
Abstract
Background
There is a marked absence of supportive care programs to address the significant distress experienced by young children with Sickle Cell Disease (SCD) and their parents. Active Music Engagement (AME) is an evidence-based music therapy intervention that uses dyadic music play to mitigate interrelated parent-child distress during cancer treatment. The purposes of this study were to explore the cultural relevance of AME for Black children and parents and its potential utility during SCD treatment.
Methods
We conducted a three-phase qualitative study that included interviews with five Black parents of children (ages 3-8 years) with SCD, interviews with four additional parents/children after experiencing a music therapist facilitated AME experience and focus group sessions with a three member Black Music Therapist Advisory Board. We used thematic analysis to analyze data and synthesized findings across all three phases.
Results
Five themes and fourteen sub-themes emerged from the analysis. Theme One described the SCD experience as a dynamic journey. Theme Two offered insights into the prevalence and function of music within Black families. Themes Three, Four, and Five offered specific recommendations to improve the AME experience for Black families. Results indicated high prevalence and diversity of music in Black lives, and the importance of culture to support AME engagement. Therapists endorsed theoretical principles that inform the structure and tailored delivery of AME, with therapist and parent recommendations centered on the importance of providing experiences that affirm Black families’ values, culture, histories, and natural forms of expression. Black families and therapists also acknowledged the importance of shared cultural knowledge when receiving and providing care.
Conclusions
These findings support the potential utility of AME to reduce stress experienced by young children with SCD and their parents, and the importance of ongoing collaboration between Black families, Black therapists and non-Black team members, prioritizing the input and engagement of Black families, alongside the leadership of Black therapists.
Sickle Cell Disease (SCD) affects nearly 100,000 predominantly Black or African American individuals in the United States and millions across the globe.1-3 While preventative public health measures such as newborn screening, penicillin prophylaxis, and vaccinations have improved childhood survival in the United States, healthcare and social disparities contribute to an average lifespan that is still 30 years less than the general population. 4 Additionally, debilitating and unpredictable pain, multiorgan involvement, and high treatment costs all contribute to experiences of elevated and sustained psychosocial distress for children with SCD and their parents (or caregivers).2,5
Living with SCD and aspects of medical treatment are considered highly stressful for young children and their parents.6,7 Repeated hospitalizations and clinic appointments, uncertainty about health outcomes, recurrent pain episodes, and disruption to normal aspects of day-to-day life are just some of the stressors encountered. 5 SCD treatment can be especially hard for young children due to their development. Immature logic makes it difficult for young children to understand their disease and treatment and they have not yet developed the ability to effectively self-regulate their emotions and attention during stressful events – coping skills that are more developed in older children/adolescents.8-11 As a result, parents are a primary source of coping for young children, and without adequate social support, parents are at an elevated risk for fatigue and psychological distress. The distress experienced by young children with SCD and parents is highly interrelated and sustained, with up to 60% of children and parents developing mental health challenges.5,12 Families require supportive care to manage both intermittent and long-term treatment disease-related distress; however, there is a marked absence of supportive care programs developed for young patients and families, especially for children with SCD and their parents. 13
In pediatric hospital settings, music therapists often use various forms of active music engagement to address the social, developmental, and treatment-related needs of young children.14-16 While receptive experiences like music listening can be beneficial, 17 most research has focused on the positive effects of active music making.18-20 The creative and improvisatory nature of this approach provides a developmentally appropriate and immersive experience supporting sustained engagement, self-expression, social connectedness, and emotional regulation.21-26 In recent years, studies have increasingly explored how interactive music making can address the interconnected needs of children, their parents, and the broader family system.16,22-25,27,28 Despite this growing body of evidence, there is a notable absence of peer-reviewed research on active music making specifically for young children with sickle cell disease (SCD). However, a growing body of research does support the use of active, culturally tailored music therapy interventions to improve pain management, self-efficacy, and quality of life for adolescents and adults with SCD.29-33
Active Music Engagement Intervention Components and Theoretical Principlesa

aTable reprinted with permission in accordance with creative commons open access license ‘Attribution-Noncommercial 4.0 International’ (CC BY-NC 4.0) https://creativecommons.org/licenses/by-nc/4.0/ for the following publication: from Russ, KA, Holochwost SJ, Perkins SM, et al. Cortisol as an acute stress biomarker in young hematopoietic cell transplant patients/caregivers: active music engagement protocol. JACM. 2020; 26(5): 424-434.
