
Abstract
Background
Patients seeking integrative health and medicine (IHM) modalities often present with multiple physical and psychological concerns. Research supports IHM’s effectiveness for addressing symptoms over longer time periods. However, few studies have evaluated immediate outpatient effects.
Objective
This study describes pre-encounter patient-reported outcome (PRO) clusters and examines the immediate clinical effectiveness of IHM modalities on pain, stress, and anxiety among outpatients with moderate-to-severe symptoms.
Methods
A retrospective review was conducted of encounters among adults presenting to outpatient acupuncture, chiropractic, massage, integrative medicine consultation, or osteopathic manipulation treatment between January 2019 and July 2020. Encounters were included if patients reported pre-encounter pain, stress, or anxiety ≥4 on a numeric rating scale (NRS). Outcome analyses included random effects for patient and provider using a mixed model.
Results
Across 7335 clinical encounters among 2530 unique patients (mean age: 49.14 years; 81.0% female; 75.9% White; 15.8% Black/African American), the most common pre-encounter PRO clusters were pain, stress, and anxiety ≥4 (32.4%); pain ≥4 only (31.3%); and stress and anxiety ≥4 (15.6%). Clinically meaningful single-encounter mean [95% CI] changes were observed across all modalities in pain (−2.50 [-2.83, −2.17]), stress (−3.22 [-3.62, −2.82]), and anxiety (−3.05 [-3.37, −2.73]).
Conclusion
Patients presenting to outpatient IHM with moderate-to-severe symptoms most often presented with pain, stress, and anxiety ≥4 on the NRS. Multiple IHM modalities yielded clinically meaningful (≥2 unit) immediate reductions in these symptoms. Future research measuring immediate and longitudinal effectiveness is needed to optimize the triage and coordination of IHM modalities to meet patients’ needs.
Introduction
Integrative health and medicine (IHM) involves the coordinated combination of conventional medicine (e.g., medication, physical rehabilitation, and surgery) and evidence-based modalities such as acupuncture, massage, and chiropractic care to address the needs of the whole person (body, mind, and spirit).1,2 Within IHM, practitioners personalize strategies to patients’ unique conditions, needs, and circumstances to best help them regain and maintain optimal health. 3
Patients seeking IHM modalities often present with multiple physical and psychological concerns such as chronic pain. According to the 2019 and 2020 National Health Interview Surveys (NHIS), 20.8% of adults in the United States (US) report chronic pain (i.e., pain on most days or every day during the prior three months). 4 In a large cross-sectional study, chronic pain (33.1%), acute pain (9.7%), stress (9.3%), and anxiety (7.7%) were among the top ten most common medical conditions addressed among 4182 patients receiving care at nine IHM clinics within the BraveNet Practice-Based Research Network (PBRN). 5 Patients in this study reported higher levels of perceived stress, pain, and depressive symptoms, and lower levels of health-related quality of life (HRQoL) compared to national norms. 6 Similarly, in a survey of 27,225 patients presenting to their initial IHM encounter, the most common reasons for seeking IHM services included spine/truncal pain (70.5%), extremity pain (8.8%), neurologic conditions (6.8%), other pain (5.4%), and generalized muscle pain (4.0%). 7 Therefore, pain-related complaints appear to be prevalent among patients seeking IHM modalities.
Prior studies have shown that patients seeking care from IHM providers (1) perceive IHM to be safe and effective for addressing their needs;8-11 (2) do so in response to dissatisfaction with conventional medical providers;9,10,12 and (3) desire an approach to care that emphasizes the therapeutic relationship and control over their health. 8 Patients within the nine BraveNet PBRN sites reported a desire to “improve health and wellness now to prevent future problems” as their top reason for seeking IHM care (83.9%). 5 However, to demonstrate the immediate impact of IHM modalities on patients’ health and wellness, patient-reported outcomes (PROs) must be embedded within clinical practice.13,14
Multiple studies and systematic reviews support the effectiveness of outpatient IHM modalities for addressing domains including pain15,16 and HRQoL 17 over longer periods of time (e.g., 1 month to 1 year). However, relatively fewer studies have evaluated immediate effects of IHM modalities on acute measures of pain, stress, and anxiety, with the majority of studies coming from the inpatient clinical setting.13,18-22 For example, hospitalized adults receiving various IHM modalities (e.g., acupuncture, massage therapy, music therapy, and/or holistic nursing) provided during 2730 hospital admissions reported an average pain reduction of 2.05 units, which was associated with a cost savings of $898 per admission. 23 Prior studies of short-term effects of outpatient IHM have also been limited to investigating single modalities (e.g., acupuncture, 24 yoga, 25 or massage) 26 and reporting symptom presentations individually rather than describing overlapping symptomology (i.e., moderate-to-severe pain, stress, and anxiety vs pain alone).
