
Abstract
Background
For individuals living with chronic conditions like diabetes mellitus and obesity, there is a need for sustainable behavioral strategies and physiologic tools. These tools support identifying and addressing barriers to healthy eating, reducing body mass index (BMI), and building increased physical resilience in real time.
Objective
To evaluate whether a 12-week learning management system designed to combine nutritional intervention with education and coaching on improving emotional intelligence (EI) could alter cardiometabolic outcomes.
Methods
This pre-post prospective study enrolled 37 adult volunteers with BMI greater than 25 to participate in a 12-week learning management system. Primary (BMI, systolic blood pressure, diastolic blood pressure, low-density lipoprotein [LDL], high-density lipoprotein, and fasting glucose levels) and secondary self-reported outcomes were assessed at baseline, 12 weeks, and 6 months after enrollment using Short Form-36, Emotional Quotient Inventory (EQi), and Whole Health Index (WHI). Linear mixed-effects regression models with random effect were used to estimate changes in primary and secondary outcomes. We adjusted for multiple testing using Holm step-down method.
Results
BMI and LDL were the only primary endpoints lower at program completion and 6-month follow-up compared to baseline levels (−1.63 and −17.77 mg/dL, respectively; P < .001). Secondary outcomes showing statistically significant improvement from baseline to 6-month follow-up included energy/fatigue (Short Form-36), self-regard (EQi), decision-making (EQi), impulse control (EQi), stress management (EQi), Whole Brain – Form A (WHI), Whole Food – Form C (WHI), and Whole Body – Form D (WHI).
Conclusion
This study provides preliminary evidence that lifestyle programs combining nutritional interventions and EI can have a significant impact on BMI and LDL. Our study highlights the potential importance of both nutrition and EI in programs targeting diet and lifestyle modification.
Introduction
Obesity and its associated comorbidities, including diabetes, heart disease, stroke, and some types of cancer, represent a major global health burden.1,2 Data from the 2017-2018 National Health and Nutrition Examination Survey reported over 42% of US adults as obese, with prevalence per state ranging between 20%‐44.5% that has tripled since 1975.1,3 The associated health care burden and economic costs have grown towards ∼ $1.96 trillion in 2020, with the projected economic increment to 4-25 by 2060, region depedent. 4 In the US, standard of care guidelines include recommending lifestyle changes like healthy diet and exercising as a first-line weight management approach.5,6 However, patients and clinicians are increasingly recognizing behavioral, socioeconomic, and personal lifestyle factors as barriers to these lifestyle choices and long-term weight loss. 7 These common barriers include perceived lack of time, perceived lack of support, situational barriers, and food cravings. There are also structural barriers to success in mitigating weight gain, such as the existence of food deserts and lack of safe places to exercise.
Despite the historical evidence supporting the impact of behavioral-centered lifestyle strategies on weight management, there has been a significant recent shift in attention and demand to integrate these sustainable behavioral strategies and physiologic tools to manage barriers to weight management and lifestyle changes; the goal is to support patients seeking to reduce body mass index (BMI) and build increased physical and mental resilience to respond to healthcare challenges in real time.8,9 Early work has suggested that eating and overeating is frequently a response to emotional stress. 10 Emotional stress can be often compounded by structural barriers comparable to those that impede lifestyle choices, including economic hardship; insufficient meaningful education and support; and systematic inequality. It has been theorized that interventions that support patients to respond to emotional stress can be meaningful and significant. Emotional intelligence (EI) has been directly associated with emotional stress. EI is defined as the ability to openly perceive and assess one’s emotions and generate new emotions that promote emotional and intellectual rigor and growth (ie, reasoning and decision-making).11,12 EI has been associated with higher orientation toward positive values, improved relationships, better attitudes, and greater adaptability.11-18
Much of the work regarding EI and health has been focused on mental health and well-being. Researchers have been able to demonstrate that higher EI is inversely correlated with lower psychological distress,15,19 depression,15,20 and anxiety21,22 and reduced anger, sadness, fear, jealousy, and sense of shame.22,23 Additionally, evidence shows that healthier individuals are more emotionally intelligent than those who are less healthy.24,25 EI has also demonstrated a significant relationship with self-perceived health,26,27 alopecia areata, 28 heart disease,29,30 and cancer.31,32 This evidence suggests that proactively incorporating EI into programs designed to support healthier lifestyle changes and sustainability will result in increased success and patient wellness. However, integrating EI with lifestyle-focused interventions to address weight management and cardiometabolic health has not been investigated previously.