Because cancer and SCD are high-risk diagnoses, with high-intensity treatments, AME may hold promise as a supportive care intervention during SCD treatment. Previous findings support AME use to reduce distress in children and traumatic stress symptoms in parents, with child-parent engagement identified as an important mediator of benefit. 38 Music serves as a prominent marker of culture, and the more culturally relevant a music experience is to an individual, the more likely they are to engage with that experience. 43 Given the importance of culture and personal preference to music engagement, and the importance of engagement for AME benefit, the purpose of this three-phase qualitative descriptive study was to engage stakeholders (parents, children, therapists) to explore the cultural relevance of AME for Black children and parents and its potential utility during SCD treatment. Findings will be used to improve the AME protocol before we initiate a larger implementation trial.
Methods
Design
We received scientific and institutional review board approvals (Indiana University IRB# approval #21992) for this three-phase qualitative descriptive research study that included interviews with nine Black parents of young children (ages 3-8 years) with SCD and members of our Black Music Therapist Advisory Board. Parent and music therapist participants provided signed informed consent and received a gift card after each interview. We used a qualitative descriptive research approach to describe the experiences of key stakeholders – parents, children, and therapists – who could speak directly to ways we might improve the intervention. This approach is appropriate for studies where the aim is not to increase theoretical or conceptual understanding but instead remains close to participants’ descriptions of their experience.
44
Phase I Parent Interviews: Explored how music functions as a part of family life and culture for Black caregivers of children with SCD, their views on using music to manage SCD related stress, and their experience with racialization in healthcare. Phase II Parent/Child Experiences with AME: Explored parent/child perceptions about AME program content (music, materials, and activities) following a therapist-delivered AME session. Phase III Black Music Therapist Advisory Board: Reviewed AME program content and findings from Phase I/II parent interviews, then offered recommendations to refine AME.
Team Positionality Statement
The AME program was initially developed by a predominantly White investigative team. It is important that we address potential for unconscious bias or misappropriation through our selection of materials. The lead author’s lived experience of being Black in the American Healthcare System, as an allied health provider, and as a patient, lends important expertise to their role in this project. The fourth and fifth authors bring to the project valuable perspectives as clinicians working daily with mainly Black patients and families with SCD. We wish to be mindful of the ways Black folks will often “code” their language and behavior in environments where they may not feel culturally seen or understood and have sought to create opportunities for authentic and meaningful engagement in this process; this includes the use of occasionally informal language in this paper, as we seek to most authentically honor the Black experience as it was expressed to us by participants, and was/is understood, mirrored and amplified by the lead author’s own Blackness.
Participants
Parent and Child Demographics for Phase 1 and Phase 2 Interviews

Data Collection
The first author, a Black PhD prepared music therapist with qualitative research expertise, conducted all interviews. The sixth author, a White masters-prepared music therapist trained on the AME protocol, delivered all AME sessions. All interviews and meetings were audio-recorded, professionally transcribed, checked for accuracy, de-identified, and stored on a HIPAA (Health Insurance Portability and Accountability Act)-compliant drive. Saturation was reached during the interviews through the use of clarifying and probing questions. This approach aims to ensure a full understanding each participant’s perspective at the individual level and differs from methods used in studies centered on theoretical or conceptual saturation. 45
Phase I
Parents (n = 5) of young children with SCD completed individual interviews that explored their use of music at home and with their child, views on using music to manage pain and stress, and experiences of racialization in healthcare. Parents were invited to participate and interviewed during a scheduled clinic appointment. Interviews were semi-structured (see supplemental material for interview guide), conducted in a private space, and lasted 30-45 minutes.
Phase II
A separate group of parents (n = 4) were invited to experience an AME session with their child. A board-certified music therapist facilitated each parent/child session, which was then followed by a semi-structured interview about their experiences and AME program content (music, materials, and activities; see supplemental materials for interview guide). AME sessions were video-recorded and lasted 20-25 minutes; interviews lasted 10-15 minutes.
Phase III
The first author recruited three board-certified music therapists from the Black Music Therapy (MT) Network to serve on our Advisory Board (AB). Two AB members identified as Biracial/Mixed Race (Half Black/Half African American), and one as Black. All three identified as female. Experience in pediatrics ranged from 5 to 12 years, with Sickle Cell related experience ranging from 3 to 12 years. After completion of Phase 2, the AB met twice virtually to review findings from Phase I/II interviews and then offered recommendations to improve cultural relevance of AME for Black children and parents.
AB members were given access to the AME protocol before their first meeting. In the first meeting, the senior author provided an overview of the AME program, use of theory to inform tailored delivery, and materials. This was followed by a 60- minute closed session facilitated by the first author and included reviewing findings from Phase I/II, and a brief discussion of recommendations (see supplemental materials for guide). A second 60-minute closed meeting was needed to complete recommendations.