Understanding immediate post-encounter effects of outpatient IHM modalities on pain, stress, and anxiety is critically important for coordinating optimal delivery of care. While immediate mean changes do not necessarily speak to the overall impact of these modalities on important domains such as pain interference, stress, mood, and HRQoL over the long-term (days and weeks), they are important for several practical and clinical reasons. First, inviting patients to reflect upon their symptoms immediately post-encounter may facilitate important conversations with IHM providers about the comparative impact of specific interventions (e.g., electro-acupuncture vs traditional acupuncture or acupressure vs fascial release) and help patients internalize an awareness of the immediate benefits of IHM. 13 Second, reducing patients’ immediate symptoms by a meaningful degree following an encounter may increase patient motivation to continue IHM treatment in pursuit of improved health and well-being. 5 Finally, understanding single-encounter effects may help providers and patients determine which IHM modalities may best address long-term health goals. Accordingly, the purpose of this study was to (1) describe pre-encounter PRO clusters and (2) examine immediate changes in pain, stress, and anxiety among patients with moderate-to-severe symptoms receiving care at four outpatient IHM clinics.
Material and Methods
Participants and Design
This study is a retrospective review of all encounters among adult patients (ages 18 and older) receiving care at one of four outpatient IHM clinics between January 1, 2019 and July 31, 2020 that met the following criteria: (1) the encounter was for acupuncture, chiropractic, massage, integrative medicine consultation (IMC), or osteopathic manipulation treatment (OMT) and (2) the patient reported at least one pre-encounter PRO ≥4 on a numeric rating scale (NRS) (i.e., moderate-to-severe pain, anxiety, and/or stress) 27 with an accompanying post-encounter NRS rating. IHM encounters not meeting these criteria were excluded from the sample.
Setting
University Hospitals (UH) is a non-profit health system in Northeast Ohio serving the needs of more than 1.2 million unique patients annually. UH Connor Whole Health (UHCWH), a team of practitioners embedded within the UH health system, provides approximately 29,000 outpatient IHM treatments among 6000 patients per year. Referrals are not required to receive services, though some patients present to UHCWH following a referral from another UH provider. At the time of this study (January 2019 to July 2020), acupuncture, chiropractic, IMC, and OMT modalities were eligible for third party reimbursement depending on the nature of the patient’s condition and health insurance. Massage therapy services were self-pay. During the study period, UHCWH employed six acupuncturists, 10 massage therapists, four chiropractors, four integrative medicine physicians or physician assistants, and one physician providing OMT within its four outpatient clinics.
Ethics and Permissions
This study was approved by the UH Cleveland Medical Center Institutional Review Board (STUDY20200308) as a retrospective chart review with a waiver of informed consent. This study was conducted in accordance with the Declaration of Helsinki.
Data Collected
Patients presenting to UHCWH between January 2019 and July 2020 were asked to complete an NRS measuring pain, anxiety, and stress immediately before and after their encounters. The NRS is a validated measure for acute pain intensity. 27 It has been widely used within studies of IHM modalities 28 and found to be more reliable than the visual analog scale in clinical trials, especially among patients of low socioeconomic status. 28 Investigators in previous IHM studies have also used the 0-10 NRS to measure anxiety18,20,21,29 and stress.19,30
Following appointment check-in, patient service representatives at the front desk presented patients with a pre-encounter questionnaire. This questionnaire consisted of the statement, “On a scale of 0 to 10 (0 being no pain/stress/anxiety at all and 10 being the worst pain/stress/anxiety imaginable) how would you rate your pain/stress/anxiety RIGHT NOW? Please circle only one number in each row,” and three rows of the integers 0 through 10 with headings and anchors for PAIN (No Pain, Worst Pain), ANXIETY (No Anxiety, Worst Anxiety) and STRESS (No Stress, Worst Stress). Providers were encouraged to review pre-encounter NRS scores prior to initiating treatment. Identical post-encounter questionnaires were completed by patients immediately after their IHM encounters and subsequently collected by clinical staff at the conclusion of the encounter. Providers then entered the pre- and post-encounter NRS scores into the electronic health record (EHR). This mode of data collection had previously been investigated by the authors in the context of longitudinal changes in PROs and was implemented here to assess acute changes. 13
We extracted the following data from all records meeting eligibility criteria: (1) demographic information including age, sex, race, and ethnicity; (2) clinical characteristics including International Classification of Diseases (ICD)-10 codes for all diagnoses and chief complaints listed in providers’ notes; and (3) IHM documentation data including modality (i.e., acupuncture, chiropractic, massage, IMC, or OMT) and PROs (i.e., NRS scores of pain, anxiety, and stress) collected pre- and post-encounter. ICD-10 codes were only available for patients who had at least one encounter with an acupuncturist, chiropractor, physician, or advanced practice provider. ICD-10 data were not available for patients presenting only to massage therapy as massage therapists were unable to document formal diagnoses within their scope of practice. All data, including full note documentation, were extracted via a single structured query language script from the UH Electronic Data Warehouse. Regular expressions functions including str_extract_all from the stringr package 31 and regmatches, gregepr, sub, and gsub from base R version 4.3.0 were used to extract clinical information from the free-text note.
