
Abstract
Objective
Musculoskeletal disorders (MSDs) include different pathological conditions of the locomotor system, characterized by pain and limitations in mobility and functioning. The most frequent arthropathies include joint disorders and arthritis. Yoga is an ancient mind-body discipline which has received great attention in clinical research. This critical review intends to analyze the updated literature on clinical outcomes of yoga interventions for MSDs.
Methods
Prospective clinical studies evaluating the effects of yoga for MSDs have been searched in Web of Sciences, Scopus and PubMed databases using yoga-related keywords in association with numerous disorders affecting the musculoskeletal system. We explored all protocols to identify similar movements or asana reported with different (uncommon) names or imprecise description, and to be useful for clinicians, we summarized yoga exercises with specific target for body areas and related pathologies.
Results
Overall, 1150 articles were screened, among which 52 prospective clinical studies (total 4151 patients) were selected. The clinical outcomes of yoga were compared with active control groups (rehabilitation, drugs) or passive controls (self-care education or no intervention). The analysis was performed towards specific musculoskeletal disease, affected body area, study type, yoga protocol details, and outcomes in measured and self-reported parameters. All 52 studies showed marked benefits in every or some parameters: measurable outcomes as well as self-reported improvements were higher in yoga groups than in controls, and in some studies even better than drug therapy.
Conclusions
This review highlights the potential benefits of yoga interventions for MSDs. Data highlights that yoga may help improve mobility, reduce reliance on medications, and enhance quality of life and could be considered as a complementary approach alongside conventional medical treatments. However, the heterogeneity of protocols, outcomes, and potential risks of bias highlight the need for rigorous trials to strengthen confidence in these findings and to identify the most effective protocols.
Keywords
Introduction
Important world-leading journals of clinical, public health, and global health knowledge, such as Lancet and BMJ - highlight the pressing issue of population aging 1 and the increasing global burden of musculoskeletal disorders (MSDs).2-4 Recently, the United Nations, European Agency and WHO 5 highlighted this alarming problem. MSDs represent a multifactorial growing worldwide problem and constitute the major cause of disability and limitation of daily working and social life, 6 affecting approximately 1.7 billion individuals worldwide living with pain and limitations in mobility. 2
MSDs include a wide over 150 conditions affecting the locomotor and connective tissue systems. These disorders can be broadly categorized into non-inflammatory and inflammatory types. Non-inflammatory MSDs include chronic back pain (such as low back disorders and neck pain), mechanical joint disorders, scoliosis, osteoporosis, and degenerative conditions like osteoarthritis. Inflammatory MSDs involve autoimmune or systemic processes and include rheumatoid arthritis, gout, psoriatic arthritis, ankylosing spondylitis, juvenile idiopathic arthritis, polymyalgia rheumatica, and lupus. 2
MSDs showed an alarming 123.4% increase of total cases in the last 30 years (1990-2020) 3 due to the rise in sedentary lifestyle and to the demanding strict working conditions aggravated by the aging of the population. 2
In 2020, 494 million of new MSDs cases have been reported and 83 100 of these have been associated with death.
MSDs currently affect around 2 billion people/individuals worldwide 2 and a further 115% increase is expected from 2020 to 2050 to an estimated 1.06 billion new cases in 2050; most regions were projected to have at least a 50% increase in cases between 2020 and 2050. 3
People suffering from joint and musculoskeletal pain and discomfort demonstrate decreased motion and strength, and kinesiophobia, showing a relationship between pain and (causal or consequent) limited/restricted range of motion.7,8 According recent studies and meta analyses, MSDs prevalence is 61% for low back and back pain and spine pathologies, 40.1% for hip soreness/suffering, 7.0% for shoulder pain, and 20.8% for osteoarthritis affliction. 9
The age-standardized global prevalence of MSDs increases with age to a peak at 65-69 years in both females and males and is 47.4% higher in females than in males.
Older people are at increased risk of MSDs.1,10 The proportion of elderly people, that is, persons aged 60 years or older, increased from 8.0% in 1950 to 12.7% in 2017, and is projected to reach 21.3% in 2050.
In this context of expected aging, it becomes a priority to pay attention to MSDs and related disabling conditions with the focus on developing effective policies for their management and prevention. WHO in 2017 launched the “Rehabilitation 2030 Initiative” to draw attention to the worldwide need to enhance prevention and rehabilitation in health systems, and the rehabilitation related to MSDs was among the most pressing needs. 6
In May 2025, the World Health Assembly (WHA) adopted its third global strategy on traditional medicine which will run from 2025 to 2034, envisaging “people-centred TCIM [traditional, complementary and integrative medicine]” following Ministry of Ayush (AYUSH, i.e., Ayurveda, Yoga & Naturopathy, Unani, Siddha, and Homoeopathy) to integrate traditional Indian practices, such as Yoga, into WHO international health intervention classification system. 11
In the last decades, yoga received increasing attention and generated growing relevant medical research demonstrating its clinical effectiveness in many medical domains, in reducing symptoms and associated disabilities in ageing-related or unrelated diseases.12-14 Pioneering Western clinical studies have been published in top-rank medical journals since the 1960s15-23 and emphasized the need to prescribe yoga and meditation to patients for well-being, healthy ageing12,17,24 and healthcare. 25
Yoga is an ancient traditional school of philosophy and practice assumed to have originated in northern India at least 2000 years ago. Historical evidence of the existence of yoga was seen in the pre-Vedic period (2700 B.C.), and thereafter till Patanjali period. Yoga is a mind-body practice involving deep concentration (dharana) with inward focusing (pratyahara, bringing the attention inwards), controlled/volitional breathing (pranayama), postures and mindful movements encompassing stretching and strengthening poses (asana), and meditation (dhyana) (Patanjali. Yoga Sutras, 200 BCE-200 CE; Krishnamacharya T. Yoga Makaranda, 1934; Iyengar BKS. Light on Yoga. New York: Shocken Books, 1979; Pattabhi K Jois. Yoga Mala. New York: North Point Press, 2002; White DG Yoga, Brief History of an idea. Princeton, 2011; Mallinson J, Singleton M. Roots of Yoga. Book Review, 2017; Eliade M. Yoga: Immortality and Freedom. Book: Princeton University Press, 1954).
Yoga protocols showed significant effectiveness for cardiovascular risk factors and pathologies, 26 gastrointestinal diseases, 27 pulmonary function such as hypoxia, hypercapnia18,19 and asthma,16,18 spine disorders28-31 carpal tunnel syndrome, 20 chronic low back pain,21-23 knee osteoarthritis, 32 balance and mobility in older adults, 33 physical function, 7 mental well-being and quality of life,34,35 cognition, 36 and for frailty and disability in older people. 37 Significant clinical evidence has also been demonstrated for psychological health, 24 side-effect management of cancer therapies, 14 depression, 34 anxiety,32,36 and perceived stress.32,36
This critical review intends to analyze and summarize the clinical evidence of yoga interventions for various MSDs to consider the possibility to use yoga as a complementary therapy and in some cases even as an alternative therapy in medical care. The ultimate purpose of this study is to outline the effects of yoga interventions for clinicians, academics and researchers, in particular physiatrists, orthopedics, neurologists, geriatrists, rheumatologists, sports medicine specialists, and physiotherapists.
Materials and Methods
Search Strategy
A comprehensive manual search was carried out in electronic databases (Web of Sciences, Scopus and PubMed) by a combination of relevant keywords and MeSH (Medical Subject Headings) terms. Two authors independently read and selected the articles from May January 2023 to November 2024. Any difference in search results were resolved through discussion or consultation with a third reviewer.