Data Analysis
We used thematic analysis with manual axial coding to analyze Phase I, II and III interviews. 46 After initial analysis by the lead author, additional team members reviewed and discussed resulting themes and resolved any questions through consensus. To reduce bias and build trustworthiness we maintained an audit trail, used prolonged engagement with participants, peer debriefing to examine preconceptions and personal bias, and data triangulation.47,48
Video recordings of Phase II AME sessions were also analyzed descriptively. The lead author made note of parent/child body language and non-verbal vocalizations in relation to each other, the music therapist, and the music, paying attention to markers of comfort or discomfort (eg, open/closed posture, frequency and duration of eye movement, volume or rate of speech and/or singing). Findings were used to supplement Phase II interview findings. After completing analyses for each phase, a final round of analysis was conducted to consolidate themes across all three phases.
Results
Themes and Subthemes From Consolidated Phases, With Representative Quotes
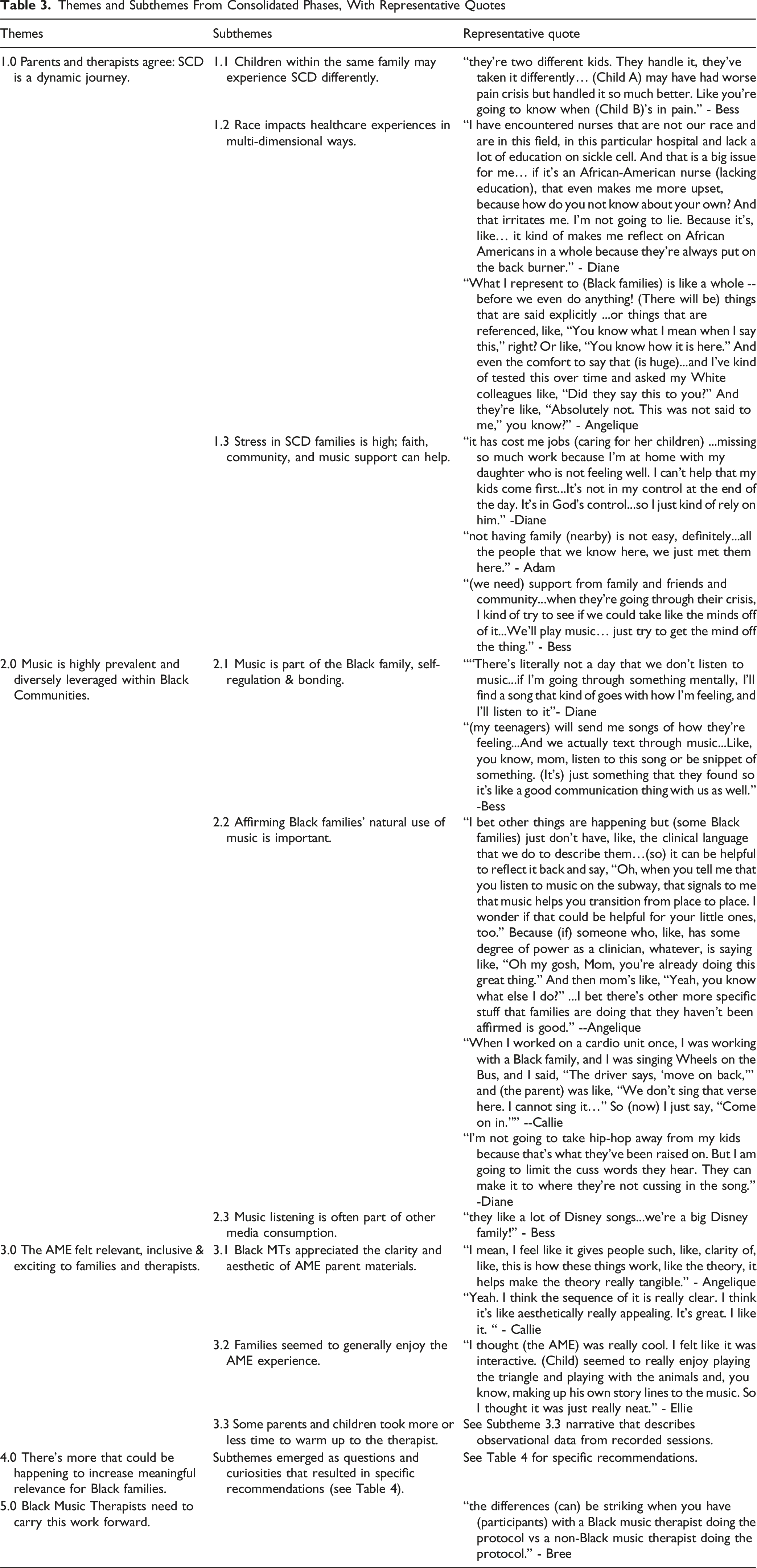
Theme 1: Parents and Therapists Agree, SCD is a Dynamic Journey for Families
Multiple parents commented on the SCD journey, with one parent (Chantelle), referring to it as “a roller coaster ride at first,” while another (Diane) described it as having “ups and downs” that reached beyond the hospital setting and involved a variety of family, healthcare and community members. Parents felt more “up” when they were being listened to and encouraged to ask questions and try new things. They felt more “down” when team members responded in ways that felt inappropriate or out of proportion to their child’s needs. Parents wanted their children to have a balance of realistic expectations and compassionate care across settings. Multiple parents also talked about there being an eventual ‘leveling out’ period with fewer crises and less frustration as their child aged.
