
Abstract
Introduction
This study aims to comprehensively evaluate health care access and utilization in rural Pakistan, shedding light on the multifaceted challenges and opportunities within the health care landscape. It explores the healthcare-seeking behaviours of individuals, particularly focusing on underserved populations.
Methods
The study employed a qualitative data collection method. Focus Group Discussions (FGDs) were conducted to gather qualitative insights. Data were analysed using thematic content analysis allowing for a comprehensive understanding of health care challenges.
Results
The study reveals significant findings, including limited healthcare-seeking behaviours due to financial constraints, lack of health insurance, and distrust in health care systems. Government health care facilities in rural areas were perceived as inadequate, with under-resourced staff and subpar quality of care. Participants expressed support for medical camps and educational sessions to address these issues.
Conclusion
This study provides critical insights into rural Pakistan’s health care access and utilization challenges. Policymakers, health care practitioners, and community leaders can draw from these findings to formulate effective strategies for improving health care access and outcomes in underserved rural areas.
Introduction
The burden of diseases is significantly rising in Pakistan. With the government developing vertical programs to target communicable diseases, the burden of non-communicable diseases is also rising due to lifestyle changes. According to World Health Organization (WHO) Noncommunicable Diseases (NCD) country profiles in 2014, 38% of the health burden is attributable to communicable and 49% to non-communicable diseases in Pakistan. 1 Health care, a basic human right, continues to suffer due to the changing socioeconomic conditions of the country. 1 of the 17 sustainable development goals, which was embraced by the United Nations in 2015, is to decrease inequalities. 2 Health care disparity is defined as discrepancies in inaccessibility to medical services, prevalence of diseases and disablement between different societies due to a range of socioeconomic and cultural factors. Health care inequality has been a concern for the longest time in Pakistan. Those living in rural areas are more susceptible to diseases due to the lack of sanitation, poor nutrition, decreased literacy, lack of clean drinking water and reduced income. In addition to this, crowded living spaces increase the risk of transmission of diseases. According to a Lancet study in 2016, Pakistan is ranked 154th out of 195 countries in the quality and accessibility of health care. 3 It shows that there has been improvement since 1990 but the Health Assessment Questionnaire (HAQ) has increased to only 37.6. 4
The United Nations (UN) annual report of 2021 shows that 1 in 4 Pakistanis experience poverty. 38.3% of the population is ‘multidimensionally poor.5,6 There have been various studies that show poverty to be associated with worse health-related outcomes so much so that it is also 1 of the seventeen goals of the SDGs.5,6 Pakistan also ranks as the fifth most populous country in the whole world. 7 Needing to cater for a greater number of people burdens this already collapsing health care system, increasing inequality. In addition, there is the growing issue of a shortage of health care workers, especially in the rural areas. 7 This wouldn’t only lead to discrepancies in preventative care but would also cause exhaustion among existing health care workers. Primary care medicine plays a vital role within the health care system, as research indicates that a greater presence of health care professionals in this field would substantially diminish disparities and enhance overall quality of life. 8 Nevertheless, there is a noticeable shortage of primary care providers. 9 There are also differences in the provision and access of health care facilities to women. It has been reported that women have increased hindrances to accessing health care.10,11 This is due to a multitude of factors including a lack of access to education and autonomy. 3 Not surprisingly, lack of female autonomy is also linked with poorer health outcomes for their children, further increasing its importance. 12 A study including 4 districts in Pakistan showed that having a literate mother was associated with receiving measles vaccine. 13 Other factors that come into play are the distance and location of the facility and the services provided by them. 10 Kennedy et al showed that increased distances from health care facilities resulted in lower usage of antenatal services. 14 Pakistan was at 149th position out of the 179 countries in maternal mortality rate. 4
Pakistan is among the countries which spend the least on their health care. Its health care system is divided into private and public sectors. Within the public sector, at the primary level, there are local pharmacies, basic health care units and rural health care units with supposedly more services. At the crux of the primary health care services are the lady health care workers who go door to door, providing basic services and creating awareness. At the secondary level are tehsil and district headquarters. Lastly, located in the major cities are teaching hospitals at the tertiary level. The private sector consists of major for-profit and some non-profit organizations. A study conducted by Khalid et al reports that 70% of the Pakistani population uses private-sector services. 15 This can be due to the lower quality of services provided by government-run health care institutions. Another study reported greater patient satisfaction from utilizing private health care establishments. 16 This results in a lot of Pakistanis, visiting private sectors in the hope of better service, suffering from financial burden when having to pay out of pocket. This further destabilizes their financial stability, increasing poverty. Those who cannot afford are left in the hands of the public health sector which most often than not, fails to deliver.
