
Abstract
Background
In university and hospital workplace environments, high levels of stress coupled with physical and mental health issues are major drivers of employee health, healthcare costs, and workplace productivity. Workplace well-being programs can help employees manage stress and promote healthy behaviors. One approach to addressing stress and the physical and mental health of employees from a whole-person health perspective is integrative health and wellness coaching (IHWC). IHWC incorporates principles of motivational interviewing, positive psychology, transtheoretical model of behavior change and self-determination theory.
Objective
The purpose was to evaluate a novel IHWC program that included group coaching, individual coaching, and a post-program text message intervention to support the maintenance of program outcomes, at an East Coast university and its affiliated hospital.
Methods
The 12-week program consisted of 6 group sessions and 6 individual sessions followed by a randomized text message-based maintenance strategy between weeks 12 and 18. IHWC sessions were conducted by National Board-Certified Health and Wellness Coaches (NBC-HWC) and student trainees obtaining hours needed for eligibility for board certification (SHWC). Employee participants (n = 50) completed baseline and follow-up surveys at weeks 5, 12, 18, and 24. Outcomes included perceived stress measured by the Perceived Stress Scale (PSS-10), and mental and physical health measured by the Patient Reported Outcomes Measurement Information System (PROMIS-10).
Results
At baseline, employees in both the university and hospital setting reported moderate levels of stress, and perceived physical and mental health that were poorer than the national average. Multivariate analyses showed significant improvements in mental health, physical health, and stress scores from baseline to 12 weeks. Significant improvements endured at 18 and 24 weeks for physical health and stress, which were not enhanced by the text messaging intervention.
Conclusion
IHWC shows promise as an approach to support employees working in high stress environments.
Keywords
Introduction
Workplace environments play an influential role in creating positive or negative employee health experiences.1,2 Due to the high levels of work-related stress combined with the sheer amount of time individuals spend working, specifically 1757 hours on average, or 30% of waking hours, the workplace presents an excellent context to promote health, well-being, and behavior change.3-5 Some of the most common stressful workplace environments poised for practicing workplace wellness and well-being include academic and healthcare settings,6-9 where those with roles such as faculty, direct patient care, and administration report particularly high stress levels.10-12 Poorer health in these working environments increases risks for decreased productivity and increased costs of health care. 13
In response to growing recognition of workplace stress, the call for workplace well-being promotion is increasing in policy 14 and for-profit sectors, where workplace wellness is a $51 billion industry. 15 Evidence from a simulated analysis suggested that Fortune 500 companies with the highest self-rated employee health management practices have higher financial returns. 16 A variety of workplace well-being programs focused on improving the physical health, mental health, stress, and fatigue of employees have been described in current literature.17-25 Because of the heterogeneity in intervention type, target behaviors, outcomes measured, populations served, and scientific rigor, the impact of worksite well-being programs on employee health and wellness is difficult to measure. There also remains a lack of consistency in outcomes and implementation models that can be applied globally, especially in workplace settings like hospitals and institutions of higher education. 26 However, systematic reviews show evidence of benefit across numerous studies.26,27
While most employee well-being programs target specific behavioral outcomes such as exercise, 28 a major driver of employee health, healthcare costs, and workplace productivity is mental health and emotional well-being. 29 Therefore, program outcomes that include both physical and emotional well-being may be more advantageous to both employees and employee well-being program administrators. Approaching employee well-being from this more whole person approach is reported as best practice. 30
An approach to promoting healthy behavior that is considered best practice in other settings is Integrative Health and Wellness Coaching (IHWC).31,32 IHWC is a client-centered process wherein a client and clinician work together to advance healthy lifestyle behavior change with techniques such as goal setting, accountability, and nonjudgmental dialogue. 33 IHWC is an evidence-based practice based on the theories of positive psychology, 34 self-determination theory, 35 social cognitive theory, 36 motivational interviewing, 37 and the transtheoretical model of behavior change. 38 IHW coaches support clients using a whole-person approach that considers all domains of health including movement, nutrition, environment, relationships, personal development, spirituality, sleep & rest, and work-life balance.33,39,40 IHW coaches support individuals through the behavioral change process to help them achieve and sustain their personal lifestyle and health-related behavioral goals. 41 For this reason, comprehensive employee well-being programs grounded in IHWC principles would be expected to impact employee well-being broadly, compared with programs targeted at a specific domain such as exercise.9,42-45
IHWC can be effectively implemented at a group or individual level. Group coaching can reach more individuals, offer motivation through vicarious experiences and create a peer-supported environment for setting well-being intentions that improve self-efficacy, which is crucial for individuals seeking to practice healthy behaviors and promote whole-person health.33,46 In contrast, individual IHWC sessions provide an opportunity for vulnerability, intimacy, and self-focus with personalized guidance. Combining individual coaching with group coaching in a single program would conceivably allow participants to experience the ample benefits of each and could be an important strategy employed to sustain behavior change in the long-term.
