
Abstract
Background
In North America, there is a notable underutilization of complementary and integrative health approaches (CIH) among non-White and marginalized communities.
Objectives
This study sought to understand how CIH educational instutitions are proactively working to redress this disparity in access and utilization among these communities.
Methods
We conducted interviews with 26 key informants, including presidents, clinicians, and research deans across 13 CIH educational institutions across the US and Canada. Thematic analysis included deductive codes based on the interview guide during interview scripts review.
Results
Six themes were identified: (1) CIH institutions often had a long and varied history of community engaged care through partnerships to increase access and utilization; (2) CIH institutions’ long-standing community outreach had been intentionally designed; (3) CIH institutions provided an array of services to a wide range of demographics and communities; (4) addressing healthcare access and utilization through community partnerships had a strong positive impact; (5) funding, staffing and COVID-19 were significant challenges that impeded efforts to increase CIH access through community engaged work; (6) identified gaps in community partnerships and services to increase access and utilization were recognized.
Conclusion
These findings underscore significant efforts made to enhance healthcare access and utilization among marginalized, underserved, and racial and ethnic communities. However, barriers such as funding constraints, resource allocation, and the need for proper measurement and accountability hinder proactive initiatives aimed at redressing disparities in CIH utilization within these communities.
Keywords
Introduction
In the US, approximately 34% of adults are estimated to access and use complementary and integrative health (CIH) for care. 1 Further, its noteworthy that the primary users of CIH services provided by practitioners (such as doctors of chiropractic, licensed acupuncturists and doctors of Chinese/Asian/traditional medicine, naturopathic doctors, massage therapists and yoga therapists) tend to have higher levels of education, income, and identify as non-Hispanic White. 1 Among non-White and marginalized communities, the utilization of CIH healthcare is estimated to be closer to 20% with variations by race/ethnicity (eg, 19% Blacks compared to 22% Hispanic), and income level (20% for those below the poverty threshold and 25% for those between 100%–200% poverty threshold). 1 Despite the evidence that shows that use of CIH positively impacts physical health, mental health and provides greater benefit for marginalized racial/ethnic groups compared to non-Hispanic Whites,2-5 CIH is underutilized among marginalized, underserved, and racial and ethnic populations. 6 Underutilization of CIH is in large part a result of structural inequities (eg, insurance coverage, availability of services in marginalized communities) that impact all healthcare access and places marginalized, underserved, and racial and ethnic communities at a disadvantage.
Increasing healthcare access and utilization to marginalized, underserved, and racial and ethnic communities has been a concern for several years. Scholars, clinicians, health institutions, and health research and funding agencies have put forth various proposals to address access and utilization, including the expansion of the healthcare workforce and the adoption of inclusive hiring practices.7,8 They have also advocated for the implementation of mobile clinics,9-13 advocated for broader insurance coverage, 14,15 and more recently, endorsed the widespread use of telehealth services,16,17 and collaborative efforts with communities for targeted outreach.18,19 While all these strategies have proven successful in advancing healthcare access and utilization, they share a common foundation: an understanding of the unique needs of marginalized, underserved, and racial and ethnic communities, which is best achieved through community engagement. Indeed, community engagement has been identified as a pivotal method for establishing and nurturing trust within communities, while simultaneously enhancing the accessibility and quality of care for individuals.20-22 Moreover, intentional community engagement stands as a linchpin in the pursuit of health equity.23-26 Allopathic schools, for instance, have demonstrated a high level of commitment to leveraging community engagement to enhance access to care and improve health outcomes.26-30
Advancing health equity in CIH necessitates the establishment of a comprehensive system that guarantees every individual equal and unimpeded access to preventative, promotive and curative health services.31-34 This access, as outlined by Levesque and colleagues, 35 extends far beyond mere availability of services or insurance coverage, and embodies a multifaceted interplay between supply and demand. In terms of demand, it encompasses an individual’s capacity to recognize their healthcare needs, actively seek out services, access facilities and resources, acquire and utilize healthcare, and ultimately receive tailored care. 35 Furthermore, this framework considers supply-related elements, including approachability, acceptability, affordability, appropriateness, availability, and accommodation. 35 Examining the factors contributing to the inequitable and limited utilization of healthcare provided by CIH practitioners among adults through this lens, it becomes evident that supply-related barriers such as limited awareness,36,37 insufficient availability,38,39 restricted accessibility 37 and financial constraints 39 play a significant role.