In times of rising crisis, there are a few philanthropic institutions that have come into being, merely by their efforts. They have employed different frameworks to try and alleviate the health care burden. One such initiative is student-led clinics. These are clinics that are planned, managed, and run on the ground, by medical students. They are intended to target locations which suffer from increased disease burden. On the ground, clinical year medical students assume a pivotal role in gathering patient histories, performing examinations, and developing a list of differential diagnoses. They are always observed and guided by medical personnel. The services provided here are free of charge. The cost of medications, equipment, and transportation is all arranged by medical students by raising donations. Sustainability is ensured by having these clinics every 2 or 3 weeks. This framework intends to decrease health care disparities along with providing essential skills to medical students. Student-led clinics have been implemented in other countries in the past for health care delivery in marginalized communities and have been proven to be an extremely economical approach to addressing health care disparities.17,18 A review conducted by Patrick et al suggests ‘positive health outcomes resulting from student-run clinics across a range of health conditions’. 19
The primary objective of the study is to identify the main challenges and consequences regarding health care access and availability faced by rural communities in a low-middle-income country, Pakistan, from the perspective of the community itself through focused group discussions (FGDs). The rationale of the study is to understand factors influencing healthcare-seeking behaviour, evaluate the perceptions about government and private health care practices, and analyse community needs and preferences as these may be significantly affected by financial constraints, inadequate infrastructure, and systemic issues in rural areas. Despite various initiatives, such as student-led clinics, which provide essential health care screening services, persistent gaps remain in understanding the broader community’s needs. By gathering qualitative insights from FGDs conducted during such medical camps, the study aims to uncover specific barriers and generate actionable recommendations to improve health care delivery. The findings will be valuable for policymakers, health care practitioners, and community leaders in developing targeted, evidence-based interventions that address the unique challenges of rural areas. Ultimately, this study seeks to enhance health care access and equity, contributing to more effective and sustainable solutions for underserved populations.
Methods
Study Design
The study employed a qualitative data collection method to assess health care access and utilization within the target community comprehensively. Focus Group Discussions (FGDs) were conducted to gather qualitative insights for health care intervention planning.
Data Collection Method
Focus Group Discussions were conducted at the proposed site of a Student-Led Clinic under the leadership of Humanity Initiative which is a Non-Governmental Organization working in Pakistan for conducting Students-Led Clinics. FGDs were conducted before the decision to arrange a medical camp to gather qualitative insights into the health care needs, challenges, and preferences of the community. Focus group discussions were chosen for their ability to elicit comprehensive, in-depth, and collective insights into shared experiences. 20 Demographic diversity in group composition was used to capture a wide range of perspectives, consistent with best practices in qualitative public health research. 20 Participants for the FGDs were selected through purposive sampling, considering inclusion criteria such as residency in the target community and willingness to participate.
Participants were encouraged to participate through the local community leaders who acted as point-of-contacts for us and helped advertise for us. The participants were divided into 4 groups based on demographics, including age and gender: adolescent group, adult male group, adult female group and combined group (consisting of both male and female members of the community). FGDs were conducted in 2022 in a neutral, accessible community setting, with each session lasting approximately 60-90 minutes.
Trained moderators facilitated the FGDs using semi-structured guides. Moderators underwent a structured training program, which included sessions on qualitative research techniques, active listening, and strategies for minimizing interviewer bias. Training also covered cultural competency to ensure that discussions were conducted with sensitivity to local customs, linguistic variations, and health care beliefs. To refine the methodology and ensure the clarity of discussion prompts, a pilot FGD was conducted with a small subset of the community, which included elders of the community, before full-scale data collection.
Inclusion criteria were set to include those who were residents of the community, had experience with health care services in the area, and were willing to participate in a group discussion. Exclusion criteria included individuals with severe communication barriers or cognitive impairments that would prevent meaningful engagement in FGDs. Efforts to minimize selection bias included outreach through local community leaders and health centers to recruit participants who might not otherwise be engaged in such research.
