
Abstract
Background
Myasthenia gravis (MG) is a rare autoimmune disease resulting in muscle weakness. Although pharmacologic treatments are typically effective at managing symptoms, prolonged use is associated with safety issues. Acupuncture treatment may have a significant positive effect in treating MG symptoms and may enhance the efficacy of medications.
Objective
The overall goal was to examine the feasibility and safety of a pilot randomized controlled trial of acupuncture treatment in individuals with MG.
Methods
Participants were randomized into 2 arms: (1) immediate start and (2) delayed start. Participants in the immediate start arm underwent twice weekly acupuncture for 12 weeks, whereas participants in the delayed start arm underwent a 12-week delay period, followed by twice weekly acupuncture for 12 weeks. A base treatment of 21 acupoints was used for all study participants. Acupuncturists made a Traditional Chinese Medicine differential diagnosis to determine whether the patient was yang deficient, yin deficient, or stagnation pronounced, and could add up to 9 additional acupoints. Participants received the same acupuncture protocol for all 24 treatments.
Results
Twenty-four individuals with MG were enrolled in the study. The average age of participants was 62 (SD = 13) with an average of 8 years (SD = 9) between diagnosis and enrollment. Seventeen of the 24 individuals who signed the consent form completed 100% of acupuncture treatment sessions and completed the full study. Only 17 adverse events were determined to be definitely or probably related to treatment, which were mostly mild site reactions. Barriers to participation included transportation issues, travel time, and the overall time commitment.
Conclusion
The results demonstrated that acupuncture treatment was overall feasible and safe in individuals with MG. Participants also self-reported improvements in MG symptoms. Next steps will include development of an efficacy RCT with a rigorous study design to examine the clinical significance and efficacy of acupuncture for MG.
Keywords
Introduction
Symptoms of Myasthenia gravis (MG), a rare autoimmune disease, can typically be managed well through medications. 1 However, prolonged medication use is associated with increased susceptibility to infections, organ toxicity, blood disorders, and long-term cancer risk. 2 Additionally, immune suppression may not be sufficient to control symptoms or improve quality of life (QOL). 2 Recent patient reported outcome (PRO) studies have shown that 33%–47% of individuals with MG are unsatisfied with current symptom management.3,4
In a recent systematic review, acupuncture was shown to have a significant positive effect in treating MG symptoms and may enhance the efficacy of medications. 5 The review examined 13 randomized controlled trials (RCT) conducted in China with 775 individuals with MG. 5 The primary outcome measure was the relative clinical score (RCS) response rate, the primary assessment used to evaluate severity and treatment effect of MG in China. 6 The review concluded that acupuncture combined with medication may be beneficial for MG. However, they also concluded that more rigorous studies with longer follow-up times were needed. Because there are limited studies in this population, the overall goal was to examine the feasibility and safety of a pilot RCT of acupuncture treatment for adults with MG.
Methods
Subjects and Study Design
Twenty-nine adults were recruited from 2021-2023 for this two-arm RCT (NCT05230082). The study was approved by the HealthPartners Institute Institutional Review Board (IRB), was conducted according to the Declaration of Helsinki, and followed Good Clinical Practice Guidelines. The design includes all elements of the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines, 7 which are an extension of the Consolidated Standards of Reporting Clinical Trials (CONSORT) guidelines. 8 All participants provided informed consent. Inclusion criteria included: (1) Age 18-80, (2) MG diagnosis, and (3) ability to provide informed consent. Exclusion criteria included: (1) Non-English speaking, (2) participation in acupuncture outside of the study, (3) history of any other serious neurological, psychiatric, chronic pain disorders, or seizures, (4) history of bleeding diathesis, other bleeding disorders, or syncope with needle puncture, (5) recent or active substance use disorder, (6) women who were pregnant, lactating, or planning to become pregnant, and (7) active or past participation (≤3 months) in an interventional study.
Participants were primarily recruited from outpatient clinics. Recruitment materials were also provided to local community partners. Participants were randomized into 2 arms: (1) immediate start and (2) delayed start. Balanced treatment assignments were achieved using permuted block randomization with random block sizes stratified by sex. The study biostatistician generated a randomization schedule using SURVEYSELECT in SAS. Assignments were not seen by other study personnel and were not changed after randomization.