To enhance access and utilization HealthyPeople 2030 emphasizes the necessity for healthcare systems and services to implement interventions that target the supply-side factors (approachability, acceptability, affordability, appropriateness, availability and accommodation), thereby eliminating barriers for individuals seeking care. 40
Given that marginalized, underserved, and racial and ethnic communities face numerous obstacles in accessing healthcare41-43 and tend to utilize CIH care less frequently than non-Hispanic whites, 1 it is imperative to inquire: What proactive measures is the CIH community taking to improve healthcare access for marginalized communities? Moreover, considering that community engagement lies at the heart of interventions to increase access and utilization, what steps are being taken to actively engage with communities to increase access and use? Key organizations within the CIH community include its educational institutions.
CIH educational institutions, such as colleges and universities that graduate naturopathic doctors and doctors of chiropractic, are central to the development, function and broader presence of the CIH professions. In addition to training new CIH providers, these institutions often offer multiple CIH degree-granting programs, promote CIH research, and function as hubs of support and networking for CIH professionals. Considering the large role that these educational institutions play for CIH professions, information about how CIH educational institutions engage with diverse communities sheds light on broader structural barriers to CIH care for non-White and marginalized communities. For these reasons, it is of interest to examine how the CIH professional education institutions have attempted to mitigate these barriers and overcome this lack of access and utilization of healthcare by marginalized, underserved, and racial and ethnic communities. This paper will document some of the ways in which CIH educational institutions have addressed these barriers while providing their students with the experience of engaging diverse populations and being exposed to the distinct health experiences of these communities.
The core objective of this study was to shed light on examples of CIH academic institutions involvement in engaging with marginalized, underserved, and racial and ethnic communities to enhance their access and utilization of healthcare. These are presented as
Methods
To understand what CIH academic institutions were doing to address healthcare access to marginalized, underserved, and racial and ethnic communities, we conducted semi-structured interviews with the institutional members of the RAND Research Across Complementary and Integrative Health Institutions (REACH) Center (https://www.rand.org/health-care/centers/cih.html). The REACH Center is a collaboration between the RAND Corporation and 13 academic institutions in the US and Canada that educate and graduate CIH practitioners and is funded through a U24 cooperative agreement grant from the National Center for Complementary and Integrative Health. This study was approved by the RAND Human Subjects Protection Committee and the reporting of this study followed the consolidated criteria for reporting qualitative studies. 44 Key informants provided a verbal consent to participating in the study.
Recruitment
Key informants were recruited from the Executive Committee (made up of the CIH institutions’ presidents) and the Research Advisory Board (research deans for the institutions who could identify other key informants) of the REACH Center. Additionally, the 13 research advisory members (1 for each school) were then queried about the potential inclusion of additional members from their academic institutions. Besides these 13 members, all other key informants (eg, clinicians, clinical directors, presidents) in the study were recommended by the research advisory member, and chosen for their experience and expertise in engaging with underserved communities to improve healthcare access and utilization.