Open-ended questions encouraged participants to share their experiences, views, and suggestions regarding health care access. Sample questions included, “What barriers do you face when accessing health care?” “How has the financial burden impacted your health care choices?” and “What sources of support do you rely on for health-related information?” This structure provided a balance between open-ended exploration and focus on the study’s primary themes, while allowing emergent issues to surface during the discussion.
Data Analysis Method
For data analysis, an inductive thematic analysis approach was employed, and carried out using NVivo v12.2, allowing themes to emerge organically from the data rather than being pre-determined by existing frameworks. The analysis was informed by Braun and Clarke’s six-step framework, including familiarization with data, generating initial codes, searching for themes, reviewing themes, defining and naming themes, and producing the final report. Two independent coders reviewed and coded the transcripts, with regular consensus meetings held to resolve discrepancies and ensure reliability. Participant quotes were carefully selected and integrated within the text to support each thematic finding, contextualizing them within broader patterns observed in the data. This approach enhanced the flow of the results section and ensured that the findings were presented coherently, highlighting the interconnected nature of the themes. Data saturation was considered achieved when no new themes or subthemes were emerging from the FGDs, and thematic repetition was noted across demographic groups. This was monitored iteratively by the research team during transcription and coding.
Ethical Statement
This study adhered to the highest ethical standards in research involving human participants. The ethical exemption was obtained from the Humanity Initiative Ethical Review Committee before initiating data collection. The study received ethical exemption as it was considered minimal-risk community-based research involving non-invasive methods. All participants provided informed consent before participating in the FGDs. For participants under 18 years of age, verbal assent was obtained along with verbal informed consent from a parent or guardian prior to participation in the FGDs. Participation was voluntary and confidentiality was strictly maintained, and data were anonymized for analysis and reporting. Participants were assured of their right to withdraw from the study at any point without consequences. Additionally, the study ensured that the health care intervention was culturally sensitive and respectful of local customs and traditions. All efforts were made to minimize any potential harm to the community and to maximize the benefits of the research findings for health care improvement.
Results
FGD Results
Demographics of Adolescent Group.

Demographics of Adult Male Group.

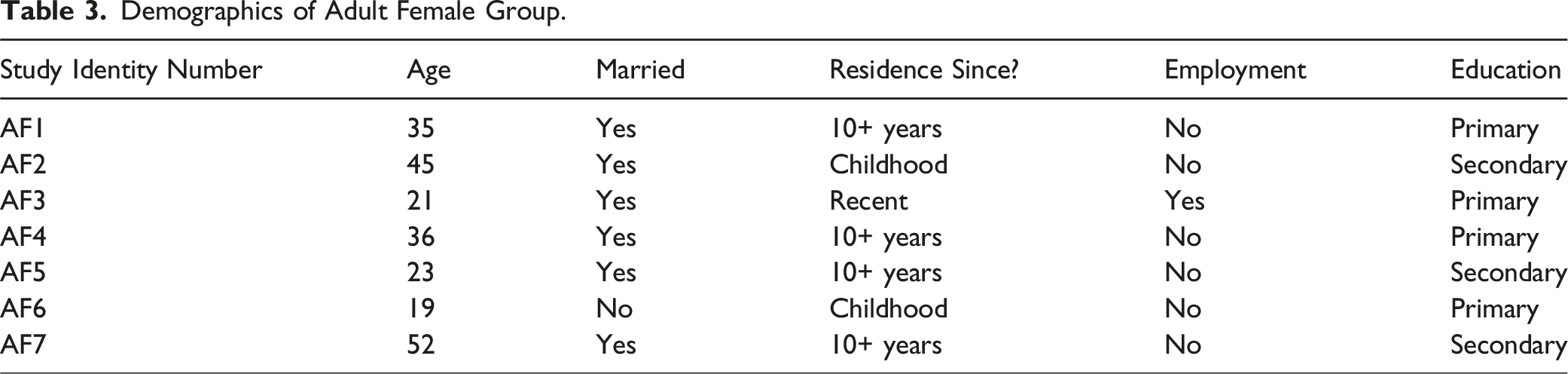
Demographics of Adult Female Group.
Demographics of the Combined Group.

FGD Key Themes and Findings
The findings from the Focus Group Discussions have been categorized into multiple different themes. These themes were expressed by some patient groups isolated and some shared by multiple groups (including adolescents, adult women, and adult men’s perspectives).