Articles search has been performed for the different body areas and related disorders using the following keywords: “Yoga”, “Yoga techniques”, “Yoga therapy”, “Yogasana”, “Asana”, “Pranayama” and “Yogic breathing” in association with: 1. (for neck and head): Neck Pain, Neck Disorders, Tension headache; 2. (for shoulder, upper back, hand, wrist): Thoracic outlet syndrome, Frozen shoulder, Disk herniation and bulging, Upper crossed syndrome, Shoulder pain, Subacromial impingement, Supraspinatus syndrome, Entrapment syndrome, Carpal tunnel, De Quervain syndrome, Tendinosis, Tenosynovitis; 3. (for low back, hip, leg): Low Back Pain, Lumbar disc herniation, Spinal disk pathologies, Ischiofemoral Impingement, Femoroacetabular impingement, Piriformis syndrome, Hip impingement, Hip osteoarthritis, Hip pain, Hip extension and gait function, Patellofemoral Pain Syndrome, Knee disorders; 4. (for arthritis): Osteoarthritis, Inflammatory Arthritis, Nontraumatic Arthritis, Chronic Hand Osteoarthrosis, Hip arthritis and Knee arthritis.
The search strategy is reported in Table S1 supplementary material.
Eligibility of Retrieved Studies
Inclusion Criteria
Population: subjects with MSDs; Intervention: Yoga therapy; Study type: clinical prospective; Primary Outcomes: studies analyzing self-reported outcomes (such as pain, quality of life or disability) and/or measured parameters (e.g., articulation movement, strength, disability score, muscle electromyography, muscle thickness, inflammatory markers and immunological parameters, drugs assumption); Language: Full articles in English.
Exclusion Criteria
Studies were excluded if they were reviews, case reports, case series, or retrospective studies due to the lack the methodological rigor and generalization. Articles without clinical data, incomplete results, or available only as abstracts were also excluded due to insufficient information for critical analysis and data extraction. Additionally, studies published in journals not indexed in recognized scientific databases were excluded to ensure the quality of the included literature.
Data Analysis
For each included clinical study, the following parameters were analyzed and summarized in detailed tables: Disease; Study type (RCT, Prospective, Pilot); Number of patients, age range and mean age; Yoga session duration and frequency; Study duration; Presence and type of a control group (active or passive); Main findings (objective or subjective outcomes); Benefits: yes (Y, statistically different improvements in yoga group compared to control group) or not (N, control group showed significant improvement compared to yoga group) or partial (some parameters significantly improved in Yoga group compared to control group) or similar (similar improvements in both yoga and control group) to the control; Yoga style; Yoga intervention that is movements (asana), breathing exercises (pranayama), relaxation techniques; Qualifications of yoga instructors. Yoga protocols have been reported in the tables without any change in sequences and (Sanskrit or English) asana names, despite sometimes written in an unusual way. Adverse reactions to yoga protocols were also accounted and divided in accordance to each paper definition as minor events (i.e., muscle pain, dizziness or nausea) or adverse events (i.e., herniated disk, muscle trauma or injury) or not reported (when no explicitly stated in the text).
Methodological Quality Assessment of Studies
Randomized clinical trials were assessed using the Cochrane Risk of Bias (ROB), evaluating 5 domains: D1: Random sequence generation (selection bias); D2: Allocation concealment (selection bias); D3: Blinding of participants and personnel (performance bias); D4: Blinding of outcome assessment (detection bias); D5: Incomplete outcome data and selective reporting (attrition/reporting bias). Each domain was judged as either low risk (“+”), high risk (“−”), or some concern (“!”), based on the level of methodological detail provided in each study.
Prospective studies were assessed using the Newcastle-Ottawa Quality Assessment Scale (NOS). The NOS assesses 3 main domains: Selection of study participants (maximum 4 points), Comparability of study groups (maximum 2 points), Outcome assessment (maximum 3 points). Each domain includes specific criteria, and a star (*) is placed for each criterion met. A maximum of 9 stars can be awarded in total. Based on their total NOS scores, studies were categorized as follows: High quality: 7-9 points, Moderate quality: 4-6 points, Low quality: 0-3 points.
Results
A total of 1506 articles were found. After duplicate removal (n = 356), a total of 1150 full articles were screened. Papers not in the English language (n = 86), reviews (n = 150), articles with incomplete results (n = 96), abstract available only (n = 46), and papers not indexed in scientific databases (n = 158) were excluded. An additional 562 articles were removed as not analyzing yoga interventions (n = 450) or being case reports or case series (n = 112). A representative flowchart of search analysis is reported in Figure 1. Flowchart of Study Identification, Screening, and Inclusion in the Review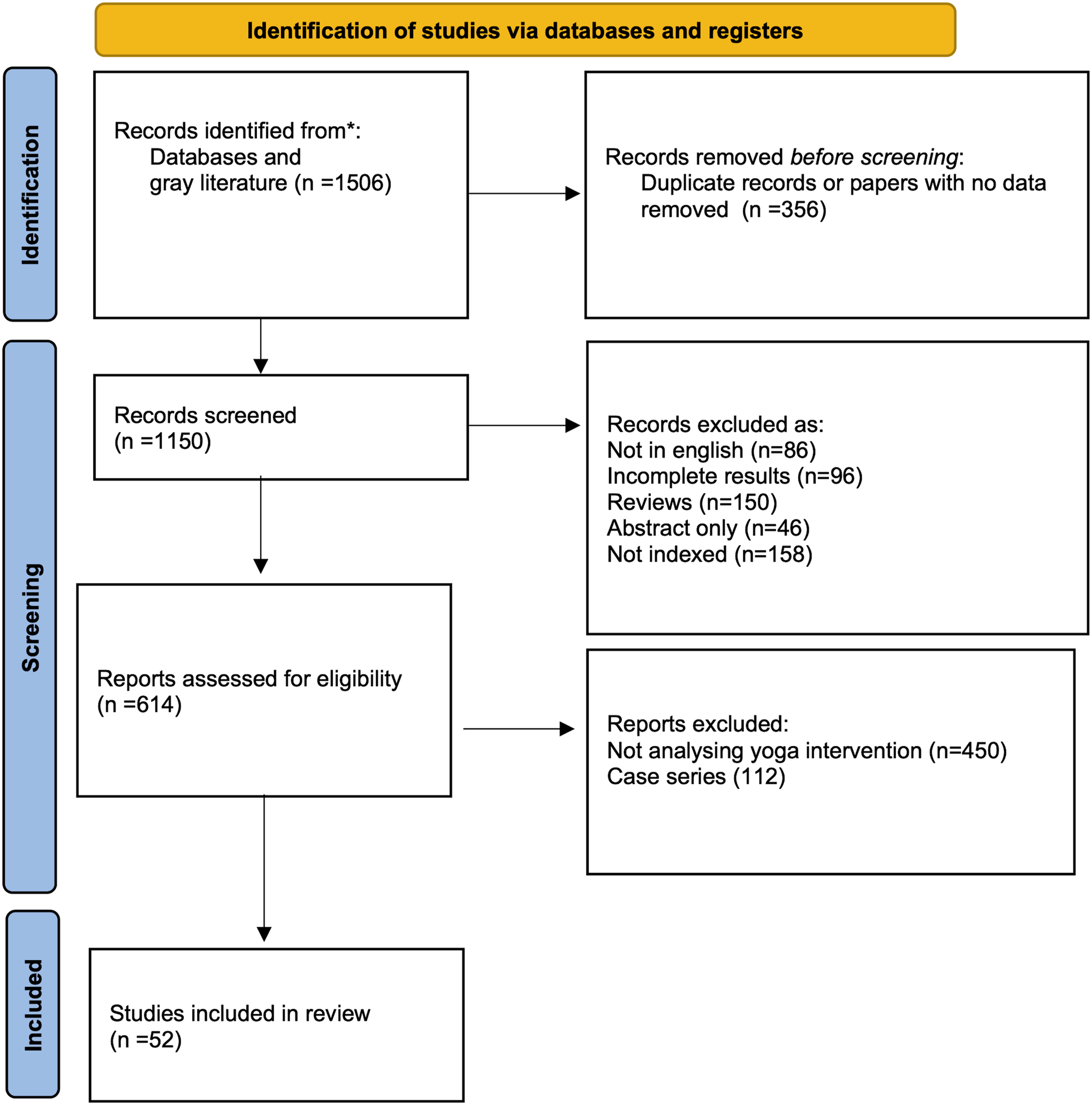
Overall, 52 prospective clinical studies (46 randomized and 6 prospective non-randomized) were included (total 4151 patients).21,22,24,38-83
A critical analysis of the similarities and differences in postures and yoga techniques used in different studies and protocols for similar MSDs in analogous body areas is presented in the discussion section and summarized in Table S2 supplementary material.