Following consent and randomization, both arms completed a pre-treatment visit where they completed the MG Quality of Life (MG-QOL15r) and the MG Activities of Daily Living (MG-ADL) assessments (Figure 1). The immediate start group began twice-weekly acupuncture for 12 weeks. Following acupuncture, the immediate start group completed 2 post-treatment visits separated by a 12-week follow up period (Figure 1). After a 12-week delay period, the delayed start group completed a 2nd pre-treatment visit and then began twice-weekly acupuncture for 12 weeks. Following acupuncture treatment, the delayed start group completed a post-treatment visit (Figure 1). Twice weekly acupuncture for 12 weeks was selected based on the study by Zhang et al, which showed that treatments lasting 12 weeks showed a statistically significant difference between groups, indicating that long-term acupuncture may be beneficial.
5
Study Timeline of Participant Activities
During all post-treatment visits, participants completed the MG-QOL15r and the MG-ADL. At the first post-treatment visit, they also completed a follow-up survey with questions about their acupuncture experience. Adverse events (AEs) and serious adverse events (SAEs) were also recorded during the study. Study staff and acupuncturists documented events, categorizing them by severity and their potential relatedness to the intervention. Each event was subsequently reviewed by the study physician and Principal Investigator (PI) for final determination and reported to the IRB. Data was collected and managed electronically via Research Electronic Data Capture, a secure, web-based software designed to support data capture for research.9,10
Intervention
Acupuncture was administered in an outpatient clinical setting by licensed acupuncturists with a master’s degree (or higher) from accredited institutions, and 5 or more years of experience. Prior to enrollment, acupuncturists practiced administration methods to ensure consistency between providers.
Standard, sterile stainless-steel, disposable needles (DongBang™ Corporation, Spring Ten 0.22 × 30 mm; Boryeoung, Republic of Korea) were inserted in the acupuncture point locations, with approximately 21-30 needles used for each treatment (described below). Needle insertion depth was approximately 1-20 mm. Needle reaction (soreness, numbness or distended feeling around the point, also known as a Deqi sensation) occurred during the initial insertion. Following 10 minutes of retention, all needles were rotated to maintain Deqi sensation, which has been shown to increase the acupuncture effectiveness.11,12 All needles were left in place for 30 minutes, a typical duration in clinical practice.