Health care Seeking Behaviour and Access
Participants across all demographic groups consistently identified major barriers to accessing health care, including financial constraints, geographic inaccessibility, and poor service quality. Many respondents reported resorting to self-medication or visiting unqualified practitioners due to the unaffordability or inaccessibility of formal care. For example, adolescents shared that hospital visits were rare and typically delayed until symptoms worsened, with parents often making the final call regarding treatment. “We usually just take medicine at home unless it gets really bad,” one adolescent noted, highlighting a trend toward informal self-care practices.
Among adult males, prevalent complaints included gastrointestinal disturbances, high blood pressure, and palpitations. However, they voiced strong distrust of government health care services, which were perceived as overcrowded and staffed by indifferent personnel. “Doctors don’t listen; we wait hours and still don’t get proper care,” one participant explained, reinforcing why many prefer to seek help from small, often unlicensed, clinics. Similarly, adult females emphasized the challenge of accessing essential medications and the financial strain of hospital visits. A female participant (AF3) recounted how her family frequently had to skip treatment altogether due to cost: “Medicines for major illnesses are not easily available in the area,” she said, underscoring the need for more affordable and accessible care.
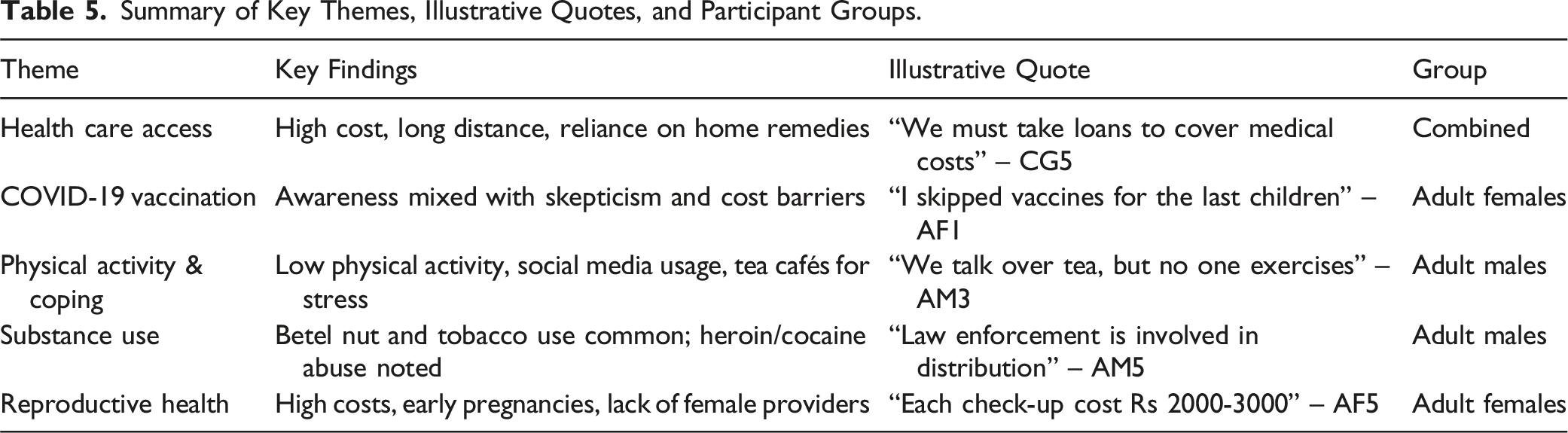
In the combined group, concerns about emergency care emerged. Participants described the absence of 24/7 clinics and the difficulty of obtaining transport at night, with several stating that they relied on home remedies until morning. “If a severe issue arises, we must take loans to cover medical costs, making repayment difficult,” (CG5) a male participant explained. There was overwhelming support for free community health camps, particularly those offering care for chronic illnesses, children, and mental health needs. As a partaker (CG3) summed up, “We need free clinics, especially for sick children and long-term illnesses. Mental health support is also essential.”
COVID-19 Awareness and Vaccination
Awareness of COVID-19 varied widely, with general acceptance of vaccination observed across groups, though not without skepticism. Among adolescents, some exhibited misconceptions about the virus and its vaccines. One participant even stated, “Vaccine leads to death in 2 years.”