Regardless of coaching modality, maintenance of program gains is notoriously poor and often requires more than one 12-week program.47,48 Few studies on IHWC have implemented a maintenance phase post-intervention and none provided a randomized intervention to assess its efficacy. In selecting a maintenance intervention to test, we sought a low-intensity intervention that could be motivating and provide an extended connection between participants and the behavior change program. Based on prior research on the feasibility and efficacy of text- and app-based interventions for physical and mental health,49,50 and findings from research in other disciplines showing that post-intervention text-based support can be a convenient way to support autonomy over health choices,51,52 we designed a text-based intervention.
The goal of this study was to test the effectiveness of a novel workplace IHWC program, the Employee Coaching Connection (ECC), and to assess the impact of text message follow-ups to improve long-term outcomes using an observational pre-post design with randomized text messaging conditions. The program was designed with the current best practices in mind to address the individual health related needs of the whole person. 30 The ECC included group coaching, individual coaching, and a post-program text message intervention to support the maintenance of program outcomes. It was hypothesized that (a) participants would increase physical and mental health and have reduced stress after the 12-week program, and (b) participants randomized to a 6-week minimal contact maintenance condition following completion of the 12-week program would continue to show improved functioning and stress levels compared to individuals who were not randomized to this maintenance condition.
Methods
Study Design and Intervention
This 24-week longitudinal pre-post program evaluation combined 12 weeks of IHWC, a 6-week randomized experimental maintenance component, and a final 6 weeks of observation only. The study design is depicted in Figure 1. Timeline of the Employee Coaching Connection Program and Survey Administration
Health and Wellness Coaching Program
The ECC was developed by a team of National Board-Certified Health and Wellness Coaches (NBC-HWC) and Employee Wellness professionals at a university and a university medical center. Feasibility of the program was tested in a pilot study. 40 Modifications to the ECC program were made based on feedback obtained from the pilot. Specifically, the groups were run as cohorts instead of rolling admission to allow participants to develop closer cohesion; individual coaching was added to the program to provide personalized guidance to complement the foundation in coaching principles provided in the group setting; and student coaches took a more active role, to allow them to gain more independence in their development as coaches.
The ECC program was guided by self-determination theory (SDT), which posits that well-being and sustained behavior change are supported when individuals’ basic psychological needs for autonomy, competence, and relatedness are met. 35 Both individual and group coaching were designed to create environments that foster these needs. By aligning the structure and facilitation of coaching with SDT principles, the program aimed to enhance intrinsic motivation and self-regulation, which are key to improving overall well-being and managing stress. This theoretical lens provides a foundation for interpreting observed changes in perceived physical/mental health and perceived stress, as measured by the PROMIS-10 and Perceived Stress Scale (PSS). The university has an educational program for health and wellness coaching students that involves 8 credits of required didactic education per the National Board of Health and Wellness Coaching guidelines taught in an approved program followed by 50 hours of coaching practice. The ECC is conducted jointly by NBC-HWCs and Student Health and Wellness Coaches (SHWC). A separate paper describes the ECC training model. 53
Group Coaching Sessions
Weekly group health coaching sessions co-led by a NBC-HWC and a SHWC were conducted using a video conferencing platform. The first 25 minutes of each one-hour session were large group work, followed by 30 minutes in small group breakout sessions. Small groups included about 4 employees, a NBC-HWC and a SHWC. In the last 5 minutes, the full group reconvened for a guided gratitude exercise. According to the framework of the SDT, these sessions added the dimension of relatedness, offered peer connection, shared experiences, and mutual support. The first 5 weeks of the program were in group format. Week 1 introduced the concept of multiple domains of health as seen on the Wheel of Health with a self-assessment for homework. Week 2 introduced the positive psychology concepts of strengths and values and how they can support the behavioral change process with the homework of identifying personal strengths. 34 Week 3 involved a guided visioning exercise to self-examine how life could look if changes in health behaviors were made, and assisted participants to understand their current stage in the behavior change process. 38 Week 4 involved discussions on determining importance and finding a focus or long-term goal for the duration of the program. Homework involved a worksheet on SMART Goals. Week 5 guided the employee through the process of breaking down the long-term goal into a small action step that the employee felt confident they could achieve.