Head MSDs
Effect of Yoga For Head and Neck MSDs

Yoga For Head and Neck MSDs

3/6 studies (241 patients) showed significantly higher (P < .050) effect/relief for headache than drugs (Nonsteroidal Anti-Inflammatory Drugs, NSAIDs, analgesics) in terms of duration, frequency, intensity, anxiety and depression scores, disability and quality of life (Tables 1a and 1b).
However, 3 studies specified tension headache38-40 while 3 studies vaguely reported migraine.41-43 Then, the data of 3 migraine studies (280 yoga group and 120 controls) have been excluded from the Tables 1a and 1b despite muscular tensions and stress are frequent trigger and coexisting factors.84,85
Neck Pain
Five studies (278 patients) on neck pain were analyzed.31,44-47 Four of five studies reported greater improvements (or similar effects in 2 studies) in muscle thickness, disability index, range of motion, sympathetic activity, sympathovagal tone, pain during movement, depression, and quality of life compared to stretching or Pilates (Tables 1a and 1b). Most studies provided detailed protocols with multiple asana, including their repetitions and duration; one study described only 5 asana (Table 1b). Control groups were mainly active (e.g., stretching or Pilates) which can make it appear less effective the observed benefits. Both objective measures (e.g., semispinalis capitis thickness, range of motion) and subjective measures (e.g., pain, quality of life, social functioning) were assessed. Yoga for neck pain showed greater benefits in both measurable outcomes and self-reported improvements than conventional exercises (Table 1a).
Three studies reported some minor adverse effects occurred in yoga group: Kim et al 45 reported 3 minor episodes of dizziness during neck-movement work, Cramer et al 47 reported 11 minor complaints (8 pain increases and 3 limb pain, migraine and vertigo events) and Michalsen et al 31 recorded 1 minor complain (transient mild low-back pain). No serious injuries occurred. It is important to note that one study explicitly reported 0 adverse events, 44 while in another one, no mention was given. 46
In detail, the analyzed studies showed important clinical outcomes with significant improvements (P < .050) in self-reported headache duration, 39 frequency,39,41-43 intensity,42-44 self-reported pain, pain rating index, 41 self-reported anxiety and depression scores,41,46 self-reported headache disability,42,45 self-reported quality of life, decrease of temporalis muscle activity 40 and semispinalis capitis muscle thickness, 46 decrease in symptomatic medication use 41 and pill count 42 decrease in heart rate, 44 sympathovagal tone and sympathetic activity. 44
Shoulder Pain
Effect of Yoga for Shoulder, Hand and Wrist MSDs and Upper Crossed Syndrome

Similar: Improvement similar to the control; Partial: improvement in some parameters compared to the control.
Yoga For Shoulder, Hand and Wrist MSDs and Upper Crossed Syndrome

Hand Disability
Six studies (963 patients) on hand disability were analyzed.20,55-59 Three studies did not specify asana names or detailed protocols,57-59 while one study tested only Shavasana. 56 Control groups included rehabilitation programs or no intervention, introducing variability. Objective measures such as nerve conduction and handgrip strength were often combined with self-reported outcomes. Four of six studies reported significant improvements (handgrip strength and endurance, flexion test, sensory and motor nerve conduction, systolic and diastolic blood pressure, pulse rate), with effects comparable to surgical intervention in 1 study and partial benefits in one Hatha yoga trial with limited asana (Table 2a). No yoga-related adverse effects were reported (Table 2b). Yoga for wrist pain produced greater improvements in measurable outcomes (e.g., mobility tests, grip strength and endurance, nerve conduction time, motor speed, diastolic blood pressure) and self-reported pain compared to rehabilitation or no intervention.
Back Pain and Disorders
Effect of Yoga For Spine, Hip and Leg-Knee Disorders and Pain

Similar: Improvement similar to the control; Partial: greater improvement in some parameters compared to the control.
Yoga For Spine, Hip and Leg-Knee Disorders and Pain

These events were generally minor and infrequent, including transient muscle pain or discomfort.23,64,69,70 Two studies reported disk herniation.23,28
The effectiveness of yoga protocols was assessed against various controls, including conventional therapeutic exercises (stretching)23,65,69-71 education/counseling/self-care,23,63,64,67,70,71 and pharmacological treatments (NSAIDs, acetaminophen, opioids, muscle relaxants) in one study with 90 patients 28 (Table 3a). Two studies compared yoga to unspecified standard/usual care,66,68 and one study lacked a control group. The heterogeneity of control interventions -from educational programs (passive) to drug therapy (active) - may influence the perceived benefits. Both objective outcomes (e.g., biomarkers, spinal mobility) and subjective outcomes (e.g., pain, stress) were evaluated.
All the studies reported significant benefits (P < .050) resulting from the yoga therapy, just 1 study (228 patients) 23 of them reported a partial improvement (P > .050) and 2 studies (97 patients)67,72 found similar benefits to controls (Table 3a).
Disk Herniation
Three prospective clinical trials (281 patients) on yoga for spinal disc diseases reported greater benefits for pain and disability compared to education or no intervention (Table 3a). One study noted minor adverse events, including transient muscle pain, an ankle sprain, and a gluteal sprain (Table 3b). 60 One study 71 explicitly stated that no adverse events occurred, whereas another 1 study did not provide any information regarding adverse events. 30
Control groups consisted of education or no intervention, representing passive comparators. Objective measures such as pain scores and functional tests were complemented by self-reported outcomes. In one study, the asana details (Sanskrit name or clear posture description) were not reported, 62 while the other 2 provided detailed protocols with multiple asana targeting low back mobilization.60,61 Yoga protocols were compared with education 60 or no intervention, 62 while 1 study lacked a control group. 61
Hip and Leg-Knee Disorders and Pain
We found 6 randomized clinical articles and 2 prospective studies, with a total of 569 subjects (327 yoga group, and 242 controls) (Table 3a).30,32,72,77
Two studies on hip pain (total 63 patients) were analyzed;30,72
The protocols were deeply detailed and included a wide explanation of performed asana. Only minor yoga adverse effects (transient leg discomfort) were reported in one investigation (Table 3b). 72
All reported greater benefits resulting from the yoga therapy, just 3 studies of them reported a partial (non-significant P > .050) improvement (154 patients) (Table 3a).
2/2 studies showed significant improvements (P < .050) of flexibility (split and hip extension), balance, stiffness, and some reduction of pelvic ante-version in addition to significant improvements of self-reported physical and psychological parameters (Tables 3a and 3b). The studies used active controls (e.g., physiotherapy) and passive comparators. Both measurable outcomes (e.g., flexibility, osteoarthritis index) and subjective assessments were reported.