Adult male participants reported being vaccinated but questioned the vaccines’ effectiveness, particularly when individuals contracted COVID-19 post-vaccination. A health care worker (AM7) expressed concern, stating, “Expired vaccines were used for some individuals.” Adult females emphasized cost as a barrier to vaccination continuity. One woman (AF1) remarked, “I vaccinated my first 2 kids but skipped the rest because I didn’t think it was necessary.”
Physical Activities, Social Interactions, and Coping Mechanisms
Recreational opportunities were notably lacking across all demographic groups. Adolescents described limited physical activities, often restricted to informal games like cricket. Many spent substantial time on digital platforms like TikTok and mobile games. One adolescent shared, “We play online games and talk to friends when stressed,” highlighting a digital coping mechanism. Discussions with parents were also identified as a source of support.
Adult males admitted they did not allocate time for physical exercise, despite recognizing the importance of healthy habits. Most relied on social interactions, such as gathering at tea cafés, as their primary method of coping with life stressors. One adult male noted, “We talk over tea, but no one exercises.”
Substance Use and Addictions
Substance use, particularly of tobacco and betel nuts, was common among adolescents and adult males. Four of ten adolescents disclosed using such substances, including one girl (AD9) who stated, “I consume churran (tobacco).” Adult males acknowledged widespread use of cigarettes and betel nuts and pointed to rampant drug abuse, including heroin and cocaine, within the community. As one participant (AM5) noted, “Drug issues are rampant because law enforcement is involved in distribution.”
Female Reproductive Health
Female participants expressed significant concerns regarding reproductive health and pregnancy-related care. High costs and the unavailability of specialized female providers deterred many from seeking adequate prenatal care. One woman (AF5) described, “Pregnancy check-ups cost Rs 2000 per visit, plus Rs 3000-3500 for medicines each month. Many here cannot afford that.” While adult males expressed supportive views about maternal health, they were largely uninvolved in actual care. Women also reported frequent miscarriages and early pregnancies, as well as reliance on local foods like potatoes and cereals for postpartum nutrition. Another woman (AF3) shared, “I had a miscarriage, and the doctor charged me Rs 7000 for the procedure.”
Community Health care Needs
There was widespread agreement on the need for accessible, affordable, and comprehensive health care services. Participants described a lack of 24/7 clinics and difficulties securing transport, especially during emergencies at night. As a result, home remedies were commonly used until care became unavoidable.
One participant (CG3) emphasized the urgency: “Free clinics are needed a lot, but we need specific services like treatment for sick children and long-term illnesses. We need doctors to provide mental health support.” Others lamented the inadequacies of government hospitals, describing long queues and substandard care. Another (CG7) added, “We need more female doctors in the community” to ensure women feel comfortable seeking medical attention.
Summary of Key Themes, Illustrative Quotes, and Participant Groups.
Discussion
The discussion for this study is presented in 2 parts. The first part describes the key themes and findings identified from the community’s perspective concerning the challenges they face while seeking health care. The second part discusses the integration and implementation of the findings of these focused group discussions in planning future medical camps and student-led clinics.
Part I: FGD Key Themes and Findings
Health care Seeking Behaviour and Access
Regarding healthcare-seeking behaviour and access, one of the findings to note was that most individuals did not seek health care for their ailments. This behaviour can be attributed to the fact that without any health care insurance, the visits to the hospitals become an additional financial burden to the people already living in poverty. The people have to self-finance their hospital visits, medications as well as transport costs since there are very less health care facilities available in nearby areas. These reasons are supported by a study that suggests that lack of health literacy, financial constraints, or distrust in health care systems may be the cause of delayed hospital visit. 21
Our findings indicate that socioeconomic factors play a critical role in shaping health care access and overall health outcomes within this community. The financial burden faced by many individuals not only limits their ability to seek timely medical care but also exacerbates issues related to addiction. 21 For instance, financial constraints often drive individuals to seek relief from stress and hardship through substances, which can lead to or worsen addiction. 21 This, in turn, can further strain financial resources due to the cost of substances and potential health care costs associated with addiction-related health issues. 6 Consequently, this cyclical relationship creates compounded barriers to health care access, as those burdened by both financial instability and addiction are less likely to prioritize or afford medical care. This interplay of socioeconomic adversity and health-seeking behavior reinforces health care disparities within marginalized populations, perpetuating a cycle of poor health outcomes. 15 Addressing these interconnected factors is essential to designing effective interventions that reduce health care inequalities and improve the quality of life for underserved communities.