The objective of this pilot study is to assess the association between emotional intelligence, cardiovascular health, and plant-based diets as a lifestyle management approach. We designed and tested a comprehensive 12-week learning management system (LMS) that combined a well-known dietary change, plant-based eating, with education and coaching to improve EI.
Methods
The reporting of this study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 33
Participants and Study Design
This pre-post, prospective, and proof-of-concept pilot study was designed to determine if use of a custom LMS in a clinical setting would alter cardiometabolic risk factors in an overweight adult population. Our 12-week LMS blended education and motivational techniques regarding plant-based nutrition and exercise with strategies to understand and improve EI (Figure 1). The study included 37 adult volunteers between the ages of 18 and 75. Patients in the Mayo Clinic Department of Family Medicine and Division of Community Internal Medicine received a recruitment flyer. Enrolled participants were assessed at baseline, 12 weeks (at the end of the LMS), and 6 months after enrollment. The 12-Weeks Plant-Based Dietary Program Transition Guide. 12-Week Dietary Transition Guide. Foods and drinks to reduce or eliminate: Group 1, Added sugars and salts, sodas and sugary drinks, condiments and snacks with high fat, sodium, and sugar; Group 2, processed packaged food; Group 3, beef and processed meats; Group 4, fried foods; Group 5, all meat except seafood; Group 6, seafood; Group 7, eggs and dairy products such as milk, yogurt, cheese, ice cream, cream, sour cream, and butter; Group 8, added oils such as margarine, salad dressing, mayonnaise, and cooking oils. Plant-based whole foods and drinks to add: Group A, drinks such as water, tea, and real fruit (not fruit juice) smoothies, nonfat condiments such as mustard, and snacks such as fruit, wholegrain bagels, fat-free baked wholewheat crackers, fat-free hummus, carrots, and celery sticks; Group B, live foods such as fresh fruit and vegetables; Group C, beans and mushrooms; Group D, food that has been steamed, baked, broiled or sauteed with vinegars (eg, sherry, white wine, balsamic, and apple cider); Group E, hemp, almond, soy, coconut, or rice products; Group F, Bean products (limited); Group G, Soy products (limited); Group H, fat-free salad dressings and vinegars (eg, sherry, white wine, balsamic, and apple cider).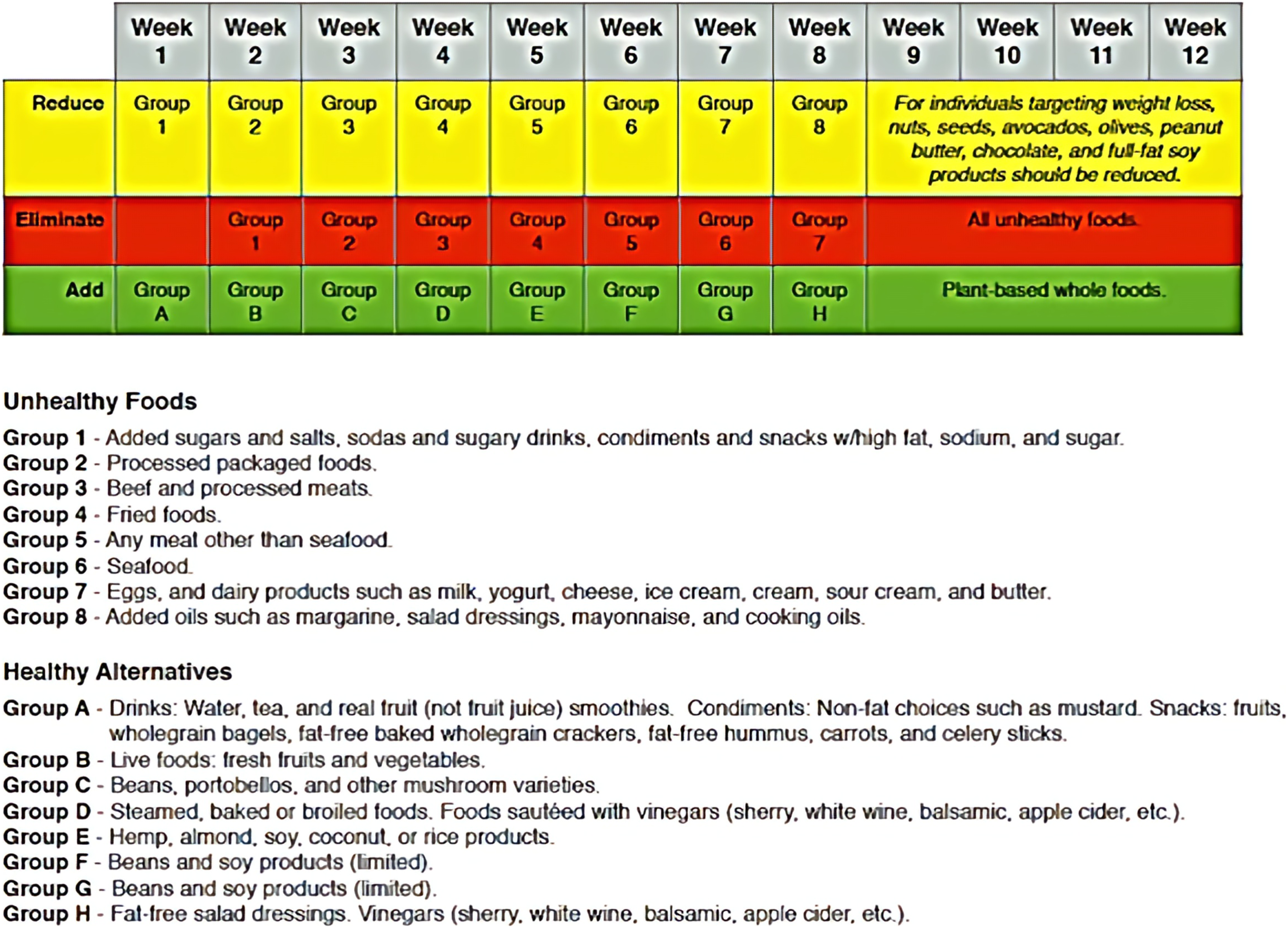
Inclusion and Exclusion Criteria
