
Abstract
Background
While there is recognition by the greater medical community and physical therapists to address the biopsychosocial needs of people with chronic, persistent pain, there are challenges in implementation and delivery including wide variability in interventions, lack of clear rationale, and absence of clinical models that are feasible and acceptable on a large scale. Important components for psychologically informed physical therapy (PiPT) for pain care include behavioral approaches (e.g., Acceptance and Commitment Therapy), mindfulness, pain neuroscience education, motivational interviewing (MI), and interoceptive skills-building. The Empower Veterans Program (EVP) Mindful Movement framework blends these components and emphasizes a mindfulness and self-compassion approach with MI and body-based experiential learning. This program was offered in-person at the Atlanta and Maryland VA Health Care Centers with published positive Patient Reported Outcomes (PRO) pre-COVID 19 crisis and shifted to entirely remote delivery in March 2020.
Objective
This paper offers an evidence-based and theory driven framework to operationalize a remotely delivered group-based psychologically informed mindful movement physical therapy intervention as part of an interdisciplinary pain care program.
Methods
Since 2021 PRO and demographics are collected using a survey administered through Qualtrics over a 12-month period at baseline, immediately post TelePain EVP, at 6 months, and at 12 months, with findings forthcoming.
Discussion/Results
Tele-pain EVP offers 6-9 groups a week with 7-9 veterans from Atlanta based team and 3-4 groups a week with 5-9 veterans from Maryland based team. Adaptations for remote delivery optimized mindfulness and active learning strategies including interoceptive skills-building and use of MI to support self-efficacy to trust, restore a sense of safety in the body, and explore adaptations for safe movement.
Conclusion
TelePain-EVP Mindful Movement provides a framework for other programs to translate for their populations and systems to further develop best practices in PiPT for pain care and integration into interdisciplinary care.
Keywords
Introduction
The socio-economic burden of chronic pain incurs an estimated $560 billion a year in direct medical costs, lost productivity, and disability programs.1-6 Age adjusted prevalence of chronic pain among adults in the US in 2021 has been reported as 19.2% of nonveteran and 27.5% of veteran populations with 6.2% reporting high impact chronic pain for nonveterans and 9.1% for veterans. 7 Upwards of 50-75% of veterans in care at the Department of Veteran Affairs (VA) report chronic pain, and also have poorer self-rated health, greater utilization of heath care resources, greater prevalence of health risk behaviors, decreased social and physical activity, lower social support, and greater psychological distress and substance use disorders.8-10 Contributing to the complex picture and needs of the veteran population are racial, social, and economic inequities which are associated with greater functional decline. 11
A primarily biomedical approach does not address the wholeness of the person experiencing chronic pain, nor their layered challenges including socioeconomic and structural inequities and inadvertent consequences of opioid analgesics which may have been prescribed for lack of better options.12-16 Best practices for a whole-person model of care, including for pain care, recommend integrating nonpharmacological, complementary, and integrative health interventions into a multimodal approach using a biopsychosocial framework (BPS).1,17-21 Improved outcomes are more likely when physical, emotional, and existential strengths and challenges to well-being are concurrently addressed rather than focused exclusively on physical treatment.22-24
The Veterans Health administration (VHA) uses an evidence-based stepped care model of pain management to address this complex biopsychosocial approach to pain care.25,26 Step 3 programs include interdisciplinary care for people with chronic pain and high levels of comorbidity and complexity.25,26 There are a growing number of step 3 programs in the VHA which are interdisciplinary, consist of intensive multimodal care, and have shown improvements in patient reported outcomes such as increased function, and decreased pain catastrophizing and sleep difficulties.25,26 The Empower Veterans Program (EVP) is an example of a Step 3 Tele-Pain program that is interdisciplinary, multimodal, emphasizes a biopsychosocial approach, and includes the Whole Health Model.25,27 EVP is a weekly 30 hour remotely delivered program (3 hours a week, on one particular day of the week, for 10 weeks) for veterans with high impact chronic pain. EVP is delivered in a group medical appointment format with cohorts ranging from 3-20 veterans. The program consists of an interdisciplinary team with each facilitator leading a class focused on Acceptance and Commitment Therapy (psychotherapist); mindful movement (physical therapist); and whole health/mindfulness (chaplain).
This interdisciplinary work necessitates each facilitator to have a sensitivity to and general knowledge of one another’s areas of expertise and professional strengths for consistent messaging and for optimal reinforcement and integration of material.20,28 For EVP physical therapists (PT) this means supporting the topics taught by the psychologist and chaplain while integrating PT specific material within the mindful movement class. The development of psychologically informed physical therapy (PiPT) programs help physical therapists integrate emotional/cognitive components of care and is advantageous to implementation of interdisciplinary programs.22,29-31
Typical components of PiPT interventions include some combination of education, cognitive-behavioral techniques for addressing coping strategies and responses to pain, and practices that influence psychophysiology such as body awareness and mindful movement.31-34 The inclusion of patient centered communication (e.g. motivational interviewing) aid in supporting a healthy therapeutic alliance and self-efficacy for change.31-34 Interest and evidence for PiPT practice continues to grow for pain-related conditions when compared to standard physical therapy for improving physical function, disability, psychological outcomes, and pain.22,31,32,34,35 Challenges to implementation and delivery of PiPT include wide variability in programs with no clear rationale or framework for inclusion, or exclusion, of specific components.22,31-34 The lack of clear competencies, rationale, framework, and clinical models that are feasible and acceptable make it difficult to develop, adopt, and apply best practices for the spread and adoption of PiPT programs.22,23,31,33,36
This paper hopes to support the development of best practices by offering a framework for psychologically informed mindful movement that includes a theoretical background, rationale, implementation data, and changes made for remote delivery (TelePain-EVP). This framework may support PTs as they integrate into interdisciplinary pain care teams to implement mindful movement based on an evidence-informed, theory-driven, biopsychosocial model. Findings from the on-going implementation evaluation of TelePain-EVP may inform patient-centered systems of care, practice, and policy decision making adapted to remote delivery.