Data Collection Procedures
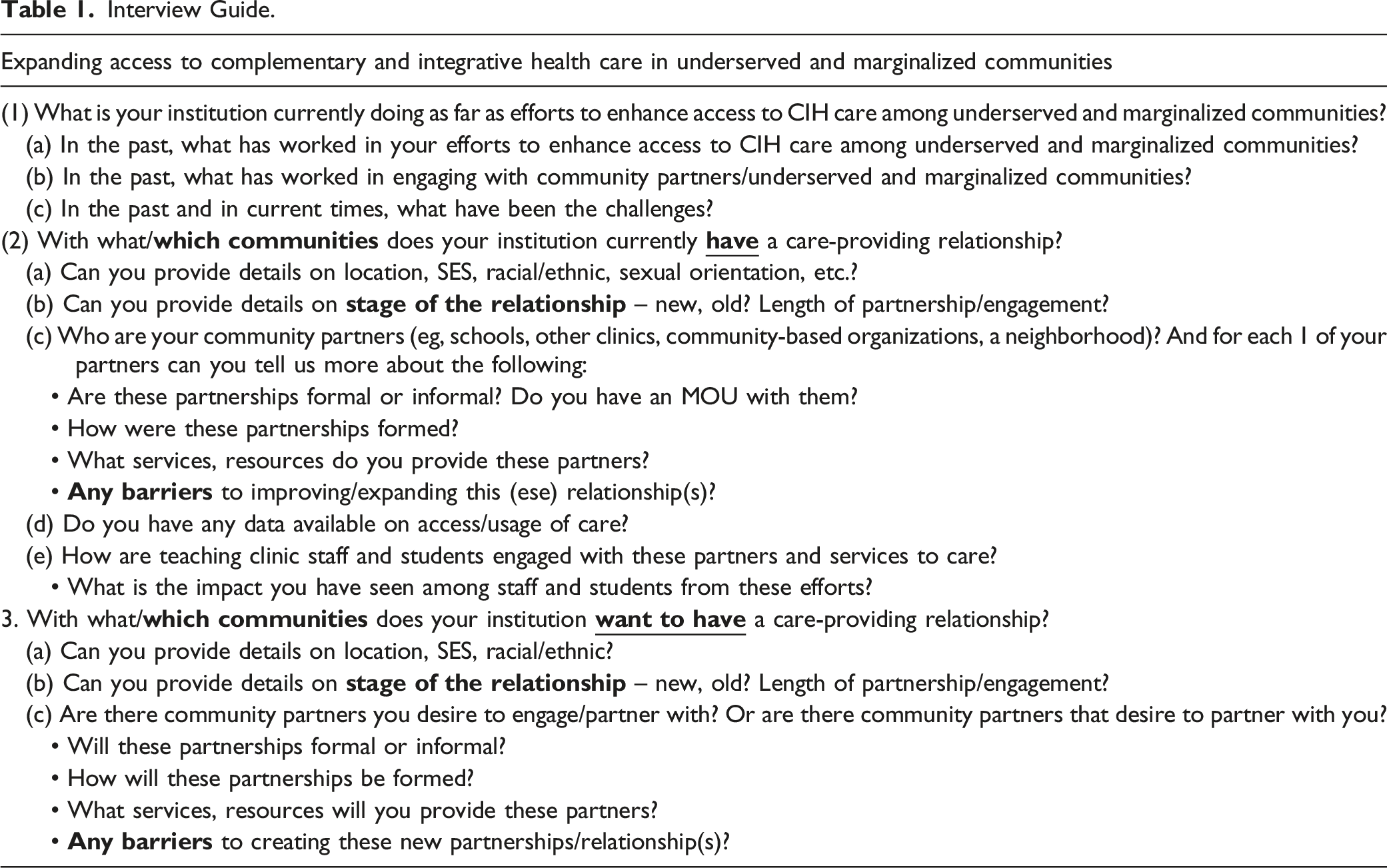
Interview Guide.
Reflexivity and Positionality
Two authors (NM and PMH) conducted the interviews. Some were conducted jointly, and others were led by only 1 of them. The interviewers are trained in qualitative methods in behavioral science and health services research, coupled with substantial prior experience conducting interviews and analyzing qualitative data. NM is a social epidemiologist who specializes in community-based participatory research to understand and address health inequities in underserved communities. PMH is an NCCIH-supported methodologist, resource economist, and licensed naturopathic doctor.
Data Analysis
The qualitative data was analyzed using thematic analysis methods 49 by 2 independent researchers (NM and PMH). The data was first assessed by the units of analysis (CIH institutions) through open coding, where sentences or paragraphs were examined and a descriptive label was attached to them.50,51 NM and PMH collaborated, engaging in discussions to establish consensus on codes and themes which were developed through manual analysis. Thematic analysis included deductive codes based on the interview guide during interview scripts review. The study team convening to collectively discuss and summarize findings within and across themes. 52 Thematic analysis was conducted across the data as it has been shown to be an effective method for evaluating this type of qualitative data.53,54 The results in this manuscript have been deidentified.