Subtheme 1.1: Children within the Same Family may Experience SCD Differently
In Phase 1, three of the four families had more than one child with SCD. Parents described how each child might present and work through symptoms differently, adding to the complexity of their family experience with the disease and treatment.
Subtheme 1.2: Race Impacts Healthcare Experiences in Multi-Dimensional Ways
Multiple parents explicitly mentioned the impact of race on their experiences of SCD treatment, with therapists echoing awareness of this as well. Bess made note of the differences between the predominantly white teams they’d seen at other locations, and the predominantly Black team at their current treatment facility. Diane added a layer of nuance, stating the lack of “education on sickle cell” was something they had observed in white and Black nurses alike, and that it felt particularly painful when the lack was observed in someone from their own race.
Therapists provided rich descriptions of seeing the impact of race in interactions with their patients and families, with Angelique summarizing it as “a shared Blackness…that is felt palpably.” All three therapists agreed that Black MTs were uniquely situated to most effectively affirm Black families in this kind of work, because of the way families would respond to them differently than to their white counterparts.
Race also seemed to have an impact during AME sessions experienced by Phase II families. Felicia’s family was the only session where the first author was present, and video analysis revealed a layer of nonverbal vocable engagement that did not occur in other sessions when the first author was not present: enthusiastic “hmm”s and “ha”s, vocables traditionally associated with Black vernacular, in response to their child’s playing, which were echoed by the first author, who was the only other Black person in the room. No other parent exhibited this level of vocable engagement. A close second type of engagement would be the one parent who used vocal percussion during one of the songs, which the (white) music therapist noted in the moment as “unique.”
Subtheme 1.3: Stress in SCD Families is High; Faith, Community Support and Music can Help
All four families in Phase I referred to the stress of managing their child’s condition as impacting their lives. Chantelle summed the stress up as being “through the ceiling” whenever their child had to be hospitalized. For Diane, her faith was a large part of what helped her through her family’s SCD experience. Diane and other parents also felt that family and community support was something that would be (or had been) helpful for them. In addition, multiple parents across Phases named music as part of how they coped with life in general. Therapists affirmed hearing parents refer to prior practices of using music with their children intentionally, regardless of whether they’d ever heard of or experienced music therapy.
Theme 2: Music is Highly Prevalent and Diversely Leveraged within Black Communities
Three of four parents in Phase I named music engagement as an activity that was undertaken multiple times a day in multiple locations, with “lots of listening” (Bess) “everywhere” (Chantelle). R & B, specifically that of the late 80s and early 90s, Gospel, and some country music, were lifted as preferred genres. Bess also noted that intergenerational listening was common, and an important part of family bonding.
Subtheme 2.1: Music is Part of the Black Family, Self-Regulation, & Bonding
All four Phase I families noted specific cultural practices relating to music, some in statements that overlapped with discussion of how music was utilized in their family during major rites of passage, such as birth and marriage, in cookouts (barbecues), or during more everyday experiences like cleaning or preparing for bed. The integration of music and dance also entered discussion; in fact, at one interview where the child was present, the first author enjoyed a well-rehearsed presentation of the viral dance sequence from Beyonce’s “Texas Hold ‘Em.” Multiple parents also described music listening as a shared familial and cultural experience that was therapeutic for them and their children, with Bess and Diane expressly describing how they modeled this process for their children with their own music use.
Subtheme 2.2. Affirming Black Families’ Natural Use of Music is Important
The Black MTs noted how the families they worked with seemed most receptive to music therapy when it was described in terms that affirmed their values and natural forms of expression. Parents echoed this, with Diane particularly noting how the dominant culture would often reduce the dimensionality of Black music in order to censor it. She spoke specifically about Hip-hop artist Da Baby, and how him talking about “real-life stuff” like drugs and poverty was something that she felt she could connect with, and that sense of connection was important to her; she expressed appreciation for the discussion of personal/cultural connections to music being affirmed in our project.