Theoretical Foundations for Psychologically-Informed Mindful Movement Physical Therapy for Pain Care
Acceptance and Commitment Therapy Based PiPT
A number of different behavioral interventions could be incorporated into PiPT. The choice should not only be based on being an evidence-based therapy (EBT), but also on being congruent with other frameworks for a particular PiPT. ACT is an EBT shown to be feasible, acceptable, and with a growing evidence base for addressing key measures for a pain intervention. Several specific measures with clinical improvements after ACT include: pain (interference, and intensity), anxiety and depression, disability, quality of life, and for promotion of physical activity.22,37-39 ACT is intentionally transdiagnostic, meaning that it is not oriented to a particular diagnosis (e.g. pain, depression, anxiety). 40 ACT is concerned with developing a deeper psychological flexibility for all of one’s life congruent with a whole-person and mindful approach to well-being. Furthermore, ACT is values-based, in that it aims toward goals only if those goals are aligned with one’s life purpose(s).
Six Core Processes of ACT.

ACT informed PiPT has demonstrated improvement for back-related disability, function, and pain-interference, addressed barriers for engagement in physical activity, and patients report the program supports greater internal awareness that their whole being was not defined by their pain experience.22,36,44,46
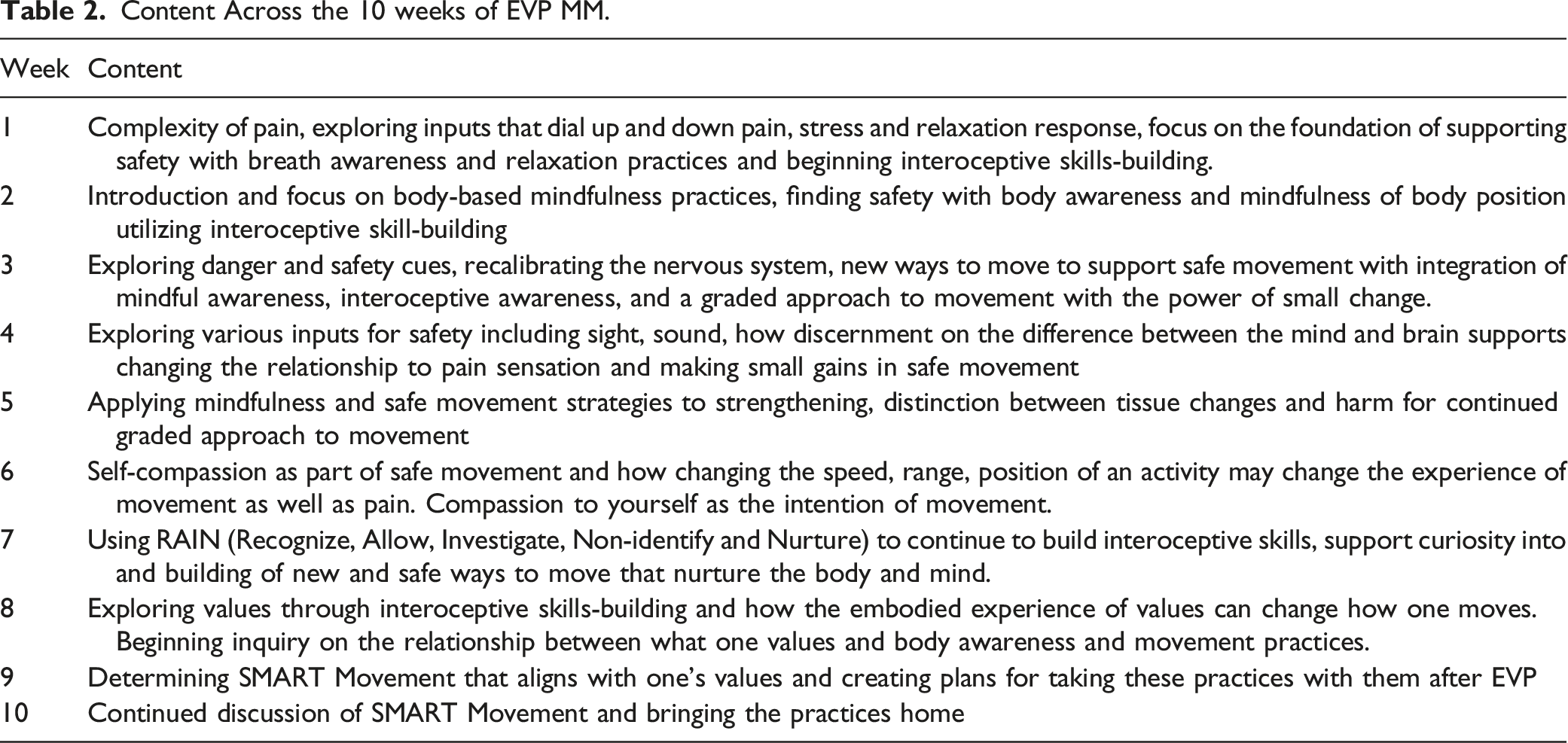
While ACT informed PiPT is promising, delivery by PTs is mixed and inconsistent for which of the six processes are utilized and for adherence to ACT methods throughout interventions.38,44 Continued clarification is needed to implement all six interlinked processes of ACT for physical activity promotion and PiPT. ACT informed PiPT may support fully embracing the current experience (e.g. to both notice and allow for distressing thoughts, emotions, and/or body sensations without judging or trying to change or fix them) while encouraging the person’s commitment to valued living as ongoing motivation to explore movement in new and adaptive ways.38,44 These six processes of ACT are integrated throughout the EVP Mindful Movement framework described below and in Figure 1. Framework for EVP Mindful Movement: Supporting safety and trust building and empowerment with Motivational Interviewing provides a foundation for the program. The structure of the program includes practices that emphasize interoceptive skills-building for self-regulation and resilience; incorporation of values and moving towards what matters as part of SMART movement strategies; and renewed relationships with sensation as the person gains insight into how to apply these learnings to movement to make small changes towards what matters. Overarching each teaching is how to make choices for committed action under an umbrella of mindful awareness with self-compassion.