Individual Coaching Sessions
Beginning at week six, participants met weekly with a SHWC for 20-minute individual remote coaching sessions. In individual coaching sessions, participants experienced autonomy through self-directed goal setting and competence through skill-building and progress toward personal health goals. SHWC were mentored by a NBC-HWC who would listen to the recorded sessions with the student and provide guidance. 53 At the sixth individual session, participants were invited to write six encouraging messages to promote intrinsic motivation for change and to help them sustain their focus on well-being after the program ended. 35 For the final (12th) session of the program, the participants reconvened as a full group for a closing session to celebrate participants’ successes, and to develop strategies for maintaining behavioral changes.
Throughout the group and individual sessions, the coaches’ communication style included motivational interviewing practices focusing on asking open ended questions, providing reflections and affirmations 37 while partnering with each participant to help evoke change. Since participation in the program was voluntary, most participants were in the contemplation or preparation stages of behavioral change as characterized by the transtheoretical model of change. 38 Coaches engaged participants according to their stage of readiness.
Maintenance
At the end of the 12-week synchronous coaching, participants were randomly assigned to a 6-week low-contact maintenance group or a control group. For the first six weeks of the maintenance phase (weeks 13-18), participants in the experimental group received one of their self-written messages each week from a program coach who sent them manually through SMS text, and control participants did not receive any additional contact. From weeks 19-24, none of the participants received contact from the program staff. At the final assessment, participants indicated whether they remembered receiving the weekly messages, and the extent to which the messages were helpful.
Recruitment
Starting in fall, 2022, an East Coast university and its affiliated medical center offered the semester-long ECC IHWC program as part of their Employee Wellness departments. All employees of the two institutions were eligible to participate in the ECC. The program was subsequently offered in successive academic semesters, a total of 4 times (fall 2022, spring 2023, fall 2023, spring 2024). Participants in the ECC were recruited to participate in a program evaluation study. Enrollment in the study was optional. The only criterion for inclusion in this study was to complete baseline surveys and at least one subsequent survey. This research was reviewed by the University of Vermont Committee for Human Research in the Behavioral and Social Sciences and found to be Exempt Category (2)(ii). Waiver of Documentation of Consent was approved under 46.117(c)(1).
Procedures
Employee participants were surveyed at baseline, 5, 12, 18, and 24 weeks (See Figure 1). All measures were administered at all 5 time points, with exceptions noted below. Employees were incentivized to complete surveys with a chance to win a $25 gift card for each survey completed. Enrollment in the study closed on the first day of the ECC program, and participants could withdraw from the research study at any time without withdrawing from the ECC program. Study data were collected and managed using Research Electronic Data Capture (REDCap), a secure, web-based software platform designed to support data capture for research studies. 54
Measures
Patient-Reported Outcomes Measurement Information System (PROMIS-10)
The PROMIS-10 is a 10-item person-centered measure of physical health, mental health quality of life, function, social activity, physical activity, and pain. 55 that has extensive validity evidence.56-58 It was chosen for this study because of its brevity and because it has shown sensitivity to change in other whole health coaching programs.9,40,59 The measure calculates overall scores in Global Mental Health (GMH) and Global Physical Health (GPH) and scores are converted to standardized T-scores with a mean of 50 and a standard deviation of 10. Higher scores indicate better health. Meaningful change is considered as 2-6 T-score points or .5 standard deviations, depending on the source.60-62
Perceived Stress Scale (PSS-10)
The PSS-10 is a 10-item questionnaire designed to assess an individual’s past-month experience of life stress. 63 The measure’s psychometric properties have been confirmed in numerous studies.63,64 It was chosen for this study because of its brevity and because it has shown sensitivity to change in other whole health coaching programs.49,59 Scores range from 0 to 40 with a higher score representing higher perceived stress. Scores between 0 and 13 indicate low levels of perceived stress, scores between 14 and 26 are considered moderate, and scores above 26 are considered high perceived stress. 65
Wellness Focus Area
A central concept in the ECC program is the Wheel of Health, which identifies 9 domains of health that comprise personal well-being. 40 A single question asked, “What area of health from the UVM Integrative Health Wheel of Health are you working on? You may choose more than one.” Options were work life balance, mind and body, movement, nutrition, environment, relationships, personal development, spirituality, and sleep and rest. This item was assessed at the 5 and 12-week surveys.