Acupuncture points were selected for classical Traditional Chinese Medicine (TCM) indications13,14 relevant to MG symptom pathology and their modern biological,15-18 muscular,15,16,19 immunological,16,18 and neurological15,17,18,20 actions. Anatomical locations were based on the World Health Organization’s acupuncture point guideline.
21
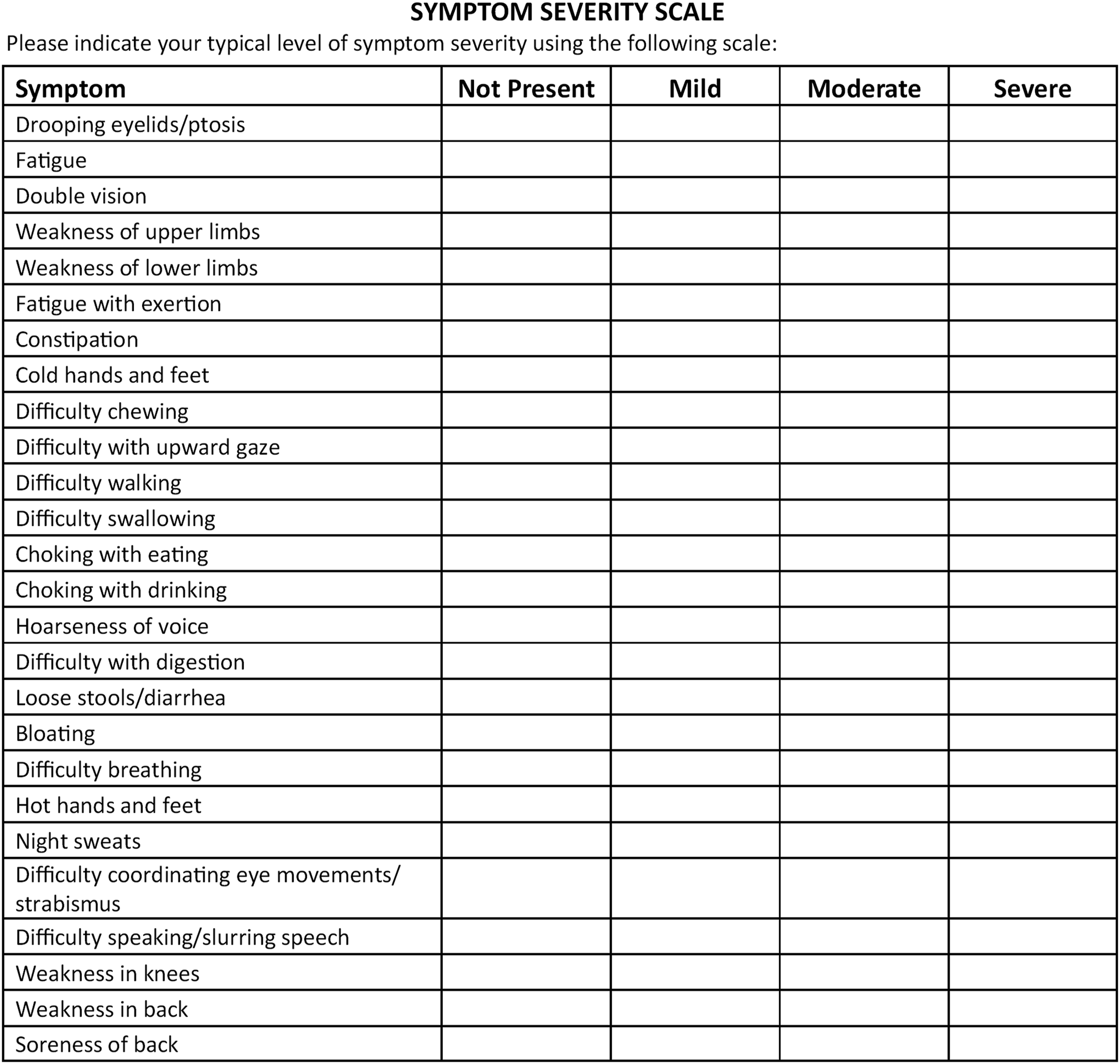
TCM acupuncture was used for all sessions. A base treatment of 21 needling points was used for all study participants (Figure 2). An unscored symptom severity scale was developed to assist acupuncturists with TCM assessment examining each patient’s individual symptoms; it was not used as an outcome tool (Figure 3). The scale included the most common symptoms of MG along with different levels of severity. Using this information, acupuncturists made a TCM differential diagnosis to determine whether the patient was yang deficient, yin deficient, or stagnation pronounced, which are diagnostic categories that acupuncturists use to classify patterns of disharmony or imbalance within the body.
22
The yin and yang principle indicates the balance of 2 opposing, yet complementary forces.
22
Yin is related to nourishment and repair functions, whereas yang is related to defense and immune functions. Stagnation pronounced indicates a disruption in the flow of Qi (energy) and blood and is often marked by pain.
22
Based on the acupuncturists’ differential assessment at the beginning of the first treatment visit, up to 9 additional acupuncture points could be added to the base treatment plan (Figure 2), allowing for individually tailored treatment. These points were used for all 24 visits. Acupuncture Treatment Points Used for the Study Intervention. *Note: Bilateral Acupuncture Points Were Utilized, when Appropriate Symptom Severity Scale Developed by Study Investigators for Determining Individualized Acupuncture Treatment Plan for the Study
Participant Assessments
Participants completed the MG-QOL 15 Revised, a 15-item disease-specific questionnaire including items assessing vision, speaking, eating, and activities. 23 Scores range from 0 to 30 where a higher score indicates a greater impact on QOL. They also completed the MG-ADL, an 8-item scale developed to assess the effects of MG symptoms (diplopia, ptosis, chewing, swallowing, voice/speech problems, and respiratory symptoms) on daily activities. 24 Scores range from 0 to 24 with higher scores indicating more severe symptoms. A semi-structured follow-up survey of participants was conducted with questions about their acupuncture experience, such as, “Have you noticed any changes in your symptoms of MG after completing acupuncture treatment? If yes, which symptoms?” These assessments were included to evaluate the feasibility of collecting potential outcome measures for a future efficacy trial and were not used to estimate treatment effects.