People also had concerns about the government health care facilities not being up to the mark where the staff is usually unresponsive, not attentive and has rude behavior. Some reasons why that might be the case are that the government facilities in rural areas are often understaffed due to which the health care workers must deal with a larger burden of patients. They are often also underpaid and overworked which is why they are not able to deliver quality health care. The lack of resources and equipment in the government facilities also adds to the levels of frustration. It is suggested that to improve the health care services in rural areas the government must be more involved in addressing these challenges. In general, the population was very supportive of medical camps that would deliver educational and awareness sessions regarding the prevention of communicable diseases through contaminated food and water as this was recognized and accepted as a major issue in rural settings. This positive attitude of the community towards learning should be encouraging for people setting up medical camps in the area. Overall, the findings of this section highlight the complex interplay of socioeconomic and health care system factors in healthcare-seeking behaviour and access. Addressing these challenges requires a multifaceted approach that includes health education, community engagement, and health care system reforms to ensure equitable access to quality health care.
COVID-19 Awareness and Vaccination
Regarding COVID-19 Awareness and Vaccination, it was encouraging to note that amongst the population there was a general acceptance of vaccination as a preventive measure. This emphasizes the positive impact made by the immunization programs. However, there were still certain concerns regarding the effectiveness of the vaccine and the use of expired vaccines highlighting potential issues in the supply chain, storage, and distribution of vaccines. To deal with the scepticism, it is important to ensure quality control of vaccines throughout the supply chain and at vaccination sites to maintain public trust in immunization programs. Some people believed that the pandemic had ended while others believed that the vaccine could lead to death in 2 years. All these ideas indicate a potential gap in information that needs to be addressed through targeted health education campaigns at different age group levels. A point of concern raised by the female group was that they would fully vaccinate their first 1 or 2 children but did not do the same for the other kids. This can be a result of the lack of accessibility or cost of the vaccines. The issue can be addressed by making vaccinations more affordable or providing free vaccination services, especially for marginalised populations. In conclusion, the study findings highlight both the positive aspects as well as challenges regarding COVID-19 awareness and vaccination in Pakistan. Efforts should be made to improve education and awareness and remove any economic barriers to receiving vaccination to enhance public health outcomes.
Physical Activities, Social Interactions, and Coping Mechanisms
A point of concern for the population was the unavailability of space for recreational and physical activities despite of willingness to be physically fit. This finding emphasizes the need for creating opportunities for physical activities and safe and accessible recreational spaces that would help individuals overcome the sedentary lifestyle and long and stressful working hours that can contribute to many endocrinal and cardiovascular issues in the long term. Individuals also talked about their engagement in digital technology and social media at a young age to spend their leisure time. Screen time may have negative impacts such as on mental well-being and physical inactivity. 22 Measures can be taken to involve in more productive activities such as outdoor sports. The main coping mechanism of adults was talking to their family and friends which is an essential aspect of socialization and maintaining and healthy mental status.
Addictions
Use of Paan, chalia (betel nuts) and smoking cigarettes were common amongst various age groups. According to existing literature, lack of education, poverty and lack of employment opportunities can increase vulnerability to substance abuse among adolescents due to the increased stress to support their families which may push them towards substance abuse as a coping mechanism. Studies show that interventions addressing these social determinants can be effective in reducing addiction rates. 23 The prevalence of severe addictions can be fueled by lack of access to addiction treatment services and corruption as suggested by AM5 in the results section. Research indicates that addressing community-level addiction requires a multifaceted approach involving law enforcement, health care and social services working towards a common goal. 24
Female Reproductive Health
Regarding female sexual and reproductive health, the findings were suggestive of the fact that the males had a supportive and empathetic stance towards pregnant women and taking care of maternal and child health. This is crucial for the overall physical and mental well-being of the mother and the child, and such support can help reduce maternal and child morbidities and mortalities in these low-income areas in Pakistan which has been a major concern for a long time. 25 The females on the other hand had very relevant emerging concerns including pregnancy-related challenges such as lack of proper access to health care facilities, infrastructure and transport issues and high costs for maternal care. These challenges related to maternal health care access and costs are consistent with global literature highlighting disparities in maternal and child health services, particularly in low-resource settings. 26 Our findings suggest that it is crucial to invest in health care infrastructure and the expansion of maternal health services in underserved areas to improve health care outcomes. An additional issue identified was teenage pregnancies and lack of knowledge and awareness about menstrual hygiene which can act as significant health risk factor. The issue of early pregnancies aligns with research on adolescent reproductive health, which underscores the importance of comprehensive sex education and access to contraceptives. 27 Due to religious and cultural reasons, individuals often hesitate in seeking knowledge about comprehensive sex education and contraceptive methods. Considering the discussion above, it is strongly suggested that the health care services accessibility to pregnant women needs to be addressed by the relevant authorities with increased education and awareness campaigns about menstrual hygiene and contraceptive use.