Statistical Methods
Descriptive statistics were conducted to assess the demographic characteristics of the employee participants across sites. For the mixed model analysis, SPSS Statistics [version 29.0.2.0, IBM Corp., Armonk, NY] was used. Multiple mixed models were run to analyze PROMIS-10 physical health and mental health, and PSS-10. The general form of the mixed models included work site, maintenance condition (texted vs not texted), age and week of survey deployment. Participant IDs were considered the only random effect. Significance was assessed at alpha = 0.05. We evaluated the intervention’s effects on three distinct outcomes—stress, physical health, and mental health—using separate statistical tests for each. An unadjusted alpha level of 0.05 was applied to each test. Following García-Pérez, 66 adjustments for multiple comparisons are not required when each outcome is analyzed independently and reported with separate inferences rather than as part of a collective omnibus hypothesis. Since we make distinct claims about each outcome, the Type I error rate of 0.05 applies individually to each test. An a priori power analysis was not conducted for this study.
This evaluation was designed as a pragmatic, observational study to examine the real-world implementation of the ECC program. As such, our dataset includes all eligible participants who enrolled in the ECC program across one of four academic semesters, consented to the research and completed the required surveys. This approach reflects the applied and exploratory nature of the study, which prioritized ecological validity and feasibility over hypothesis-driven sample size estimation. Although the absence of a formal power calculation limits statistical inference, the observed trends and statistically significant changes across time points provide meaningful insight into the program’s potential effectiveness in a workplace setting. Additionally, cohort was not included as a covariate in statistical models. All cohorts were combined for analysis due to consistency in program facilitators, structure, and participant characteristics across semesters. While we recognize that seasonal variation in affect may occur—particularly in northern climates where affect tends to decline in fall and improve in spring—our cohort distribution included two fall and two spring semesters, which we anticipated would balance potential seasonal effects. Given the small sample size, adjusting for cohort would have further reduced statistical power.