Data Analysis
To summarize patients’ primary diagnoses, ICD-10 codes were categorized into Major Expanded Diagnosis Clusters (MEDC). Descriptive statistics were calculated for patient demographics, clinical characteristics, and pre-encounter PROs. To examine immediate changes in PROs overall and by modality, we adjusted for multiple sessions on the same patient using a mixed model, including a random effect for patient and another random effect for IHM provider. This approach allowed for summarized mean NRS scores, 95% confidence intervals (CI), and rates of clinically significant changes to control for the effect of multiple encounters from a proportion of high-utilizing patients32,33 as well as any provider-specific effects. Conducting formal tests comparing NRS changes between IHM modalities was beyond the scope of this study and inappropriate given the high variability in patient presentation and intervention delivery.
Prior studies of IHM modalities have defined NRS reductions ≥2 units as clinically significant.19,24,34 Thus, we reported adjusted counts and percentages of NRS reductions ≥2 units in defining clinical significance in the current study. We extracted data from clinical narratives, analyzed descriptive statistics, and generated plots using R Version 4.3.0 and RStudio Version 2023.06.0 + 421. 35 The mixed model was generated using SAS software, Version 9.4 of the SAS System for Windows (Cary, NC).
Results
Sample
Between January 2019 and July 2020, there were 7335 encounters among 2530 patients reporting at least one pre-encounter PRO ≥4 with an accompanying post-encounter PRO. These 7530 included encounters for acupuncture (37.5%), massage (36.4%), chiropractic (16.2%), IMC (9.1%), and OMT (.7%). At the provider level within this sample of 7335 encounters, a median (IQR) of 287 (103.5 – 513.5) treatments were provided per provider. A median of 129 (54.5 – 189) patients were seen per provider.
Demographics, Chief Complaints, and Utilization
Demographics, Chief Complaints, and Utilization.
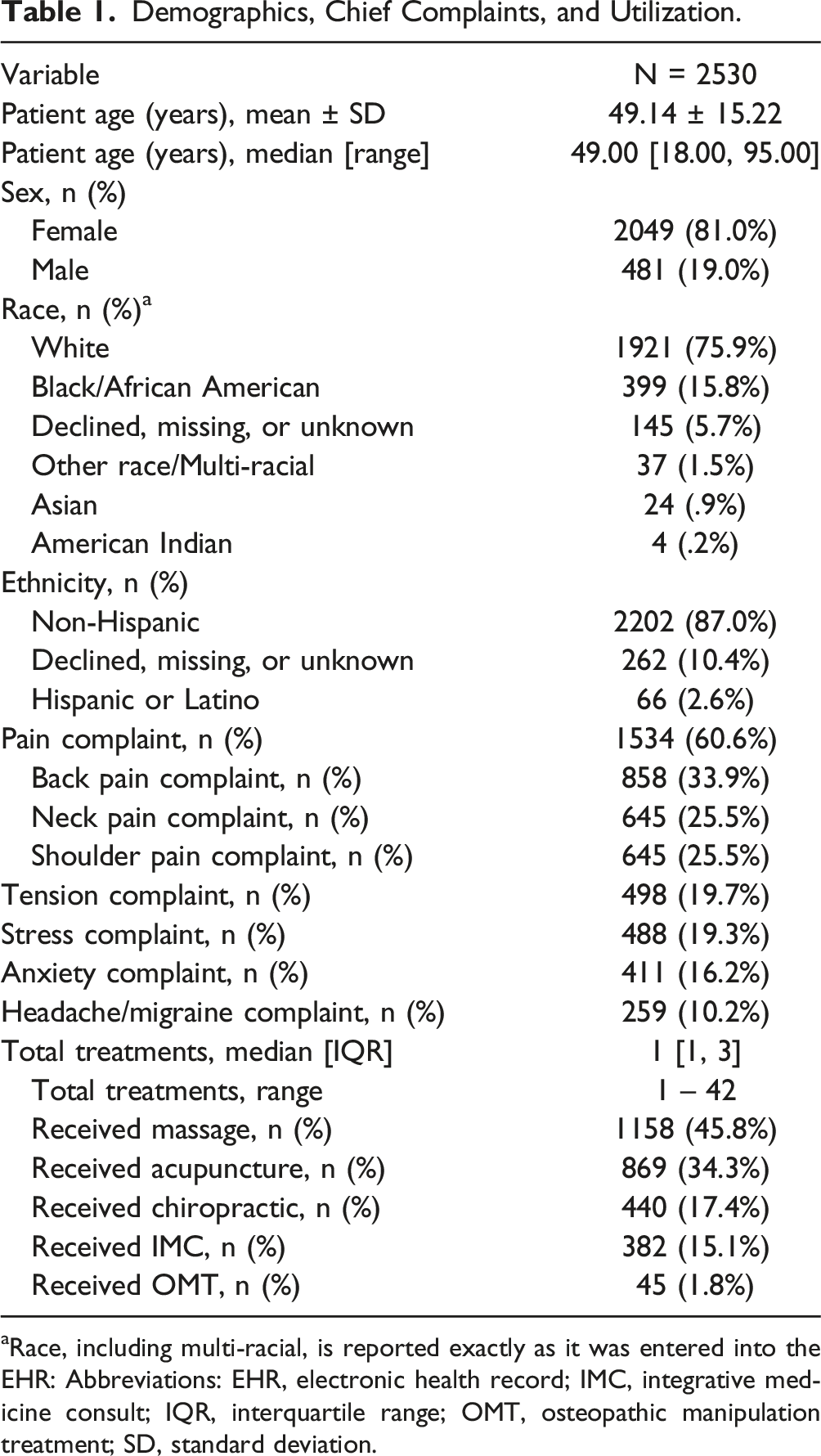
aRace, including multi-racial, is reported exactly as it was entered into the EHR: Abbreviations: EHR, electronic health record; IMC, integrative medicine consult; IQR, interquartile range; OMT, osteopathic manipulation treatment; SD, standard deviation.