Statistical Analysis
Descriptive statistics were used to summarize recruitment and enrollment. Randomization success was assessed by comparing patient characteristics across study arms. Adherence was evaluated based on the percentage of treatment sessions attended and participant assessment completed. Safety was assessed by summarizing the frequency, severity, and treatment relatedness of AEs and SAEs. Participant survey responses were summarized to capture patient experience. All analysis was conducted in R version 4.2.
Results
From 2021-2023, 29 individuals were screened and 5 were ineligible (Figure 4). Twenty-four individuals were consented and of those 4 withdrew after randomization, but prior to the start of the acupuncture. Two individuals did not attend their first acupuncture visit and were unable to be reached; therefore, they were withdrawn by the PI. The other 2 individuals determined they were unable to commit to the schedule and chose to withdraw. Twenty participants started acupuncture and of those 1 experienced medical complications unrelated to the study intervention and did not complete acupuncture for >14 days; therefore, were withdrawn by the PI. Two other participants chose to withdraw due to illness unrelated to the study intervention and feeling that the study was lasting too long. Seventeen of the 24 individuals who signed the consent form completed the full study (71% study completion rate). Of the 7 individuals who withdrew from the study (Figure 4), 4 were randomized to the immediate start group, and 3 to the delayed start group. CONSORT Diagram of Study Enrollment
Participant Characteristics at the Time of Study Enrollment (N = 24)

aTwo arms compared using 2 sample t-tests with equal variances. (Time since MG Diagnosis) or Fisher’s exact tests (all other variables).
bAll participant identified as non-Hispanic ethnicity.
cIndividual originally classified at stagnation pronounced switched to yang deficiency after 3 treatments.
Notes: MG - Myasthenia Gravis; SD – Standard Deviation; IQR – Interquartile Range; All summary stats n (%) or Mean ± SD.
On average, participants enrolled completed 92% (SD = 21%) of acupuncture treatment sessions. Of the 17 participants who completed the full study, all completed 100% of acupuncture treatment sessions. All participants completed baseline MG-QOL15r and MG-ADL and response rates at each subsequent timepoint were 100% among those still enrolled in the study (Figure 5). Supplemental Figure 1 displays the MG-QOL and MG-ADL distributions at the pre- and post-intervention timepoints pooled across arms. Responses from early withdrawal timepoints were grouped with the closest future timepoint. However, the number of data points available decreased over time, driven by study withdrawal and an instance of an administrative error in which a participant was not contacted to complete their second pre-treatment assessment (Figure 5). Participant Assessment Data Availability. Note: Data labels represent the number of responses at each timepoint; Assessments from early withdrawals grouped with post-treatment 1 (Immediate start, n = 1) and post-treatment (Delayed start, n = 1)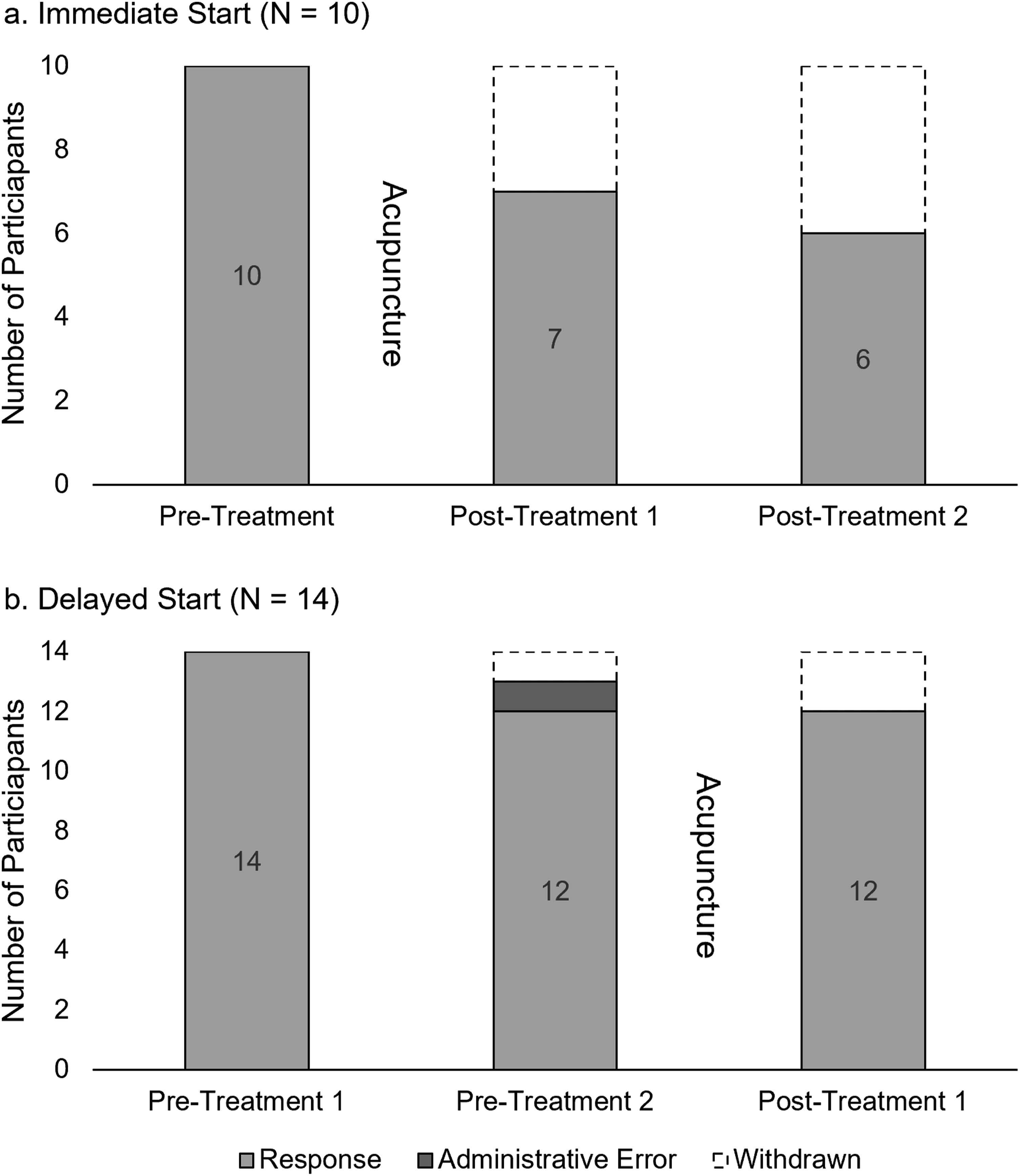