Mindfulness within an ACT Informed PiPT
Mindfulness can be defined as a nonjudgmental noticing of the present-moment experience including body, mind, and environmental phenomena with an attitude of open curiosity and acceptance.37,47 Mindfulness based interventions can vary in content and structure, however at their core they teach the person ways to observe and accept (rather than to avoid or suppress) the various body, mind, environmental stimuli with a present-moment, open, nonjudgmental attitude. Mindful awareness training is thus not aiming at changing unpleasant thoughts, emotions, and/or body sensations themselves, but rather changing the relationship and reaction to these stimuli. Mindfulness and acceptance based strategies have been shown to be associated with decreasing depressive symptoms, anxiety, stress, fatigue, pain, and with improving quality of life and sleep quality in people with chronic pain conditions.43,45
The addition of mindfulness practices to cognitive behavioral therapies has resulted in effective treatments. 48 However, compared to change-based cognitive behavioral approaches, ACT seems to be more congruent with mindfulness approaches as each shares nonjudgmental and open noticing of the present moment experiences of the body, mind, and environment. 48 Four of the ACT processes (de-fusion, acceptance, present moment awareness, and self-as-context) are directly shared with mindfulness perspectives. These processes and mindfulness teachings may help the person adopt a more flexible attitude accepting the moment to unfold as it is with insight into how thoughts and sensations may occur in the body or mind without these stimuli (e.g. pain) defining the totality of oneself. 48 This shift in perspective can lead to greater acceptance of oneself, others, and of one’s circumstances. 48 The final two ACT processes of value exploration and committed action are essential to behavior change. 49
Pain Neuroscience Education
Pain neuroscience education (PNE) is an integral part of physical therapy pain care. PNE supports a reconceptualization of pain including helping to reframe beliefs around fear of movement, or other adverse relationships to pain, that inhibit a return to function and/or negatively impact quality of life.20,28,50-52 Through PNE the person may gain insight that helps them shift from a perspective of pain as equal to tissue damage to a more broad understanding of pain as a protective and adaptive response which may be activated from a wide array of body, mind, and environmental stimuli.28,50-53
Evidence suggests that PNE is not an effective intervention by itself and that PNE should be part of a larger picture of a full biopsychosocial (BPS) intervention.20,51,53,54 Integration of PNE with active interventions and cognitive based approaches demonstrates a synergistic and larger effect for clinically important improvements in pain and disability, kinesiophobia, and function.20,51,52,55 Integration of mindfulness and acceptance based approaches may help provide insight into BPS contributors to pain and change perceived threat and activations for danger thereby influencing pain catastrophizing and activity-related fear.20,51 An ACT-informed PNE approach would encourage psychological flexibility so that the person learns to seek out potentially maladaptive pain behaviors while exploring new ways to relate to stimuli, and to connect one’s movement with one’s personal values. Choosing an ACT-informed approach is congruent with a PiPT practice emphasizing the learning of how “to be with” distressing thoughts, emotions, or sensations rather trying to change them.
Motivational Interviewing for Pain Neuroscience Education
One possible limitation of PNE may arise from how it is communicated. PNE from a primarily didactic approach can be felt as confronting to a person’s beliefs which may then be met by a reluctance to accept the education (including potentially labeling the training as irrelevant to one’s situation).28,56 Shifting the mode of delivery from more didactic approaches to emphasizing patient-centered communication may foster receptivity to examine one’s beliefs, support willingness and readiness for change, and to explore personal relevance.20,28,50,52,56 Motivational Interviewing (MI) is a patient-centered communication style supportive of an empowering therapeutic alliance to allow personal insight for intrinsic motivation for behavior change.20,52,57 The guiding style of communication of MI draws out the person’s own reasons for change and pre-existing internal strengths for change. 57
MI-consistent PNE would include requesting consent before offering information in a shared-decision making process (“elicit-provide-elicit”) to reinforce the client’s own problem-solving skills and to empower self-guided behavior change. 57 MI can match language to the person’s stage of readiness and willingness to change to support knowledge-sharing about pain, awareness of one’s beliefs, and developing insight into BPS factors for safety and danger which may affect the threat value of pain. 52 This guiding style of communication provides insight to individualize PNE (e.g. examples to draw out and build from), to ascertain beliefs that may be obstacles to learning and change, and to identify specific interventions aligning with the person’s preferences and values.20,52,53 Using MI with PNE has shown positive effects for the management of chronic pain and adherence to treatment and is well-aligned with a PiPT acceptance and mindfulness approach to pain care. 52
Active learning to Empower and Embody Pain Neuroscience Education
PTs can utilize many tools to support learning of PNE along a continuum of more passive modalities (e.g., external heat applications or some manual therapies) to cognitive or didactic education, to more active learning strategies (e.g., movement). With their expertise in the movement system, PTs can utilize and emphasize an applied, active strategy of imparting PNE. Active strategies have demonstrated they can support PNE and provide an opportunity to translate the skills learned into real-life application for movement.51,55 The group format can be advantageous to active learning as each person explores movement with real-time feedback from others in the group supported by the PT. Listening to others and learning what works and does not work for each person reinforces that there is not a “one size fits all” approach to movement. The person learns that movement is an individual endeavor, and they are encouraged to explore and choose different ways to move with confidence and ease. Sharing what works for them, and listening to others, can provide insight into new strategies for movement. Additionally, with PTs offering remotely delivered care, it is vital to identify and maximize these kinds of active learning strategies to empower clients in effective self-care.