Results
Fourteen interviews were conducted with 26 key informants from Center member institutions. Interviews with key informants from the institutions varied: 4 institutions each contributed 1 interviewee; in the case of 6 institutions, each had 2 key informants in an interview; 2 institutions featured 3 key informants in a single interview each, while 1 institution had 4 key informants interviewed together. Among the participating institutions, 6 trained practitioners in acupuncture, 7 in chiropractic care, 6 in naturopathic medicine and 9 offered training programs in other fields such as yoga therapy, ayurveda, herbal medicine, massage therapy, east Asian medicine, Chinese Medicine and nutrition. The total number of types of CIH institutions exceeds 13, as most schools educated practitioners in multiple CIH fields.
Of our key informants, 13 were research directors overseeing clinical and community-based research initiatives, 6 were clinical directors overseeing internal and external clinical work, 4 were clinician working in communities, 2 were a university president and 1 was the vice president for diversity, equity, and inclusion.
All schools reported engagement in care delivery with marginalized, underserved, and racial and ethnic communities. Additionally, 5 schools reported engaging in extra community activities, such as offering resources and participating in community events, aimed at establishing trust and building partnerships to enhance clinical care delivery.
Six themes were identified in the interviews, and are described below.
Theme 1: CIH institutions often had a long and varied history of community engaged care through partnerships to increase access and utilization
The CIH institutions reported an average of 15 (range 1 - 25) years of engagement with local organizations and partners to provide healthcare to marginalized, underserved, and racial and ethnic communities. Informants described the need to build partnerships founded on trust in order to be invited into the communities as guided by the principles of community based participatory research. These partnerships were built through collaborations with organizations that had already gained the trust of the community or by the CIH academic instutition seeking to built trust with a community itself. The CIH institutions delineated 2 principal pathways for establishing partnerships. In 1 approach, the institutions reported taking a proactive stance, identifying community of interest (eg, Indigenous, immigrant) or community partners (eg, Salvation Army, schools) of interest and nurturing relationships with them over time. During the relationship-building phase, the institutions aimed to discern their partners’ specific needs and how they could effectively collaborate to address health and social needs. The second reported route to partnership formation was instigated by community or organizational partners who actively sought out the institutions drawn by their reputation, resources and demonstrated impact in working with communities. These partnerships, they believed, would bolster accessibility and utilization of healthcare services provided by CIH practitioners within these communities. “In finding our partners, we come through it using community based participatory research principles. We have built relationships with community partners and through those partnerships, the communities have told us what they need” – CIH Institution 4 “The other day a woman called and asked if we would like to partner with her community. She has a pop-up unit already in existence and all we would have to do is show up and provide services” – CIH Institution 5 “First, we find the partner and build a partnership using community based participatory principles. Once we have built relationships with the community partners, it is through those partnerships then that the communities have told us what they need” – CIH Institution 4
The reported partnerships included homeless shelters and recovery centers, non-profit/charitable organizations (eg, Salvation Army, YWCA), school districts, residential incarcerated centers, senior centers, women’s and children’s day centers, Veterans Affairs facilities, federally qualified health centers, community centers, state universities, churches, and Indigenous organizations and clinics. “We have been partnered with [Name of Organization] since 1998. Together we go to various churches and other locations and take over a triage location with several practitioners and provide care” – CIH Institution 9 “We are partnered with the YWCA and serve women experiencing homelessness in [Name of City]. The YWCA has been a great partner because they give us the space to see women and provide care, but they are also invested in us just as we are invested with them” – CIH Institution 1 “The Community Health Initiative was first established in 1993 and it continues through to today…Some sites are designed to support under resourced and marginalized communities, while others support the general population. Some locations are ongoing sites while others are offered on a one-time or short-term basis” – CIH Institution 12
Theme 2: CIH Institutions’ Long-Standing Community Outreach had Been Intentionally Designed
Recognizing the profound impact that a strong community connection could have on their mission and their students, these institutions reported prioritizing engagement as a means to bridge the gap between academia and the needs of their surrounding neighbors. These institutions reported such an approach as a way to better prepare and equip their students, practitioners, and clinics to serve their surrounding community. “Being in the community is part of the university’s strategic plan” – CIH Institution 1 “We want to be more active in the community so that we can also connect with the patients and know how to better serve them” – CIH Institution 2 “We set up our student program in such a way that it allows students to get to learn how to engage with low-income rural populations” – CIH Institution 3 “The dean of our [Name of State] campus is really passionate about outreach. That is his mission in life and a mission he has extended to that campus and so they are very active in their community outreach” – CIH Institution 11 “Supporting community-based organizations is a mission-driven and growing component of [Name of Institution], exemplified by the partnership with [Name of Partner]. [Name of Partner’s] mission is to end poverty, and its holistic approach integrates on-the-ground services to create stable homes, workforce development, and neighborhood revitalization” – CIH Institution 12