Clinical Characteristics
Supplemental Table 1 summarizes the MEDCs among 1577 (62.3%) patients who attended at least one IHM encounter that was not massage. Common MEDCs included musculoskeletal (79.1%), general signs and symptoms (52.8%), neurologic (48.0%), psychosocial/mental health (27.7%), and administrative (e.g., lab abnormalities, preventive care) (25.5%).
Pre-encounter Patient-Reported Outcomes
Supplemental Table 2 summarizes mean and 95% CI for PRO scores adjusted for multiple encounters per patient overall and by modality. Across all 7335 encounters in which patients reported at least one pre-encounter PRO ≥4 and a complete post-encounter PRO, 5434 (74.1%) were among patients who reported pre-encounter pain ≥4 (mean [95% CI] = 5.65 [5.54, 5.77]); 4694 (64.0%) were among patients who reported pre-encounter stress ≥4 (5.89 [5.80, 5.97]); and 3805 (51.9%) were among patients who reported pre-encounter anxiety ≥4 (5.71 [5.61, 5.82]). Figure 1 presents a Venn diagram of the intersections between unadjusted rates of pre-encounter pain, stress, and anxiety ≥4. Among 7335 encounters, the most common pre-encounter PRO clusters were pain, stress, and anxiety ≥4 (32.4%); pain ≥4 only (31.3%); and stress and anxiety ≥4 (15.6%). Patient-Reported Outcome Clusters Venn diagram representing the count and percentage of encounters falling into moderate-to-severe PRO thresholds for pre-encounter pain, stress, and anxiety.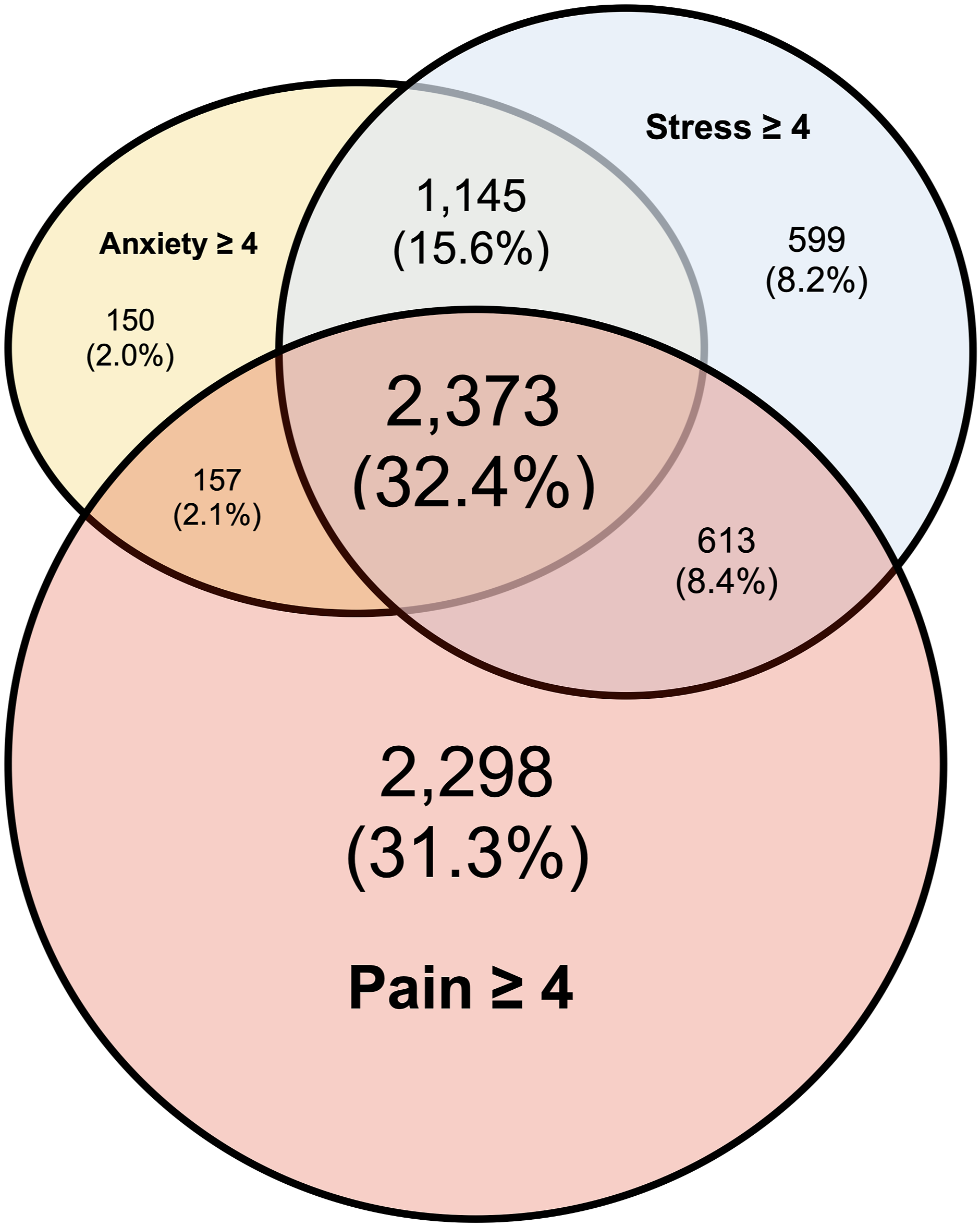
Immediate Effects of IHM
Supplemental Table 2 and Figures 2–4 summarize the immediate effects of IHM modalities after adjusting for multiple encounters per patient. When combining all encounters with moderate-to-severe pre-encounter PRO scores, patients reported clinically meaningful (i.e., ≥2 unit) mean [95% CI] reductions in pain (−2.50 [-2.83, −2.17]), stress (−3.22 [-3.62, −2.82]), and anxiety (−3.05 [-3.37, −2.73]). The largest mean immediate changes in PROs were observed among massage encounters, with patients reporting reductions in pain (−3.07 [-3.24, −2.89]), stress (−4.02 [-4.21, −3.83]), and anxiety (−3.64 [-3.85, −3.42]). In contrast, the smallest mean immediate changes in PROs were observed among IMC encounters, with patients reporting