Six studies (total 506 patients) on knee pain and disability were analyzed32,73-77; The intervention protocol was detailed in 5 studies, while one trial did no report asana names and the description of the protocol was vague. 74 Minor adverse reactions (13 patients with transient muscle pain) were recorded in just one investigation. 32 One study explicitly stated that no adverse events occurred, 73 while 4 studies did not provide any information regarding adverse events.74,76,77
4/6 studies reported significant betterments of stiffness and flexibility (2/6 studies), walking and physical performance, osteoarthritis index, in addition to significant improvements of self-reported parameters and psychological health (Tables 3a and 3b).
Generalized Arthritis
Effect of Yoga For Generalized Arthritis

Similar: Improvement similar to the control; Partial: greater improvement in some parameters compared to the control.
Yoga For Generalized Arthritis

In arthritis studies, the control groups were predominantly active pharmacological treatments (Disease-Modifying Antirheumatic Drugs, DMARDs), which may have masked part of yoga’s effects. Objective outcomes such as inflammatory markers were evaluated alongside self-reported pain and mood improvements (Table 4a).
Yoga practice for 6-12 weeks produced significant improvements of self-reported pain, swelling, fatigue, mood, and induced a significant reduction of inflammatory markers.78-83 All the studies reported significant benefits resulting from the yoga therapy. In detail, 4/6 studies reported significantly higher benefits vs antirheumatic drugs DMARDs (Table 4a), namely reduction of inflammatory markers (2/6 studies), amelioration of disease activity or clinical disease (2/6 studies) and increase of mind-body communicative markers (1 study) (Tables 4a and 4b). Only one study (n = 26 patients) found similar benefits to the pharmacological-treated controls. Better improvements than educational group 78 or no intervention. 82
Methodological Quality Assessment of Included Studies
Risk of Bias (ROB) Assessment of the Included Randomized Clinical Trials


D1 = Randomisation process; D2 = Deviations from the intended intervention; D3 = Missing outcome data; D4 = Measurement of the outcome; D5 = Selection of the reported result.
Green Circle = low risk of bias; Yellow Circle = some concerns; Red Circle = High risk of bias.
In contrast, D1 (random sequence generation) consistently rated in most of the study as low risk. It should be noted that D2 (allocation concealment) was often underreported. Concerning missing outcome data (D3), very low drop rate was observed in most of the studies. The full evaluation data are reported in research data section (Table S3 of Supplementary materials).
Newcastle - Ottawa Quality Assessment Scale of the Included Prospective Studies
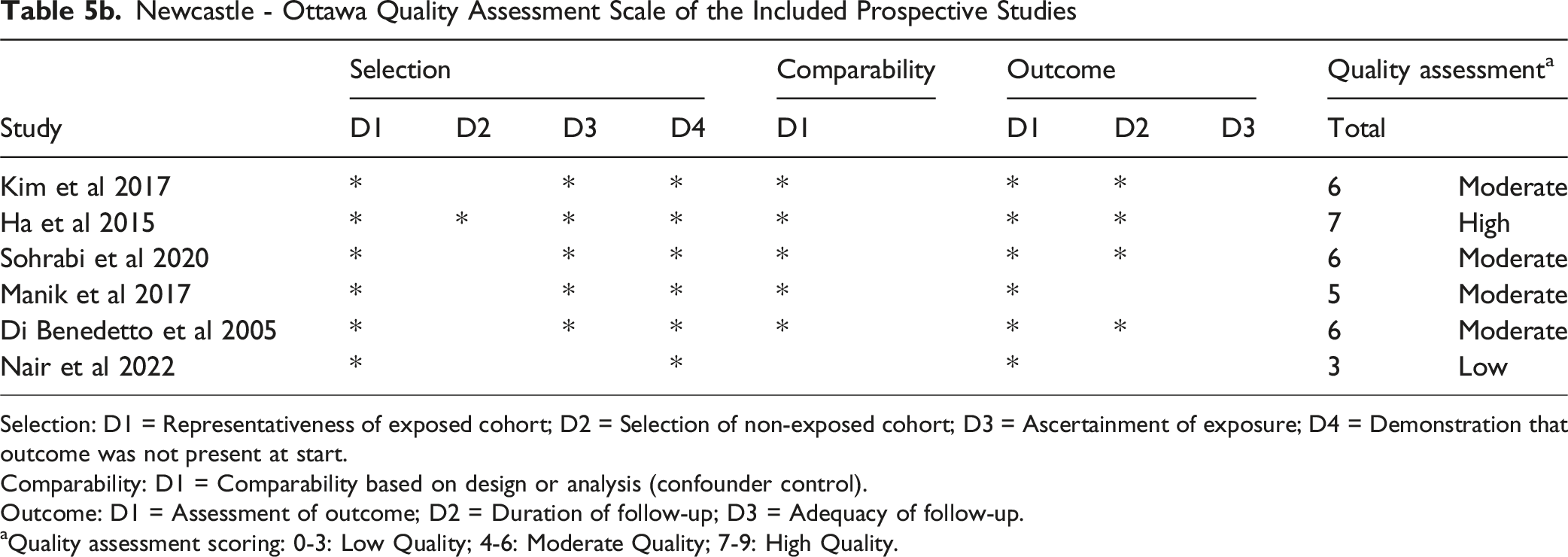
Selection: D1 = Representativeness of exposed cohort; D2 = Selection of non-exposed cohort; D3 = Ascertainment of exposure; D4 = Demonstration that outcome was not present at start.
Comparability: D1 = Comparability based on design or analysis (confounder control).
Outcome: D1 = Assessment of outcome; D2 = Duration of follow-up; D3 = Adequacy of follow-up.
aQuality assessment scoring: 0-3: Low Quality; 4-6: Moderate Quality; 7-9: High Quality.
Discussion
This review examined the clinical effects of yoga interventions for MSDs and pain in prospective and randomized clinical studies. The analysis focused on specific factors such as specified musculoskeletal diseases and pain conditions, details of yoga protocols, and reported benefits including both measured parameters and self-reported outcomes (e.g., pain, disability, mobility test, quality of life). The summary of the clinical results/outcomes emphasized an updated effectiveness of yoga interventions for musculoskeletal disorders and pain.
Yoga comprises the physical practice of yoga (asana) and relates to the body. Asana practice focuses on the physical aspect of yoga, consisting of performing yogic postures related to awareness, concentration, control, balance, flexibility and endurance. Yoga asana involve deep/intense postures and movements and myofascial stretching in which the entire muscle-tendon system included myofascia subcategories (perimysium, epimysium and endomysium) are stimulated.
These postures of deep stretching exert a renewal action by a squeezing effect 86 with circulation and renewal of biological fluids, dehydration-rehydration alternance, removal of catabolites and supply of nutrients and growth factors, towards “sponge-like” connective tissues (muscles, tendons, ligaments and fascia). The biological effect on tissues depends on the accuracy, intensity, frequency and duration of asana practice and on histological characteristics related to age, sedentary/active lifestyle and dietary habits.72,87-89
This review showed that yoga appears to be effective to reduce musculoskeletal symptoms and pain. The biological rationale of yoga effectiveness is related to the physiological recovery of joint mobility and intra-articular spaces, and the softening and lengthening of stiff and retracted muscle-tendon-ligamentous structures.90-93 This is likely a feasible explanation for every musculoskeletal area. Then, effective yoga protocols involving specific movements and exercises targeted to progressive stretching and strengthening in selected body areas94,95 and achievement of maximum biomechanical range of motion useful to reverse or reduce states of pain and/or reduced mobility.