Parents also spoke about how they set boundaries with music, like finding the “radio edit” version of a song, or making sure, in Bess’s words, that their kids knew not to “get any ideas” about behaviors that would not be aligned with their family’s values. Adam made a point to state that the way his children used music was acceptable within their practice as a Muslim family because of its educational value. Aesthetic music listening for pleasure, however, was regarded as less acceptable in their family’s religious practice.
Black MTs echoed and affirmed what families had shared, and they emphasized how important it was to them to meet families where they were, which sometimes meant respecting the request to not use certain songs or elements of music. Therapists agreed that when parents felt their values and practices were affirmed, that they seemed more receptive to engaging with music therapy in general.
Subtheme 2.3: Music Listening is Often Part of Other Media Consumption
Phase I Parents Adam and Bess noted that music for their child was often consumed as part of another piece of media, like a show, movie, or other kind of video. During a Phase II session, one child exclaimed excitedly “This song from Coco Melon!” when they heard “Five Green & Speckled Frogs” sung by the therapist. This tying of a familiar song to the media context in which it was heard was echoed by the Black MTs as a common practice for kids that they served.
Theme 3: The AME Felt Relevant, Inclusive & Exciting to Families and Therapists
All Phase II parents named some aspect of relevance between the AME goals and/or structure and their personal lives, and expressed appreciation for the encouragement of parental participation in the experience as well. They felt the songs were relevant and familiar to them, which was echoed by the Black MTs in Phase III who also expressed familiarity with most songs and materials included in the AME. Parents and therapist also expressed general familiarity with the instruments provided. When asked if anything in the kit felt unfamiliar, all parents and therapists expressed being unfamiliar with the story of Abiyoyo, a folk tale with South African origins. This unfamiliarity didn’t seem to be a deterrent to any of the families, however, with Senna saying “we love, love, love coming to (clinic) appointments because we always get the Black character-themed books.” Therapists acknowledged simply that the African continent is vast, and that it was not surprising there might be some material that was more or less familiar than others.
Subtheme 3.1: Black MTs Appreciated the Clarity and Aesthetic of the AME Parent Materials
Black MTs expressed excitement about the parent materials created for the AME. Angelique posited that there might be even more that could be done to provide materials to parents after the close of the session, suggesting the possibility of a QR code that could lead to a folder or some other “way to make (customized songs) something that you take home if the therapist had the bandwidth to facilitate a recording process.” The other two therapists and the first author all expressed excitement at this idea, to create a possible living archive of materials that had been suggested by parents and recorded by therapists.
Subtheme 3.2: Families Seemed to Generally Enjoy the AME Experience
All Phase II parents and children engaged with the AME for the entirety of the session. There was only one moment where a parent had to disengage to take a phone call, otherwise each family seemed keen to partake in every aspect of musicking together, from choosing a goal on which to focus (like relaxing or having fun together), to selecting songs/materials and singing or playing along with each one. Multiple instances of smiles and playful interaction were noted in video analysis of engagement between adults in the room (the music therapist and parent), as well as between each adult and the child. In particular, parents and their children seemed deeply and consistently attuned throughout each song, often leaning in towards each other with smiles as they sang or played, contributing extended eye gaze in each other’s direction, and occasionally laughing.
Subtheme 3.3: Some Parents and Children Took More or Less Time to Warm up to the Therapist
Every family in Phase II took some time to warm up to the therapist, and during that “warm up” period, parents could be observed glancing sideways at the therapist or avoiding turning their body in their direction entirely while instructions were being given initially. Gradually as sessions went on, however, each parent and child opened their posture and made more sustained eye gaze towards the therapist. Sometimes the child was the first to do this and other times children seemed to follow their parents’ lead. Every session ended with children excited to take their AME materials home to explore further, and parents expressing appreciation to both the music therapist and the first author for the experience.
Subtheme 3.4 Sometimes the Therapist Made Accidental Cultural References
We anticipate that white music therapists may occasionally miss cultural references that are familiar to Black families. During one session, the white therapist made an accidental reference to an element of Black pop-culture slang during an improvisational rhyming sequence. In this instance, the therapist chose to rhyme the word “lap” with “wap,” (intending it to be a nonsense word). In response, the parent uttered a slight chuckle and lowered their head as they briefly struggled to compose themselves. “WAP” is the title of a song by the hip-hop artist Cardi B, in collaboration with Megan Thee Stallion, and has become a sexual reference in popular culture, originating within the Black American community. While the therapist was familiar with the song, it was not their intent to make this kind of reference during a family session. This type of accidental miscommunication might be possible when a therapist does not share the same cultural point of origin as a patient or their family.