smaller reductions in pain (−.52 [(−.90, −.13]), stress (−1.35 [-1.78, −.92]), and anxiety (−1.35 [(−1.82, −.88]). Immediate Changes in Pain Intensity Overall and By Modality Red dots represent means, while error bars represent 95% confidence intervals after adjusting for the random effects of patient and provider. The downward arrow represents the magnitude of the immediate change in PRO scores from pre-to post-encounter. The orange line at 4 represents the threshold for at least moderate pain rated 4/10 on the numeric rating scale. Abbreviations: Δ, change; IMC, integrative medicine consultation; NRS, numeric rating scale; OMT, osteopathic manipulation treatment. Immediate Changes in Stress Overall and By Modality Red dots represent means, while error bars represent 95% confidence intervals after adjusting for the random effects of patient and provider. The downward arrow represents the magnitude of the immediate change in PRO scores from pre-to post-encounter. The orange line at 4 represents the threshold for at least moderate stress rated 4/10 on the numeric rating scale. Abbreviations: Δ, change; IMC, integrative medicine consultation; NRS, numeric rating scale; OMT, osteopathic manipulation treatment. Immediate Changes in Anxiety Overall and By Modality Red dots represent means, while error bars represent 95% confidence intervals after adjusting for the random effects of patient and provider. The downward arrow represents the magnitude of the immediate change in PRO scores from pre-to post-encounter. The orange line at 4 represents the threshold for at least moderate anxiety rated 4/10 on the numeric rating scale. Abbreviations: Δ, change; IMC, integrative medicine consultation; NRS, numeric rating scale; OMT, osteopathic manipulation treatment.


In examining rates of PRO reductions (estimate [95% CI]) across all encounters, 69.5% [68.1%, 71.0%] reported pain reduction ≥2 units, 82.6% [81.4%, 83.9%] reported stress reduction ≥2 units, and 80.7% [79.2%, 82.2%] reported anxiety reduction ≥2 units. Like the mean changes, the highest rates of PRO change at each threshold were observed among massage encounters while the lowest rates were observed among IMC encounters.
Discussion