Emblematic principles of yoga as conservative therapy for the treatment for musculoskeletal pain and disabilities94,95 involve several aspects: i. the recovery of mobility in all spatial directions and restoration of intra-articular spaces; ii. the reestablishment of spinal lordosis and the reduction of intervertebral pressure on the discs for neck and back pain; iii. the downgrading of intra-acetabulum pressure and the reduction of traction and compression forces towards the acetabular labrum together with the recuperation of lumbopelvic rhythm and pelvic tilt by improvement of nutation and counternutation movements, spinal lordosis for hip pain; iv. the recovery of shoulder joint and scapula mobility, the downgrading of intra-glenohumeral pressure at shoulder joint and the reduction of traction and compression forces towards the acromion or glenoid cavity for shoulder pain.
Yoga may also influence the main factors that maintain chronic musculoskeletal pain, such as increased pain sensitivity (inflammation and central sensitization),79,80,96 negative emotions (depression, anxiety, stress), fear of movement (kinesiophobia), 65 and low confidence in managing pain (confidence in self-efficacy). Yoga combines gentle and progressive movements, controlled breathing, and mindful attention, which can help calm the nervous system, reduce stress, and improve pain tolerance. 94 Some studies have shown that yoga can lower pain-related fear and negative thoughts, improve mood, and increase confidence in daily activities.32,34-36
We elaborated the following consecutive cause-effect and/or intercorrelated events in MSDs affected area. Disuse, and lack of movement reduce blood afflux & circulation, with low nourishment/nutrients supply, O2 deficiency & increased CO2 (local acidosis) and catabolites. Prolonged disuse for kinesiophobia reduces mobility and causes tissue contraction and stiffening with consequent joint compression, reduced joint range of motion, growing disability and decreasing day life autonomy.94,95
We highlight that asana involves deep movements and represents the key to induce biological changes (both histological and anatomical) with following effects on the histological tissues (muscles, tendons, ligaments and fascia) and restoring physiological kinesiology (the range of movement spontaneously increase in intensity with practice - allow a gradual and delicate self-rehabilitation).
We underline that in tissues subjected to stretching, a significant regulation of oxidative stress and expression of pro- and anti-inflammatory genes and mediators occurs, a remodeling of the extracellular matrix expressed by changes in collagen and matrix metalloproteinases levels, an increase of microvascular volume, number of capillaries per muscle fiber, levels of hypoxia-inducible factor 1, vascular endothelial growth factor and nitric oxide synthetase.
Stretching and relaxation exercises such as yoga lower stress levels, enhance the immune response, reduce circulating IL-6, and increase anti-inflammatory IL-10 levels. 96
These effects, together with its physical benefits, help explain why yoga is effective across different musculoskeletal conditions, even when compared with active treatments such as exercise or physiotherapy.
The authors of this review wish to emphasize the importance of the protocol details for the relevance of a study. Some studies included in this review underestimated the importance to show asana images or to describe unequivocally and in detail each posture inserted in the protocol, preferably also including the Sanskrit name. It was unexpected that even when designed by yoga experts, in some studies protocols were not detailed or imprecise, likely because they are not scientists or researchers, bringing out the need to have authors who are both practitioners and researchers (academic research scientists). It is highly recommended for future studies to a adopt a minimum standard checklist yoga-specific extension reporting detailed lists of asanas with their names, repetitions, duration, sequencing, as well as breathing and relaxation components (e.g., our proposed parameters template tables). In addition, most of the discussions in the analysed papers are short or very short and just compare the obtained clinical outcomes with the results of previous studies. Many of the analyzed studies do not include comments on the physiological response or biological events related with yoga practice that could have supported and allowed to identify the physiological mechanisms and interpret the clinical outcomes and the rationale of yoga interventions.
In this review, the analysis of the yoga protocols has been challenging as looking for analogies of asana and for the comparability of protocols in terms of frequency and total duration. Asana and yoga techniques reported in the selected studies were often indicated with different (uncommon) names or imprecise description. Then, a great effort was made to identify equal or similar asana in the various protocols. The detail of the Sanskrit asana name or its English translation/description is important for the precise/unequivocal identification of a posture. We explored all protocols to identify same movements or asana reported with different names. Then, for clinicians practical use, we summarize below yoga exercises specifically targeted for body areas and related pathologies. There are different parameters to take into consideration in order to analyze and interpret the effects of yoga asana over time. Specifically, asana practice with equal total minutes of execution is not the same when the practice is short and frequent or long and deferred over time. In addition, also the accuracy and intensity of asana execution (the movement should be gently and gradually forced) have a great effect on clinical results and benefits for MSDs.
Yoga For Headache and Neck Pain
This review highlights that yoga for headache and neck pain supplied more improvements of both measurable outcomes and self-reported improvements than drugs or self-care of control group. Yoga showed benefits in both tension headache and migraine as both neck-related headaches.84,85
Neck pain is a prevalent neurologic and musculoskeletal complaint in the general population and is often associated with primary headache disorders such as migraine and tension-type headache. A high rate, ranging from 73% to 90%, of people with migraine or tension-type headache have coexisting neck pain, and there is a positive correlation between headache frequency and neck pain. Furthermore, neck pain has been identified as a significant risk factor for migraine and tension-type headache.84,85
Comments or speculations on the biological effect of yoga on pathophysiological mechanisms have been expressed just in 3 studies40,41,47 suggesting that yoga may alleviate symptoms and pain, and modulate stress responses through integrated physiological mechanisms as modulation of autonomic and neuroendocrine response, neck spine mobilization and decompression, release of neck muscles.40,41,47,84
Cramer et al suggested that yoga postures can be seen as a form of isometric muscle training, involving prolonged static muscle contractions and increasing cervical proprioceptive acuity. 47 Yoga also was able to increase awareness of muscle tonus and joint position and is also thought to help in recognizing and changing habitual patterns of posture and muscle tension in daily life. 42
John et al proposed that yogic breathing modulates autonomic and neuroendocrine responses and calming the stress response contributing to a state of calm alertness through the enhancement of parasympathetic drive. 40
Kumar et al suggested that the mechanism of reducing headaches symptoms of yoga postures is related to the increase of vasovagal tone, to the shift on a parasympathetic drive and the potential increase of nitric oxide levels, an endothelium-derived relaxing factor-like substance. 41
We want to draw attention that nowadays lifestyle never requires looking upwards and not even to extend your neck, and intense rotation is rarely necessary. Therefore, yoga protocols for neck disorders involve mainly asana in extension and passive flexion to release the stiff (and painful) posterior neck and nuchal muscles, to mobilize and decompress spine discs. 93 As further support, a recent study clearly demonstrated that ergonomic interventions (specifically neck and core combined stabilization practices) improved pain, disability and strength in patients with chronic non-specific neck pain. 97
Yoga practices in various protocols for head and neck have been interpreted (to overcome the inhomogeneous names and definitions) and condensed in Table S2 specifically elaborated for clinicians to simplify/facilitate and encourage their use. Asana for cervical flexion and extension (forward, lateral and right/left) and rotation (right/left) have been then highlighted: -Asana involving active or passive neck extension (in some associated back extension) reported in many protocols are Bhujangasana, Ustrasana, Ardha Chakrasana, Dhanurasana, Matsyasana, Salabhasana. -Asana requiring passive neck flexion were in protocols including forward flexions of the trunk as Adho Mukha Svanasana, Padahastasana or Paschimottanasana or Uttanasana, or Shashankasana (or Balasana or Apanasana), Setu Bandhasana (or Sarvangasana or Viparita Karani). -Asana with neck rotation were present in many protocols, such as Trikonasana (or Parsvakonasana), Vakrasana, Bharadvajasana, Virabhadrasana II, and Ardha Matsyendrasana. -Generic neck rolls (Greeva Sanchalana) and flexion/extension are reported in 2 studies. -Just 1 protocol included Suryanamaskar and 2 protocols enclosed Pavanmuktasana.
Yoga For Shoulder and Wrist-Hand Pain, and For Upper Crossed Syndrome
This review suggests yoga for shoulder and wrist-hand musculoskeletal-related pain provides greater benefits of both measurable outcomes and self-reported pain conventional stretching, exercises, rehabilitation or even NSAIDs.