Randomization
Participants who completed the ECC program were randomized into the text message follow-up and control conditions at week 12. All participants received the same ECC program content and assessments at weeks 0, 5, and 12, ensuring equivalent baseline exposure across groups. At week 12, all eligible participants were entered into an Excel spreadsheet and assigned to groups using a random number generator. No blocking or stratification was applied.
Results
Employee Demographics and Response Rates
Participant Demographics

Wellness Focus Area
Participants could choose more than one area to focus on during the program. At both the 5-week assessment and 12-week assessments, the most frequently selected focus areas were movement (n = 51/87), nutrition (n = 37/87) and sleep (n = 30/87).
PROMIS-10 Physical Health and Mental Health
PROMIS Global Physical Health (GPH) and Global Mental Health (GMH) T-scores are standardized to a U.S. general adult population mean of 50 with a standard deviation of 10, based on a large and demographically diverse sample reported by Hays et al.
55
While not official normative benchmarks, these values allow for approximate comparisons to national averages. Raw mean T-Scores on the PROMIS-10 GPH and GMH at each assessment are graphically displayed in Figure 2. As shown, baseline mean GPH T-score (46.67) and GMH T-score (46) were both below the national average of 50. At the end of the program (week 12), mean GPH T-score increased by an estimated 2.3 points, significantly higher than baseline (95% CI [0.54, 4.00]). GPH T-scores at 18 and 24 weeks remained significantly higher than baseline (P < .001). GMH T-scores increased by an estimated 2.3 points at 12 weeks (P = .01). Mean GMH T-scores at week 18 were not significantly different from baseline. At week 24, a marginal increase of 1.8 points was observed (95% CI [−0.01, 3.60]). Mean Patient Reported Outcomes Measurement Information System (PROMIS-10) Global Physical Health (GPH) and Global Mental Health (GMH) T-Scores at Each Assessment Period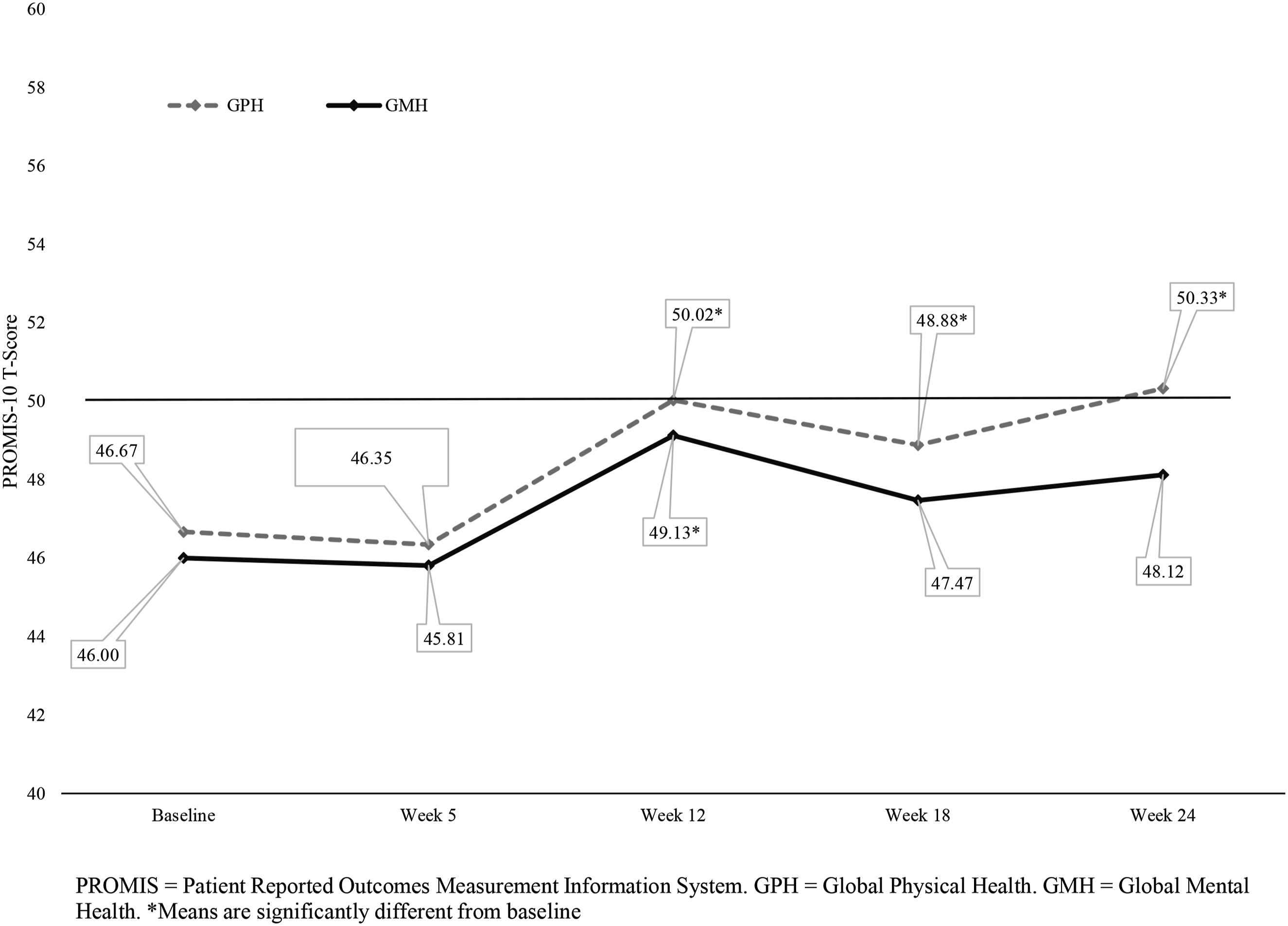
Mixed Model of Fixed Effect for PROMIS GPH T-Score and PROMIS GMH T-Score

Note. PROMIS GPH = Patient Reported Outcome Measurement Information System Global Physical Health scale; PROMIS GMH = Patient Reported Outcome Measurement Information System Global Mental Health scale. *Indicates the result is statistically significant (alpha <0.05).