Theme 3: CIH institutions provided an array of services to a wide range of demographics and communities
Key informants reported that their partnerships enable them to reach a wide demographic range of people in their community, including those who are low-income, unhoused, formerly incarcerated, children, the elderly, immigrants (including Southeast Asians, and Somalis), individuals from diverse racial/ethnic backgrounds (including Indigenous, Hispanic, Black, Vietnamese, Asian), as well as sexual and gender minorities. Their reported efforts are also spread across diverse settings, encompassing urban, rural, and highly rural areas.
The CIH Institutions reported offering an extensive array of services that cater to the diverse healthcare needs of their community partners. Beyond CIH services such as chiropractic, acupuncture, ayurvedic medicine, naturopathic medicine, and Chinese medicine, these services also includeprimary care, trauma-informed care, physician assistant assessments, nutrition, diabetes care, sports medicine, rehabilitation programing, and specialized spinal stenosis programs. The comprehensive range of reported services is made possible by the extensive training and resources available at each institution. “We provide a wide range of care for these communities, from acupuncture and Chinese herbs to primary care and naturopathic specialty care. In addition to these, we also have a long tradition of providing health screenings, education and support at community fairs, events, and school functions. We are also a long-standing member of our area Coalition of Community Health Centers and serve primarily low-income patients at all of our clinical sites” – CIH Institution 4 Top problem that we can help with right now in [Names of communities] is opioid and substance use problems and so that is what we are doing. That is where the need is and we adapt our services to that” – CIH Institution 5 “Over the years we have provided Ayurvedic medicine, physician assistant assessments, acupuncture, and chiropractic care. But as of Aug 2023, we are only offering chiropractic care” – CIH Institution 9
CIH institutions reported another aspect that was crucial to their work with communities was engaging with their community partners based on the partners’ own terms and needs. This meant identifying the distinct social determinants of health (such as housing, food, and educational resources) within the communities of interest or their community partners. Then the CIH institutions would align their offerings (e.g., provision of housing vouchers, food and educational resources) with the specific needs of the communities, to ensure that that they were responsive to the communities of interest/community’s partners needs and remained relevant, effective, and accessible to all. “We just did a social determinants of health survey and we also asked if people want help or want to talk to someone about their social and home needs. This has allowed us to help them find air conditioning, housing vouchers, and other social support resources. We have also just gone live with a platform for social services that allows us to narrow down by zip code. We have 3 members on staff to help with application assistance for Medicaid and resources and hoping to have an MSW to oversee and help interns with these services” – CIH Institution 4 “We partner with Islamic Relief USA and on top of our health services we provide supplies that are needed such as Backpacks, sleeping bags, rain ponchos, socks, knitted hats, hygiene kits, large storage carry bags, school kits, non-perishable food, veggie burgers, bottled water, donuts, and ChapSticks. We also help with public transportation, job searches, ergonomic assessment, and domestic violence counseling” – CIH Institution 10 Weekly, [Name of institution] distributes nutritious, low-cost recipes developed by [Name of Institution’s] students and faculty using ingredients commonly found at food banks. Over 500 recipes have been developed to date. Some recipes are tailored to the micro-culture of the local region and population, and some have been translated into Spanish and Russian – CIH Institution 12
Theme 4: Addressing healthcare access and utilization through community partnerships had a strong positive impact on CIH student providers
Key informants emphasized the transformative influence of prioritizing community engagement to address access, underscoring its benefits not just for the served communities but also for their students. They shared how efforts to enhance access for marginalized, underserved, and racial and ethnic communities enriched their students’ perspectives, inspiring some to pursue roles in federally qualified health centers or to establish their own mobile or stationary clinics in low-income and marginalized areas. Additionally, certain students sought career paths focused on developing interventions that would continue to support the communities they engaged with during their studies. “I know of one student who after graduation, went to work at a federally qualified health center in Dartmouth. His experience as a student pushed him to do this. Another student went to Russia and set up a mobile clinic for athletic training” – CIH Institution 3 “[Our work] has a big impact [on the people