Interoceptive Learning to Reinforce an Experiential Approach to Pain Neuroscience Education
Interoception comprises the bidirectional communication between the brain and body representative of our internal state and includes the processes by which we sense, interpret, integrate, and regulate signals within our body. 58 From a PNE perspective, interoceptive skills-building helps the person notice relationships between inputs (physiology, and BPS factors that influence threat or safety), and the output/experience of pain.58,59 These insights empower the person to recognize their own unique triggers with less judgement, to build trust in themselves, and to find ways to change the relationships and reactions to these bodily activations. From an ACT and mindfulness approach to PiPT incorporating this interoceptive noticing into movement, with strategies for regulation, can help build trust and restore a sense of safety in one’s body while exploring what is possible to decrease threat with movement. The person learns to use their own discernment to adapt and modify through this moment-by-moment sensing and making small changes in posture and various aspects of movement (e.g., range, speed, muscle activations, effort) to increase the sense of safety. Essentially, interoception provides “in-built” biofeedback through which the person can unlearn habitual bodily reactions to BPS stimuli and patterns of moving that may exacerbate the experience of pain. New relationships to BPS stimuli and new ways to move can then be supported through active strategies of body awareness and exploration of safe movement. This interoceptive skills building is foundational to shift from a cognitive learning of PNE to a body-based, experiential knowing.
Framework for EVP Mindful Movement
The above-described theories were explicitly selected to create an evidence-informed, theory-driven model for the mindful movement component of the interdisciplinary Empower Veterans Program (EVP) at two host facilities. The framework for this comprehensive mindful movement program may support the development of best practices to implement a PiPT mindful movement physical therapy program for pain care that has real-world implementation, has been adapted for remote delivery (TelePain-EVP), and can be integrated within interdisciplinary teams. (Figure 1)
The Foundation: Steps of Safety and Trust Building and Empowerment with Motivational Interviewing
The foundation of EVP MM, Supporting Safety, builds on key teachings shared by PNE and mindfulness which describe the importance of identifying and supporting safety cues, or a “warm pathway”, for the person to experience peaceful, calm, or regulated states.47,51 For those with greater dysregulation, such as in chronic pain, it may be essential to achieve some measure of body-mind regulation as a beginning step for mindfulness practices and for finding cues of safety taught in PNE. 47 PNE teaches that by becoming aware of a particular perceived threat received via any input (e.g. visual, auditory, cognitive, emotional, or social), and by then reassessing the credible evidence of danger, that the threat level changes, helping modulate the pain output. 51 The person learns to notice what their personal “danger” cues are (e.g. nociceptive, emotions, social situations), how they show up as bodily activations, and how they impact the pain experience. 51 At the same time, the person learns their own “safety” cues to help cultivate peaceful and calm mind-body states. Ultimately, the person discovers how to engage the factors that increase or decrease threat and safety which enables them to reduce fear, increase movement, and to explore and change beliefs, behaviors, and lifestyle choices that may decrease the intensity or interference of pain for an improved quality of life.20,51 These insights into safety and danger cues, and their effect on the mind, body, and behavior, empowers the person to find ways to “dial up” safety with its de-activation of heightened protective responses and potential to “dial down” one’s pain experience.20,51
Upon the foundation of supporting safety is the next step of trust building and empowerment with motivational interviewing. The spirit of MI within group inquiry, supports trustworthiness of the facilitator(s), and centers the authority and responsibility for choices on the client, with the practitioner coaching alongside. Participants are encouraged to explore what they notice about how safety and danger show up in the body as well as what inputs contribute to a sense of safety or a sense of danger. Furthermore, the group format supports idea-sharing for how the practices can be used to support greater safety in the body and mind, and to problem-solve next small steps for application to one’s daily life activities. Thus, the group provides a space for gathering insight from one another as peers and active decision makers in their own care plans.
First Pillar: Building Body Awareness with Interoceptive Skills-Building for Self-Regulation and Resilience
The first pillar emphasizes body-based experiential learning to facilitate greater body-mind self-regulation and resilience through interoceptive skills-building. Developing awareness of how stimuli contribute to bodily activations or relaxations is taught as a step before considering changing one’s response to danger or safety cues. Breath and body awareness practices (e.g., diaphragmatic breath, progressive muscle relaxation, posture changes) provide tools to help decrease maladaptive body-mind activations and to support more regulated, parasympathetic-dominant states. Biofeedback practices for more objective noticing include tactile cues from hands on the body to monitor breath and body tension for insight into one’s patterns of activated or relaxed states in response to body, mind, and environmental stimuli.