PSS-10
Raw mean PSS-10 scores at each assessment period are shown in Figure 3. Results of the mixed model analysis of PSS-10 scores are shown in Table 2. PSS-10 scores were not significantly associated with work site, age, text message condition or 5-week assessment, but they were significantly lower at the 12-week, 18-week and 24-week assessment periods, compared to baseline. On average participants reported moderate stress levels at baseline and week 5. Levels were in the low stress category for weeks 12, 18 and 24. Mean Perceived Stress Scale Scores at Each Assessment Period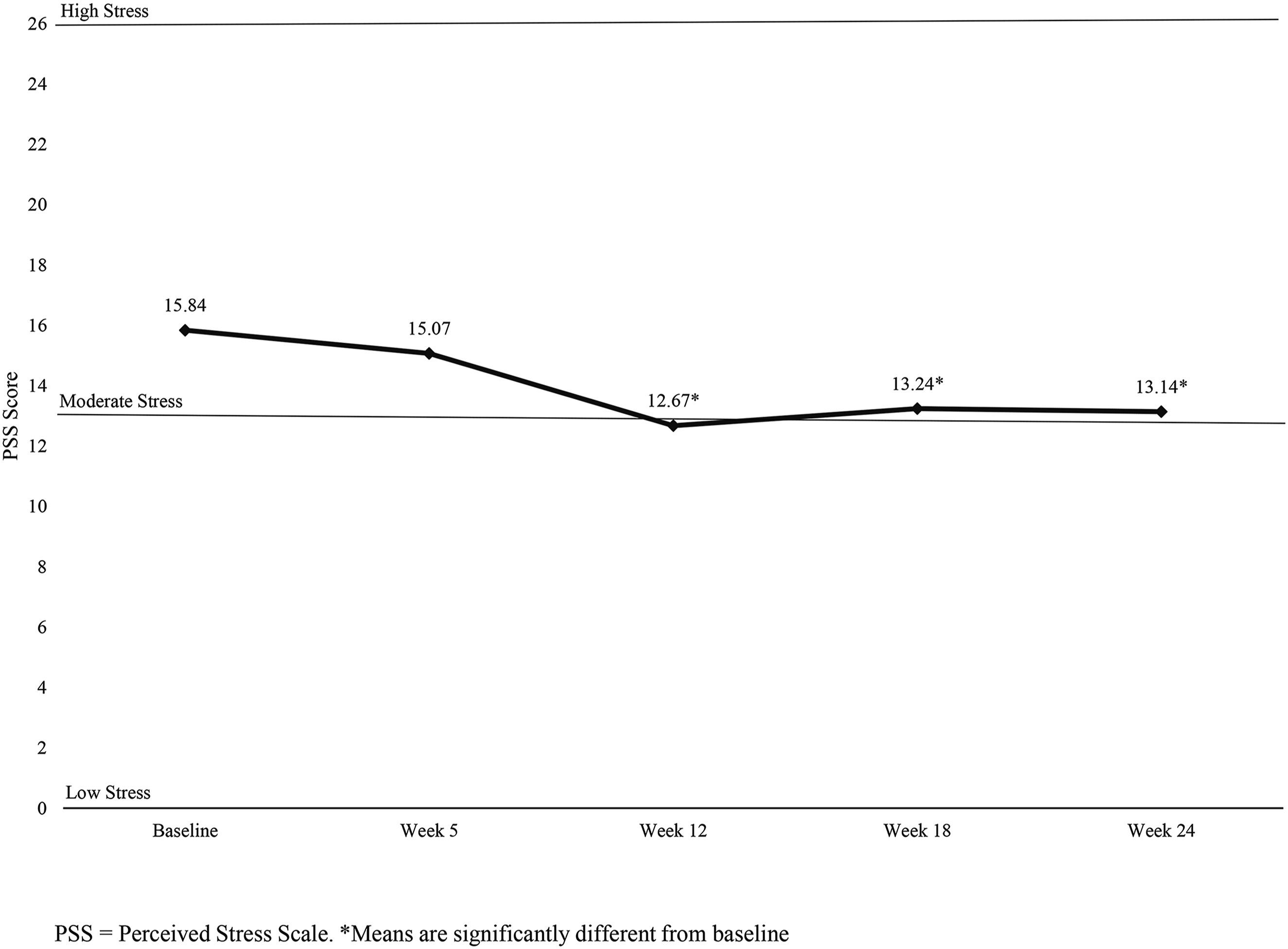
Post Hoc Analysis
Most employees who participated in the ECC were female (n = 45, vs 5 who identified as male or non-binary gender). Although this study’s objective was not to investigate gender differences, an exploratory descriptive comparison of PROMIS-10 GPH T-Scores by participant gender was conducted to better understand the experiences of female and non-female participants in one of the primary outcomes. Due to sample size considerations, male and nonbinary participants were grouped. Mean PROMIS-10 GPH T-Scores showed nearly the same linear pattern over the 5 assessment periods for both gender groups, but females’ mean T-scores were consistently higher, between 3.61 and 9.19 points depending on the assessment period. The extent of difference represents approximately one-third to nearly one full standard deviation. See Supplemental Figure 1.
Maintenance Phase
Demographics and Baseline Scores of Participants Randomized to Text Message vs Control Maintenance Conditions

Note. PROMIS GPH = Patient Reported Outcome Measurement Information System Global Physical Health scale; PROMIS GMH = Patient Reported Outcome Measurement Information System Global Mental Health scale. PSS = Perceived Stress Scale.