we serve and partner with] because it makes people be seen. Our work allows people to know that there are those who care about them and are willing to meet them where they are at” – CIH Institution 1 “I know that students find their work at community sites to be an excellent learning experience. They are busy and working with limited resources. They encounter many conditions and cases they would not otherwise encounter in our other teaching clinics... We have had very good feedback from community members over the years with respect to the care they have received” – CIH Institution 13 After going through our community-based programs as students, some of our alumni started walk-in clinics for those who are Medicare patients, Medicare eligible or undocumented individuals. They charge $60 for new visits and $40 for established visits. They have over 2000 active charts” – CIH institution 9 “One student became so passionate about our work in the Salvation Army that they later went and got their MPH and later their PhD and her dissertation was on education programs for the individuals in the Salvation Army. She wanted to help them get jobs and placements. And she is still continuing that work. That is how it works, when you try to help someone else you end up being the one who is transformed” – CIH Institution 11
Theme 5: Funding, staffing and COVID-19 were significant challenges that accompanied efforts to increase CIH access through community engaged work
The endeavors of these institutions were not without their share of challenges. Key informants identified 3 key challenges: funding, shortage of staffing, and the implications of COVID. Nearly all the institutions emphasized the necessity for additional funding to sustain their efforts within communities. Funding was identified as a fundamental component in their collaboration with community partners, yet it was also identified as a significant shortfall. “Funding for some of the work we do is a big barrier” – CIH Institution 5 “A lot of times with foundation grants, they want to fund new initiatives. So, it’s hard to get funding for things we are already doing when in actuality that is what we need for sustainability” – CIH Institution 9 “Finances are a challenge. Because we do not charge for visits at these community sites, we must cover the cost of faculty supervision. Financial constraints of our patients are also a challenge, as therapeutic products are not covered by drug plans” – CIH Institution 13
Staffing shortages also emerged as a significant challenge. As they deepened their collaborations with communities, they increasingly identified gaps in services that required attention. However, addressing these gaps necessitated additional staff. Faculty members are essential for spearheading certain community initiatives and while students can assist in meeting some staffing needs, both are currently lacking. “We have had community care sites with a huge range, but due to low staffing, we have had to pull back to 6-7 sites” – CIH Institution 1 “Enrollment is fluctuating. Our student numbers are down. Five years ago, our graduating class was five times larger than it is now” – CIH Institution 4
Lastly, the COVID-19 pandemic had a substantial impact on the institutions’ interaction and outreach with their community partners. While some institutions have not fully regained their previous level of community engagement, others experienced the loss of partnerships due to financial constraints, personnel turnover, and the necessary adjustment in the post-COVID era. “Things have been hard to start up again since COVID. We had a 15-year relationship with FQHCs. And it’s been hard to restart that again” –CIH Institution 6 “We used to see approximately 30 unhoused women in the 5 hours we are in the community on Sunday but since COVID, we have been struggling to build back up again to that number” – CIH Institution 1
Theme 6: Identified gaps in community partnerships and services to increase access and utilization were recognized
Despite a history of successful collaboration both within and alongside communities, key informants articulated the pressing need to extend their community initiatives and gain deeper insights into their influence on accessibility. They persist in identifying deficiencies in service provision and care delivery, underscoring the sustained requirement for focused endeavors to narrow these disparities and bolster their effect within the communities they engage with. Furthermore, they recognize gaps in the documentation of their work, which is essential for comprehending their impact in evaluating access. “I would like to see us going back to the Indigenous people and to grow that. We have so much to learn from them and their philosophy for life and healthcare and we would love to collaborate with them. Chiropractic care can also grow in supporting women’s health and I would like to see that area grow as well. From women’s care before period, to having children to menopause and all the pain issues they experience. There is so much that chiropractic care can do and we need to start doing that” – CIH Institution 2 “We are hoping to engage with Historically Black Colleges and Universities. To build partnerships with them long term” – CIH Institution 10 “[We] would like to have the resources to be able to see the outcome data to show the effect of our implementation” – CIH Institution 7
Discussion
The current study addresses a significant gap in the literature by providing an understanding of the undocumented outreach CIH academic institutions’ have had engaging with marginalized, underserved and racial and ethnic communities to increase healthcare access and utilization. To better understand the CIH academic institutions’ partnerships, the scope of services provided, impact, and challenges, we interviewed representatives of 13 CIH institutions across the US and Canada and extracted their feedback on their knowledge and experiences.