Interoceptive skills are incrementally introduced and supported throughout the 10 weeks as the person is encouraged to develop a nonjudgmental noticing of inner sensations (e.g., heart rate, qualities of breathing, muscle tension) particularly in relation to safety and danger cues. ACT and mindfulness concepts (e.g. acceptance, present-moment awareness, self-as-context, committed action) are essential and integrated into how movement is approached from equanimity to support body-mind regulation and to efficiently move between activated and relaxed states. Emphasizing kindness and compassion with movement (including the use of the pneumonic practice of RAIN-recognize, allow, investigate, nurture and non-identify) further supports this “warm pathway” to work with body and mind reactivity, support equanimity and trust, and to foster a larger window of tolerance to body, mind, and environmental stimuli. 47 Over the 10 weeks the person learns skills to appraise, integrate, and respond to body, mind, and environmental stimuli for healthy, adaptive self-management. 58 These learning strategies for self-regulation and resilience helps the person to maintain or return to the calm, homeostatic mind-body states that are indicative of the “safety” that was learned in the first steps of the program and to experience greater equanimity amongst the ever-changing stimuli of bodily sensations, emotions, thoughts, and outer circumstance.47,59-61
Over the course of the program, the practices move from establishing greater safety in the body to creating safe levels of activation for functional activities, including for independent activities of daily living (IADLs). Adaptive interoceptive skills-building is brought to movement practices as the person learns to match effort (e.g., how muscles engage or relax for a movement or activity) appropriately to the task, rather than over-engaging or moving in a way that increases danger signals. MI group dialogue reinforces the therapeutic alliance as each person shares their personal learnings as to how they promote safety in the body and mind to build greater capacity for movement and participation in life activities.
Second Pillar: Values and SMART Movement
The second pillar focuses on the integration of ACT processes of values and committed action. An MI approach encourages each person to self-identify what they value (e.g., what is important, what matters) to provide direction for committed actions towards one’s purpose. The group discussion format has been useful in meeting the challenge that arises when working to distinguish goals from values and exploring how to match movement intentions to one’s self-identified values and purpose.
SMART goals (Specific, Measurable, Attainable, Realistic, Time-bound strategies) were initially used to support these topics of committed action and movement towards what matters for each individual. However, this approach was not well aligned, and in some ways seemed contrary, to the layered theories emphasized in this ACT and mindfulness informed PiPT program. The perspective inherent to this program needed to emphasize a shift away from focusing on the particular attainment of a “thing” to the emphasis on an aim to move towards what matters. To this point, it was observed that by using the word “goals” it sometimes unnecessarily increased participants’ angst, for example a longing to return to some past function or identity, or a hopelessness or frustration regarding a future they may not be able to attain. There was a need to identify an approach for committed action that mindfully acknowledged and allowed for the day-to-day, moment-by-moment changes in the body, mind, and/or environment that is the regular experience of the person with chronic pain.
In the spirit of iterative QI, the phrase “SMART Movement” was piloted, and after positive reception by veterans was adopted, to use the same acronym to identify present moment approaches to body awareness and movement supportive of one’s values. This adaptation addresses the tension of actively acknowledging the fluctuating nature of pain, while encouraging safe levels of movement, all within the framework of committed action toward what matters. Present moment interoceptive awareness is utilized to encourage mindful welcoming of body, mind, and environmental stimuli as well as the empowerment to choose strategies for self-management towards one’s values. The person reflects on a range of body practices from relaxation, strengthening, and flexibility with unlimited modifications and adaptations. Application of SMART Movement goes beyond physical movement intentions within EVP’s training to all of life in the broadest BPS sense. Practices for relaxation or regulation can support intentions of rest, energy level, creativity, patience in relationships, or clearer thinking. Strength building practices (selecting from a range of exercises from isometrics to dynamic motion) also increase confidence, energy, and motivation. Examples of SMART Movement application from participants include: using a body scan and breath awareness while talking with others to be more present in the body and to be able to fully participate in conversations with the other person; balancing acceptance for what the body can currently do in this moment with the vision towards a more comprehensive exercise plan for this week to be better equipped to serve others in the future; or using relaxation practices and movement synchronized with breath to experience more energy, happiness, and quality of life in the body. By connecting body awareness and movement to what is valued, the person can maintain a mindful connection to the body without becoming overwhelmed or impeded by emotions such as regret or frustration. They can use these practices for improved quality of life, for energy management, and for participation in IADLs. SMART Movement provides a flexible approach that empowers the person to do the next committed action towards their valued living, all the while being open to the present-moment circumstances.
Work with values is also embedded into experiential learning and interoceptive skills-building to support body awareness and movement. Using the idea of safety input from PNE, reflecting upon one’s values can become another portal to foster body-mind regulation. Rather than moving from an intention of trying to meet a goal of a certain number of repetitions, of a faster speed, or of more weight lifted, the person is encouraged to move in a way that strengthens the intention of what this value feels like in the body. The person explores how connection to their values supports a more relaxed bodily state, the feeling in their body when they connect to this value (e.g., a sense in their body of lightness, expansion, stability, and/or vitality), the changes in breathing pattern or muscle tension, and even the change in movement itself. A result of intentionally aiming towards what matters alters the experience of movement itself. Ultimately the person learns how to move from a more regulated and safe bodily state to support greater ease and to develop a more equanimous relationship with sensations.
Third Pillar: Insight for Compassionate Application to Movement
The third pillar supports SMART movement to start, complete, sustain, and grow movement possibilities. This pillar reinforces insights gained for promoting safety in the body through making small changes towards valued living for direct application to movement.