Theme 4: There’s More that Could Be Happening to Increase Meaningful Relevance for Black Families
Theme Four: Parent and Therapist Recommendations to Improve Active Music Engagement Content and Materials
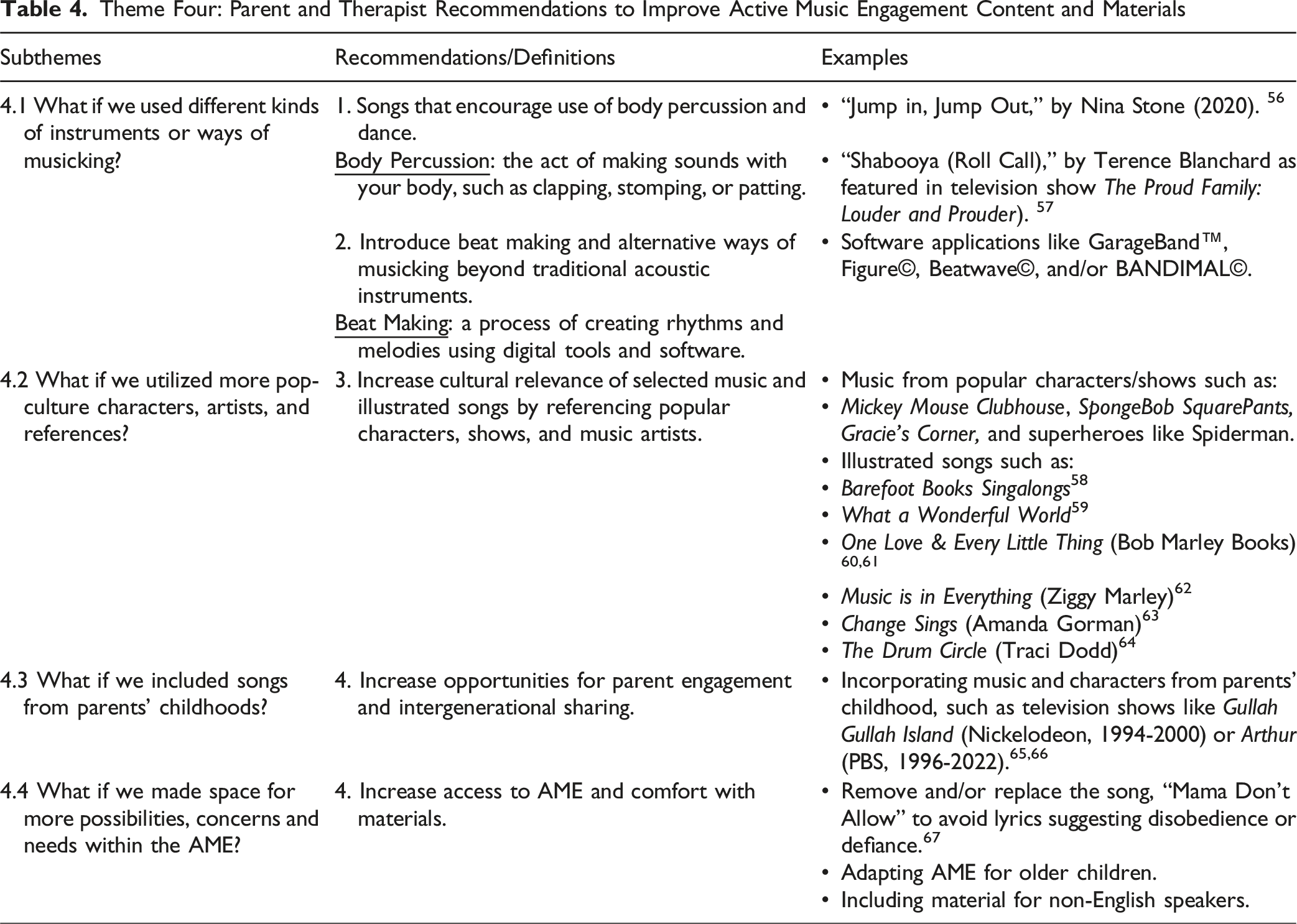
Subtheme 4.1: What if we Used Different Kinds of Instruments or Ways of Musicking?
All Phase II parents were noted to briefly clap their hands or tap on their laps during songs, though it wasn’t typically prompted in the moment. Sidney used body percussion in an extended way, beatboxing (also unprompted) during her family’s experiencing of the AME. Making space for multiple ways of musicking—particularly movement and beat-making—was lifted throughout the Black MTs’ discussion in Phase III, and the importance of affirming nonverbal engagement, like vocables, as observed in the session with Felicia’s family.