The study yielded several notable findings. First, CIH institutions demonstrated a purposeful and longstanding dedication to actively partner and engage with marginalized, underserved, and racially and ethnically diverse communities. This effort was aimed towards increasing healthcare access and utilization, and rooted in the trust they had built with their partners. These results correlate with existing literature which highlight that successful academic-community partnerships arise from a genuine and intentional focus on equity, along with a commitment to establish trust and mutual respect.23,25,55,56 This is significant because such dedicated efforts not only bridge gaps in healthcare accessibility and utilization, but it also contribute to the overall well-being and empowerment of communities, ultimately fostering a more inclusive and equitable landscape for all. 57 Moreover, CIH institutions sought to enhance healthcare accessibility and utilization by proactively addressing the social determinants of health within their partner communities. This approach aligns with studies indicating that interventions targeting improved healthcare access and utilization must encompass efforts to address the social factors that may hinder individuals from accessing healthcare or attaining their health-related objectives.58-60 This finding reveals that CIH institutions and care systems are successfully leveraging effective methods to enhance healthcare access and utilization among marginalized, underserved, and racially and ethnically diverse communities.
Results also revealed that community connections are and have been important to the CIH academic institutions’ goals. Many key informants emphasized how their strategic plans and key personnel are committed to engaging with marginalized, underserved, and racial and ethnic communities, are intrinsically linked with their active community involvement. Literature25,61 supports such an approach by arguing that intentional application of culturally informed community engagements is necessary to enhance health equity practices and efforts. This study’s findings reveal that these institutions view active engagement with their surrounding community as a fundamental element of their mission, 1 that enriches the educational experience of their students and equips their practitioners and clinics to provide more effective care. This deliberate approach not only strengthens their relationship with the community but also reinforces their commitment to the well-being of all those they serve.
CIH institutions also showcased that they are focused on providing equitable healthcare to all. Their reach spanned socioeconomic status, housing status, criminal history, age, immigration status, race, ethnicity, and sexual and gender orientation. This inclusive approach is further reinforced by the diverse range of healthcare services they offered, indicating a concerted effort to address the varied healthcare needs of their community partners. Furthermore, these CIH institutions were rooted in the basic tenets of patient-centered care62-64 and whole person health65-67 by responding to what the patient needs and addressing the social determinants of health in the lives of their communities.
A theme underscoring the positive influence of community engaged work on healthcare access and utilization revolves around its impact on students. By deliberatively integrating community outreach into their strategic agendas, CIH institutions not only demonstrate a commitment to educating their students but also to fostering a nuanced understanding of the communities they may eventually serve. Research consistently indicates that involving students in community outreach brings about favorable shifts in their emotion, thoughts, and actions. 68 CIH institutions reported noteworthy effects, with their students showing motivation to take proactive measures aimed at enhancing healthcare access and utilization after graduation. These measures included initiatives like establishing mobile or stationary clinics in low-income and marginalized areas. Some graduates aspired to instigate broader changes at the community and systemic levels. Consequently, the CIH institutions report that the approach of community-engaged care demonstrated a multiplier effect, extending its impact on equity beyond the targeted community. While the CIH institutions only had anecdotal information on the possible impact on students, they lacked concrete empirical evidence to substantiate the broader effects of these initiatives on the students’ professional development and community engagement. Such transformations and the systemic collection of data to demonstrate such changes are essential for realizing lasing improvements in healthcare accessibility and equity.68,69 While this study provides anecdotal data on impact, future research initiatives are necessary to assess the significant impact of students interacting with diverse populations and how it shapes their future professional practice.