Patients ≥18 years old of any race and sex, with BMI >25 that demonstrated additional cardiometabolic risk factors, including metabolic syndrome, hypertension, elevated lipids, or elevated blood sugars, who were willing to have baseline, 12-week, and 6-month evaluations. We excluded patients who were <18 years old age and/or patients who are judged by their clinician or research personnel to have limitations in cognition, sensory input, or language as to face significant barriers to give written informed consent. Patients were invited to participate in the study by the clinical team during in-person visit or using electronic patient portal messages. Patients who expressed an interest in participating were briefed about the study and that participation is voluntary. Study activities were approved by the Mayo Clinic Institutional Review Board. All participants were recruited and consented according to approved study procedures.
Intervention
The 12-week dietary program consists of integrating and eliminating two main food cohorts; (1) non-plant based or unhealthy food options (to eliminate); and (2) healthy alternatives food options (to integrate). Each one of these two main food cohorts then include eight different groups of foods that are planned to be, gradually and attainably, reduced, eliminated, and/or reduced on a weekly basis plan as part of the overall 12 weeks program. The “Eliminate” food groups include processed or ultraprocessed foods and all meat-based foods. The “Reduce” food groups include restricting the quantity of high-calories healthy fat and full-fat soy products (eg, nuts, avocado, olive-based products, no-sugar dark chocolate). The “Add” food groups include plant-based whole foods and non-meat based healthy alternatives, including all fresh vegetables and fruits, legumes, beans, whole grains, and limited soy-based products. Participants received information on healthy eating and training on EI as they transitioned to this whole-foods, plant-based diet over the course of 12 weeks (as shown in Figure 1). The group met in person on a weekly-basis and tracked their progress in a nutrition and fitness journal and through a semi-guided group coaching discussions. The moderating staff is a trained professional on motivational-interviewing skills, goal-setting skills, accountability, and supportive behavior tracking.
Outcomes
The primary endpoint were changes in cardiometabolic and anthropomorphic profile as defined by BMI, systolic and diastolic blood pressure (SBP; DBP, respectively), low-density lipoprotein (LDL), high-density lipoprotein (HDL), and fasting glucose levels (measured at baseline, 12 weeks, and 6 months). Secondary, self-reported, outcomes at baseline and 6 months included using the following questionnaires: Emotional Quotient Inventory (EQi), designed to measure EI using 5 composite scales (intrapersonal, interpersonal, adaptability, stress management, and general mood); Short From-36 (SF-36), a questionnaire to assess overall quality of life with scores in 2 categories (SF-mental health and SF-physical health), and has been extensively used and validated in different weight-related patient populations34,35; and Whole Health Index (WHI), a novel validated measure that incorporates 6 domains (self-perception, interpersonal skills, stress management, decision-making, and self-expression components) (Supplemental Table 1).