The person who is experiencing chronic pain may potentially find movement very challenging and starting small may sound “weak”, or “not-committed”, or frustratingly slow. The foundational steps of beginning with supporting safety in the body and trust in the process and in the facilitator, is essential to work with these potential concerns. Using the teachings of mindfulness, acceptance, and self-compassion with an MI approach can support the person on this journey of movement exploration. The theme of “power of small change”, which naturally arises throughout the program, supports this compassionate perspective and permission to explore what it might mean to do movement safely at 5% or 10% of one’s maximal effort. The workability of acceptance and present-moment awareness alongside small steps along the way for committed action to valued living are discussed and supported with colloquial wisdoms such as “inch by inch is a cinch, yard by yard is hard.” Participants may be more likely to start and sustain movement practices as they gain their own conviction that small changes over time add up to have a lasting and meaningful impact.
MI discussions offer opportunities to explore how Mindful Movement can be translated to everyday activities. The MI approach encourages each person to find their own individual strategy for movement to enhance safety, regulation and resilience, and purposeful action to take small steps towards what matters. In a group format, each person learns from one another and develops a therapeutic alliance to work together to find solutions that fit each person’s situation.
By playing on the often acted upon belief of “no pain/no gain,” a reframing is offered based on the learnings of PNE, and of acceptance and mindfulness principles from EVP. “Know Pain/Know Gain” represents this shift to a mindful, curious, nonjudgmental approach whereby greater understanding of one’s pain (what input may dial it up or down) empowers the person to make gains as they find new strategies for self-care to re-engage in valued life activities. The 6 processes of ACT are incorporated into this movement application as the person considers the difference between the mind and the brain to encourage curiosity into an aspect of themselves separate from the fluctuating inputs of body, mind, and environmental stimuli (through use of present-moment awareness, defusion and self-as-context). In addition, PNE topics such as how “hurt does not equal harm” are approached through a MI-led discussion to both de-fuse from pain sensations and identify with something more (e.g., what is valued or one’s true self) for the purpose of committed action (defusion, self-as-context, values, action)
Body-based experiential learning is key to EVP Mindful Movement sessions as each concept provides an opportunity to find ways to support safety with movement while providing small steps for committed action for valued living. Interoceptive based mindfulness practices reinforce and provide direct experience of how bodily, mind, or environmental stimuli contribute to habitual patterns of tensing or moving that may perpetuate the pain cycle and to explore new safe ways of moving the body. A graded approach to movement focuses on each part of the body, starting with the spine and pelvis and moving to the shoulders, hips and feet, to notice maladaptive patterns and support new strategies for safe movement. From this foundation for safe movement, integration of the various regions of one’s body, as taught in the first sessions, become whole body movement. Postures and movement adapted from yoga and tai chi are integrated to reinforce a mindfulness and acceptance-based approach to whole body movement.
Ceiling: Choices for Committed Action
Each foundational step and pillar of EVP Mindful Movement offers a choice for committed action. In the spirit of MI, each participant is “in the driver’s seat” and the facilitator has an opportunity to return authority and responsibility to the client, over and over.
EVP MM offers an abundance of choices, of action steps. The foundation includes action steps for the development of greater safety and body awareness as well as self-efficacy for change. The action steps within the pillars help refine interoceptive skills-building and body awareness for self-regulation and resilience, develop plans for present-moment SMART movement towards what matters, and for insight into how to apply this to movement to take small steps towards change. Committed action throughout each stage of the program helps the person move from supporting greater safety to finding ways to be more engaged in valued living. The choice is theirs!
Roof: Mindful Awareness with Self-Compassion
Mindful awareness with self-compassion is the over-arching rooftop for Mindful Movement. Nonjudgmental attention to the present moment is the lens through which each topic is introduced and practiced. Exploring how to be compassionate to oneself frames each discussion regarding what safety in the body might mean or how they might choose to apply body awareness in movement. “N” for Nurture within the RAIN tool can become a habit to strengthen safety and reinforce a mindful and compassionate approach to the body and movement. This practice encourages the person to be present with the various bodily, mind, and environmental stimuli with equanimity. Choosing to regularly practice RAIN can support choices for a kinder approach to their body or movement. Movement choices form a large part of this being kind to yourself to be more rested, more energized, and more connected to valued living. One veteran encapsulated this perfectly when they stated, “movement is being kind to your present and future self”. When PNE is taught from this compassionate approach, a stronger therapeutic alliance is possible through providing opportunities and space for personal insight and application of each topic. Lastly, this present-moment focus supports the empowerment of each person to both understand their pain experience and to make small steps for movement that supports their valued living.
Content Across the 10 weeks of EVP MM.
Clinical Operationalization: Moving From In-person to Remote Delivery
Program evaluation for the in-person EVP program has demonstrated feasibility and acceptability through both completion and satisfaction rates, as well as promising improvements in primary pain outcomes of intensity, interference, and catastrophizing from pre-to- post EVP. 27 Improvements have also been noted for acceptance (activity engagement despite pain, willingness to experience pain), depression, anxiety, sleep disturbance, mindfulness (non-reactivity to negative thoughts and emotions, observing their experiences), fatigue, adoption of healthy self-care, greater positivity and empowerment to participate in life, changing medication use, and reduction in total mortality among veterans with chronic pain and opioid use.62-65
Transition to Remote Delivery
In March 2020, Atlanta VA Healthcare System (AVAHCS) EVP transitioned from an in-person format to TelePain-EVP, i.e., fully remote delivery, with onset of the COVID-19 Crisis. With active support from AVAHCS EVP, VA Maryland Health Care System (VAMHCS) EVP also transitioned to fully virtual care in May 2020. The two nationally networked sites of EVP continue to only deliver online services. In 2022, with change management leadership and technical support from TelePain-EVP Atlanta, TelePain-EVP Maryland, expanded care to veterans served by all four VAs in West Virginia.