While much of the community engagement endeavor taken up by CIH institutions was reported as successful, CIH institutions grappled with financial and staffing constraints in sustaining their efforts. Studies have revealed that CIH institutions receive very limited grants and funding and rely mostly on student tuition. 70 This has limited their capacity to not only do research but has also limited their reach among marginalized, underserved, and racial and ethnic communities and their efforts to increase healthcare access and utilization. Allopathic medicine institutions, many of which also rely on student tuition, also cite insufficient funding as a hurdle in their community engagement initiatives aimed at enhancing accessibility.29,30 Funding is documented as the cornerstone of efforts to improve healthcare access and utilization as it addresses resources, staffing, outreach and education efforts, implementation and research, and data collection.58,71 Funding also underpins initiatives to address health disparities, such as subsidizing the cost of treatments, making them affordable for individuals who face barriers and instituting cultural competency training and language accessibility. Therefore, securing robust and sustained funding is imperative to fortify and enhance the impact and reach of CIH institutions in their mission to enhance healthcare access and utilization for marginalized, underserved, and racial and ethnic communities.
Finally, while the CIH institutions have been reported being proactive at engaging with marginalized, underserved, and racial and ethnic communities in order to increase healthcare access and utilization, they still recognize that there is more to do. They have identified gaps in community partnership (eg, with Historically Black Colleges and Universities, Indigenous populations), specialty care (eg, women’s health), ways to intentionally measure short- and long-term impact, and resources (such as a diverse workforce) to positively influence access and utilization. More work is still needed and these CIH institutions commitment to improvement signifies their unwavering dedication to achieving lasting and meaningful advancements in healthcare accessibility and utilization for all.
The results of the current study should be interpreted in light of several limitations. First, the study relied on self-reported data and so it is possible that the institutions provided responses that were socially desirable or incomplete. Second, data came from an informed convenience sample of REACH Center member presidents, clinicians, and research deans, and therefore they may not be representative of all CIH academic institutions in North America, nor of their community partners and students. Future research with a larger and more representative sample including current and graduated students, community partners, and community members is needed to address these limitations.
Despite these limitations, this study represents a significant first step in understanding what CIH educational institutions are doing to address healthcare access and utilization needs. This study has not only shed light on the rich history of CIH educational institutions’ engagement with marginalized communities, but it has also highlighted the transformative impact of such endeavors. From dedicated outreach efforts to the proactive steps taken by inspired students, the influence of community engagement on healthcare access is encouraging. However, it is crucial to recognize the resource limitations and financial and staffing constraints that these CIH academic institutions grapple with underscoring the critical need for sustained funding. In addition, lack of resources also make it challenging to measure the direct impact of community engagement on access and utilization. These barriers hinder the proactive initiatives taken by the CIH insitutuions to address access and utlitzation disparities. By addressing these challenges and continuing to prioritize community engaged work, CIH institutions can play an instrumental role in bridging healthcare disparities and fostering a more inclusive and equitable healthcare landscape for all.
Footnotes
Acknowledgments
This work would not have been possible if it was not for the member institutions of the Research Across Complementary and Integrative Health Institutions (REACH) Center. We would like to thank the following CIH institutions, their presidents, and research directors: Bastyr University, Canadian College of Naturopathic Medicine, Canadian Memorial Chiropractic College, Maryland University of Integrative Health, National University of Health Sciences, National University of Natural Medicine, Northeast College of Health Sciences, Northwestern Health Sciences University, Palmer College of Chiropractic, Parker University, Southern California University of Health Sciences, Sonoran University of Health Sciences, University of Western States.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Board of Chiropractic Examiners and National Center for Complementary and Integrative Health of the National Institutes of Health under Award Number U24AT012549. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the National Board of Chiropractic Examiners.