Subtheme 4.2: What if we Used More Pop-Culture Characters and Artists?
Parents recommended characters familiar in popular culture, as well as some that were unique to the Black community, like Senna’s suggestion of Gracie’s Corner, a Black YouTube channel run by a father/daughter team who create and promote educational songs written in various African Diasporic styles of music. Therapists in Phase III also discussed how prevalent superheroes were in the worlds of today’s Black children, and made several picture book recommendations in the context of this discussion. They noted that the picture books added important non-verbal elements to the text, and visually represented people of different racial backgrounds, in ways that amplified the values within the source material.
This raised the question of what this might mean for the physical materials of the kit, which currently featured various animal stuffies and finger puppets. Therapists went back and forth briefly over how important it was or wasn’t to have a physical representation of Spiderman or any other pop culture character or icon that a child might name. Bree and Callie both shared how common the use of iPads was in their practices, and all therapists agreed that technology could be utilized in such situations to find photo representations, or kids could just be encouraged to use their imaginations.
Subtheme 4.3: What if we Included Songs from Parents’ Childhoods?
Songs that were familiar to parents’ own childhoods or younger years came up for Phase III Therapists on a few occasions, including as lullabies or “calm down” songs. As an example, Angelique shared a practice of asking parents what songs they might have slow danced to, in order to establish a baseline of songs that held meaning for the family.
Subtheme 4.4: What if we Made Space for More Possibilities, Concerns and Needs Within the AME?
The desire to affirm Black families was interwoven into all feedback given by Black Therapists, and was sometimes lifted as concerns that came from an embodied place when something “didn’t feel quite right.” In general, therapists raised questions that reflected curiosities, more than concerns, about elements like the AME’s relevance to the clinical environment, use with older children, and ways to involve non-English speakers. None of these seemed to register for the therapists as primary concerns, but topics to consider.
Theme 5: Black Music Therapists Need to Carry This Work Forward
All three therapists agreed that Black MTs were uniquely situated to most effectively affirm Black families in this kind of work, because of the way families would respond to them differently than to their white counterparts. Each of the Black MTs in Phase III expressed willingness to support future work.
Discussion
As primary caregivers, parents of young children with SCD experience sustained, significant stress with managing their child’s disease and supporting their child’s development of effective coping strategies.5,6 Reducing interrelated parent-child distress and developing positive coping strategies early in treatment holds promise for improved symptom management, adjustment to illness, and well-being for both parents and children – yet few interventions have been developed and evaluated for young children with SCD and parents. 13 Active Music Engagement is a dyadic, music based play intervention that lowers distress in young children with cancer and parents, with parent-child engagement identified as an important mediator of benefit. 38 To explore the potential utility of AME during SCD treatment, we explored parents’ experiences of, reactions to, and recommendations for AME. We also sought to deepen our understanding of how music functions for Black families and engaged a Black music therapist advisory group to further explore and develop AME as a culturally responsive, engaging intervention.
There is a Need for More Culturally Attuned and Strengths-Based Tools to Reduce Stress in Black SCD Families
Parents and therapists confirmed and emphasized the multidimensional stress of having a child (or multiple children) with SCD, and the unique stressor that is being Black in America while having a child with a highly stigmatized disease. Receiving care from predominantly white healthcare teams presents challenges related to having a shared racial and cultural identity that can affect their sense of trust and willingness to engage with treatment. Even when healthcare providers have a shared racial identity, parents still encounter providers who lack knowledge about SCD that sustains medical mistrust, with ripple effects that cascade into multiple aspects of their lives. However, there did seem to be a positive impact on the parental experience when a healthcare provider shared their racial identity, possessed knowledge about SCD, and affirmed the parents as meaningful participants in their child’s care, as exemplified by the interaction between the one parent and researcher exchanging culturally significant Black vocables during their session. These experiences are consistent with findings from other qualitative studies of Black and African American families’ experiences with SCD and its treatment, including the pervasive impact that the disease has on the life of young children and families, risk of social isolation, the need for interventions based on family-strengths and culturally attuned care.6,12,49-51 However, more research with a larger sample size of participants would be needed to explore this further.