Interestingly in frozen shoulder, yoga asana significantly improved shoulder abduction, shoulder flexion, and shoulder internal rotation compared with physiotherapy control group, 48 and similar valuable improvement of yoga in self-reported pain and disability scores compared to the control group receiving NSAIDs and physical therapy. 49
For shoulder pain, sauna yoga significantly improved balance abilities and self-reported quality of life (but no significant improvements of lateral flexibility of the spine, shoulder flexibility, strength in lower extremities as we can expect following a low number of asana and intensity of practice), 50 and also yoga induced significant improvements in self-reported pain in shoulder and arm. 51 Satyananda yoga significantly reduced pelvic obliquity and improved lumbo-pelvic posture, and increased strength in shoulder abduction in both affected and non-affected arms. 51 Hatha yoga exercise markedly affected plasma biomarkers, with a significant decrease of malondialdehyde reflecting reduction of oxidative stress and a significant increase of superoxide-dismutase antioxidant enzyme activity. 52
Iyengar yoga intervention for upper crossed syndrome led to a significant increase in the cervical and shoulder angles, and a significant decrease in thoracic flexion angle. 54
Hatha yoga for carpal tunnel syndrome induced self-reported pain reduction, improvement in grip strength, and in Phalen sign (Wrist Flexion Test); no differences were reported in self-reported sleep disturbance, Tinel sign, sensory and motor nerve conduction time compared with wrist splint in controls. 55
Interestingly, it has been speculated that the effectiveness of joint mobilization in individuals with carpometacarpal joint osteoarthritis may exert its effects through a neurophysiological rather than a biomechanical response, and also suggested that supraspinal pain-inhibitory areas, including the periaqueductal gray matter, can be stimulated by joint mobilization. 98
In handgrip strength in patients with stroke, hatha yoga decreased significantly the systolic blood pressure, while the diastolic blood pressure decreased but not significantly. Hand grip strength improved significantly in both unaffected and affected hands. The control group showed no significant change in systolic or diastolic pressure, and no significant change in grip strength for both hands. 56 Yoga induced a significant increase in pulse rate and blood pressure following the handgrip test, 57 a significant increase in hand grip strength and hand grip endurance compared with control, 58 and a significant increase in motor speed in repetitive finger movements of patients with hand rheumatoid arthritis. 59
Varied shoulder joint and arm(s) movements are omnipresent movements in yoga protocols, namely vertical flexion or hyperflexion, vertical hyperabduction, extension or hyperextension with external rotation or medial rotation, horizontal and inferior abduction (in standing, sitting, kneeling or supine position).
Yoga practices and joint movements in various protocols for shoulders and wrist-hand pain, and for upper crossed syndrome have been interpreted (to overcome the inhomogeneous names and definitions) and condensed in Table S2 specifically elaborated for clinicians to enable their use. Yoga interventions involve: -Vertical flexion or hyperflexion of the shoulder w/wo external rotation or medial rotation is involved in Urdhva Hastasana, Ardha Chakrasana, Virabhadrasana I, Utkatasana, Vrksasana, Adho Mukha Svanasana, Parivrtta Parsvakonasana, Astha Chandrasana, Anjaneyasana, Dandayamna Bharmanasana, Shashankasana, Darmikasana, Adho Mukha Svastikasana, Gomukhasana (Gomukhasana involving the complex and compound movement of external rotation & abduction (for upwards arm) + internal rotation and adduction (for downward arm). -Extension or hyperextension with abduction or adduction and external rotation or medial rotation is performed in Dwikonasana, Purvottanasana, Setu Bandha Sarvangasana, Viparita Karani, Halasana, Marichyasana, yoga Mudrasana, Matsyasana, Salabhasana. -Abduction, Hyperabduction, horizontal and inferior abduction is practiced in Tadasana, Tiryaka Tadasana, Ardha Kati Chakrasana, Kati Chakrasana, Garudasana, Virabhadrasana II, Parivrtta Trikonasana, Vasisthasana, Supta Matsyendrasana, Parivrtta Pashimottanasana.-Circumduction is carried out in Skandha Chakra.-Generic neck rolls (Greeva Sanchalana) and shoulder circles (Skandha Chakra) are reported in 3 studies.
Shoulder pain and disabilities are mainly related to joint compression, reduced mobility, and impingement. Joint compression may arise from retracted or stiffened musculotendinous unit-ligament complex. Key points of yoga treatment for shoulder pain are asana involving glenohumeral joint mobility, and their practice with intense movement. 90 In yoga asana, movements and postures involving arms flexion and extension - which spontaneously increase in intensity with practice - allow a gradual and delicate self-rehabilitation. Shoulder extension movements such as (hyper)extension with abduction and external rotation or with adduction and medial rotation (as in Gomukhasana, Parsvottanasana, Kati Chakrasana, but also Garudasana and Purvottanasana) appear to create the greatest benefit. Yoga asana create joint distraction that enlarge/increase glenohumeral joint space, and stretches and softens the musculo-tendinous-ligament system.
Yoga For Spine, Hip and Leg-Knee Disorders and Pain
Yoga For Disc Herniation
Yoga intervention has been successfully used for neuropathic pain due to lumbar disc herniation related to nociceptive sprouting within a degenerated disc, to mechanical compression of the nerve root, and to the inflammatory mediators arising from the degenerating disc. 60 The repetition of stretching and strengthening poses in yogasana, involving lumbar spine range of motion exercises together with neural mobilization (neural tensioning technique) and stabilization exercises to protect the spine explain the achieved significant improvements in clinical outcomes of yoga group. 60 The authors believe that mobilization and tensioning may improve patient symptoms, such as hyperalgesia and allodynia, resulting in overcoming the pathogenic pathway of neuropathic pain and disability. 60 Among the multifactorial origins of yoga improvements should be included the decreased allodynia and hyperalgesia induced by the increase of anti-inflammatory cytokines, and the healing or regeneration of intervertebral disc mechanical compression imparted by the applied forces/stress and loading pattern during yogasana. It is also believed that molecular and cellular changes in dorsal root ganglion sensory neurons can be induced by exercise. 60
An interesting retrospective clinical study supports these affirmations. 29 Yoga practitioners showed significantly less degenerative disease at disc levels C3/C4, L2/L3 and L3/L4 assessed by magnetic resonance imaging than the control group. The assumed biological mechanisms responsible for the clinical improvements have been discussed, speculating that the various positions held by the spine during the yoga sessions retard disc degeneration by increasing the ability of nutrients to diffuse into the disc, and also that disc compression and tension during yoga exercises can stimulate the synthesis of growth factors by the fibrocytes and chondrocytes residing in the disc. 29
Yoga For Chronic Back Disorders and Pain
This review highlights that yoga for chronic back pain provides greater benefits of both measurable outcomes (as inflammatory cytokines, beta-endorphins, disability, nociceptive reflex, spinal mobility) and self-reported pain, stress, disability, kinesiophobia, emotion regulation, energy, quality of life than conventional educational strategies. Significant changes in biomarkers related to pain transmission and intensity, like salivary CGRP (Calcitonin Gene-Related Peptide), TNF-α and β-endorphin together with reduction of pain intensity and type, pain catastrophizing scale, fear of movement, functional ability and quality of life in patients with low back pain after 1 and 3 months of yoga intervention. 61
Of great scientific and clinical relevance is the demonstration of the epigenetic effect of yogasana reported by Adhikari et al 2022. 66 They suggest a mechanism of action of yoga on pain by inducing self-efficacy and emotion regulation, pain severity changes and neurophysiological changes as well as through changes in gene expression and DNA methylation profiles. 66 The analysis of differential expression genes from pre- to post-intervention identified a unique transcriptional response to yoga. Yoga intervention induced increased expression of antisense genes, some of which are pain involved genes, and these participants reported a greater reduction in pain following the 12-week yoga intervention. In addition, it has been demonstrated the 33 differentially hypomethylated positions after yoga with implication of genes involved in NIK/NF-kB signaling, a major pathway that modulates immune function and inflammation. 66
Frequent causes of low back pain are related to psoas muscle shortening and loss of lumbar lordosis due to the sedentary lifestyle and shortening/retraction of the knee flexor muscles, mainly hamstrings due to prolonged sitting. 95 Therefore, pivotal/pillar movements for back pain are asana in extension (frequently in the form of backbends).