Discussion
The ECC program showed robust temporal change in physical health, mental health and stress outcomes during the active 12-week program. The physical health and mental health scores increased from about one-third standard deviation below national average at baseline to almost exactly the national average at the end of the program. Stress scores changed from moderate to borderline-low at 12 weeks. In contrast with other studies that implemented experimental test message-based post-program interventions to maintain post-program outcomes, 51 in this study the control group and experimental group both maintained post-program outcomes, suggesting the ECC alone was sufficient for maintenance.
The ECC expanded earlier IHWC research to the employee well-being context and blended several novel components including (a) group plus individual coaching formats to provide both peer support and personalized guidance, (b) NBC-HWCs accompanied by SHWCs obtaining hours required for certification to expand the workforce and provide valuable clinical experience, (c) collaboration between two different workplaces with unique job demands and organizational cultures, and (d) a randomized maintenance component designed to maintain contact between the employee and their coach. Aligning both coaching formats with the SDT principles created an intervention that supported internal motivation and adaptive coping; mechanisms likely reflected in improved PROMIS and PSS scores. This philosophy of autonomy was oriented to whole person health and received strong leadership support, which are identified best practices in workplace wellness. 30 Unlike traditional programs that focus on one or more singular outcomes, the ECC’s approach embraced behavioral goal attainment as an important but not primary objective. Some participants chose multiple areas of well-being to focus on, either simultaneously or sequentially, which increased pragmatism but at the expense of rigorous evaluation of behavior change goal attainment.
The outcomes measured in this study are highly relevant to employee productivity and personal health, in particular stress reduction, which has been demonstrated to reduce incidence of chronic disease.67-69 Furthermore, our results align with emerging research that supports positive impact from individually focused interventions, including health and wellness coaching, on reducing stress and improving mental well-being.70,71 The uniqueness of the ECC program is that improvements in physical health and stress were sustained for 12 weeks after the program concluded. This is a crucial finding as many studies lack long term follow up data. 70 This suggests that the IHWC model with its whole person, self-determination theory grounded approach may be particularly effective for long-term behavioral change. 33
Strengths
First, including participants and coaches from two different institutions strengthened the program because it allowed for cross-institutional collaborations and an emphasis on the value of employee well-being regardless of the setting. While each institution had its own distinct employee well-being program, the two programs had consistent goals and values. The ECC NBC-HWCs from both institutions collaborated to develop and implement the program. The virtual format of the ECC allowed all participants to conveniently participate, theoretically allowing the program to be scalable to other regions and employers. Second, the reliability of these findings is enhanced by including data from 4 cohorts over 2 years, which minimizes the influence of secular trends, cohort effects, or seasonal factors on the results. Third, the response rates for the midpoint (5-week) and post-program (12-week) surveys was 90% and 86%, respectively, which is generally considered high. A fourth strength was the random assignment of participants to the text-message intervention vs no-text control condition. This allowed us to conclude that the positive follow-up findings were not a result of the text messaging intervention as implemented.
Limitations
First, the generalizability of results is limited by the small homogeneous sample that was predominantly female and likely skewed to higher education levels. Other studies have similar gender ratios,72,73 suggesting that employee well-being programs consistently attract more women. A post-hoc analysis showed that women in this sample had higher self-reported physical health than men and non-binary participants at baseline, during the program, and at all follow-up assessments. It is likely that our recruitment resulted in a self-selected sample of employees already interested in health and wellness.
Second, the coaching intervention portion of this study was observational, limiting our ability to prove causality. However, the observed changes were strong and in the expected direction, both during the program and after completion when participants were not receiving additional support from program staff.
Third, our survey obtained few demographic characteristics. This decision was made to reduce participants’ concerns about confidentiality. This is a small sample of individuals in a predominantly white, non-Hispanic region, so racial and ethnic data might make individuals’ identities identifiable. However, absence of these characteristics reduces our ability to contextualize our findings and identify race-based directions for future research.
Fourth, our outcome measures were self-reported and broad in scope. More refined measures of specific health and wellness outcomes might have enabled us to detect specific changes that would allow for stronger conclusions.