The purpose of this study was to (1) describe pre-encounter PRO clusters and (2) examine the immediate clinical effectiveness of IHM modalities on acute measures of pain, stress, and anxiety among patients with moderate-to-severe symptoms receiving IHM. Among 7335 encounters for acupuncture, massage, chiropractic, IMC, or OMT in which patients reported at least one pre-encounter PRO ≥4 on the NRS, nearly one-third (32.4%) presented with co-occurring pain, stress, and anxiety ≥4. This finding is consistent with the prior BraveNet PBRN study where pain, stress, and anxiety were among the top ten most common medical conditions addressed. 5 From a neurobiological perspective, the co-occurrence of stress and anxiety with chronic pain may be a result of dysfunction within the functional and structural connectivity of the neural circuits that govern sensory, emotional, and cognitive functions. 36 Scioli-Salter and colleagues 37 proposed that high rates of co-occurring chronic pain and conditions such as post-traumatic stress disorder (PTSD) may be explained by shared pathophysiological mechanisms such as (1) stress-stimulated increases in peripheral and central nervous system levels of neuropeptide Y and GABAergic neuroactive steroids and (2) dysregulation of the opioid, endocannabinoid, and immune systems in chronic pain and PTSD.
Most clinical encounters (74.1%) within this sample were among patients reporting moderate-to-severe pre-encounter pain ≥4. This finding is consistent with a prior cross-sectional study in which pain conditions were the most common reasons for seeking IHM services. 7 Furthermore, prior analyses of National Health Interview Survey data have demonstrated increased odds (adjusted odds ratio [95% CI]) of using IHM among (1) adults with limiting low back pain as compared to non-limiting low back pain (1.1 [1.0 – 1.2]); 38 (2) adults with severe migraine and recurring headache as compared to recurring headache alone (3.36 [2.08, 5.43]); 39 and (3) adults with arthritis and joint pain as compared to no joint pain (2.08 [1.46, 2.96]). 40 Given the prevalence of acute pain among individuals engaging in IHM and its association with increased odds of engagement in IHM, it is critically important for IHM centers to collect PROs related to pain at baseline and over time to assess effectiveness.
