional recovery. For this reason, rehabilitation should be performed in patients below 8 or 9 years of age, prior to the maturity of their vision system.
Our experimented treatment has also been effective in patients older than 9 years, with a matured vision system; this supports the presence of a neuronal plasticity that tends to decrease with age but is ever present and then can therefore be exploited.13,14,29
Compliance relating to current therapies does not achieve acceptable levels and often it drastically compromises expected results. 8 Searle et al 19 revealed in their study that only 54% of parents were achieving orthoptists' recommendations to patch their child.
Our aim is to develop therapeutic techniques that could improve compliance and, at the same time, guarantee positive functional recovery results.
Correct communication with parents is fundamental, Emily TC Tan et al 30 provides useful source of inspiration; in their study they wondered: how do parents experience patching or dichoptic action video gaming as amblyopia treatment? They noticed that the gaming group’s treatment responsibility was significantly lower compared to the patching group. Also, parents would like to arrive at a well-informed, shared decision regarding the different type of amblyopia treatment, wherein the healthcare professional discusses organisational aspects of treatment and their child’s traits.
After participating in this study, we recommended that all participants resume any previous therapies.
Limitations
A control group was not provided in this study due to the exploratory nature of the study itself. It was our interest to evaluate the potential of this different approach to better organize a subsequent comparative study between conventional and unconventional treatments. For the same reason we did not focus on the improvement in stereoscopic acuity, which has been evaluated during the first examination. The main outcome we focused on was visual acuity, in order to assess the usefulness of a subsequent study. Moreover, data relating to patching therapy, atropine therapy or other conventional treatments are already present in the literature.
Conclusions
It is important that research and experimentation does not cease at this stage. Larger sample sizes and extended treatment periods must be undertaken, in order to obtain objective data relating to visual acuity maintenance.2,3
The aim of the researchers is not to suggest the ultimate solution to the issue of amblyopia; our mission is to study in depth, as much as possible, every aspect relating to binocular rehabilitation.
To achieve this, sample must be divided by age ranges; into these ranges 2 separated groups, one of which should receive only binocular rehabilitation and the other one should receive only patching therapy, in order to achieve the highest degree of objectivity in results.
Our future intentions are to develop a brand-new App, specially created by vision professionals, who will be able to recognize and improve the critical features of current App available and used in previous studies, to provide a useful and efficient tool for the rehabilitation of amblyopia. This study was designed to test the potential of this technique for the first time in Italy. This also served us, as researchers, to have a direct and effective experience as the starting point for creating a new and optimized App.
Footnotes
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.