Outcomes Collected for Telepain-EVP.
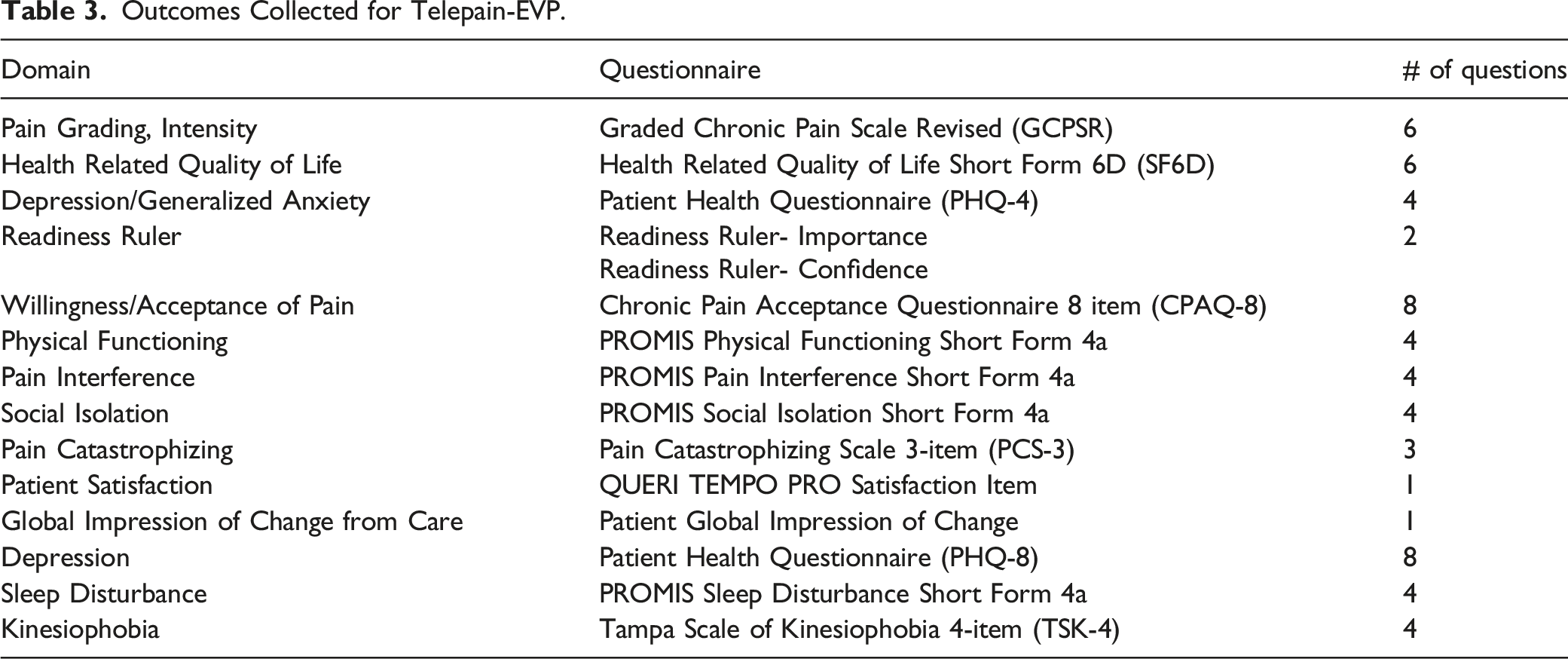
The patient-reported outcomes (PRO) and demographics battery of information are collected using Qualtrics, a secure cloud-based electronic data collection platform. Qualtrics has demonstrated validity for collection of PRO data within the VA system. 66 These measures are administered from within Qualtrics using a sequential, single-survey administration format. PRO are collected over a 12-month period including baseline (Week 1), post TelePain EVP (week 10), at 6-months (week 26) and again at 12-months (week 52). Veterans have the option of being contacted to participate in a qualitative interview within three weeks of completing EVP. If the Veteran agrees to be contacted for an interview they are entered into a sub-sample and subject to random selection. Emory University Institutional Review Board reviewed data collection protocols for ethical compliance. This project was determined as non-research and conducted as quality management. All veterans were provided project overview and intent prior to participation.
Telepain-EVP Atlanta provides 6-9 concurrent groups a week, each restarting approximately every 10 weeks, with an average of 7-9 veterans in each group. Telepain-EVP Maryland provides 3-4 concurrent groups a week with an average of 5-9 veterans in each group.
Quality Improvement Adaptations for Remote Delivery
The Mindful Movement component has been iteratively refined over time using the Institute of Healthcare Improvement’s Model for Improvement. 67 Aims for tests-of-change for this PiPT included increased experiential learning and reinforcement/integration of the mindfulness and ACT principles taught in the other two training components. Aims also focused on consistent facilitation from a MI stance of the groups’ discussions while exploring body-based experiential learning for each of the PNE principles. Specific adaptations for remote delivery presented unique challenges as well as being a motivator for innovation and rapid cycle improvement of Mindful Movement. Aside from being able to continue to serve clients with high impact chronic pain, even during a global pandemic, several improvements emerged and were kept.