Occurrence, Severity, and Type of Adverse Events During Study Period

Notes: All summary stats count of events (n).
Participants’ Experience Survey Results (N = 16)

aPost-treatment surveys sent to participants who completed the study intervention.
Notes: MG - Myasthenia Gravis; SD – Standard Deviation; IQR – Interquartile Range; All summary stats n (%) or Mean ± SD.
Discussion
Overall, the results demonstrated that acupuncture treatment was feasible and safe in adults with MG. Response rates for participant assessments were high across all measurement timepoints among those still enrolled. Attrition over the course of the study reduced the number of participants contributing data at later timepoints. This pattern highlights strong engagement among retained participants and suggests that future studies implement strategies for maintaining study participation to ensure adequate PRO data to assess intervention effectiveness. Although 53 AEs were reported, this was likely due to the recording of all illnesses or injuries, regardless of relatedness to the intervention. Of the 53 AEs reported, only 17 were determined to be definitely or probably related to treatment, which were mostly mild site reactions that resolved quickly, indicating that acupuncture was safe in this study. Individuals self-reported that acupuncture was moderately helpful (3.6/5) and 75% of participants self-reported improvements in their MG symptoms, suggesting that acupuncture was feasible in adults with MG. The only reported barriers to study participation were transportation issues or travel time (n = (2) and time commitment (n = 3), indicating that individuals generally faced few challenges participating in the study.
A major limitation to acupuncture research is the use of fixed protocols to minimize the difficulty of treatment quality control, which is not in line with typical clinical practice and may lead to an underestimation of the treatment effect. 25 In clinical practice, acupuncturists typically complete a differential diagnosis focusing on the 8 Principle Patterns of TCM to determine the best treatment approach. 22 For this study, acupuncturists used an individually tailored treatment approach more typical to what is done in clinical practice, which may increase the real-world generalizability of the results. The study demonstrated that an individually tailored treatment approach was feasible to implement in individuals with MG.