PROs are of vital importance in healthcare delivery, and their use is now becoming mandated by The Centers for Medicare & Medicaid Services within oncology 41 and joint arthroplasty. 42 PROs demonstrate whether symptoms and/or HRQoL are improving (or not) in response to treatment;13,14 facilitate shared care and decision making with the healthcare system; 43 and can improve rates of patient satisfaction. 43 Collecting PROs is also essential within practice-based research for evaluating the effectiveness of IHM modalities across healthcare systems.13,28,30,44
In the context of this study, collecting acute NRS measures of pain, stress, and anxiety may have helped providers tailor the delivery of IHM modalities to a given patient’s immediate needs. 13 As NRS measures were integrated within routine care, providers reviewed the pre-encounter measures and used them to inform their overall assessment of patients’ symptoms and guide their clinical decisions. For example, chiropractors within the clinic used the pain NRS in conjunction with the Oswestry Disability Index 45 to help determine patients’ pain disability at the initial visit and track changes in pain outcomes over time.
Patients within this study reported clinically meaningful reductions in pain, stress, and anxiety that are comparable to or exceed reductions observed in prior studies of inpatient IHM. However, direct comparisons to prior studies are challenging given differences in IHM modalities, timing of PRO collection, number of PROs collected, and pre-intervention PRO thresholds applied (e.g., none, ≥1, or ≥4). Nevertheless, the overall observed mean reductions in pain (2.50 units), stress (3.22 units), and anxiety (3.05 units) were similar to findings from a recent study of inpatient music therapy within community hospitals in which patients reporting pre-session PROs ≥4 on the NRS also reported clinically meaningful single-session reductions in pain (2.04 units), stress (3.48 units), and anxiety (2.80 units). 19 Mean pain reduction observed within this sample was also similar to prior observational studies of inpatient IHM among patients reporting any pain ≥1 including studies of various IHM modalities (i.e., acupuncture, massage, holistic nursing, and music therapy) among 2730 hospitalized adults (2.05 units), 23 post-surgical acupuncture among 1977 adults undergoing hip or knee replacement surgery (1.91 units), 22 and combination aromatherapy among 2444 hospitalized adults (3.43 units). 21
When comparing findings from this study to other outpatient studies of IHM among adults with acute and/or chronic pain, patients’ reported mean reductions in pain with chiropractic (2.44 units) were slightly lower than reductions at 1 month in response to chiropractic care observed among 79 patients with acute low back pain (2.98 units) 46 and higher than reductions at 1 month among 44 patients with chronic low back pain (1.31 units). 47 Patients’ reported immediate reductions in pain with acupuncture (2.38 units) were similar to reductions at 24 hours among 117 active duty military, dependents, and retirees with acute and chronic pain receiving acupuncture (2.5 units). 48
Finally, in comparing our results to those from observational studies of IHM among adults with cancer receiving acupuncture, we observed greater mean reductions in pain (2.38 units) and anxiety (2.87 units) than those reported by Miller and colleagues 24 (N = 68, mean pain reduction 1.90 units, mean anxiety reduction .90 units) and Thompson and colleagues 49 (N = 87 for pain, mean pain reduction: 1.39 units, N = 85 for anxiety, mean anxiety reduction: 1.26 units). We also observed massage encounters resulting in greater mean reductions in pain (3.07 units) and anxiety (3.64 units) than those reported by Lopez and colleagues 26 (N = 168, mean pain reduction: 1.55 units, mean anxiety reduction: 1.34 units). However, it is important to note that these studies within oncology did not apply a pre-encounter PRO threshold of ≥4 and thus included patients who did not have moderate-to-severe symptoms as was the case in the current study.
Although the current study did not formally compare single-encounter PRO changes between IHM modalities using statistical tests, numerical differences were apparent – particularly the higher reductions observed within massage encounters relative to the lower reductions observed within IMC encounters. Massage therapy may be unique in yielding large immediate reductions in pain, stress, and anxiety given the characteristics of the intervention (e.g., continuous hands-on massage techniques provided over 30 to 60 minutes). In contrast, IMC encounters include physical exams, verbal assessments in which patients discuss their health concerns, clinical referrals to IMH modalities, and discussions of ways to implement therapeutic changes in between appointments over the longer term (rather than during the IMC encounter). Thus, even if stress and anxiety ratings were to decrease during this therapeutic encounter, pain would not be expected to decrease by the same degree observed with hands-on interventional approaches such as massage. Furthermore, research has shown that the effects of some IHM modalities (e.g., acupuncture and chiropractic) on acute symptoms may become more apparent at 24–72 hours. 50 However, to better understand response patterns in the real-world of ambulatory clinics, future longitudinal research with more frequent data collection is needed to compare the effects of various IHM modalities on acute symptoms at various time points (e.g., post-encounter, 24 hours, 1 week, and 1 month).