Statistical Analysis
Cardiometabolic Risk before and after a 12-Week Learning Management System to Alter Risk.

Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SBP, systolic blood pressure; SE, standard error.
aThe change in each outcome between time periods was estimated from linear mixed-effects regression models with random effect.
bP values ≤.0056 were considered statistically significant after a Holm step-down adjustment for multiple testing.
Changes in SF-36, EQi, and WHI From Baseline to 6-Month Follow-Up.
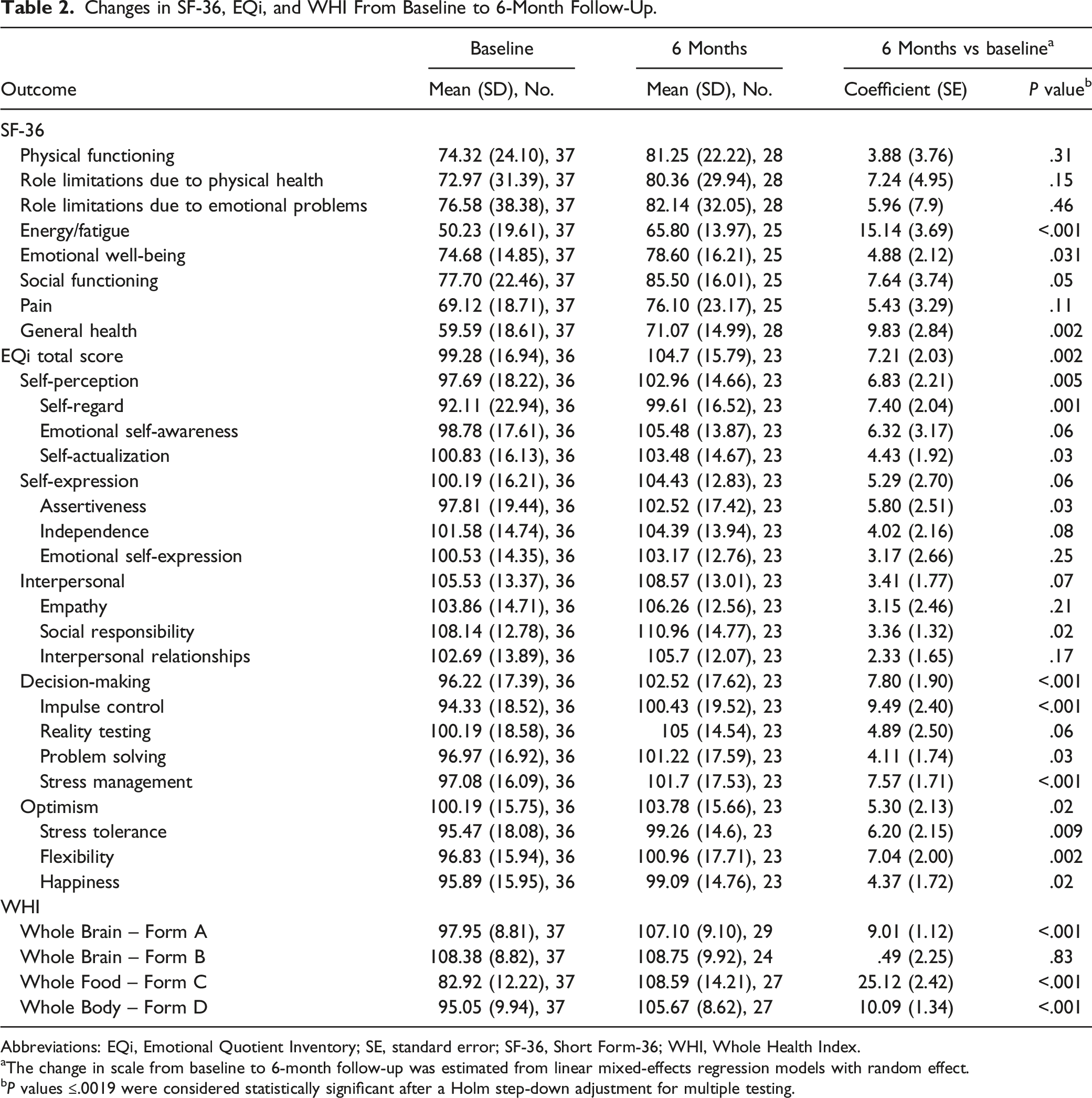
Abbreviations: EQi, Emotional Quotient Inventory; SE, standard error; SF-36, Short Form-36; WHI, Whole Health Index.
aThe change in scale from baseline to 6-month follow-up was estimated from linear mixed-effects regression models with random effect.
bP values ≤.0019 were considered statistically significant after a Holm step-down adjustment for multiple testing.