Yoga practices in various protocols for spine and chronic low back pain have been interpreted (to overcome the inhomogeneous names and definitions) and condensed in Table S2 specifically elaborated for clinicians to enable their use. Yoga interventions involve:-Asana in extension included in many protocols are Dhanurasana, Bhujangasana, Ardha Urdhva Dhanurasana, Bitilasana, Urdhva Mukha Svanasana, Setu Bandha Sarvangasana, and Ardha Chakrasana. This increase and improve the lordosis of the lumbar spine. Matsyasana and Salabhasana involve the extension of the entire lumbar-thoracic-cervical spine.-Asana in flexion are key movements to elongate and release the back muscles, mainly erector spinae and quadratus lumborum. Many protocols included Uttanasana, Padangustasana, Padottanasana, Balasana, Adho Mukha Virasana, Apanasana, Halasana, Jhulana Lurhakanasana, and Pawanmuktasana.-Twisting and side bendings are essential movements to release the deepest back muscles, namely intervertebral muscles including interspinales and transversospinales (intertransversarii, multifidus, rotatores) but also semispinalis (capitis, cervicis, thoracis), longissimus, iliocostalis and multifidus. Asana present in the protocols achieved this were Marichyasana (and its variants), Ardha Matsyendrasana, Vakrasana, Bharadvajasana, Kati Chakrasana, Ardha Kati Chakrasana and Parsva Urdhva Hastasana and Ardha Chandrasana and Shithilikarana Vyayama, Tiryaka Tadasana, Parivrtta Trikonasana, Parivrtta Utkatasana, Parivrtta Parsvakonasana and Parivrtta Baddha Parsvakonasana, Parivrtta Anjaneyasana, Parighasana, Parivrtta Pashimottanasana, Parivrtta Janu Sirsasana, Bananasana, Supta Matsyendrasana, Jathara Parivartanasana, Markatasana, Supta Udarakarshanasana, and Shava Udarakarshanasana.
Yoga For Hip and Leg-Knee Disorders and Pain
This review emphasizes that yoga for hip disorders supplied more improvements of measurable outcomes (e.g., mobility tests, osteoarthritis index, stiffness, physical performance, pelvic tilt) and self-reported pain compared to education or no intervention.
Changes in hip extension and anterior pelvic tilt demonstrated strong and linear dose-response associations with both duration and frequency of yoga practice, suggesting a direct, causal relationship between yoga intervention and postural and biomechanical changes. 72 Yoga therapy helps to improve tone of the muscles around joints and, therefore, improved flexibility, and hence in the present study, showed the improvements in pain and function. The increase in muscle flexibility and strength decrease the level of pain and improve the function. 76 Gradual slow and prolonged lengthening is preferable to minimize activation of stretch reflex and subsequent increase in muscle tension and reflexive resistance to muscle elongation during stretching. The lack of wide hip movements related to lifestyle (prolonged sitting or standing) leads to stiffening and retraction of musculoskeletal structures involved in hip mobility and stability, increase the acetabular tear consisting in excessive contact stress/force of the femur-head against acetabular fossa and/or labrum hip impingement). Yoga protocols for hip joint 95 involve asana to regain/restore the physiological kinesiology by improving tissues extensibility, reducing connective tissues tightness and retractions, decreasing the excessive acetabular tear (femur-head towards acetabulum) at the hip joint and restoring the acetabulum-femoral head space.
Hip joint muscles pulling the femur towards the acetabulum (or labrum) by bone-to-bone traction force generate femur-head to acetabular fossa compression/crushing forces. Gluteus minimus, gluteus medius, pectineus pull obliquely upwards and medially; sartorius, tensor fasciae latae, biceps femoris, gracilis, adductors and iliopsoas pull upwards; piriformis pulls obliquely medially and (slightly) upwards; quadratus femoris pulls medially; gemelli and obturators pull obliquely medially and (slightly) downwards. In yoga protocols analyzed in this review, full movements involving leg(s) and hip joint are omnipresent in standing, sitting, kneeling or supine asana. Yoga positions include flexion, vertical abduction, horizontal and inferior abduction and adduction, extension, maximized whenever possible (hyperflexion with posterior glide of the femur head, hyperabduction, hyperadduction, hyperextension with anterior glide), with external/lateral rotation or internal/medial rotation.
Yoga practices in various protocols for hip and leg have been interpreted (to overcome the inhomogeneous names and definitions) and condensed in Table S2 specifically elaborated for clinicians to simplify/facilitate and encourage their use. Yoga interventions involve:-Femur head distraction is present in most of the protocols to reduce the intra-articular pressure exerted by the femur head on the acetabulum. Hip distraction is obtained by compound hip movement flexion+abduction+external rotation with the knee flexed, as in Gomukhasana, Garudasana, Supta Matsyendrasana, Ardha Matsyendrasana, Ardha Padmasana; hip distraction in association with posterior glide of femur head is achieved in Eka Pada Rajakapotasana, Adho Mukha Svastikasana, Parivrtta Utkatasana, Parivrtta Baddha Parsvakonasana, Parivrtta Baddha Parsvakonasana and Parivrtta Trikonasana. -Posterior glide of the femur head is obtained in Marichyasana, Uttanasana, Ardha Uttanasana, Aschwa Sanchalanasana, Balasana, Darmikasana, Adho Mukha Virasana, Shashankasana, Apanasana, Janu Sirsasana, Padangustasana, Pada Hastasana, and Supta Padangustasana.-Anterior glide of the femur head is achieved in Purvottanasana, Setu Bandha Sarvangasana, Ardha Chakrasana, Virabhadrasana I, Anjaneyasana, Astha Chandrasana or Alanasana, Dhanurasana, Urdhva Dhanurasana, Ardha Urdhva Dhanurasana, and Ustrasana. -Asana with rotation in one or both hip joints are performed in Eka Pada Rajakapotasana, Garudasana, Ardha Matsyendrasana, Supta Matsyendrasana, Bharadvajasana, Parivrtta Trikonasana, Parivrtta Parsvakonasana, Gomukhasana, Sukhasana. These asanas are very intense and powerful in removing joint compression and in reducing muscle retraction and stiffening.-Asana involving hip flexion or hyperflexion w/wo external rotation or medial rotation are Urdhva Hastasana, Ardha Chakrasana, Virabhadrasana I, Utkatasana, Vrksasana, Adho Mukha Svanasana, Parivrtta Parsvakonasana, Astha Chandrasana, Anjaneyasana, Dandayamna Bharmanasana, Shashankasana, Darmikasana, Adho Mukha Svastikasana, and Gomukhasana;-Asana with hip extension or hyperextension with abduction or adduction and external rotation or medial rotation are performed in Dwikonasana, Purvottanasana, Setu Bandha Sarvangasana, Viparita Karani, Halasana, Marichyasana, Yoga Mudrasana, Matsyasana, Salabhasana; -Asana with hip abduction or hyperabduction are practiced in Tadasana, Tiryaka Tadasana, Ardha Kati Chakrasana, Kati Chakrasana, Garudasana, Virabhadrasana II, Parivrtta Trikonasana, Vasisthasana, Supta Matsyendrasana, Parivrtta Pashimottanasana.