Finally, participants’ engagement in the experimental maintenance condition was low, due in part to features of the ECC design and research study coordination. Notably, the text messages were part of the research and not specifically part of the coaching curriculum. The timing of requesting the messages coincided with the last SHWC-run individual session that focused primarily on reviewing progress and bringing the individual sessions to a close. In this context, the extra request for participants to generate encouraging messages for the research study was at times overlooked. While in some cases the SHWC or NBC-HWC reached out to the participant afterward to request these messages, response to that outreach was low. In addition, some participants chose not to write messages even when offered per protocol, and the response rate to the final survey (73%) was below the generally accepted standard of 80%.
Directions for Future Research
Despite our null findings for the maintenance intervention, the success of text message-based interventions in other fields suggests that they are worthy of ongoing study.48,49 For example, future studies could evaluate a more seamless integration of message writing into the coaching curriculum itself and could investigate the efficacy of a longer maintenance phase. Future studies also could evaluate bi-directional electronic engagement with coaches and participants during the maintenance phase, which could contribute to the understanding of challenges associated with maintaining new health behaviors. More research is needed to investigate the efficacy and implementation of maintenance interventions in employee well-being program design.
Methods for improving the measurement of behavioral goals and their achievement in the context of a whole-health focused coaching program should be explored further. The ideal measurement strategy would reliably assess the heterogeneity of goals over time in a way that minimizes recall bias. A balance between feasibility, pragmatism in program design, and opportunities for improved reporting consistency was sought in this study; however, improvements are required for ongoing evaluation of the ECC program and its potential benefits to university and medical center staff.
Research could be invested in understanding how to engage employees in workplace HWC initiatives. A number of implementation strategies for promotion, marketing and recruitment, and determining employee priorities and values32,74 could be tested empirically. In this study, the two organizations collaborating on the ECC employ approximately 14 000 individuals and the program was available to all of them. Yet, only 50 employees enrolled in the ECC over two years, most of them women. This is not unique to the ECC: Participation rates reported in other programs range from 10-64%,75-77 and they are even lower for men. The consistency and magnitude of this gender difference suggests that efforts to understand the factors behind this difference, and strategies to design and promote programs that attract all genders, should be explored. While implementation of HWC in the workplace can improve health outcomes for employees, the mere availability of a program does not automatically lead to engagement and participation. 78
Finally, randomized trials that include a control group are needed to better evaluate the program’s efficacy and rule out regression to the mean as a causal explanation. Research with a dismantling design could help identify the most influential components of the program.
Conclusion
In conclusion, this novel 12-week workplace-based program that combined individual and group IHWC led by NBC-HWC and SHWC and a randomized post-intervention maintenance intervention showed pre-post improvements in stress, physical and mental health, and improvements in stress and physical health that endured for 12 weeks after the program concluded but did not support an additional benefit of the maintenance intervention. These results support the value of promoting employee health in a way that serves the needs of the individual through a whole person approach and suggest that a post-program intervention may not be necessary to sustain changes. Given the difficulty in implementing programs that help people to sustain new skills and behaviors, our results are promising and suggest that IHWC in both group and individual format should be continued at the host institutions and trialed in other workplaces to support employee health.
Supplemental Material
Supplemental Material - Impact of an Employee Health and Wellness Coaching Program on Self-Reported Stress, Physical Health, and Mental Health in Hospital and University Employees
Supplemental Material for Impact of an Employee Health and Wellness Coaching Program on Self-Reported Stress, Physical Health, and Mental Health in Hospital and University Employees by Gail L. Rose, PhD, Alyssa Smith, MS, OTR/L, NBC-HWC, Jurdan Mossburg, DPT and Karen Westervelt, PhD, PT, ATC, NBC-HWC in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgements
An important facilitator of the implementation of this employee well-being program was the leadership support we had from the University Provost, who is a strong supporter of well-being initiatives. In addition, the employee wellness departments at the institution financially supported the program’s operation. The authors also acknowledge the contributions of Ally Dovano, Sara Falconer, Kyler Huffert, Mackenzie Lillis, Abigale Whitman, Ashlyn Woods, Ashley Pelkey, Gina Russin, and Emma Severn to an early draft of this manuscript.
Ethical Considerations
This project was reviewed by the University of Vermont Committee on Human Research in the Behavioral and Social Sciences and found to be Exempt Category (2)(ii).
Consent to Participate
A consent form preceded the survey which stated that completion of the survey was considered implied consent to the study. University of Vermont Committee on Human Research in the Behavioral and Social Sciences approved a Waiver of Documentation of Consent under 46.117(c)(1).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: GR received internal funding to support her effort on this research. KW, AS, and JS received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data can be shared upon reasonable request. Please contact the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.