Correlation of Baseline SF-36, EQi, and WHI With Change in BMI and LDL From Baseline to 12 Weeks.

Abbreviations: BMI, body mass index; EQi, Emotional Quotient Inventory; LDL, low-density lipoprotein; SF-36, Short Form-36; WHI, Whole Health Index.
aCorrelations between baseline assessments and change in BMI and LDL from baseline to 12 weeks were evaluated using Pearson correlation test.
bP values ≤.0015 were considered statistically significant after a Holm step-down adjustment for multiple testing.
Changes From Baseline to 6-Month Follow-Up: Correlation of SF-36, EQi, and WHI With BMI and LDL.

Abbreviations: BMI, body mass index; EQi, Emotional Quotient Inventory; LDL, low-density lipoprotein; SF-36, Short Form-36; WHI, Whole Health Index.
aCorrelations for the change from baseline to 6-month follow-up assessment results with change in BMI and LDL from baseline to 6-month follow-up were evaluated using Pearson correlation test.
bP values ≤.0016 were considered statistically significant after a Holm step-down adjustment for multiple testing.
Results
Our study included 37 participants with a median (range) age of 59 years (29-77); participant demographics are available in Supplemental Table 1. After adjusting for multiple tests (Holm step-down method), BMI and LDL were significantly lower at 12-week and 6-month follow-up compared to baseline levels. The mean change in BMI and LDL from baseline to 12 weeks was −1.63 and −17.77 mg/dL, respectively (P < .001). Oxn the other hand, HDL, blood glucose, and blood pressure markers were not statistically significant.
After adjustment for multiple testing, the only self-reported scales that showed statistically significant improvement from baseline to 6-month follow-up were energy/fatigue (SF-36); self-regard, decision-making, impulse control, and stress management (all sub-constructs within EQi); and Whole Brain – Form A; Whole Food – Form C; and Whole Body – Form D (components of WHI) as shown in Table 2.
When assessing correlation between measures of SF-36, Emotional Quotient Inventory (EQi), and Whole Health Index with change in BMI and LDL-C from pre-to post-program, BMI and LDL were the only primary endpoints that showed statistically significant short- and long-term improvement. Correlation of baseline assessments with changes in BMI and LDL from baseline to 12 weeks was therefore assessed. None of the baseline assessments were significantly correlated with change in BMI or LDL from baseline to 12 weeks after adjustment for multiple testing (Table 3). Improvements in emotional well-being (SF-36) and WHI subscales were correlated with reductions in BMI from baseline to 6-month follow-up after adjustment for multiple testing (Table 4).
Discussion
This study was designed to evaluate whether a 12-week LMS combining education and motivational techniques regarding plant-based nutrition, exercise, and EI concepts would improve cardiometabolic risk factors in overweight individuals. Of the primary outcomes assessed, BMI and LDL showed short- and long-term significant improvements when compared to baseline levels. Additionally, there was a significant improvement from baseline to 6-month follow-up in the following secondary outcomes: energy/fatigue (SF-36), self-regard (EQi), decision-making (EQi), impulse control (EQi), stress management (EQi), Whole Brain – Form A (WHI), Whole Food – Form C (WHI), and Whole Body – Form D (WHI).