Part II: Integration and Implementation of Focused Group Discussions in Planning Medical Camps and Student-Led Clinics
The results of our study helped us identify numerous challenges faced by Pakistan’s health care system, particularly in rural areas, from the perspective of the community itself. The findings also guided the identification of the most commonly encountered health issues (Figure 1) and medications prescribed (Figure 2), which were then used to better prepare our volunteers for future student-led clinics (see Supplemental File for details). These findings were integrated directly into the planning of subsequent clinics by aligning available treatments and health education material with community-reported needs, a model supported in similar student-led initiatives.
28
Frequency of common illnesses reported in rural community health camps. Most Commonly Prescribed Medicines in the medical camps.

Some of the main concerns of the community included limited accessibility to health care services due to inadequate infrastructure, overburdened and insufficient health care personnel, restricted clinic hours, the financial burden of treatment and transportation, and a lack of gender-sensitive care. These issues mirror broader challenges reported across South Asian rural settings.29-31 Our student-led clinics (SLCs) were structured to address these gaps by providing free, community-based health care services with extended accessibility. Prior literature on SLCs in underserved populations highlights their effectiveness in improving health access while also enhancing medical students’ competencies in social accountability and primary care delivery.32,33
To address the high burden of communicable diseases, the SLCs incorporated public health education into their model. 34 This approach is grounded in evidence showing that patient education and community-based hygiene awareness programs can significantly reduce infection rates and promote health-seeking behaviors in low-resource settings. 35
The findings of our focus groups offer a comprehensive understanding of the barriers that must be addressed for any long-term improvement in health care delivery in Pakistan and similar low-resource countries. Rural health care is a complex system requiring ongoing, context-sensitive research and community-centered interventions. Future studies should explore the effectiveness of health awareness programs in improving outcomes related to reproductive health, nutrition, and infectious disease prevention. 36 Additionally, longitudinal studies should be conducted to assess the long-term impact of student-led clinics on the overall health indicators of the community, including the reduction of preventable diseases and changes in healthcare-seeking behavior.
Telemedicine also emerged as a potentially transformative solution to rural inaccessibility. Prior studies in Pakistan and other LMICs have demonstrated the feasibility and cost-effectiveness of telehealth platforms for bridging rural-urban health care gaps.37,38 Evaluating the use of mobile-based teleconsultation in underserved areas can provide further insight into sustainable care delivery.
Additionally, comparative studies should be conducted to evaluate the relative effectiveness of student-led models vs traditional government-led primary health care interventions. Community-driven clinics in regions such as Sub-Saharan Africa and rural Brazil have shown success in improving both access and trust in health care systems.39,40 These international examples offer valuable strategies that can be adapted to the Pakistani context. Research should examine the existing health care facilities in rural areas and their role in improving health outcomes, assessing gaps in service delivery and potential areas for collaboration between student-led initiatives and governmental policies.
By situating this study within the global context, it becomes evident that student-led and community-based health models hold promise in reducing disparities and increasing health equity. Future research should continue drawing from these global experiences to refine SLC implementation and develop scalable, culturally appropriate models for rural health delivery in Pakistan.
Strengths
This study included a diverse range of participants, including adolescents, adult males, and adult females. The diversity in the sample population from the community allows for a comprehensive understanding of healthcare-related perspectives across different age and gender demographics in rural Pakistan.41-43 The focus of this study was mainly on a rural health setting, identifying the crucial challenges that are unique to them. This information can be integrated by policymakers in addressing disparities in health care services. The study also utilized multiple data sources such as focused group discussions and medical camp data to validate and cross-reference findings. This approach plays a role in enhancing the credibility of study conclusions. Another strength of this study is its practical applicability, as it includes recommendations and guidance for improving health access. Additionally, the research findings can contribute to the broader body of global public health literature, offering comparative insights for health care improvement strategies in other low-resource settings. By linking this research to global studies, it enhances its applicability and provides a framework for scaling similar models in other developing regions facing health care challenges.