This study had some notable limitations. First, we did not assess PROs longitudinally across or between IHM encounters, and thus our analysis focused on immediate changes. Second, this study used observational data within a single IHM center without a control or comparison group. To better understand the real-world effectiveness of IHM as compared to conventional care, future observational studies should consider comparing patients who received IHM to propensity-score matched controls who did not receive IHM over the course of treatment. Third, there is a potential for response bias among patients reporting post-encounter PROs as patients may have wanted to please the providers by reporting improved scores. This risk was somewhat mitigated as patients completed their post-encounter evaluations on paper and had the option of dropping off their evaluations to the patient service representatives at the clinic’s front desk. Furthermore, the observed symptom reductions within IMC encounters being numerically lower than those observed in response to interventional modalities (e.g., massage and acupuncture) provide some assurance that patients were reporting their symptoms accurately and honestly. Future studies could consider collecting PROs through a mobile device or having research assistants blinded to patients’ participation in IHM collect PROs to reduce this risk of bias. 51
Fourth, though NRS measures were presented to patients as part of routine clinical care rather than as part of a formal research study, there is the potential for the Hawthorne effect within this study whereby patients’ perception of being observed and measured may have modified their NRS responses. Fifth, this study primary consisted of middle-aged individuals (mean 49.14 years) identifying as female (81.0%) and white (75.9%). This demographic profile does not reflect that of the county where the study took place (30.5% Black/African American), 52 and may not reflect the population of individuals with moderate-to-severe symptoms engaging in IHM modalities nationally.
Finally, this study used single item 0-10 NRS scores rather than more comprehensive instruments for pain, stress, and anxiety. However, more robust measures such as the Patient Reported Outcome Measurement Information System (PROMIS) are often more suited toward capturing outcomes over a period of several days or weeks than capturing outcomes immediately pre- and post-encounter like the NRS. Strengths of this study include the large sample size, diversity of clinical populations, use of real-world EHR data, and the collection of PROs immediately before and after IHM encounters.
Conclusions
Patients presenting to an outpatient IHM center with moderate-to-severe symptoms most often presented with pain, stress, and anxiety ≥4 on the NRS (32.4%) followed by pain ≥4 alone (31.2%). The results from this study support the clinically meaningful impact that IHM modalities can have on moderate-to-severe symptoms within a single encounter and add to a growing body of evidence supporting the real-world clinical effectiveness of IHM for pain15,16 and HRQoL. 17 Multiple IHM modalities yielded clinically meaningful reductions (i.e., ≥2 units) in these symptoms within a single encounter. Future research is needed to (1) assess changes in these acute measures and more global HRQoL measures over time, (2) compare outcomes between IHM and a matched comparison group, and (3) utilize PRO data to best triage and dose IHM modalities to optimize care. Future researchers should be encouraged to measure immediate and longitudinal effectiveness as a means of optimizing the triage and coordination of IHM modalities to meet patients’ immediate and long-term needs.
Supplemental Material
Supplemental Material - Immediate Effects of Integrative Health and Medicine Modalities Among Outpatients With Moderate-To-Severe Symptoms
Supplemental Material for Immediate Effects of Integrative Health and Medicine Modalities Among Outpatients With Moderate-To-Severe Symptoms by Samuel N. Rodgers-Melnick, MPH, MT-BCORCID, Roshini Srinivasan, RYT, Rachael L. Rivard, MPH, Francoise Adan, MD, ABIHM and Jeffery A. Dusek, PhD in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgements
We thank the patients who received the integrative health and medicine modalities analyzed in this study. We would also like to thank the following collaborators on this study: The Information Technology Senior Developers Carl Langdon and Ryan Jaskolka; study coordinators Tracy Segall, MSHS and Jessica Surdam, MPH; the patient service representatives; and all participating integrative health and medicine practitioners. We especially appreciate the support of Chris and Sarah Connor.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the generosity of Chris and Sarah Connor, Cleveland, OH. Chris and Sarah Connor had no role in the study design; the collection, analysis, and interpretation of data; the writing of the report; or the decision to submit the article for publication.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy restrictions as the databases contain information that could compromise the privacy of research participants. However, the de-identified datasets are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.