Recent evidence has strengthened the association between stress management, EI, and weight loss to combat obesity. Several studies have shown that individuals who are obese are more likely to experience mental health difficulties, including social anxiety and depression.37-39 Inversely, patients who achieve weight loss have reported significant improvements in anxiety and depressed mood. 35 Consistent with current evidence,40,41 our analysis showed that EI training can improve decision-making, impulse control, and stress management, 3 of the 5 scales of the EQi. Furthermore, our findings demonstrated that weight loss is associated with improvements in energy and fatigue assessed by the SF-36.34,35
In a 2010 meta-analysis by Martins et al, 16 improved EI, and its fundamental traits like self-regulation, was correlated with improved mental, psychosomatic, and physical health as well as decrease in emotional overeating, 42 which is a risk factor for obesity. 43 EI can be developed and improved through education and training.40,44 To date, however, the application of EI training in the clinical setting remains limited.45-47 There are exploratory studies identifying associations between EI and health-related outcomes, but to our knowledge, there have been no clinical studies investigating EI training in the context of obesity and cardiometabolic risk factors. Previous research has shown that individuals with eating-disordered attitudes measured by Global Eating Attitudes Test-26, have lower emotional self-awareness, poorer mood, and less stress tolerance. 41 Therefore, it has been hypothesized that individuals who are more capable of expressing and regulating their emotions may be less likely to engage in maladaptive eating behaviors than those with lower EI.
Another important competency associated with EI is self-motivation which is an essential factor for treatment adherence and achievement of goals. Motivation is often correlated with the extent to which an individual engages in weight-related lifestyle behaviors and is a key factor in improving metabolic syndrome components.48-50 Thus, our findings may partially suggest that individuals with higher EI who are better able to self-motivate will have better outcomes associated with weight management and metabolic health.
Finally, individuals with higher EI scores tend to report less stress.22,40 There is strong evidence that associates stress levels with certain hormonal and biomarkers as well as behavioral changes.34,51 This may explain the decrease in our study population not only of weight but other cardiometabolic markers associated with stress.
Strengths and Limitations
Our study had several noteworthy limitations. Some clinical measures were not available at the different time points for every participant; therefore, we used linear mixed-effects regression models so all available data were included for each patient. Additionally, data were only assessed at two postintervention time intervals, and behavioral patterns may have changed during subsequent periods. Furthermore, we did not account for medication changes that may have occurred during the study period. Although we have objective measures for anthropomorphic and cardiometabolic factors, psychological and emotional evaluation was obtained via self-assessments (ie, SF-36, EQi, and WHI).
A strength of our study was that the program was offered in person. In-person lifestyle programs tend to lead to higher weight loss than other platforms.48,52 However, a future study could evaluate delivering the educational material online or via a smartphone application, which would facilitate scalability and reach. While the study population was more educated than the general population (89.2% with college education or above), the population was ethnically and racially diverse, with ethnic minorities representing 62.2% of our study population (Supplemental Table 1), corresponding to current trends of obesity among minority populations.1,3,6 A future direction could be to explore the potential variances in cardiometabolic, physical, and emotional health between different ethnic populations before and after intervention.
Conclusions
It has been Obesity and other components of cardiometabolic dysfunction, stress, and mental health remain major challenges for many individuals. This study is first of its kind that shows how lifestyle programs that integrate nutritional and coaching interventions and EI-centered strategies can significantly impact certain cardiometabolic profile (BMI and LDL) in a adult overweight population. These findings align with previously demonstrated evidence of how physical and emotional health are strongly interdependent as well as the importance of lifestyle-centered interventions to address them. These findings warrants further development and study, especially in larger randomized and diverse settings.
Supplemental Material
Supplemental Material - Nutrition and Emotional Health Education: The Use of Emotional Intelligence and a Plant-Based Diet to Reduce Cardiometabolic Risk
Supplemental Material for Nutrition and Emotional Health Education: The Use of Emotional Intelligence and a Plant-Based Diet to Reduce Cardiometabolic Risk by Abd Moain Abu Dabrh, Claire B. Haga, Jarik Conrad, Adam I. Perlman, Megan A. Allyse, Monica L. Albertie, Maia Martinez-Heath, Colleen T. Ball, and Floyd B. Willis in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgment
The Scientific Publications staff at Mayo Clinic provided copyediting, proofreading, administrative, and clerical support.
Authors’ Contribution
Conceptualization and methodology: A.M.A.D., C.B.H., J.C., M.L.A., M.M-H., and F.B.W. Data curation and analysis: A.M.A.D., C.B.H., A.I.P., M.A.A., C.T.B., and F.B.W., Writing- Original draft preparation: A.M.A.D. and C.B.H. Writing- Reviewing and editing: A.M.A.D., C.B.H., J.C., A.I.P., M.A.A., M.L.A., M.M-H., C.T.B., and F.B.W.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Notes
Dr Martinez-Heath is now a practicing physician in private practice.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.