Limitations
However, the sample size in each participant group is relatively small, which limits the generalizability of the findings to a broader population. A larger sample size would have provided more robust insights. In addition to that, the findings may not be representative of all rural regions in the country since the focus group discussion is based on a single community from a single province in Pakistan. Socioeconomic factors, infrastructure, and other challenges may differ slightly from 1 region to another. The qualitative nature of the study means that the findings are exploratory and may not provide quantitative data on the prevalence of specific health care issues. Although translators and cultural sensitivity were factors that were considered during the interpretation of findings, cultural and linguistic differences may impact participants’ responses, which is another limitation of the study. Self-reporting bias could not be excluded from this study as the participants involved in FGDs may have underreported or overreported certain behaviors or challenges due to social desirability bias or fear of judgment. Future research should address these limitations by incorporating larger sample sizes, conducting multi-site studies across different provinces, and integrating mixed-method approaches to gather both qualitative and quantitative data for more comprehensive insights.
Conclusion
In conclusion, the key themes and findings discussed in this study shed light on the multifaceted challenges and opportunities within the health care landscape of rural Pakistan. It was found that limited accessibility to quality health care services, alongside gaps in education and awareness, significantly impacted healthcare-seeking behavior within the community. While these findings provide valuable guidance for policymakers, health care practitioners, and community leaders striving to improve health and well-being in underserved areas, it is important to acknowledge the methodological limitations of this study. The relatively small sample size and focus on a single rural community limit the broader applicability of the findings. Additionally, the qualitative nature of the study, while valuable for exploring key themes, does not provide quantifiable prevalence data, restricting statistical conclusions. This study contributes to the global body of knowledge by demonstrating how community-driven health care interventions, such as student-led clinics (SLCs), can play a role in addressing disparities in rural health care access. Comparisons with successful student-led clinic models in other LMICs, such as those implemented in rural communities, can provide valuable insights for refining and expanding SLC initiatives in Pakistan.
To address these limitations, future research should expand the sample size and include multiple rural communities across different provinces to improve generalizability. Mixed-methods research, incorporating quantitative studies, should complement qualitative findings to allow for statistical analysis of health care barriers and outcomes. Longitudinal studies should also be undertaken to assess the long-term impact of student-led clinics on healthcare-seeking behavior, disease prevalence, and overall health indicators. Furthermore, comparative studies between SLCs, government health care initiatives, and other rural health programs should be explored to evaluate the effectiveness of different intervention models. Additionally, global comparisons with similar rural health care programs in developing countries could help identify best practices for improving health care access and quality. While the implementation of student-led clinics holds promise as a cost-effective and scalable solution to address health care disparities in rural Pakistan, further validation through rigorous research is necessary before widespread adoption as a sustainable health care intervention model.
Supplemental Material
Supplemental Material - Integrating Community Perspectives to Improve Healthcare Interventions: A Qualitative Analysis of Focus Group Discussions for Students-Led Clinics in Karachi
Supplemental Material for Integrating Community Perspectives to Improve Healthcare Interventions: A Qualitative Analysis of Focus Group Discussions for Students-Led Clinics in Karachi by Syed Muhammad Aqeel Abidi, Faiza Qureshi, and Syeda Kainaat Fatima in Global Advances in Integrative Medicine and Health
Footnotes
Acknowledgements
I am grateful to Humanity Initiative, the Non-Governmental Organization working in Pakistan for conducting Student-Led Clinics and supporting me in this regard. Humanity Initiative is a non-governmental organization (NGO) that relies solely on crowdsourcing and donations for its funding. It does not receive any financial support from governmental or corporate entities.
Author Contributions
SMAA: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. FQ: Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. SKF: Writing – original draft, Writing – review & editing, Supervision.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Syed Muhammad Aqeel Abidi served as the president of Humanity Initiative and is the current managing supervisor, Faiza Qureshi served in the core team of Humanity Initiative, and Syeda Kainaat Fatima is serving in the leadership of Humanity Initiative.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author Disclaimer
The opinions expressed in this paper are those of the authors and do not necessarily reflect the views of any organization or institution with which they may be affiliated. The information presented in this paper is intended for academic and research purposes only and should not be construed as professional advice or recommendations.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.