Zhang et al. reviewed 13 RCTs with 775 participants, 8 of which included TCM manual acupuncture as an adjunct to medication. 5 They found that acupuncture combined with medication was more effective than medication alone in improving the RCS response rate and clinical absolute score, a quantitative assessment used to examine the severity of MG used in TCM. 6 Only 1 study examined QOL using the Short Form 36 and found that acupuncture combined with medication had a greater impact on QOL than medication alone. Of the 13 RCTs, none of the studies collected information on ADLs or obtained qualitative self-reported feedback. Safety data were limited with only 3 studies reporting AEs, which were mostly mild. Importantly, there were no SAEs reported related to acupuncture. Finally, the authors reported that the quality of evidence was low overall and there was in general a high risk of bias and methodological inconsistencies, including differences between medications and acupuncture interventions utilized.
Xue et al reviewed 14 RCTs of acupuncture for MG in 1009 individuals, 26 with only 3 overlapping with Zhang’s review. Most studies reported a higher clinical effective rate in the acupuncture group, as measured by a >25% reduction in TCM relative clinical score, or improvement of symptoms as a dichotomous measure (effective or ineffective). Acupuncture also showed greater improvements in TCM relative clinical scores, clinical absolute scores, and Quantitative MG scores compared to controls. Two studies also reported that acupuncture had a positive effect in improving QOL. Only 1 study mentioned safety, stating that there were no apparent differences in AEs between the groups. None of the studies examined ADLs or obtained qualitative feedback from participants. Finally, the authors noted low study quality, methodological flaws, and variability in acupuncture protocols, highlighting the need for future studies.
In contrast to previous studies, this feasibility pilot RCT collected PROs, including QOL (MG-QOL15r), ADLs (MG-ADL), and participants’ self-reported symptom improvements. Most treatment-related AEs were mild site reactions indicating that acupuncture was generally safe. Although 1 participant in this study experienced an SAE, it was determined to be unrelated to treatment (hospitalization for gastroparesis). In this study, participants were not required to or prevented from making changes to their prescription medications, providing a more pragmatic evaluation of the feasibility of acupuncture as an adjunctive treatment in this heterogeneous population. These findings support the feasibility and acceptability of acupuncture for MG and highlight the need for a rigorously designed efficacy RCT to determine therapeutic benefit.
Limitations
This study had several limitations, including a small sample size, with only 17 participants who completed the full study; however, the primary focus of this study was on feasibility and safety. This study also utilized a delayed-start design, which has many methodological considerations.27,28 While the design may have impacted our attrition rate due to the 12-week delay, only 3 of the 7 participants who withdrew were randomized to the delayed-start group. The choice of the delayed-start design allowed all participants to access the intervention which improved ethical acceptability. Another limitation to this study was the lack of blinding, which is a common challenge in acupuncture trials and not unique to this study. 29
Conclusion
The results of this study demonstrated that acupuncture treatment for adults with MG was feasible and safe. Participants also self-reported improvements in MG symptoms. Barriers to participation in the trial included transportation issues, travel time, and the overall time commitment. Next steps will include development of an efficacy RCT with a rigorous study design to examine the clinical significance and efficacy of acupuncture for MG.
Supplemental Material
Supplemental Material - Acupuncture Treatment for Individuals With Myasthenia Gravis – A Pilot Randomized Clinical Trial
Supplemental Material for Acupuncture Treatment for Individuals With Myasthenia Gravis – A Pilot Randomized Clinical Trial by Amanda A. Herrmann, Ella A. Chrenka, Lap Pui Chung, Sophia G. Bouwens, Ellie K. Tansey, Lixin Qin, Ayla A. Wolf, Marny T. Farrell, Samantha J. Sherman, Aleta L. Svitak, Leah R. Hanson, and Gaurav K. Guliani in Global Advances in Integrative Medicine and Health
Footnotes
Acknowledgments
We would like to acknowledge HealthPartners’ Neurology and Rehabilitation Departments for their assistance and support with this study and the study acupuncturists. We would also like to thank the participants for their contributions to this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the HealthPartners Park Nicollet Foundation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical Trial Registration
NCT05230082
Data Availability Statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.