There is a Strong Prevalence and Potential of Music in Black Families of Children with SCD
Parents also identified music as important to their everyday life, a way that they cope with life stressors, and something they model for their children as a shared, intergenerational experience that is important to family bonding. They also noted the importance of music to specific cultural practices and rites of passage, including requests for culturally resonant forms of active music making using the voice and body, as well as instruments. All these findings are consistent with those from a study that observed variations in patient-selected treatment goals and uses of music of Black and white adult cancer patients receiving music therapy to manage pain. 52 As noted by the authors, these variations suggest that personalization and cultural adaptation, as opposed to a standardized set of music experiences, are essential to achieve equitable outcomes in racially diverse patient populations.52,53
Future Research Could Amplify AME’s Existing Relevance and Address More Specific Potential for Black Families of Children with SCD
Our primary finding was that the theoretical principles that underlie the structure of AME play experiences, and their tailored delivery, are relevant and important in supporting Black children and parents. Parents and therapists found the content and materials to be relevant, inclusive, and enjoyable. Black music therapists also endorsed the structure, content, and use of the collaborative goal setting and tip sheets, noting that these brought clarity about the purpose of AME sessions for participating families. However, they identified important ways to increase the cultural relevance of AME experiences for Black families and in turn, more meaningful engagement and benefit.
Recommendations centered on the importance of providing music and music-making experiences that affirm Black children and parents’ values and natural forms of expression, emphasizing the importance of shared cultural knowledge when receiving and providing care, which is a central tenant of culturally competent care.53,54
This has important implications for future trials, including ongoing collaboration with Black parents, children, and therapists as we explore the potential benefits of AME for parents of young children with SCD. Next steps are to identify, create, and expand music-play experiences that more fully represent the diverse range, and music preferences of Black families – while maintaining theoretical principles specified in the Contextual Support Model of Music Therapy to guide their structure and tailored delivery. Black music therapists are best positioned to lead this work, including ways to augment AME training and resources that support personalization and cultural adaptation of AME for Black families.52,55
Limitations
Our primary aim was to obtain Black parents’ and therapists’ perspectives about the AME intervention and its cultural relevance and utility during SCD treatment. Our small sample might be viewed as a limitation; however, we included key stakeholders (parents, children, therapists) who could speak to the relative strengths and limitations of the AME protocol in terms of its cultural relevance and identify specific ways to improve the protocol before starting a larger trial. We did not aim to answer theoretical questions or gain conceptual understanding, which often requires a larger number of participants to achieve. In future studies, increased representation from primary caregivers who identify as fathers, grandparents, or other family members and greater representation across the targeted child age group (3-8 years) will be needed to explore the broader, lived experience of AME during treatment for SCD. And while findings from this study cannot be extrapolated to global populations, it does indicate the importance of understanding the experience of music in other groups when considering adaptation of interventions, like AME, globally. Future studies, in the U.S. and in other countries, will benefit from sustained involvement of parents, children and therapists in a collaborative and advisory role.
Conclusion
Theoretical principles that inform the structure and tailored delivery of AME experiences are relevant and important in supporting Black children with SCD and their parents. Therapists endorsed these theoretical principles to support engagement and the importance and inclusive nature of the intervention materials including the collaborative goal setting and parent tip sheets. Although families found the AME experience to be relevant, inclusive, and enjoyable, they identified important ways to increase the cultural relevance of AME experiences for Black families. Recommendations centered on the importance of providing music and music-making experiences that affirm Black children and parents’ values and natural forms of expression. This has important implications for future trials, including ongoing collaboration with Black parents, children, and therapists as we explore the potential benefits of AME for parents of young children with SCD.
Supplemental Material
Supplemental Material - Music as Supportive Care for Young Children with Sickle Cell Disease and their Parents: A Three-phase Qualitative Exploration into the Cultural Relevance of Active Music Engagement with Black Families
Supplemental Material for Music as Supportive Care for Young Children with Sickle Cell Disease and their Parents: A Three-phase Qualitative Exploration into the Cultural Relevance of Active Music Engagement with Black Families by Natasha Thomas, K. Maya Story, Elizabeth Harman¸ Seethal A. Jacob, Julia E. LaMotte, Claire Kendrick, Sheri L. Robb in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgments
Special thanks to the music therapists who served on our Black Music Therapist Advisory Panel: Jasmine Edwards, MA, LCAT, MT-BC, Chantise Hunt, MA, MT-BC, and Lauren Ragan, MA, MT-BC.
Ethical Approval
This study received approval from the Indiana University IRB (approval #21992) on February 26th, 2024 in accordance with the Common Rule.
Consent to Participate
Written informed consent to participate in this study, and for anonymized patient information to be published in this article was provided by the participants’ legal guardians. All people named in the acknowledgements consented to having their names published in this manuscript.
Author Contributions
All Authors contributed to study conceptualization/design. NT, SAJ, JEL, CK contributed to data collection. NT, EH, KMS, SLR contributed to data analysis. All authors contributed to writing and final approval of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Walther Cancer Foundation through the last authors’ endowed professorship. EH is supported by the National Cancer Institute of the National Institutes of Health (T32CA117865; Champion/Mosher, MPIs).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.