One of these adaptations was how to replicate hands-on cueing or assistance with various exercises for safe movement. Tele-delivery required a shift to a more internalized and personalized experience of safety which was accomplished by introducing mindfulness and interoceptive skills building earlier and in more depth. This approach also provided greater support for personal exploration and autonomy to find safe movement. This focus on interoceptive skills-building begins before physical movement is initiated through noticing BPS cues of danger or safety and how these are reflected in the body. Mindful awareness and self-compassion are introduced and repeated throughout the practices with reminders of the power of small change so that each person can choose their expression of safe movement. After movements are described and modeled, participants are invited to “try it out” while encouraging them to explore their own version by changing speed, range, amount of effort (e.g., 10%) and even their own version of the movement itself. Cueing includes exploring what is sensed in the body and breath as they continue to make small changes. This process supports unlearning of patterns of movement which may trigger more danger signals, and it supports self-directed learning of how to live, moving with more confidence and ease.
Greater emphasis on motivational interviewing style inquiry also supports this personal empowerment to find unique ways to move safely. The group environment adds to this power of choice and variety of modifications as the participants share the unique ways they find to optimize safe movement. With tele-delivery a greater “menu” of options for variations and modifications is available to increase accessibility for safe movement. This includes using the bed or couch for supine versions (with in-person delivery the veteran might sit out of an exercise if they could not get to the floor). Overall, tele-delivery optimized the integration of mindfulness and interoceptive skills building and veteran empowerment for choice as they learn to tune into their body and make real-time adjustments to explore movement safely.
Discussion
This paper offers a PiPT framework for mindful movement that is evidence-based, theory-driven, and has real-world implementation with positive outcomes for an integrated approach to interdisciplinary pain care.63,65,68 With both national and international physical therapy organizations advocating for the role of PTs to support a biopsychosocial approach and integrating mental health, 37 this framework can support the development of best practices for PiPT. This paper offers insight into how to integrate ACT, mindfulness, MI, and PNE through an emphasis on interoceptive, body-based learning to optimize self-efficacy for movement. This framework may support PTs as they integrate into interdisciplinary teams to implement best-practices for a biopsychosocial model of mindful movement. This method of PiPT pain care may be particularly valuable and advantageous for working with people that have comorbid physical and mental health concerns and/or history of trauma and/or moral injury; those frustrated by treatments that have had limited/short-term success or when other approaches have not worked; and working with significant pain beliefs that are barriers to trying movement.
This program also demonstrates a successful translation to this approach for pain care to remote delivery. This shift to remote delivery created the opportunity to optimize active learning strategies including interoceptive skills-building, and use of MI to support self-efficacy to trust and restore a sense of safety in the body and explore adaptations for safe movement. With the prevalence of pain being comorbid with psychological distress and related to rural residence it is paramount that these programs are accessible to those with chronic pain.1,2,69-71 Online delivery of PiPT has been shown to be beneficial in reducing cost, increasing accessibility, retention, patient satisfaction, and to be non-inferior to in-person care. 72 The successful translation of this program to remote delivery provides benefit to those for whom access to transportation would be limited, or the process of getting to a clinic would increase physical and mental stress or be cost-prohibitive. In addition, in-home delivery allows the person to integrate what they are learning right to their home environment and to use their space to help support movement practices.
With this mindful movement component as one part of the interdisciplinary program there is a need for good communication between practitioners and understanding across disciplines to optimize learning and decrease the potential for mixed messages.20,28 By understanding one another’s approach, how the classes intersect, and how information is delivered there can be optimal reinforcement and integration of material. This requires adequate training for each practitioner, and for the EVP MM PT this includes the principles and practices of mindfulness, PNE, MI, and an ACT-informed approach to PiPT. The success of delivery of PiPT and PNE has been shown to be impacted by the PT’s confidence and comfort with the program as well as the therapist having the qualities necessary to implement patient-centered care.20,28,32,35,44,52 Therefore, continued exploration of optimal training for PT’s, including non-evaluative post-training fidelity checks/feedback, is important to the growth of these pain care programs.31,73,74
Limitations
One obstacle that may contribute to attrition is the length of 3 hours a week for 10 weeks. Ongoing QI pilots to address this include splitting the program with the classes spread over two sessions a week and, for less challenged clients, offering one 90-minute condensed session for 8 consecutive weeks, focusing on the ACT and Mindful Movement pieces delivered collaboratively with an EVP PT and psychologist.
While online access is a facilitator to participation, it can also be a barrier, a “digital divide”, with limitations within device, experience level, or connectivity. Current methods to address this have included using loaner tablets on a limited basis. Future quality improvement efforts are focused on identifying, testing, and spreading strong practices and strategies for remote delivery.
To date, EVP MM’s framework has only been implemented in a veteran, mostly male population at two sites. Further implementation of this framework and/or program in multiple sites or for various clinical populations may help provide information on the generalizability and needed adaptations. Findings from the current VA enterprise-wide initiative funded TelePain EVP mixed-methods implementation evaluation includes an examination of barriers and facilitators of the TelePain EVP implementation process and may inform patient-centered systems of care, practice, and policy decision making.
Conclusion
TelePain-EVP Mindful Movement provides a framework for physical therapists to integrate a PIPT mindful movement program that is theory-driven, has real-world implementation, and has been adapted for remote delivery. This program, and on-going implementation evaluation, may also help establish best practices in PiPT mindful movement influencing interdisciplinary clinical care and policy making.
Footnotes
Acknowledgments
Special thanks to the trailblazing present and former EVP Staff, including those members innovating in new settings: Jennifer Gansen DPT; Mary Elizabeth Hammonds PhD; and Jennifer DelVentura PhD. Several authors are employees of the Department of Veterans Affairs, Veterans Healthcare Administration. The views expressed in this article are those of the authors and do not necessarily reflect that of the Department of Veterans Affairs or the federal government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.