Yoga For Generalized Arthritis
This review emphasizes that yoga for arthritis provides better improvements of both measurable outcomes (e.g., inflammatory markers, pain disability, swelling) and self-reported pain, mood, disability compared to antirheumatic drugs and DMARDs.
Comments or speculations on the biological effect of yoga on pathophysiological mechanisms have been expressed in only 2 studies that highlighted yoga’s potential role in modulating autonomic function, reducing inflammation, and improving overall physiological and psychological balance.79,80 Ganesan’s study found that the decrease of sympathetic activity provided by yoga postures lead to reduced secretion of inflammatory markers IL-1, Il-6, and TNF-alpha as well as cortisol levels. 79 Gautam reported that yoga postures influenced the release of pro-inflammatory cytokines (decreased TNF-alpha, TGF-beta, IL-6) and downregulated T cell receptor signaling and pathways (NFKB, RELA, TNFR2). Moreover, yoga therapy modulated the vagus nerve activity and increased mind-body communicative markers (beta endorphin, sirtuin). 80
Yoga practices in various protocols for arthritis have been interpreted (to overcome the inhomogeneous names and definitions) and condensed in Table S2 specifically elaborated for clinicians to simplify/facilitate and encourage their use. Yoga interventions involve:-Asana with spine extension such as Bhujangasana and/or Dhanurasana, Marjariasana, Matsyasana and asana involving strengthening with spine extension such as Setu Bandhasana and/or Viparita Karani, Salabhasana, and Matsyasana.-Asana with hip abduction with external rotation (and knee flexion) as Konasana (4/6) and its Konasana variations, Sukhasana (easy crossed-legs pose), Ardha Padmasana (half lotus), Vrkshasana (Tree pose), Ardha Bhekasana (half frog), Janu Sirsasana; -Asana involving knee flexion as Vajrasana (Thunderbolt pose) or knee flexion with abduction such as Veerasana and Virasana (Hero Pose) or hip adduction and distraction such as Gomukhasana;-Side bending or twisting movements such as Trikonasana, Ardha Chandrasana, Tiryaka Tadasana, Katichakrasana, seated twist, and Bharadvajasana.
Methodological Considerations
We would summarize final considerations on the methodological variability and limitations. While the overall findings suggest that yoga interventions provide measurable benefits for musculoskeletal disorders and pain, the considerable variability in study design and results presentation represent an important limit for generalized conclusions.
It was not possible to perform a formal meta-analysis primarily due to the substantial methodological heterogeneity across the included studies, which limited the feasibility of pooling data in a statistically meaningful way and reducing the reliability of aggregated effect estimates.
There was wide variability in sample size (20-250 participants) and age (18-75 years, mostly middle-aged or older adults). Sample size calculation was absent in 16 studies and inadequate in 6, limiting the generalizability of findings. Reported asana names were inconsistent across studies, making it difficult to consolidate the most used protocols for each body area.
Control groups varied considerably, including passive comparators (e.g., waitlist, no intervention) and active ones (e.g., stretching, Pilates, physiotherapy, NSAIDs, DMARDs). For neck and shoulder pain, active comparators were more frequent, potentially attenuating the relative benefits of yoga.
Outcome measures were heterogeneous, with both objective assessments (e.g., muscle thickness, range of motion, oxidative stress biomarkers, electromyography) and self-reported measures (e.g., pain, disability, quality of life). Standardized scales such as the Visual Analog Scale (VAS), Neck Disability Index (NDI), Oswestry Disability Index (ODI), Western Ontario and McMaster Universities Arthritis Index (WOMAC), and SF-36/WHOQOL were used in some studies, while others relied on non-standard tools, limiting cross-study comparability and reproducibility. In some cases, improvements reached clinically important significance.
Long-term effects remain uncertain due to the scarcity of follow-up data. Potential confounders (such as yoga instructor expertise, participant adherence, and concurrent medical treatments) may have influenced outcomes. Some minor, self-resolving complications were reported, and limited major adverse events occurred.
This review is the first to comprehensively analyse these methodological aspects and highlights that variability in control groups, outcome measures, and protocol reporting affects the clinical relevance and comparability of results.
To strengthen future trials on yoga for musculoskeletal disorders, researchers should ensure adequate sample sizes with power calculations, select appropriate control groups, and conduct long-term follow-ups. Clear reporting of participant selection, adherence, and detailed yoga protocols (including specific asana and session structure) is important to ensure reproducibility and to allow comparative analyses.
Conclusions
This review of the updated literature on yoga interventions for musculoskeletal disorders (MSDs) showed significant benefits. The data from the included studies is extensive, covering a broad range of clinical outcomes. Both objective measures (e.g., mobility, biomarkers) and subjective outcomes (e.g., pain, disability, quality of life) were generally improved in the yoga groups compared to controls, and in some studies, yoga even outperformed pharmacological treatments. Our narrative synthesis allowed us to create a summary of yoga asana and related clinical evidence. The variability of yoga styles (e.g., Iyengar, Hatha) and the numerous postures may increase the risk of confounding the specific contributions of individual asana and other yoga components. Our analytical approach allowed us to elaborate a summary of yoga techniques and related clinical evidence. The different type of yoga (as Iyengar, Hatha) and the hundreds of yoga postures may increase the risk to confound the role and effect of the yogic approach.
The present review outlines the potential effectiveness of yoga in several body areas affected by MSDs, enhancing mobility, reducing drug dependence, and improving quality of life.
In particular the review based on multiple randomized studies showed significant benefits of yoga although heterogeneity in protocols limits reproducibility, namely: 1. a significant effect to improve MSD symptoms (6/8 studies) for head and neck pain, 2. a significant positive evidence (8/13 studies) of reduced pain and disability for shoulder and hand disorders, 3. evidence of symptom relief and improved mobility for back pain, hip, and knee disorders, though some minor adverse events were reported (16/22 studies), 4. a significant positive evidence indicated pain reduction and lowering of inflammatory markers for generalized arthritis (5/6 studies).
Based on these findings, yoga might be considered as a complementary therapeutic support alongside conventional pharmacological and surgical treatments.
Supplemental Material
Supplemental Material - Yoga For Musculoskeletal Disorders: A Review of Prospective Clinical Studies
Supplemental Material for Yoga For Musculoskeletal Disorders: A Review of Prospective Clinical Studies by Maria Giovanna Gandolfi, Fausto Zamparini, Andrea Spinelli, Robert B. Saper, and Carlo Prati in Global Advances in Integrative Medicine and Health
Supplemental Material
Supplemental Material - Yoga For Musculoskeletal Disorders: A Review of Prospective Clinical Studies
Supplemental Material for Yoga For Musculoskeletal Disorders: A Review of Prospective Clinical Studies by Maria Giovanna Gandolfi, Fausto Zamparini, Andrea Spinelli, Robert B. Saper, and Carlo Prati in Global Advances in Integrative Medicine and Health
Footnotes
Author Contributions
Conceptualization, M.G.G.; methodology, M.G.G.; formal analysis, M.G.G.; investigation, M.G.G., F.Z; data curation, F.Z.; writing-original draft preparation, M.G.G.; writing, review and editing, M.G.G., F.Z., C.P., and R.S.; visualization, F.Z. and A.S.; supervision, M.G.G.; project administration, M.G.G.; funding acquisition, M.G.G.
Funding
The authors received no financial support for the research or authorship. For publication of this article the university research funds (RFO) of Professor Gandolfi have been used.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are derived from previously published studies that are publicly available in scientific databases. Extracted data supporting the findings of this review are available from the corresponding author upon reasonable request.
Preregistration/Protocol
This review was not preregistered, no review protocol is available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.